
Abstract
Objective:
Radiation-induced oral mucositis (RIOM) is one of the most painful and treatment-limiting toxicities of head and neck cancer (HNC) therapy, often leading to unplanned treatment breaks, dose reductions, compromised oncologic outcomes, and death. Despite its clinical significance, RIOM remains largely unexplored in terms of molecular predictors and prognostic markers. This review bridges radiation biology, transcriptomics, and clinical oncology to reveal how long non-coding RNAs (lncRNAs) orchestrate the injury-repair cycle of irradiated oral mucosa.
Methods:
This review was conducted by a structured screening process to ensure comprehensive coverage of relevant literature. Publications on lncRNAs associated with RIOM were retrieved from PubMed, Web of Science, and clinical trials databases using keywords such as “lncRNAs in RIOM,” “lncRNAs in radiation-induced oral mucositis,” “lncRNAs in oral mucosa,” “lncRNAs in radiation-induced DNA damage and oxidative stress,” “lncRNAs in radiation-induced inflammation,” and “lncRNAs in radiation therapy in head and neck cancer.” Priority was given to studies directly examining lncRNA expression in normal oral mucosa under radiation stress, with additional contextual evidence drawn from cancer and other epithelial injury models when RIOM-specific data were lacking.
Results:
Direct transcriptomic studies of lncRNAs in radiation-exposed normal oral mucosa are scarce. Limited evidence suggests that certain lncRNAs, such as MALAT1 and NEAT1, respond to radiation and influence inflammation, DNA damage repair, and epithelial regeneration. In cancer and other tissue injury contexts, additional lncRNAs, including MEG3, TUG1, and TP53COR1, have been implicated in the regulation of oxidative stress and apoptosis, processes relevant to RIOM pathophysiology. While these findings have not yet been validated in normal irradiated oral mucosa, they highlight biologically plausible candidates for future investigation. Addressing this gap will require integrated approaches that combine pretreatment lncRNA profiling, functional validation in relevant in vitro and in vivo models, and longitudinal patient studies to link molecular signatures with clinical outcomes.
Conclusion:
Current knowledge of lncRNAs in RIOM is largely extrapolated from cancer biology and other epithelial injury models. By prioritizing oral tissue-specific profiling and functional validation under radiation conditions, future research could identify novel biomarkers and therapeutic targets, ultimately enabling precision-guided prevention and management of RIOM. Moreover, proteins regulated by these lncRNAs (if detectable in saliva or serum) could be adapted into rapid, point-of-care lateral flow assays (LFAs) for early clinical decision-making, transforming a currently reactive management paradigm into a proactive, personalized approach.
Introduction
Radiotherapy (RT) is a cornerstone in the treatment of head and neck cancers (HNC), either as a primary modality or in combination with surgery or chemotherapy. However, the efficacy of treatment is frequently hampered by a severe and nearly universal side effect of radiation-induced oral mucositis (RIOM). It leads to painful ulcerations and impaired oral function. Clinical data indicate that the median treatment duration is 41 days, with a mean interruption rate of 14.5% due to toxicity, underscoring the significant impact of RIOM on treatment continuity and outcomes. 1
RIOM is an acute inflammatory and ulcerative condition of the oral mucosa triggered by RT-induced damage to rapidly proliferating epithelial cells. Virtually all patients receiving head and neck RT experience some degree of mucositis, and approximately 35%–56% develop severe (Grade 3 or 4) mucositis, especially when treated with altered fractionation or concurrent chemoradiotherapy.2–4 These severe lesions often necessitate treatment interruption to allow mucosal healing. This not only compromises the continuity and efficacy of RT but also worsens clinical outcomes by increasing the reliance on parenteral nutrition, opioid analgesics, antifungal treatments, and supportive care, thereby escalating hospital costs and reducing the patient’s quality of life.5–7
Despite the high frequency and burden of RIOM, current strategies for its prevention and management remain inadequate. Existing prophylactic approaches, ranging from sucralfate or benzydamine mouthwashes, chlorhexidine rinses, pilocarpine, and keratinocyte growth factor-1 (palifermin), have shown limited efficacy, and many are cost-prohibitive or impractical in resource-limited settings.5–7 In recent years, novel therapeutic approaches, such as cell-based treatments, platelet lysates, and immune cell-based interventions, have shown promise in preclinical and early clinical studies, although their widespread application is still under investigation. 8 Even with optimal oral hygiene and supportive care, mucositis occurs in nearly all patients undergoing head and neck RT, with a substantial proportion experiencing debilitating and treatment-limiting toxicity.
Given this urgent clinical challenge, there is a critical need to identify reliable radiation-specific molecular biomarkers that can predict the risk and severity of RIOM before therapy initiation. Currently, diagnosis and grading are based on clinical presentation or cytological evaluation, which are subjective, labor-intensive, and incapable of offering predictive insight. To date, no validated biomarkers are available globally for the early prediction or prognosis of RIOM, representing a major unmet need in the management of HNC.
Recent advances in transcriptomics have highlighted the potential role of long non-coding RNAs (lncRNAs) as regulators of radiation response. LncRNAs, which are transcripts longer than 200 nucleotides without protein-coding capacity, participate in numerous cellular processes, including inflammation, apoptosis, DNA repair, and tissue regeneration, all of which are central to RIOM pathogenesis. 9 Radiation-induced alterations in lncRNA expression profiles have been reported in various cancer models and cell systems, suggesting their feasibility as novel biomarkers for radiation injury.10–12
This review consolidates the emerging evidence linking lncRNAs to the pathobiology of RIOM, emphasizing their potential predictive and prognostic value. We highlight the mechanistic relevance of radiation-responsive lncRNAs to mucosal injury and repair and evaluate their utility in developing a cost-effective, non-invasive tool for early risk assessment and personalized RT planning in patients with oral cancer.
Literature Search and Study Selection
Publications on lncRNAs in the context of RIOM were retrieved from PubMed, Web of Science, and clinical trial databases. Search strategies combined terms such as “lncRNAs in RIOM,” “lncRNAs in radiation-induced oral mucositis,” “lncRNAs in oral mucosa,” “lncRNAs in radiation-induced DNA damage and oxidative stress,” “lncRNAs in radiation-induced inflammation,” and “lncRNAs in radiation therapy in head and neck cancer.”
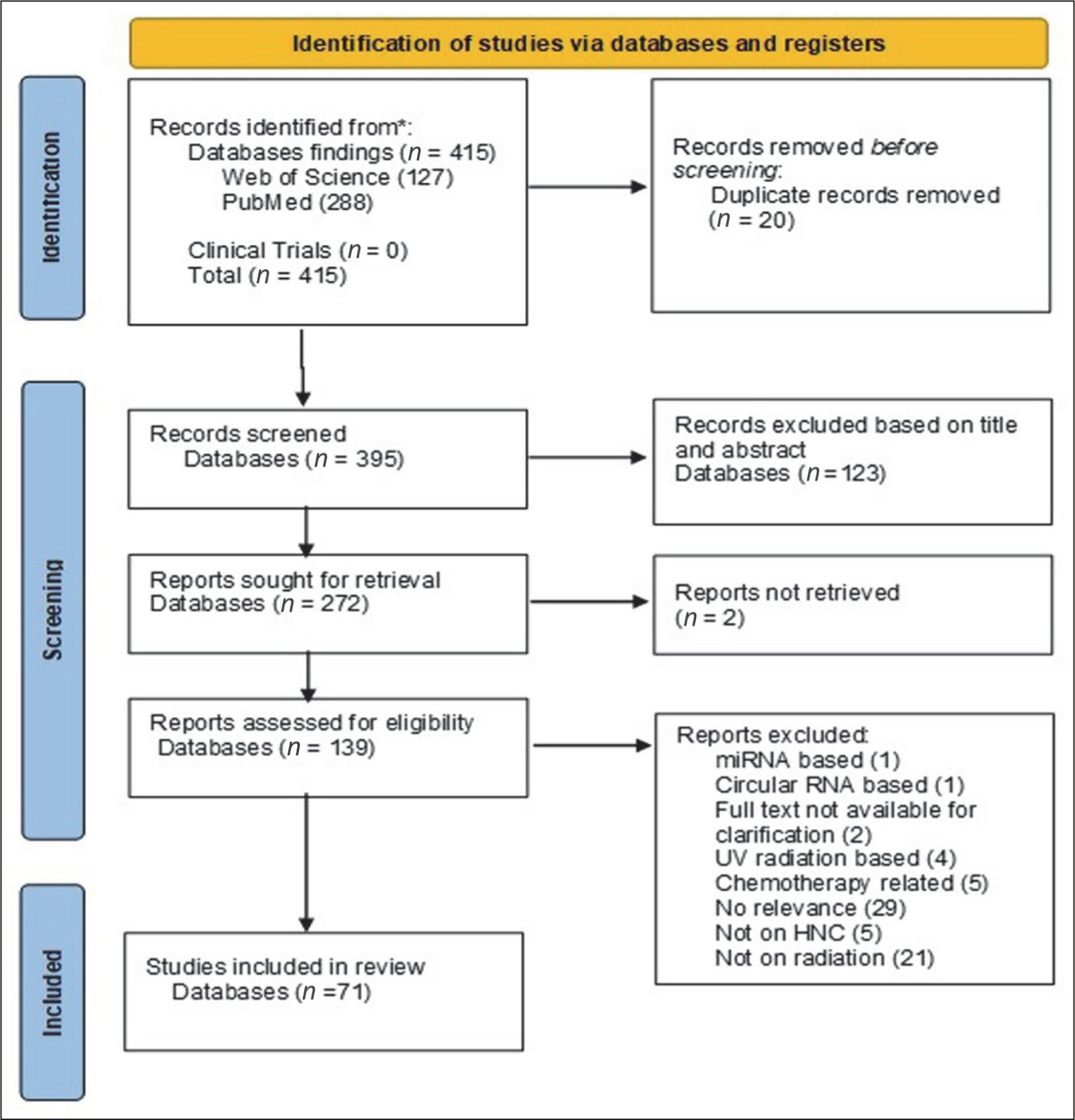
Priority was given to studies directly examining lncRNA expression in normal oral mucosa under radiation stress. In the absence of RIOM-specific data, contextual evidence was drawn from studies in HNCs and other epithelial injury models. The search yielded 415 records, of which 20 duplicates were removed. After screening 395 records by title and abstract, 272 were assessed for retrieval. Following full-text evaluation of 139 articles, 68 were excluded for the following reasons: miRNA-based (n = 1), circular RNA-based (n = 1), full text not available (n = 2), UV radiation-based (n = 4), chemotherapy-related (n = 5), not relevant (n = 29), not on HNCs (n = 5), or not related to radiation (n = 21). Ultimately, 71 studies were included in this review (Figure 1).
PRISMA Flowchart of Literature Screening and Selection Process.
LncRNAs as Biomarkers and Regulators in RIOM
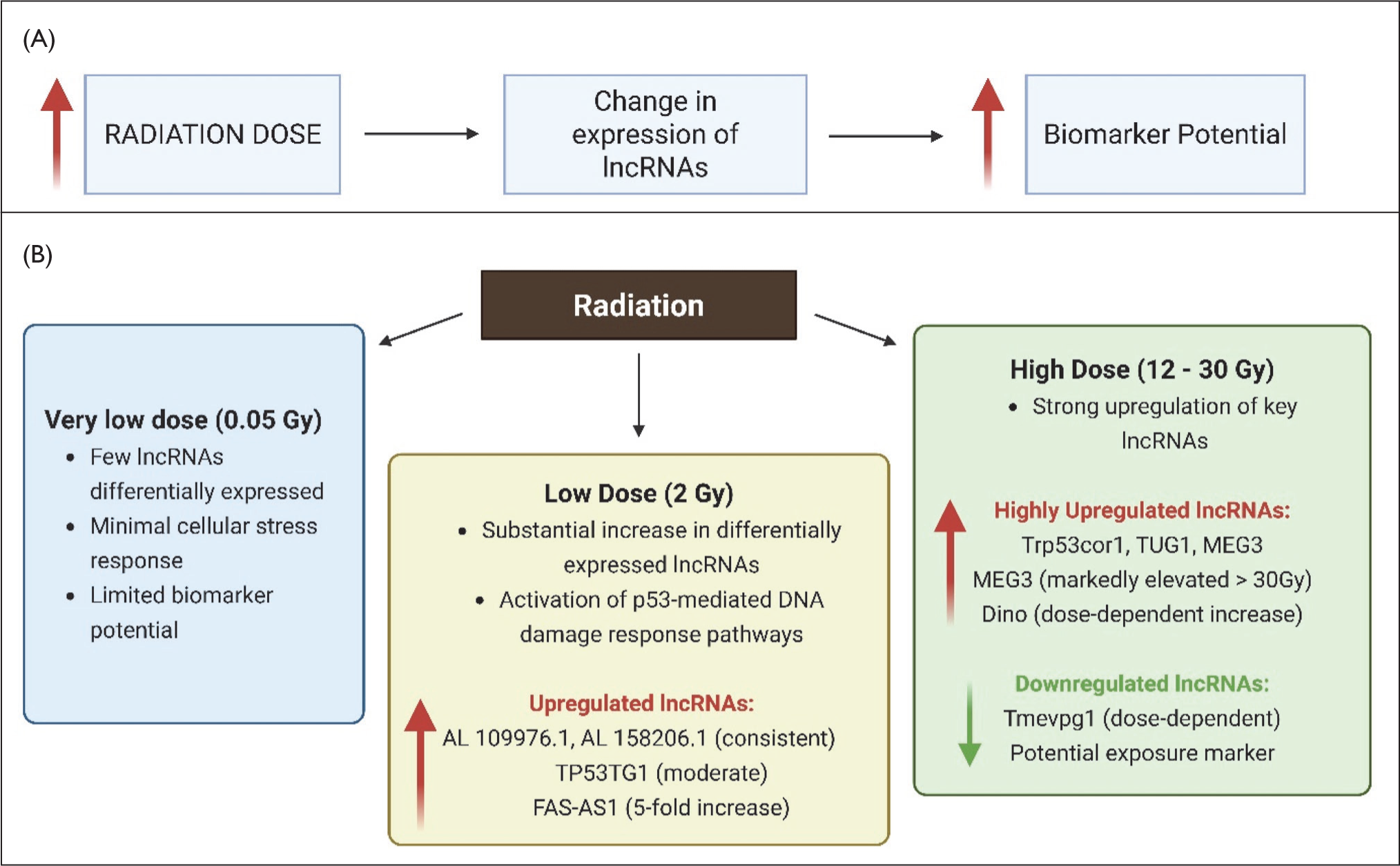
LncRNAs play a significant role in regulating cellular responses to radiation through mechanisms such as microRNA sponging and interaction with various proteins. Due to these functions, lncRNAs are increasingly recognized as potential diagnostic and prognostic biomarkers for radiation-induced tissue damage, including RIOM. Several lncRNAs have been observed to change expression levels following radiation exposure, with notable upregulation of TP53COR1, TUG1, DINO1, MEG3, PVT1, MIR4435-2HG (MORRBID), HOTAIR, GAS5, ANCR, CCAT1, LINC00963, UCA1, TP53TG1, FAS-AS1, and PAPPA-AS1, alongside the downregulation of Tmevpg1.11,12 Among these, TP53COR1, TUG1, and MEG3 stand out as consistently validated markers across multiple radiation exposure models and have been implicated in the regulation of p53-mediated pathways, particularly those governing cell cycle progression and apoptosis. 13 While MEG3 is thought to function as a tumor suppressor by stabilizing p53 protein, other lncRNAs, such as MALAT1, PVT1, and TUG1, have demonstrated oncogenic properties, highlighting the diverse and context-dependent roles of lncRNAs in radiation response and tumor biology. 11 Recent transcriptomic analyses have demonstrated that lncRNA expression varies significantly with radiation dose, suggesting a dose-dependent regulatory response. At a very low dose of 0.05 Gy, only a few lncRNAs were differentially expressed, with slight variations across the lymph node status groups. In contrast, exposure to a low dose of 2 Gy triggered a substantial increase in the number of differentially expressed lncRNAs across all groups. Notably, AL109976.1 and AL158206.1 were consistently upregulated at this concentration. Co-expression analysis has linked these lncRNAs to key pathways, including the p53-mediated DNA damage response (DDR) and cell cycle regulation, highlighting their potential role in radiation-induced cellular stress adaptation. 10 Moderate increases in TP53TG1 and FAS-AS1 were also observed at low doses in cultured lymphocytes, with FAS-AS1 showing up to a fivefold increase. 12 High doses induce strong upregulation of lncRNAs, including TP53COR1, 13 TUG1 and MEG3, with MEG3 being markedly elevated at doses above 30 Gy in humans 13 and 12 Gy in mice. 11 Other lncRNAs display variable responses: Dino increases dose-dependently, PVT1 and MORRBID show inconsistent upregulation, while IFNG-AS1 is uniquely downregulated in a dose-dependent manner, potentially serving as a marker of radiation exposure. 11 These dose-dependent patterns reflect a complex lncRNA regulatory network activated by radiation, which may aid in biomarker development and patient risk assessment, and may serve as a distinguishing marker between exposed and non-exposed individuals (Figure 2). In addition, induction of the lncRNA Dino and the p53 pathway-associated genes CDKN1A, DDB2, BBC3 (PUMA), and microRNAs was also observed, indicating activation of p53-mediated DDR. 14 Although much of the current knowledge on lncRNAs is derived from cancerous tissues, their function in normal oral mucosa, particularly under conditions of stress, such as ionizing radiation, remains less well understood. Outside oncogenic contexts, radiation exposure has been shown to alter lncRNA expression in various cell types, suggesting that these molecules play roles in modulating radiation response and stress signaling.12,15 Radiation exposure can induce complex molecular responses in oral epithelial cells, including DNA damage, inflammation, and repair mechanisms, in which lncRNAs may play critical regulatory roles. Taken together, these findings suggest that specific lncRNAs respond sensitively to radiation-induced damage and have the potential to be used as biomarkers to predict or monitor the onset and severity of RIOM. Understanding their precise regulatory roles may open new avenues for early detection and targeted interventions to reduce mucosal injury in patients undergoing RT.
Dose-dependent Regulation of LncRNAs by Ionizing Radiation and Their Biomarker Potential. (A) Increasing Radiation Doses Lead to Differential Regulation of Specific LncRNAs, Reflecting Their Potential as Biomarkers for Radiation Exposure and Cellular Response. (B) Distinct LncRNA Profiles Across Various Dose Ranges. For Example, at Low Dose, AL109976.1 Is Involved in Immune Modulation, Autophagy, and Radiosensitivity; AL158206.1 Regulates DNA Repair and Epithelial–Mesenchymal Transition (EMT); TP53TG1 Contributes to Apoptosis and EMT; FAS-AS1 Is Implicated in Fas-mediated Apoptosis. While at High Dose, TP53COR1 Is Upregulated, Which Plays a Role in Tumor Suppression and Radioresistance; TUG1 Is Linked to Proliferation and Drug Resistance; MEG3 Exhibits Anti-proliferative and Anti-angiogenic Functions; Dino Stabilizes P53 and Enhances Chemosensitivity. Importantly, IFNG-AS1 (Tmevpg1) Is Progressively Downregulated in a Dose-dependent Manner, and May Serve as a Marker of Radiation Exposure.
Oncogenic LncRNA Networks Driving Radioresistance and Oral Mucosal Toxicity
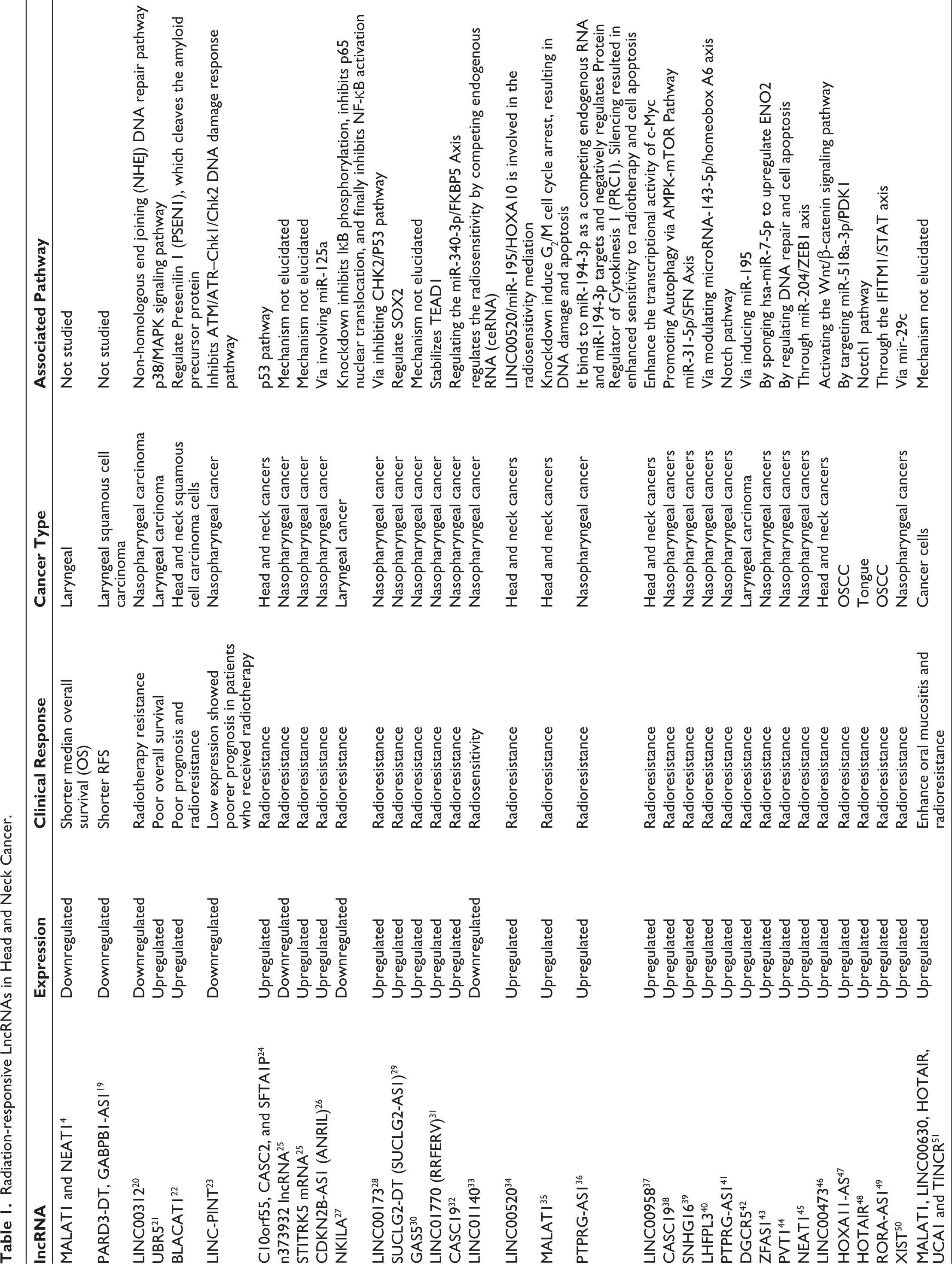
A growing body of evidence indicates that multiple lncRNAs are responsive to radiation in HNC, with potential implications for RIOM) As summarized in Table 1, lncRNAs such as MALAT1, NEAT1, BLACAT1, CASC19, HOXA11-AS, and HOTAIR are consistently upregulated following irradiation and contribute to pathways involved in DNA damage repair, oxidative stress, apoptosis, and epithelial homeostasis. Conversely, lncRNAs such as LINC00312, LINC-PINT, NKILA, and n373932 are downregulated, and their loss is associated with impaired DNA repair or heightened NF-κB activity, promoting radioresistance. Notably, several lncRNAs, including MALAT1, NEAT1, HOTAIR, and UCA1, have been implicated both in enhancing oral mucositis severity and in promoting radioresistance, suggesting a dual role at the interface of tissue injury and tumor progression. Although these findings derive primarily from tumor tissue studies, the same regulatory axes, such as p53, NF-κB, Wnt/β-catenin, and ceRNA networks, are highly relevant to radiation-induced injury in normal oral epithelium.16–18 Thus, mapping these lncRNA-driven pathways in non-malignant oral mucosa represents a critical next step. This may ultimately allow certain lncRNAs, or their regulated protein products, to be translated into clinically feasible biomarkers (e.g., lateral flow assays [LFAs]-based assays) for predicting RIOM risk before RT.
Radiation-responsive LncRNAs in Head and Neck Cancer.
LncRNAs in Normal Oral Mucosa
LncRNAs are increasingly recognized as important regulators of gene expression in the oral mucosa, contributing to tissue homeostasis and cellular function. Early studies profiling lncRNA expression have demonstrated that these transcripts are actively expressed in normal oral mucosa and undergo significant alterations in oral premalignant lesions, suggesting a potential role in early mucosal changes preceding malignancy. 52 More recent transcriptome-wide analyses comparing oral squamous cell carcinoma (OSCC) to healthy oral mucosa have identified numerous lncRNAs with differential expression, reinforcing the idea that lncRNAs are involved in the progression from normal tissue to cancer. 53 However, studies directly investigating lncRNA expression and function in radiation-exposed normal oral mucosa are scarce. Elucidating these roles is essential for understanding RIOM and developing targeted interventions to mitigate mucosal injury during cancer treatment.
Pathogenesis of RIOM and Putative Roles of LncRNAs
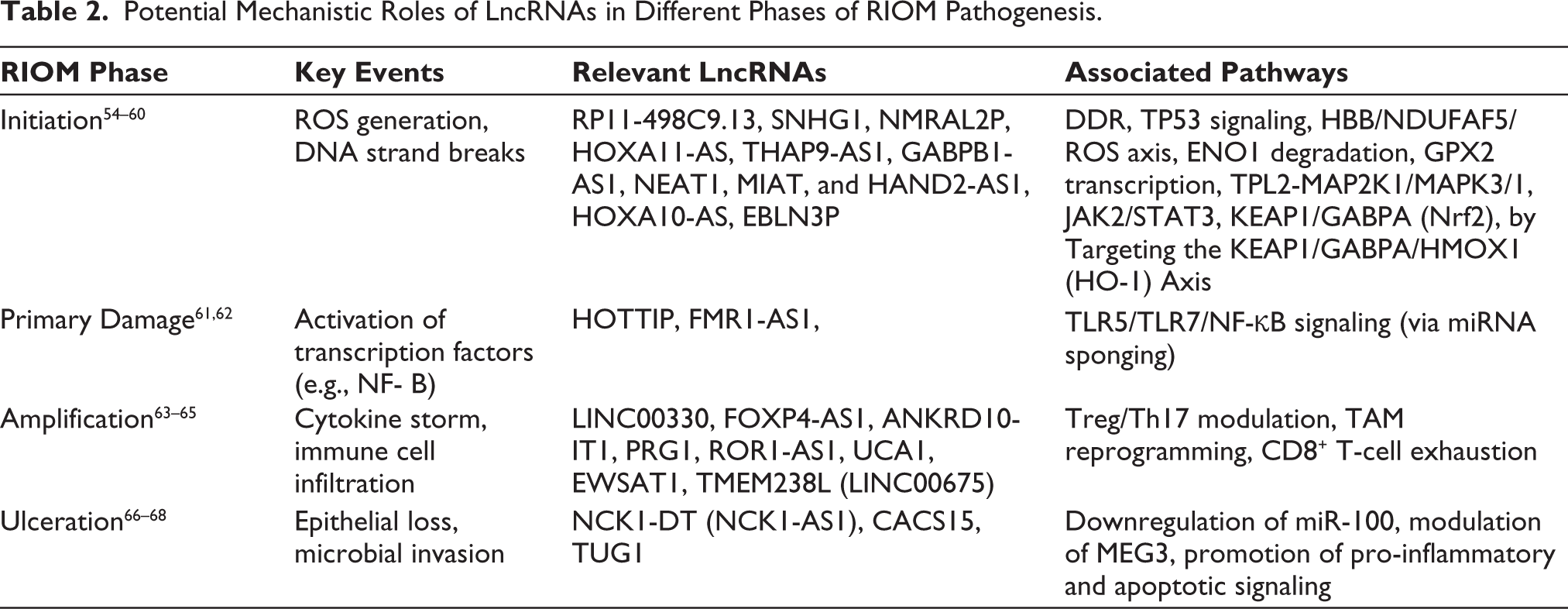
LncRNAs display highly specific expression patterns that vary by tissue type and pathological context, making them promising candidates for biomarker development. The pathogenesis of RIOM involves a complex interplay of biological processes initiated by radiation-induced damage to the basal epithelial cells and the submucosal tissues. A widely accepted model describes five sequential phases: initiation, primary damage response, signal amplification, ulceration, and healing. Central to these stages is the release of inflammatory mediators, oxidative stress, DNA damage, and disruption of epithelial integrity, which collectively drive mucosal injury and delayed recovery. 9 The involvement of specific lncRNAs across the five well-characterized phases of RIOM pathogenesis, including their mechanistic contributions to tissue injury and repair, is outlined in Table 2.
Potential Mechanistic Roles of LncRNAs in Different Phases of RIOM Pathogenesis.
DNA Damage and Oxidative Stress
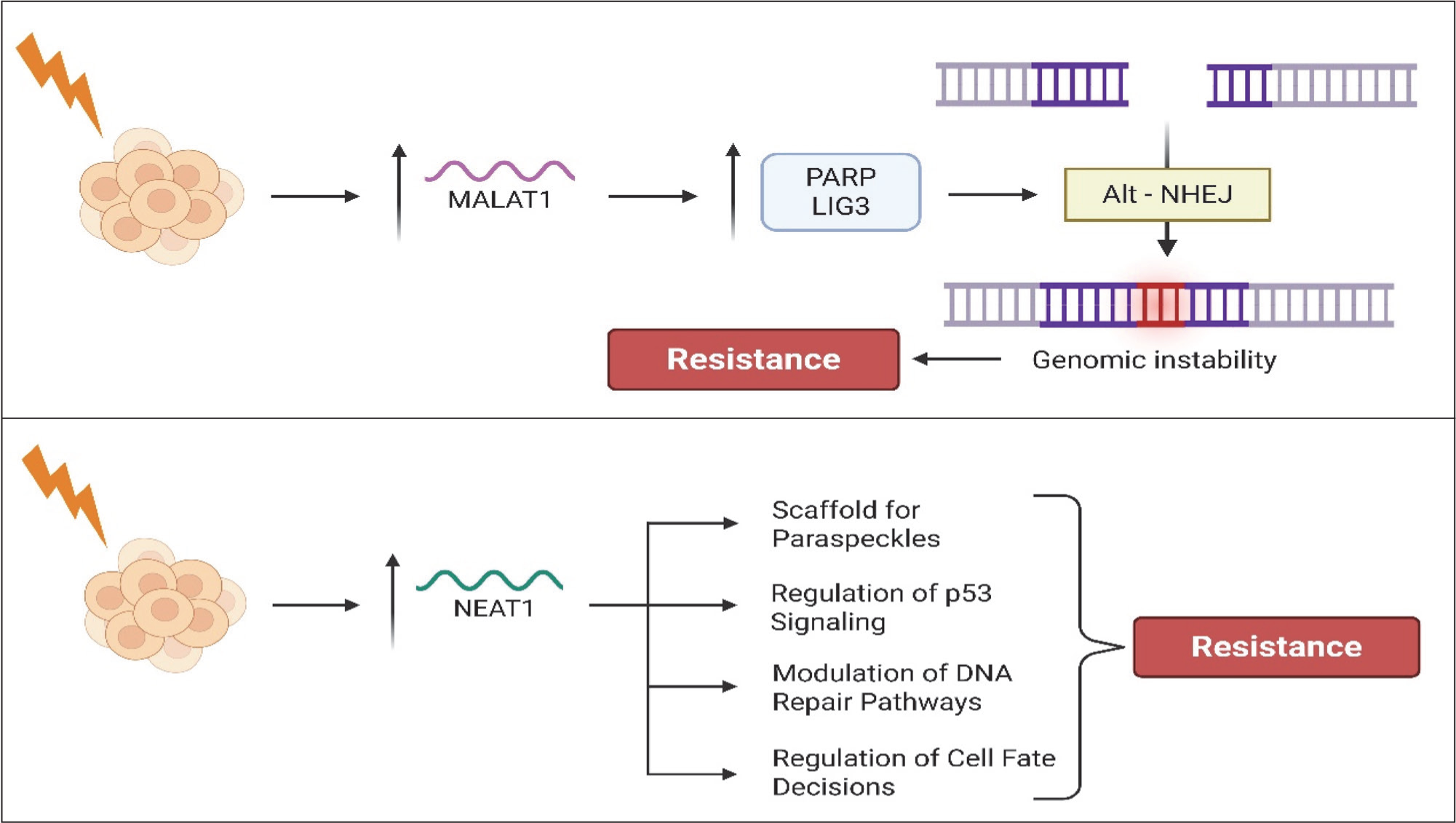
Ionizing radiation primarily causes cell damage by producing reactive oxygen species (ROS), leading to DNA strand breaks and activation of apoptotic pathways. Among the molecules involved in the cellular response to such damage are lncRNAs, such as MALAT1 and NEAT1, which play important roles in regulating the DDR and influence cell survival after irradiation. MALAT1, in particular, is believed to stabilize transcripts related to oxidative stress defense and may modulate the function of p53, a key factor regulating apoptosis in irradiated epithelial cells. Clinical observations in patients with HNC have revealed significant fluctuations in MALAT1 expression during treatment. Serum MALAT1 levels notably decreased after intensity-modulated radiotherapy (IMRT) (p < .001) and chemotherapy (p = .021), suggesting its potential as a marker for treatment response. Conversely, high MALAT1 expression in tumor tissue correlates with more advanced disease stage (p = .009), poor histological differentiation (p = .002), and lymph node metastasis (p = .011), indicating a complex and context-dependent role in cancer progression. 69 Separately, another study examining patients with RIOM found that those with severe (Grade 3) mucositis tended to have slightly higher MALAT1 and NEAT1 expression levels, although these differences were not statistically significant (MALAT1: 0.41 vs. 0.38, p = .891; NEAT1: 0.42 vs. 0.39, p = .522). 4 The association between their elevated expression and increased mucositis severity suggests that these lncRNAs may play a role in regulating tissue responses to radiation-induced injuries. Furthermore, the high combined expression of MALAT1 and NEAT1 has been linked to poorer overall survival in patients undergoing radiotherapy, underscoring their potential prognostic value (Figure 3).
Mechanisms of MALAT1 and NEAT1-mediated Radiation Resistance. This Schematic Illustrates the Distinct Roles of MALAT1 and NEAT1 in Promoting Resistance to Radiation-induced DNA Damage. Upon Exposure to Radiation, MALAT1 Expression Is Upregulated, Enhancing the Recruitment of PARP and LIG3 and Activating the Alternative Non-homologous End Joining Repair Pathway. In Parallel, Radiation Induces the Upregulation of NEAT1, Which Contributes to Resistance Through Multiple Mechanisms, Including Acting as a Scaffold for Paraspeckles, Regulating p53 Signaling, Modulating DNA Repair Pathways, and Influencing Cell Fate Decisions. These Combined Effects Contribute to Enhanced Cell Survival Following Radiation Exposure.
Antagonistic Pleiotropy of LncRNAs in Tumor Radioresistance and RIOM Repair
The ulcerative stage of RIOM is a pivotal and symptomatic phase marked by epithelial breakdown, microbial infiltration, and deep mucosal ulceration. Although direct evidence linking specific lncRNAs to ulcer formation in RIOM is limited, studies have identified key inflammatory and regulatory roles for lncRNAs, such as MALAT1 and NEAT1, in the radiation response. Clinical observations suggest that lower expression levels of these lncRNAs correlate with increased severity of mucositis, anemia, and liver dysfunction, implying a protective role against radiation-induced epithelial injuries. Conversely, MALAT1 is consistently overexpressed in aggressive head and neck squamous cell carcinoma (HNSCC) and is known to activate oncogenic signaling pathways, such as EZH2/STAT3/AKT1, with downstream activation of NF-κB and β-catenin, both of which are also implicated in RIOM pathogenesis by stimulating inflammatory cytokines and generating oxidative stress. 70 Similarly, UCA1, activated by radiation, engages the AKT pathway to support cell survival but may impair mucosal repair if it is persistently expressed.71,72 These findings highlight the dual nature of lncRNA-mediated responses in RIOM.
Given that immune dysregulation and inflammatory signaling are central to both epithelial injury and repair during the ulcerative phase of RIOM, insights from other immune-mediated mucosal ulcerative disorders may help explain the context-dependent dual functions of lncRNAs. Emerging data from other mucosal ulcerative disorders provide compelling insights. A transcriptomic study of treatment-naïve patients with ulcerative colitis (UC) used RNA sequencing and dual alignment approaches to identify 99 differentially expressed lncRNAs, including 15 previously uncharacterized transcripts. These lncRNAs were co-expressed with 602 protein-coding genes, and KEGG enrichment analysis indicated their association with biologically relevant pathways, including T-cell receptor signaling and lipid metabolism. 73 This finding suggests a potential regulatory role of lncRNAs in immune-mediated mucosal injury, analogous to the immune dysregulation observed in RIOM. Although these UC-associated lncRNAs have not been studied in the context of the oral mucosa, the shared features of epithelial inflammation, barrier compromise, and immune activation support their possible relevance in radiation-induced ulcers.
In addition, broad reviews of lncRNA involvement in chronic inflammatory diseases, including cardiovascular disease, osteoarthritis, sepsis, asthma, COPD, and acute lung injury, have consistently highlighted lncRNAs as critical modulators of inflammatory signaling, macrophage polarization, and cytokine expression. These include lncRNAs that regulate NF-κB, STAT3, and TLR pathways, which are core components of the pro-inflammatory response observed in RIOM. The parallels in immunopathology further strengthen the hypothesis that lncRNAs could influence the inflammatory cascades and epithelial degeneration underlying ulcer formation in RIOM. 74
Additional support for the involvement of lncRNAs in oral inflammatory modulation comes from a transcriptomic study examining the effects of cryotherapy on LPS periodontal ligament cells. Although not focused on radiation injury, this study revealed that cryotherapy significantly suppressed the expression of pro-inflammatory cytokines, such as IL1B and IL6, by downregulating lncRNA SNHG1. Mechanistically, SNHG1 acts as a competing endogenous RNA (ceRNA) that sequesters miR-9-5p, thereby sustaining NFKB1 expression. Disruption of this lncRNA–miRNA–mRNA regulatory loop attenuates the inflammatory response. 75 However, at the same time, SNHG1 also enhances tumorigenesis via decreasing Poly(ADP-ribose) polymerase family member 6 (PARP6) expression. 76 These findings highlight the central role of lncRNAs in modulating NF-κB signaling and provide additional rationale for exploring similar ceRNA networks in the context of RIOM, particularly given the prominent role of NF-κB in radiation-induced mucosal inflammation. Further evidence for the involvement of lncRNA-mediated ceRNA networks in oral inflammatory diseases comes from a study investigating the immunomodulatory dysfunction of mandibular bone marrow-derived mesenchymal stem cells (BM-MSCs) in a mouse model of periodontitis. The study identified that lncRNA SPIRE1, which is downregulated in BM-MSCs under inflammatory conditions, acts as a competitive endogenous RNA (ceRNA) for miR-181a-5p, thereby regulating the expression of prolactin receptor (PRLR) and the activation of the JAK/STAT3 pathway. Functionally, this regulatory axis modulates the Th17/Treg cell differentiation balance, which is a critical determinant of mucosal immune homeostasis. Although not directly focused on radiation injury, these findings provide mechanistic insights into how lncRNAs in the oral microenvironment influence immune signaling and tissue inflammation. Given the immune dysregulation observed during the ulcerative phase of RIOM, particularly involving pro-inflammatory cytokines and T-cell responses, the SPIRE1/miR-181a-5p/PRLR/STAT3 axis may represent a transferable immunoregulatory pathway that is worth investigating in radiation-induced mucosal injury. 77
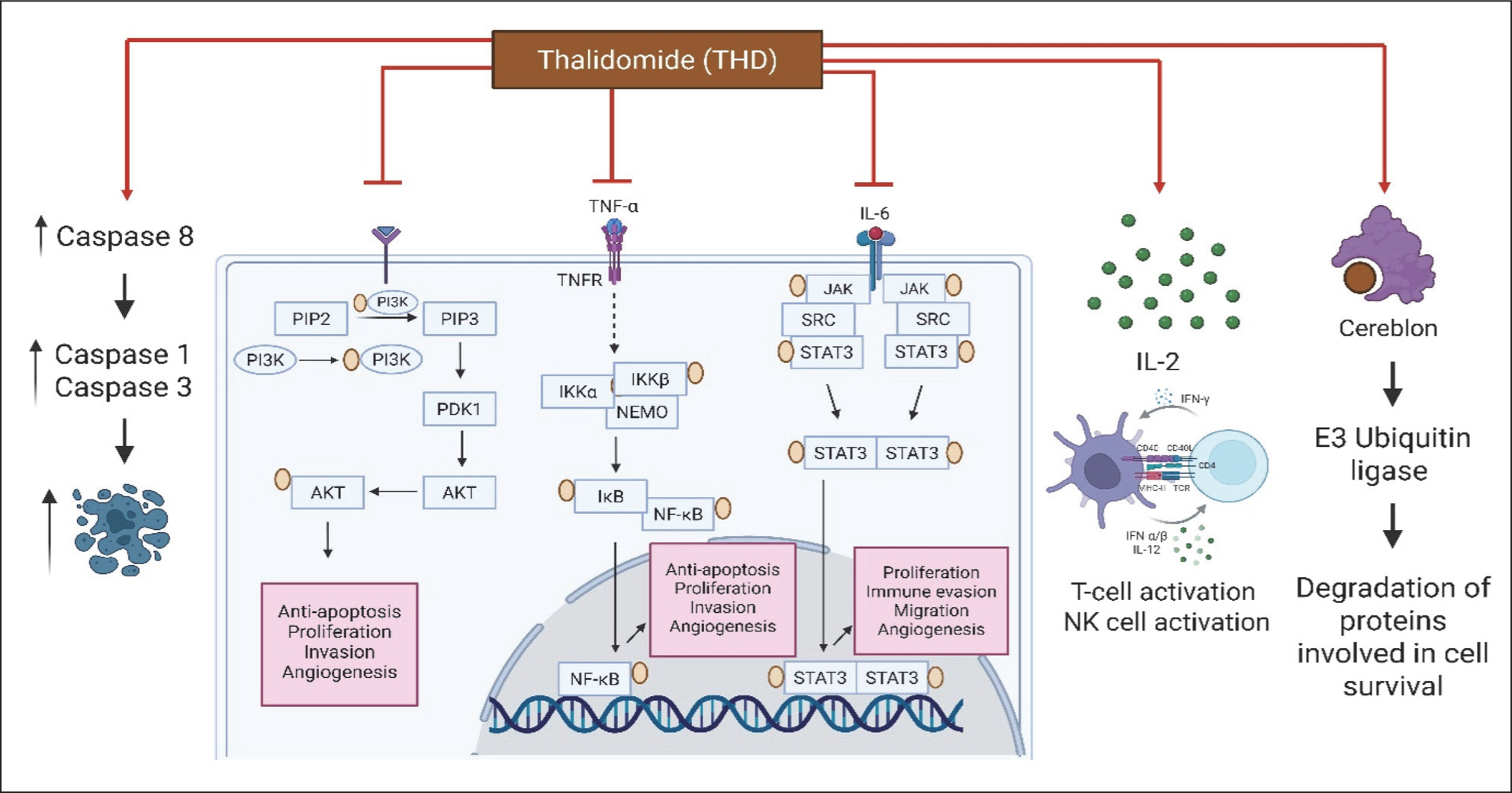
Moreover, therapeutic interventions targeting lncRNA-regulated pathways are being developed. For instance, thalidomide (THD) has been shown to reduce RIOM severity in patients with nasopharyngeal carcinoma by upregulating LZTS3, a negative regulator of inflammation and apoptosis in irradiated cells. 78 This, combined with lncRNAs such as MALAT1 and NEAT1, underscores a broader molecular framework wherein ncRNAs and associated modulators jointly orchestrate epithelial damage, inflammation, and repair in RIOM. It is also important to note that both of these lncRNAs promote radioresistance.35,45 As illustrated in Figure 4, THD exerts these effects by suppressing NF-κB/STAT3 signaling, enhancing caspase activation, and promoting immune modulation, thereby intersecting with lncRNA-regulated stress response pathways.
Mechanistic Actions of Thalidomide (THD) in Modulating RIOM Through LncRNA-regulated Pathways. THD Attenuates Epithelial Injury and Inflammation by Suppressing NF-κB and STAT3 Signaling, Reducing the Transcription of Pro-apoptotic and Pro-inflammatory Genes. It Enhances Caspase-8 Activity While Modulating Caspase-1 and Caspase-3, Thereby Rebalancing Apoptosis and Survival in Irradiated Cells. THD Also Promotes IL-2–Mediated T-Cell and NK Cell Activation and Targets Cereblon-mediated E3 Ubiquitin Ligase for Degradation of Proteins Critical for Tumor Survival. These Mechanisms Intersect With LncRNA-driven Regulatory Axes, Such as MALAT1 and NEAT1, Highlighting a Convergent Molecular Framework Where NcRNAs and Pharmacological Modulators Orchestrate the Balance Between Epithelial Damage, Immune Activation, and Repair.
Taken together, these findings indicate that a number of lncRNAs, which stimulate radioresistance, survival signals, and repair of the damaged DNA in HNSCC, also play a role in epithelial integrity, inflammatory resolution, and healing of the oral mucosa upon irradiation. Although these lncRNAs improve the survival of tumor cells during radiation stress, they can also improve the recovery of mucosa by inhibiting apoptosis, stabilizing epithelial cells, and regulating the cascades of inflammation. This duality has made lncRNAs molecular “two-sided swords which makes it difficult to address radiation toxicity and preserve tumor control.” This effect is an example of antagonistic pleiotropy, whereby the same lncRNAs promote a survival benefit to tumor cells exposed to radiation stress and, at the same time, promote epithelial healing and inflammatory clearance of normal oral mucosa. The findings provide evidence for a conceptual model of antagonistic pleiotropy in RIOM, where lncRNAs act as molecular two-sided swords at the tumor-mucosa interface.
The Oral Microbiome-lncRNA-immune Axis in RIOM
RIOM is progressively being considered as a multifactorial process where the injury of the epithelium is exaggerated by the presence of microbial dysbiosis and activation of the immune system. The oral cavity supports a complex microbiome, which is vital in ensuring mucosal homeostasis, but radiotherapy interferes with this balance, causing pathogenic bacteria to overgrow and loss of commensal species. This radiation-induced dysbiosis acts as a potent driver of mucosal inflammation and ulceration. Moreover, pathogenic species also play a role in the aggravation of the complications of the RIOM, which is the most frequent side effect of the radiation therapy of HNSCC. 79
Emerging evidence indicates that microbial signals produced in the context of dysbiosis regulate host transcriptomic responses, including lncRNA regulation. It was recently demonstrated that the abnormal lncRNA expression in the oral cavity is caused by the dysbiosis of the oral microbiome (including Fusobacterium, Pseudomonas, Bifidobacterium and Actinobacter) under the influence of some risk factors. 80 Toll-like receptor 4 (TLR4) pattern recognition receptors, which sense bacterial lipopolysaccharides, are stimulated in irradiated oral mucosa, trigger the downstream NF-kB and MAPK signaling cascades and determine the intensity and duration of the mucosal immune response.81–83 Although these mechanisms can initially facilitate epithelial defense and healing, the chronic activation of lncRNAs in the context of chronic dysbiosis can be associated with excessive inflammation, slow healing, and persistence of ulcers. In this regard, the lncRNAs can act as a molecular mediator between microbial dysbiosis and host immunity.
The microbiome-lncRNA-immune axis provides a significant degree of complexity to the pathogenesis of RIOM, beyond the classic model of injury-repair. Instead of working independently, lncRNAs are a part of an interactive network which is affected by oral microbes, epithelial stress, and immune reactions. This interaction can be used to support why the severity of RIOM is different across patients and suggest that combined interventions that focus on both the oral microbiome and lncRNA-regulated pathways might enhance the prevention and management of RIOM.
LncRNAs in Tissue Regeneration and Wound Healing
LncRNAs have emerged as important regulators of tissue regeneration and wound healing processes by modulating the expression of genes involved in cell proliferation, differentiation, inflammation, and senescence. In the context of RIOM, where epithelial damage and chronic inflammation impair mucosal repair, lncRNAs play pivotal roles in orchestrating the molecular pathways that control mucosal healing. A key challenge in tissue regeneration is overcoming cellular senescence, which restricts cell renewal and promotes a pro-inflammatory environment. Specific lncRNAs have been shown to inhibit senescence in various tissues, including the skin and liver, thereby promoting cellular rejuvenation and enhancing regenerative capacity. 84 This suggests that targeting lncRNAs could prevent or reverse senescence in irradiated oral mucosa, facilitating faster and more effective wound healing.
lncRNAs also influence stem cell function, which is crucial for regeneration. For example, lncRNA XIST enhances osteogenic differentiation of periodontal ligament stem cells by recruiting transcription factors to activate key osteogenic genes. 85 This mechanism highlights how lncRNAs regulate stem cell-mediated tissue repair, which is relevant for oral mucosal recovery after radiation injuries.
Moreover, lncRNAs such as TUG1 86 and MEG3 87 modulate signaling pathways, such as Wnt/β-catenin, which are essential for cell proliferation, apoptosis, and differentiation during wound healing. By controlling these pathways, lncRNAs contribute to the restoration of the epithelial barrier and resolution of inflammation in the damaged mucosa.
In summary, lncRNAs serve as crucial molecular switches in tissue regeneration and wound healing by regulating cellular senescence, stem cell differentiation, and signaling pathways. Understanding their specific roles in RIOM may open new avenues for targeted therapies aimed at improving mucosal repair and patient outcomes.
Potential Diagnostic and Therapeutic Implications
LncRNAs offer promising opportunities as biomarkers and treatment targets for RIOM. Their distinct expression during tissue damage and healing may help in the early diagnosis of RIOM and monitoring its progression, allowing for more personalized patient care. From a therapeutic standpoint, lncRNAs that contribute to inflammation or cell death can be targeted to reduce tissue damage. Approaches such as antisense oligonucleotides, small interfering RNAs, or CRISPR-based techniques may suppress harmful lncRNAs, such as HOTAIR or UCA1. Conversely, enhancing the activity of lncRNAs that promote healing could accelerate mucosal repair. Therefore, therapeutic targeting of lncRNAs raises an important clinical dilemma, summarized in Table 3. Delivering these therapies effectively remains a challenge, but recent advances in nanoparticle carriers and exosome-based delivery systems show promise for targeted treatment in preclinical studies. Further investigations are needed to confirm the role of specific lncRNAs in RIOM and to develop safe and efficient delivery methods that can bring these molecular strategies closer to clinical use.
The Therapeutic Dilemma of Targeting Oncogenic LncRNAs in HNSCC and RIOM.
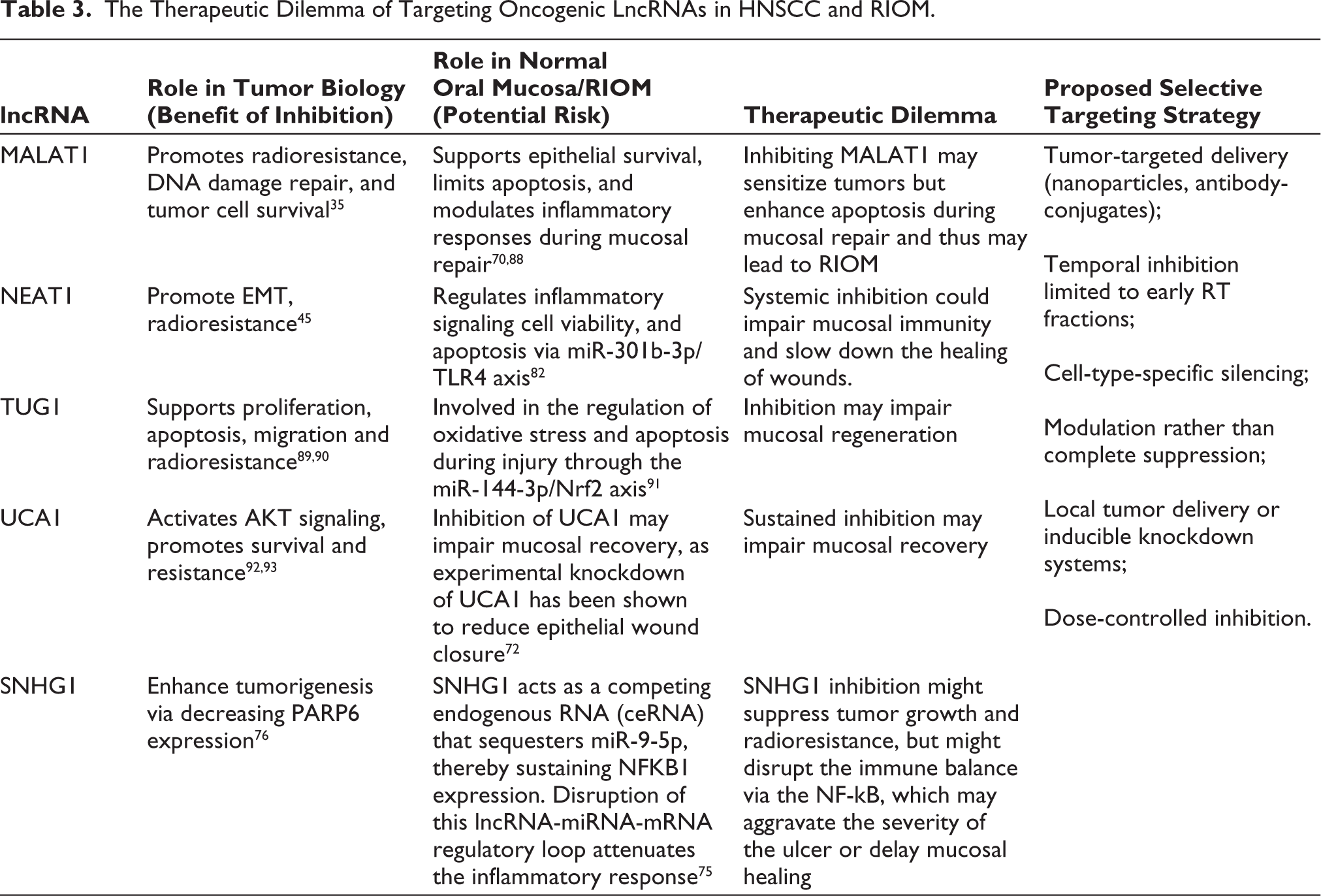
The given therapeutic dilemma highlights the notion of antagonistic pleiotropy, where the same lncRNAs that help to protect normal mucosa against radiation also contribute to tumor radioresistance. As a result, systemic inhibition of oncogenic lncRNAs will lead to a risk of inducing severe RIOM. Future therapeutic interventions should hence focus on selective targeting methods, such as tumor-restricted delivery systems, temporal modulation with radiotherapy cycles, and combination therapy methods that do not compromise mucosal repair but magnifies tumor radiosensitivity.
Limitations and Future Directions
Our current understanding of lncRNAs in RIOM largely depends on studies from related fields, such as cancer biology, radiation effects in other tissues, and general inflammation models. Direct experimental data specifically examining the roles of lncRNAs in the oral mucosa during RIOM are still limited. To bridge this gap, future research should prioritize comprehensive transcriptomic analyses of oral mucosal samples from patients with RIOM to identify relevant lncRNAs. Functional validation through laboratory models, including cell culture systems and animal studies employing targeted knockdown or overexpression of candidate lncRNAs, is crucial to clarify their specific contributions to mucosal injury and repair. Moreover, integrating lncRNA expression profiles with data on inflammatory cytokines, changes in the oral microbiome, and tissue histopathology could provide a more comprehensive understanding of their biological impact. Importantly, a correlation between circulating cell-free DNA and radiation toxicity in patients with prostate cancer has also been identified. 94 Since most Alu elements reside within lncRNAs and untranslated regions of mRNAs, some with regulatory functions, we hypothesized that lncRNAs containing Alu sequences may exhibit radiation dose-dependent expression changes. These lncRNAs may serve as predictive biomarkers for oral mucosal toxicity prior to radiation therapy. Finally, correlating molecular findings with clinical parameters, such as mucositis severity and patient outcomes, will help establish the clinical relevance of lncRNAs. Achieving these goals will require close collaboration across disciplines, bringing together expertise from radiation oncology, molecular biology, and immunology to translate molecular insights into improved diagnostics and therapies for RIOM.
Conclusion
LncRNAs have emerged as key regulators of the complex processes of inflammation, tissue damage, and healing associated with RIOM. While current knowledge is largely derived from related disease models, growing evidence suggests that lncRNAs influence the critical pathways involved in mucosal regeneration and immune responses. Their potential as biomarkers and therapeutic targets offers promising avenues for improving the diagnosis and treatment of RIOM. However, further focused research is needed to fully understand their specific roles in the oral mucosa and develop effective lncRNA-based interventions. Integrating molecular insights with clinical studies is essential to advance personalized management strategies and enhance patient outcomes in RIOM. Such research could yield predictive biomarkers to stratify RIOM risk before the initiation of radiotherapy and inform novel therapeutic strategies targeting lncRNA-regulated pathways. In addition, proteins regulated by these lncRNAs (if detectable in easily accessible biofluids such as saliva or serum) could serve as candidates for rapid, point-of-care testing platforms such as LFAs, enabling early intervention and personalized care. Ultimately, these advances hold the potential to pave the way for precision-guided prevention and therapeutic strategies that can transform the current reactive management of RIOM into a proactive, personalized approach.
Footnotes
Acknowledgements
None.
Authors’ Contribution
MP collected the related article. CJ, MP and SP drafted and wrote the manuscript. RG contributed to the design of the review and assisted in drafting and revising the manuscript. All authors reviewed and approved the final version.
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Institutional Statement
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Parul University.
Patient Consent
Not applicable.