
Abstract
Autoimmune pancreatitis (AIP) is an uncommon inflammatory condition of the pancreas characterized by glandular enlargement and ductal narrowing arising from dysregulated immune activity. Its clinical and imaging overlap with pancreatic malignancy makes accurate distinction essential. We describe a case series of four patients who initially presented with a pancreatic mass suspicious for malignancy, but received a confirmed diagnosis of AIP following thorough diagnostic evaluation. The cohort comprised three male patients (aged 32, 55, and 68 years) and one female patient (aged 73 years). The predominant presenting features included abdominal pain (n=2), scleral icterus (n=3), and pruritus (n=1). Laboratory workup demonstrated elevated total and direct bilirubin in all patients, and serum IgG4 levels were above the normal range in every case. Cross-sectional abdominal imaging with contrast-enhanced CT or MRI identified a pancreatic mass in each patient. All four patients underwent endoscopic ultrasound (EUS)-guided fine needle biopsy (FNB) with rapid on-site evaluation (ROSE), none of which revealed evidence of malignancy. Histopathologic examination showed intact pancreatic acinar architecture in all cases; chronic inflammation and fibrosis were noted in three patients. IgG4 and CD138 immunohistochemical staining was non-reactive in three patients. All patients underwent endoscopic retrograde cholangiopancreatography (ERCP) with biliary stent placement to address biliary obstruction. Interval ERCP confirmed resolution of the obstruction, enabling stent removal without subsequent recurrence. Following establishment of an AIP diagnosis, all patients were treated with a corticosteroid taper, resulting in symptomatic resolution and complete radiologic clearance of the pancreatic mass, with removal of biliary stents thereafter. Patients remained asymptomatic with no evidence of relapse at 3-, 6-, and 12-month follow-up intervals.
Introduction
AIP is becoming increasingly recognized in Western populations, now accounting for approximately 2% of all chronic pancreatitis cases. 1 Two histologically, serologically, and morphologically distinct subtypes have been described. Type 1 AIP, designated as lymphoplasmacytic sclerosing pancreatitis, predominates in Asian populations and is associated with elevated immunoglobulin G4 (IgG4) concentrations. Type 2 AIP, referred to as idiopathic duct-centric pancreatitis, is more prevalent among Caucasians and is linked to granulocytic epithelial lesions and concurrent inflammatory bowel disease. 2
Clinically, AIP type 1 typically manifests with painless jaundice alongside histological hallmarks such as storiform fibrosis, obliterative phlebitis, and multi-organ involvement. By contrast, AIP type 2 commonly presents with abdominal pain and jaundice, is histologically characterized by granulocytic ductal infiltration, and lacks systemic organ involvement. Serologically, AIP type 1 is distinguished by markedly elevated IgG4 levels, frequently exceeding twice the upper limit of normal. Both subtypes respond favorably to corticosteroid therapy; however, relapse in type 2 AIP is uncommon. 2 On cross-sectional imaging, CT characteristically demonstrates a diffusely enlarged pancreas with loss of normal lobular contour and delayed parenchymal enhancement, occasionally accompanied by a rim-like capsular appearance. The main pancreatic duct may show dilatation or an abrupt cutoff. 3 Localized pancreatic enlargement can also occur, creating a focal mass-like lesion on imaging. 3 This constellation of findings poses a significant diagnostic challenge given the considerable overlap with pancreatic ductal adenocarcinoma.4-7
Given this diagnostic ambiguity, distinguishing AIP from pancreatic cancer based solely on clinical findings is difficult, as both conditions can present with weight loss, jaundice, and new-onset diabetes mellitus. Although laboratory and imaging data provide valuable diagnostic clues, the substantial overlap between these two entities frequently complicates the workup. We present a case series of patients whose initial imaging was concerning for pancreatic malignancy, but who were ultimately found to have AIP upon comprehensive evaluation.
Case Series
Case Table
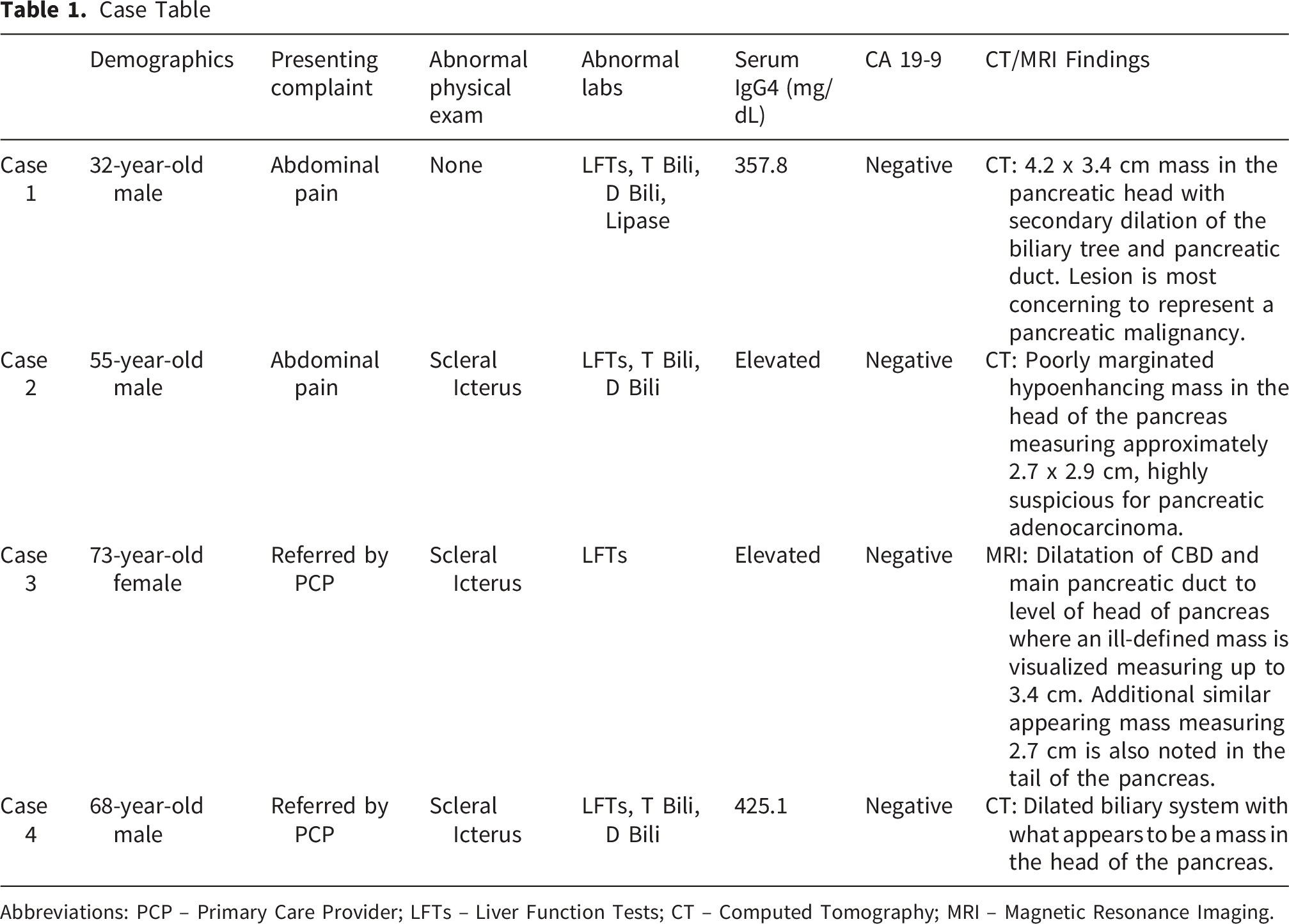
Abbreviations: PCP – Primary Care Provider; LFTs – Liver Function Tests; CT – Computed Tomography; MRI – Magnetic Resonance Imaging.
Case 1
A 32-year-old male was admitted with a three-week history of severe abdominal pain. Physical examination was notable for tenderness in the left upper quadrant and epigastric region. Laboratory evaluation revealed abnormal liver function tests in an obstructive pattern, with a serum lipase of 2128 U/L — more than three times the upper limit of normal. Abdominal and pelvic cross-sectional imaging demonstrated an ill-defined 4.2 × 3.4 cm lesion in the pancreatic head with upstream dilation of both the biliary tree and pancreatic duct, raising concern for pancreatic malignancy (Figure 1A). Notably, serum IgG4 was elevated at 357.8 mg/dL, while CA19-9 was within normal limits. EUS revealed diffuse hypertrophy of the pancreatic parenchyma with a normal-caliber duct and stenosis of the distal common bile duct. Fine needle biopsy of the pseudomass in the pancreatic head demonstrated no evidence of neoplasia. ERCP identified a focal stricture in the common bile duct, and an 8 mm × 8 cm fully covered metal stent was deployed for biliary decompression (Figure 1B). Immunohistochemical staining revealed only minimal IgG4 and CD138-positive plasma cells (fewer than 3 cells per tissue section). Given the cumulative clinical and pathologic picture, AIP was suspected and corticosteroid therapy was initiated. Post-treatment CT imaging demonstrated resolution of peripancreatic fat stranding with a reduction in pancreatic head prominence, indicating a favorable treatment response. The patient achieved clinical and biochemical improvement and was discharged on a steroid taper, subsequently undergoing ERCP for biliary stent removal. (A) MRI Abdomen showing an ill-defined mass in the pancreatic head. (B) ERCP fluoroscopic views showing a common bile duct stricture before treatment (left) and restoration of ductal patency after treatment (right)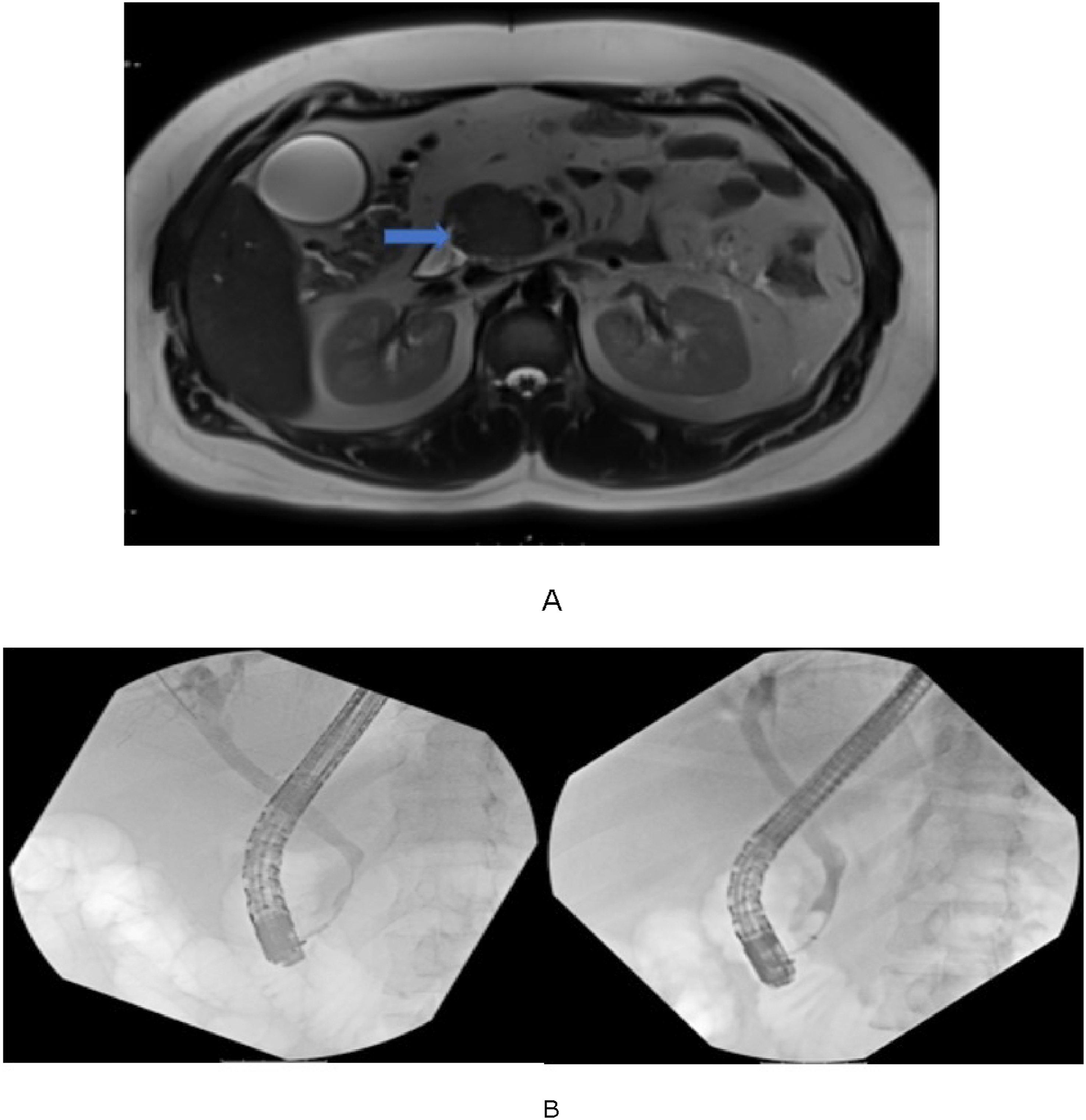
Case 2
A previously healthy 55-year-old male presented with right upper quadrant abdominal pain, scleral icterus, and pruritus. Physical examination confirmed scleral icterus with a soft, non-tender abdomen. Laboratory studies demonstrated an obstructive hepatic enzyme pattern; CEA and CA 19-9 were both negative, while IgG4 was elevated at 425.1 mg/dL. Cross-sectional abdominal imaging identified a poorly defined hypodense mass in the pancreatic head measuring approximately 2.7 × 2.9 cm, raising high suspicion for pancreatic malignancy (Figure 2A). EUS demonstrated an irregular hypoechoic lesion with poorly defined endosonographic margins and enlarged peripancreatic lymph nodes. FNB targeting the pancreatic head was performed, but the specimen was insufficient for definitive diagnosis. ERCP revealed a high-grade stricture in the distal third of the common bile duct, and a 10 mm × 6 cm covered metal stent was placed (Figure 2B). The patient was discharged with outpatient gastroenterology follow-up. However, he subsequently returned with an episode of acute pancreatitis. Repeat cross-sectional imaging showed the hypodense mass to be unchanged, with involvement of the proximal superior mesenteric vein. Repeat EUS with FNB was performed, revealing normal pancreatic acini amid a background of chronic inflammation and fibrosis, with no malignant cells identified. Cytologic examination showed no IgG4-positive cells. Nevertheless, given the imaging characteristics, persistently elevated IgG4, and two consecutive benign biopsies, a diagnosis of AIP was established and steroid therapy was initiated. The patient demonstrated clinical improvement and was discharged for outpatient follow-up. (A) CT Abdomen and Pelvis showing a poorly marginated mass in the head of the pancreas. (B) ERCP fluoroscopic views showing a common bile duct stricture before stent placement (left) and restoration of ductal patency after stent extraction and treatment (right)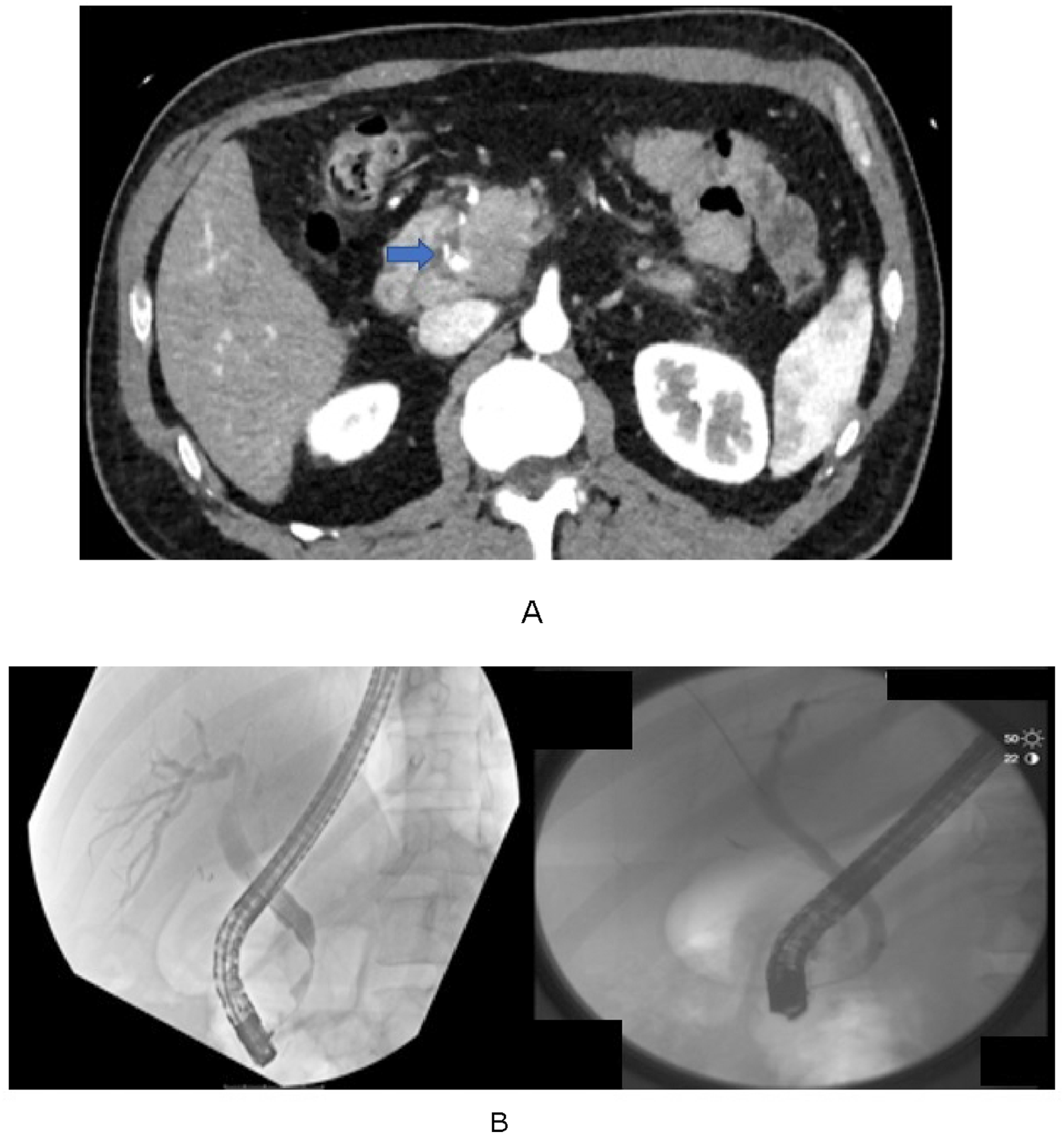
Case 3
A 73-year-old woman with a past medical history of asthma and hypothyroidism was referred for evaluation of new-onset scleral icterus, decreased appetite, acholic stools, and an obstructive liver function test pattern. MRI/MRCP demonstrated dilatation of the common bile duct and main pancreatic duct extending to the level of the pancreatic head, where an ill-defined mass measuring up to 3.4 cm was identified (Figure 3A). An additional similar lesion measuring 2.7 cm was noted in the pancreatic tail. Laboratory results included a markedly elevated IgG4 at 1159.6 mg/dL, CEA of 3.1, and CA 19-9 of 39. EUS demonstrated common bile duct dilation to 14 mm, with diffuse parenchymal echogenicity and lobularity throughout the pancreas and a mass effect on the adjacent bile duct from the head lesion. FNB of the pancreatic head was performed; pathology was negative for malignancy, though cytologic evaluation identified reactive and atypical bile duct epithelial cells. ERCP confirmed a severe stricture in the lower third of the main bile duct with marked biliary dilation; a 10 Fr × 9 cm temporary plastic biliary stent was inserted. A subsequent ERCP demonstrated a smooth stricture, and the initial stent was removed to allow for a stent-free trial (Figure 3B). A follow-up CT scan performed four months later showed no significant interval change. Repeat EUS with tissue sampling showed negative IgG4 and CD138 immunostains with no malignant cells. Corticosteroid treatment was initiated and the patient was discharged with outpatient gastroenterology referral. Follow-up cross-sectional imaging confirmed complete resolution of the previously identified focal pancreatic lesions. The patient continues outpatient follow-up with full symptom resolution and normalized laboratory values. (A) MRI Abdomen showing an ill-defined mass was visualized in the pancreatic head. (B) ERCP fluoroscopic views showing a common bile duct stricture before stent placement (left) and restoration of ductal patency after stent extraction and treatment (right)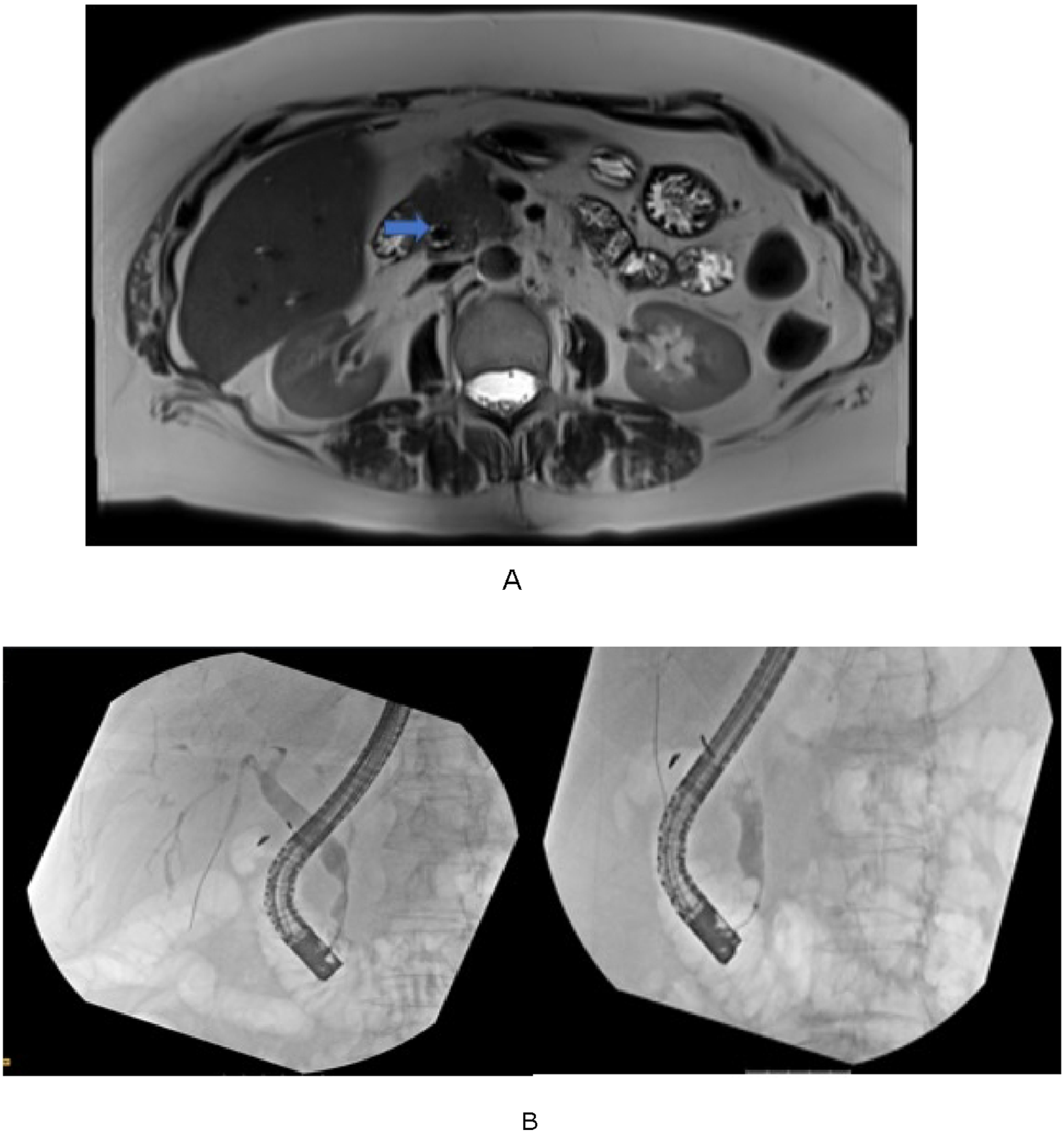
Case 4
A 68-year-old male presented with a progressive history of dark urine and jaundice. Laboratory testing demonstrated an obstructive liver function pattern with a negative CA 19-9. CT of the abdomen identified a dilated biliary system and a mass-like lesion in the pancreatic head. He was discharged from the emergency department with a referral to surgical oncology. A follow-up CT scan demonstrated diffuse sausage-shaped pancreatic enlargement with a peripheral hypoattenuating pseudocapsule and peripancreatic lymphadenopathy (Figure 4A). Severe intra- and extrahepatic biliary dilation was present, with an abrupt ductal cutoff at the junction above the pancreatic head, attributed to autoimmune pancreatitis. He was subsequently referred to gastroenterology for further evaluation. Serum IgG4 was elevated at 425.1 mg/dL. EUS revealed a 40 × 27 mm hypoechoic lesion in the pancreatic head with poorly defined borders. FNB demonstrated pancreatic parenchyma with chronic inflammation and fibrosis; IgG and IgG4 staining showed diffuse non-specific reactivity, rendering the stains non-contributory. ERCP identified a severe stricture in the lower third of the common bile duct, and a covered metal stent was deployed. Corticosteroid therapy was initiated and outpatient follow-up was arranged. Follow-up ERCP for stent removal demonstrated substantial improvement in the common bile duct stricture (Figure 4B). At follow-up, the patient was jaundice-free and asymptomatic; steroids were successfully tapered, and interval MRI three months later demonstrated a reduction in overall pancreatic parenchymal volume with resolution of ductal prominence and a decrease in the extent of common bile duct stenosis. (A) CT Abdomen and Pelvis showing a dilated biliary system with a mass in the head of the pancreas. Also noted is diffuse sausage-like enlargement and enhancement of the pancreas with peripheral hypoattenuating. (B) ERCP fluoroscopic views showing a common bile duct stricture before stent placement (left) and restoration of ductal patency after treatment (right)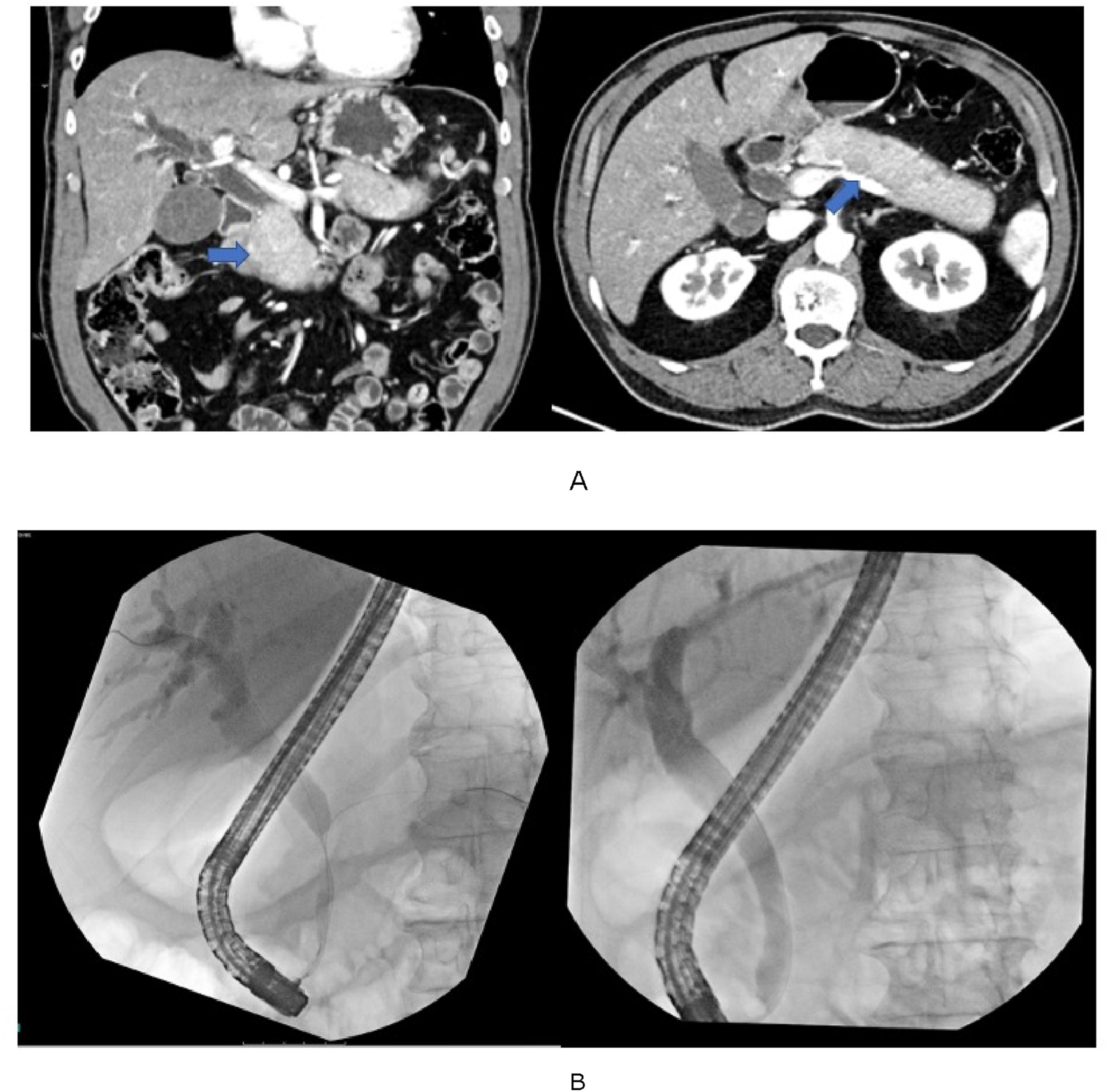
Discussion and Literature Review
Our case series illustrates the diagnostic complexity inherent to AIP, particularly when it manifests as a focal pancreatic lesion that is radiologically indistinguishable from adenocarcinoma. It underscores the importance of employing a multimodal diagnostic approach and emphasizes that malignancy must be rigorously excluded before a diagnosis of focal AIP can be entertained. AIP was first conceptualized in 1995, when a subset of patients was noted to exhibit both chronic pancreatitis and autoimmune features. The condition received its formal diagnostic classification in 1996. 8 Two subtypes of this disease are recognized in the literature. Type 1 AIP is by far the more prevalent form, accounting for the majority of cases in the United States and Europe and virtually all cases in Korea and Japan. 8
AIP type 1 represents the pancreatic manifestation of IgG4-related disease (IgG4-RD) and is histologically characterized by dense lymphoplasmacytic inflammation with more than ten IgG4-positive plasma cells per high-power field, together with storiform fibrosis and obliterative venulitis. Systemically, IgG4-RD is a fibroinflammatory disorder capable of affecting nearly any organ. 9 Recognized manifestations encompass AIP type 1, retroperitoneal fibrosis, chronic periaortitis, autoimmune hypophysitis, sclerosing cholangitis, Riedel’s thyroiditis, and Mikulicz disease. 9 AIP type 2, by contrast, is confined to the pancreas and does not represent a systemic condition. Its hallmark pathologic finding is the presence of granulocytic epithelial lesions (GELs), affecting the epithelium of medium- and small-caliber ducts as well as the acinar tissue. AIP type 2 has also been reported in association with inflammatory bowel disease. 10
Establishing a diagnosis of AIP is inherently challenging, as malignancy must first be excluded. The diagnostic workup integrates imaging, serologic, and histopathologic data. 11 Characteristic imaging features of AIP include parenchymal enlargement with a “sausage-shaped” morphology, a peripancreatic edematous halo, and narrowing of the main pancreatic duct without upstream dilatation. 12 A Japanese epidemiological analysis found that approximately half of AIP cases demonstrated focal or segmental pancreatic enlargement on CT, with focal involvement defined as affecting less than one-third of the gland and segmental involvement encompassing more than one-third but less than two-thirds. 13
Per the International Consensus Diagnostic Criteria (ICDC), at least one of five cardinal diagnostic features must be present to confirm a diagnosis of AIP. These encompass pancreatic parenchymal and ductal morphology assessed by CT/MRI and ERCP/MRCP, serologic findings (IgG4, IgG, and antinuclear antibody), extrapancreatic organ involvement, pancreatic histopathology, and therapeutic response to corticosteroids. 14
Atypical imaging features — including hypodense masses, pancreatic ductal dilatation or irregularity, cysts, strictures, or multi-organ involvement — may occasionally be encountered. When present, particularly in the setting of obstructive jaundice and/or a pancreatic mass, these findings raise significant concern for malignancy. Accordingly, a thorough evaluation to exclude pancreatic cancer should be undertaken before such findings are attributed to AIP. 14
Two distinct diagnostic frameworks currently exist for differentiating AIP from pancreatic malignancy. The Japanese approach combines serum IgG4 measurement with cross-sectional pancreatic imaging and ERCP. On CT, the triad of a peripheral hypoattenuating capsule-like rim, delayed parenchymal enhancement, and atrophy of the body and tail supports an AIP diagnosis. ERCP may reveal mildly irregular narrowing of the main pancreatic duct — typically without upstream dilatation — along with involvement of secondary ductal branches. 15
A Taiwanese investigation by Chang et al. examined the combined use of serum CA 19-9 and IgG4 levels to distinguish AIP from pancreatic cancer. Their data showed that an IgG4 concentration exceeding twice the upper limit of normal, paired with a CA 19-9 below 85 U/mL, constitutes a diagnostically useful profile favoring focal AIP over pancreatic malignancy. 16
When the initial malignancy workup is unrevealing, EUS-guided pancreatic core biopsy may provide additional diagnostic clarity. Characteristic EUS findings in AIP include the absence of a discrete mass, hypoechoic foci, and inflammatory cellular infiltrates on cytology — though none of these is pathognomonic. 17 The International Association of Pancreatology criteria emphasize that a diagnosis of AIP should be rendered only after all reasonable efforts to exclude malignancy have been completed, given the potentially fatal consequences of a missed cancer diagnosis. 17 Given the variability and non-specific nature of EUS findings in AIP, adjunctive modalities such as EUS elastography and contrast-enhanced EUS have been investigated as potential tools to improve diagnostic accuracy. 18
Treatment of AIP is warranted in symptomatic patients with pancreatic or extrapancreatic involvement, as well as in asymptomatic patients with a persistent pancreatic mass on imaging or elevated liver enzymes in the context of IgG4-associated sclerosing cholangitis. First-line therapy consists of corticosteroid administration; when steroids are contraindicated, rituximab is the preferred alternative. 19 Corticosteroids have achieved consistently high remission rates across both Japanese national and international multicenter studies. In the Japanese series, 98% of steroid-treated patients achieved remission compared with 88% in the untreated cohort. The international multicenter study reported comparable outcomes, with remission rates of 99.6% in AIP type 1 and 92.3% in AIP type 2. 19
Despite high remission rates, disease relapse following steroid therapy can occur in 15–60% of patients. 20 Risk factors for relapse include persistently elevated IgG4 levels following treatment and diffuse pancreatic enlargement or concurrent involvement of other organ systems. 21 A review of the published literature found that 27% of patients required pancreatic core biopsy, an empiric steroid trial, or surgical intervention to definitively distinguish AIP from pancreatic cancer. 22
Conclusion
AIP is an uncommon condition whose complications and sequelae make timely recognition clinically important. Nevertheless, the exclusion of malignancy remains paramount before this diagnosis can be established. The clinical and radiologic parallels between AIP and pancreatic cancer underscore the inherent diagnostic complexity. Clinicians must pursue a systematic and thorough workup to evaluate and rule out malignancy prior to attributing findings to AIP. A delayed or missed diagnosis of pancreatic cancer carries grave prognostic consequences. Therefore, malignancy must be actively considered and excluded before ascribing clinical and imaging findings to an autoimmune etiology. We hope these cases reinforce the necessity of a comprehensive diagnostic evaluation to reliably differentiate AIP from pancreatic adenocarcinoma, thereby facilitating timely and appropriate management.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Prior Presentation
The above manuscript was presented as an abstract at American College of Gastroenterology meeting at Vancouver in 2023 – Lee, Brian, Swati Mahapatra, Jesus Guzman, Ioannis Konstantinidis, Vital Rangashamanna, Nawar Hakim, and Sherif E. Elhanafi. “S2129 The Great Mimicker: A Case Series of Autoimmune Pancreatitis Initially Presenting as a Pancreatic Mass Concerning for Malignancy.” Official journal of the American College of Gastroenterology | ACG 118, no. 10S (2023): S1541.