
Abstract
Peritoneal tuberculosis (PT) is a rare form of extrapulmonary Mycobacterium tuberculosis infection that may closely mimic Crohn’s disease (CD) or intra-abdominal malignancy, leading to diagnostic delay, particularly in endemic areas. We report two illustrative cases complicated by localized abscess formation. The first case involved a 40-year-old woman presenting with chronic right lumbar pain. Computed tomography (CT) revealed a large right psoas abscess associated with circumferential thickening of the cecal base and terminal ileum, along with necrotic mesenteric and iliac lymphadenopathy. Colonoscopy showed ulcerative ileocolitis, and histology demonstrated chronic granulomatous inflammation suggestive of either tuberculosis or CD. CT-guided biopsy of the abscess wall was performed, and polymerase chain reaction testing for Mycobacterium tuberculosis was positive. Histopathology examination was consistent with tuberculosis. The patient responded well to anti-tuberculous therapy with complete radiological resolution. The second case concerned a 17-year-old male admitted with right iliac fossa pain, fever, weight loss, and night sweats. CT showed a right pelvic collection adjacent to the ileocecal junction with distal ileal and cecal thickening, initially suggesting CD. Colonoscopy revealed ulcerative ileitis with granulomatous inflammation. As radiological drainage was not feasible, laparoscopy was performed and showed a friable micronodular peritoneum with terminal ileitis. Peritoneal biopsies demonstrated non caseating granulomatous inflammation, consistent with peritoneal and ileocecal tuberculosis. These cases highlight that PT may present as localized abdominal or psoas abscesses and closely mimics CD. Early integration of imaging, endoscopy, tissue sampling, and microbiological or molecular testing is essential for prompt diagnosis and appropriate curative treatment.
Introduction
Peritoneal tuberculosis (PT) is a rare form of extrapulmonary Mycobacterium tuberculosis (MTB) infection characterized by an insidious onset and nonspecific clinical features. Its presentation often mimics other abdominal conditions, such as malignancies or inflammatory bowel disease, frequently leading to delayed diagnosis and treatment.1,2 The insidious onset, nonspecific symptoms such as abdominal pain, distension, fever, or weight loss, and the absence of pathognomonic signs contribute to frequent misdiagnosis particularly in regions where the disease remains endemic. 3 This diagnostic challenge is further compounded when PT is accompanied by the development of abdominal abscesses, an uncommon complication of PT, which introduces substantial diagnostic and therapeutic complexities. In regions where tuberculosis remains endemic, maintaining a high index of suspicion for PT, especially in the context of atypical abdominal presentations, is crucial. This report presents two illustrative cases of PT complicated by localized abscesses, highlighting the importance of clinical vigilance and multidisciplinary management in endemic regions.
Clinical Cases
Case1
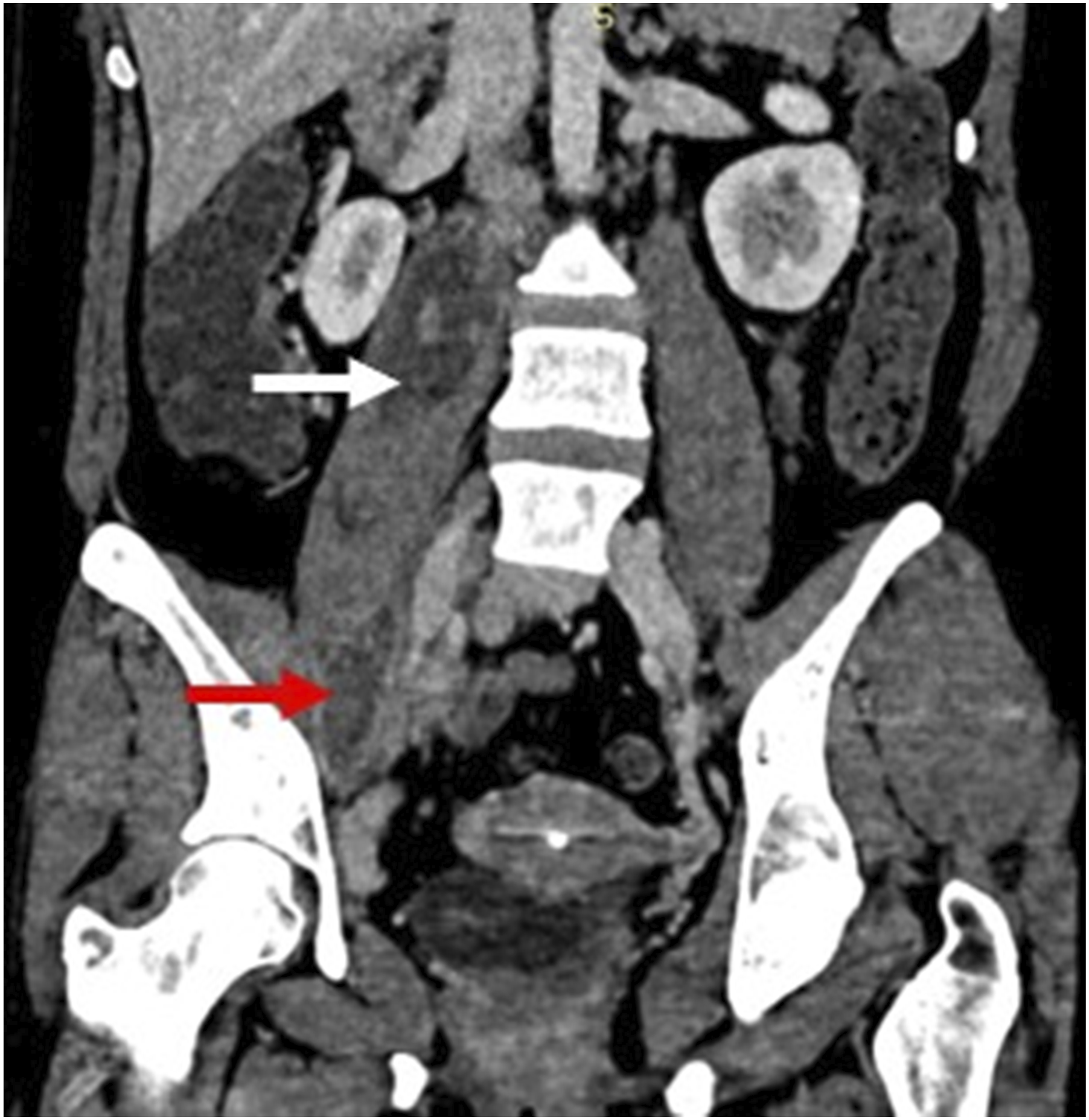
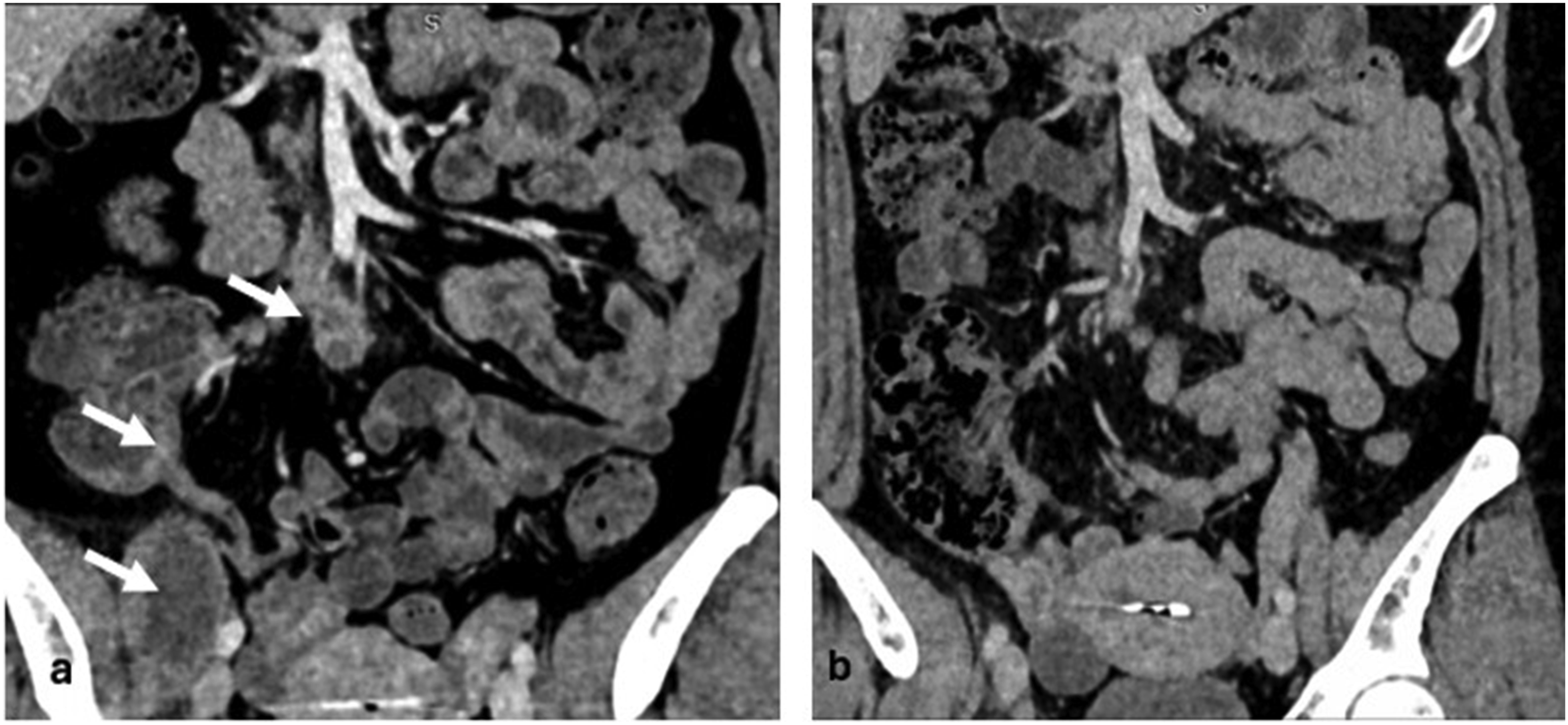
A 40-year-old women presented with right lumbar pain evolving over two months, without fever or deterioration in general health. Physical examination revealed tenderness in the right flank. Laboratory tests showed hypochromic microcytic anemia (hemoglobin 10 g/dL), a white blood cell count of 7,800/mm3, and a C-reactive protein (CRP) level of 25 mg/L. Other laboratory tests were normal. Abdominopelvic computed tomography (CT) revealed a large hypodense collection with thick, enhancing walls within a swollen right psoas muscle, communicating with an adjacent pelvic collection. There was also a circumferential mural thickening of the cecal base and terminal ileum with regular, homogeneously enhancing walls and preserved mural stratification, producing a “pulled-up cecum” appearance (Figures 1 and 2). Multiple enlarged mesenteric and right iliac lymph nodes were identified, displaying heterogeneous enhancement with central low attenuation consistent with caseating necrosis. The QuantiFERON test was negative. Colonoscopy showed ulcerations of the cecum and terminal ileum. Histopathological examination of biopsies revealed active chronic granulomatous ileocolitis suggestive of tuberculosis or Crohn’s disease (CD). Polymerase chain reaction (PCR) for MTB was negative. CT-guided biopsy of the psoas abscess wall was performed. PCR testing for MTB on the abscess specimen was positive. Histopathological examination showed granulomatous inflammatory remodeling of the muscle tissue, consistent with tuberculosis. In this setting, the presence of necrotic lymph nodes on CT, the positive MTB PCR from the abscess wall and the granulomatous inflammation on biopsy favored tuberculosis over CD. Spinal imaging showed no evidence of vertebral tuberculosis, discitis, or osteomyelitis. Diagnosis of digestive, peritoneal, and soft tissue tuberculosis was retained. Radiological drainage of the abscess was unsuccessful and did not yield any aspirated material. The patient was initiated on a four-drug antituberculous regimen (isoniazid, rifampicin, pyrazinamide, and ethambutol) for the first two months, followed by a continuation phase with isoniazid and rifampicin. A follow-up CT scan after two months showed resolution of the iliopsoas abscess, regression of the necrotic right iliac lymphadenopathy, and normalization of the mural thickening of the cecal base consistent with a favorable therapeutic response (Figure 3). Coronal abdominopelvic CT image showing smooth, circumferential mural thickening and enhancement of the appendix and cecal base (white arrow), associated with mesenteric lymphadenopathy demonstrating heterogeneous enhancement with central necrosis (red arrow), and a collection involving the iliopsoas muscle at the level of the iliac crest (blue arrow) Axial abdominopelvic CT image showing a large hypodense collection with thick, enhancing walls within the enlarged right psoas muscle (white arrow), communicating with an adjacent pelvic collection (red arrow) Coronal abdominopelvic CT images before and after antituberculous therapy. The pre-treatment image (A) shows right iliopsoas abscesses and necrotic right iliac lymphadenopathy, associated with cecal wall thickening (white arrows). The post-treatment image (B) shows complete resolution of the abscesses and regression of both the lymphadenopathy and cecal thickening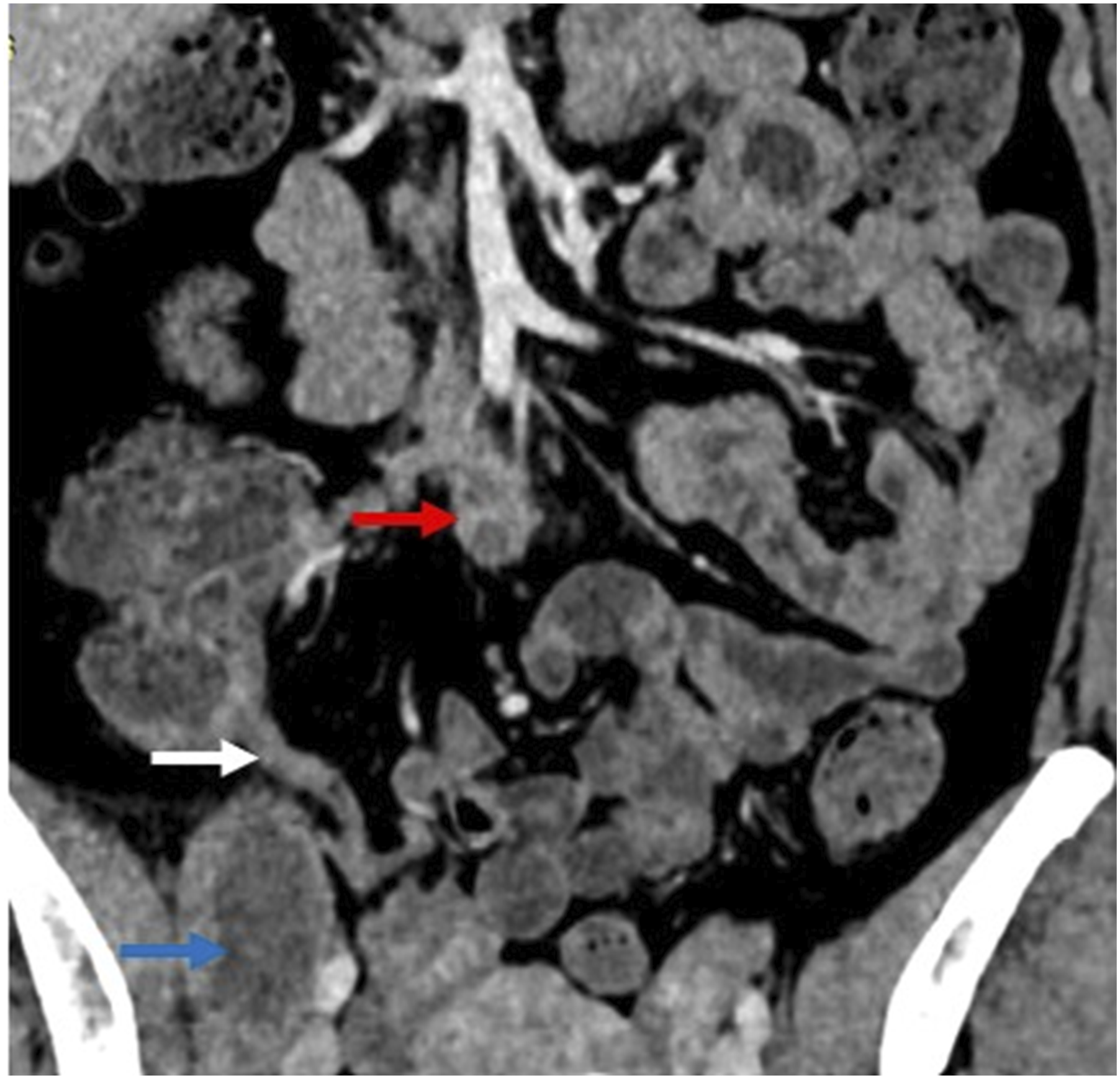
Case2
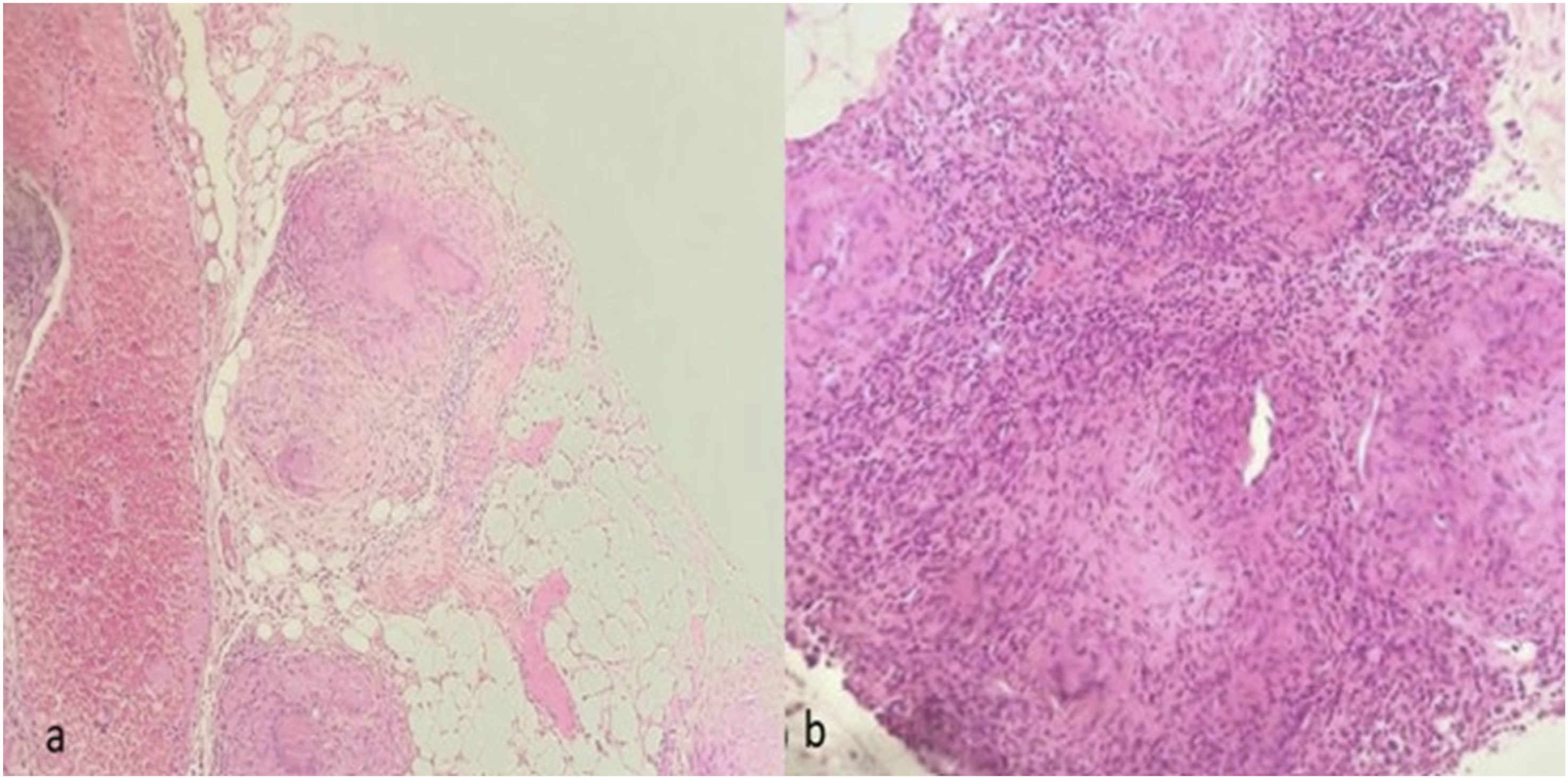
A 17-year-old male was admitted for abdominal pain localized in the right iliac fossa evolving over two weeks. He reported unintentional weight loss of 5 kg, fever, night sweats, and asthenia. Physical examination revealed diffuse tenderness, more pronounced in the right lower quadrant. Laboratory tests showed a hemoglobin of 11.8 g/dL and elevated CRP at 30.89 mg/L. The white blood cell count, liver enzymes, and renal function were within the normal range. Abdominopelvic CT showed a right pelvic fluid–air collection with a well-defined, enhancing wall in close contact with the ileocecal junction. Associated findings included regular, homogeneously enhancing mural thickening of the distal ileal loop and cecal base, suggesting an initial diagnosis of CD (Figure 4). Intravenous antibiotic therapy was initiated. The control scan performed at three weeks of follow-up revealed persistence of the collection. Colonoscopy revealed erythematous and ulcerative ileitis. Ileal biopsies were consistent with subacute granulomatous inflammatory ileitis which may suggest a tuberculous origin or CD. The QuantiFERON test was positive. Radiological drainage was considered but was not feasible due to the inaccessibility of the abscess. Diagnostic and therapeutic laparoscopy was performed and revealed a friable peritoneum coated with multiple whitish granulations of similar age and terminal ileitis. Histopathological examination of peritoneal samples demonstrated non caseating granulomatous inflammation with multinucleated giant cells. The granulomas were of epithelioid and multinucleated giant cells (Figure 5). Based on these findings, a diagnosis of peritoneal and ileocecal tuberculosis was made. Active pulmonary tuberculosis was excluded. The patient was started on standard antituberculous therapy, with progressive clinical improvement on follow-up. Axial portal venous–phase CT image showing a right pelvic fluid–air collection (arrowhead) with an enhancing anterior wall abutting the ileocecal junction, associated with regular enhancing mural thickening of the distal ileal loop (arrow) a: hematoxylin and eosin (HE) x 100: Non caseating granulomatous inflammation with multinucleated giant cells. b: HE X 200: The granulomas are of epithelioid and multinucleated giant cells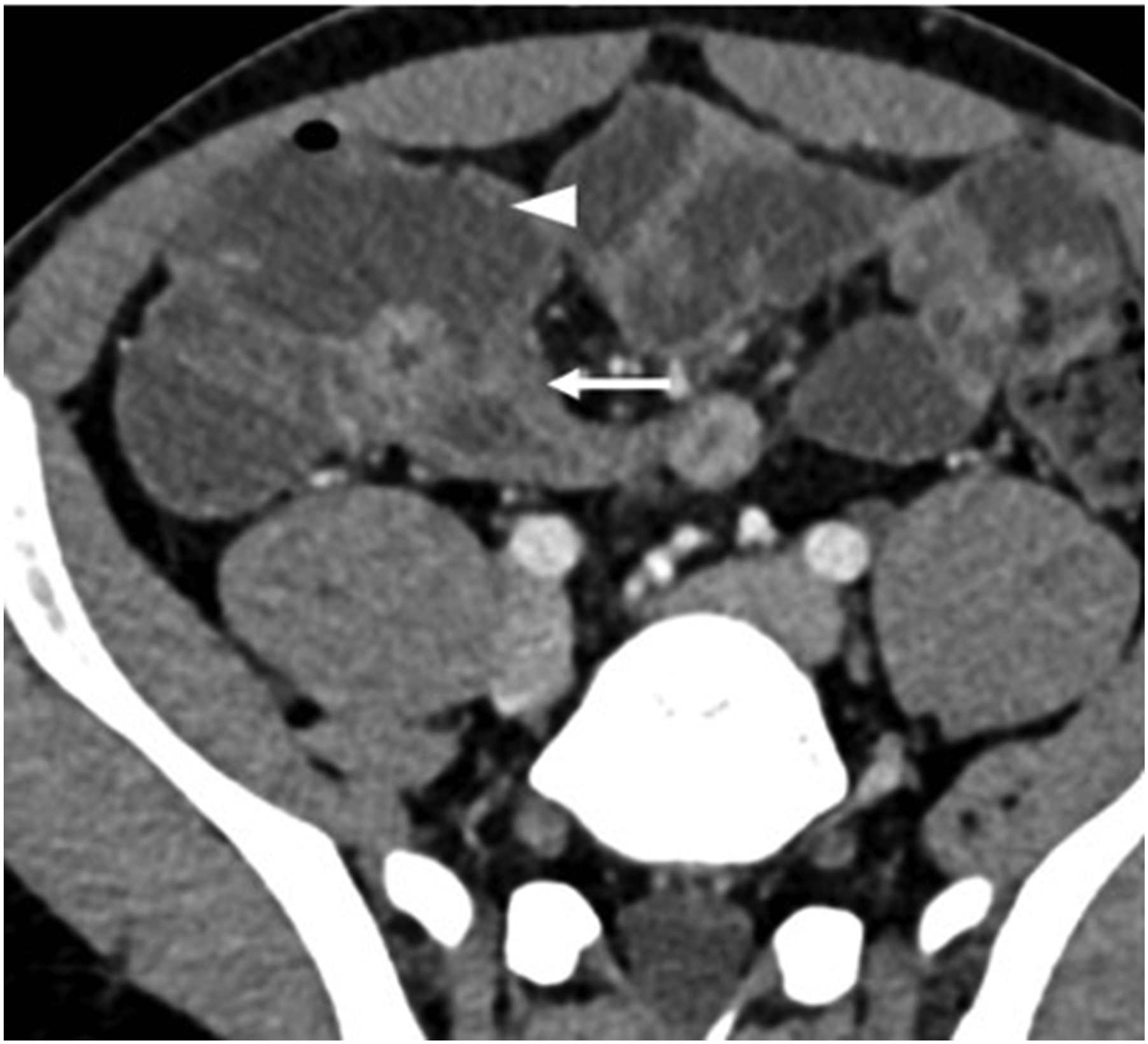
Discussion
Tuberculosis, caused by MTB, remains a significant global health burden, with an estimated 10.8 million new cases and 1.6 million deaths reported worldwide in 2023. 4 Although pulmonary TB accounts for most infections, extrapulmonary tuberculosis represents approximately 15-20% of all cases and presents diverse clinical manifestations depending on the anatomical site involved. Among these, peritoneal tuberculosis (PT) is a rare localization characterized by an insidious onset and nonspecific clinical and radiological features, making its diagnosis challenging. 3
The pathogenesis of PT generally involves hematogenous dissemination, lymphatic spread, or direct extension from adjacent infected organs such as the intestines or genitourinary tract. Beyond routes of spread, immunopathogenesis plays an important role: in many forms of extrapulmonary TB, including peritoneal disease, a marked granulomatous inflammatory response may occur despite a low mycobacterial burden, which contributes to diagnostic difficulty and overlap with inflammatory bowel disease.3,5 Clinically, patients often present with nonspecific symptoms including abdominal pain, weight loss, fever, and ascites.6,7 Complicated forms such as tuberculous abscesses, though uncommon, have been reported. These can occur via contamination from the intestines or genital tract or following rupture of an infected lymph node. 8 These abscesses may form within the peritoneal cavity or involve adjacent structures such as the psoas muscle and iliac fossa, as seen in our cases.
The first case highlights a tuberculous psoas abscess, a rare complication of peritoneal and soft tissue tuberculosis. Psoas abscesses are often categorized as primary, stemming from hematogenous spread, or secondary, resulting from contiguous spread from adjacent infections including spinal tuberculosis (Pott’s disease) or abdominal tuberculosis.9-11 Tuberculous psoas abscesses are known for their insidious progression and nonspecific presentation, with symptoms ranging from localized pain to systemic features such as fever. Imaging, especially contrast-enhanced CT, is essential to identify abscess size, anatomical extent, and to guide percutaneous drainage. 9 Etiological confirmation of tuberculosis is established either by direct demonstration of MTB in pathological specimens or by histological identification of epithelioid-giant cell granulomas with caseating necrosis on biopsy samples. Molecular diagnostic techniques such as nucleic acid amplification tests and immunological assays like the QuantiFERON®-TB Gold In-Tube test can be helpful for early and rapid diagnosis. 12 In addition to antituberculous therapy, drainage of suppurative abscess collections is usually indicated and can be performed either surgically or under image guidance. Percutaneous drainage is preferred for uniloculated and multiloculated abscesses with few septations, as observed in our patient. Indications for open surgical drainage include failure of percutaneous drainage, inability to identify the causative pathogen, and the presence of concomitant intra-abdominal or retroperitoneal pathology requiring surgical intervention.13,14
The second case underscores the diagnostic complexity of ileal and peritoneal tuberculosis mimicking inflammatory bowel disease, particularly Crohn’s disease (CD). The overlap in clinical symptoms, endoscopic findings of ulcerations, and radiological features such as bowel wall thickening lead to significant diagnostic dilemmas. 2 Distinguishing intestinal tuberculosis from CD relies heavily on histopathological examination, with granulomas exhibiting caseous necrosis being pathognomonic for tuberculosis. 15 Additionally, diagnostic laparoscopy and biopsy of peritoneal nodules remain the gold standard for definitive diagnosis in unclear cases, as it allows direct visualization and targeted sampling. Macroscopic findings include white regular granules of equivalent sizes (1 to 3 mm), hyperemia of the peritoneum, numerous dispersed and friable nodules at biopsy as our case, filamentous peritoneal adhesions, as well as clumping of bowel loops with fibrin deposition. 16
This diagnostic overlap has been described for decades in the classic literature on intestinal TB mimicking inflammatory bowel disease.17-19
Misdiagnosis as Crohn’s disease has important consequences. Initiating corticosteroids or biologic therapy in unrecognized tuberculosis may lead to clinical deterioration, dissemination, and delayed microbiological confirmation. This risk reinforces the need for microbiological or molecular testing whenever possible before starting immunosuppression in patients with suspected inflammatory bowel disease in endemic settings. 20
Management of peritoneal tuberculosis complicated by abscesses is based on prolonged multidrug antituberculous therapy consisting of an initial phase with isoniazid, rifampicin, pyrazinamide, and ethambutol for two months, followed by a continuation phase with isoniazid and rifampicin for four months according to the World Health Organization’s for the National Tuberculosis programme guidelines. 21 While most cases respond well to medical therapy alone, surgical intervention or percutaneous drainage is warranted in cases presenting with large abscesses, intestinal obstruction, or other significant complications. 22 A multidisciplinary approach integrating infectious disease specialists, radiologists, gastroenterologists, and surgeons is recommended to optimize patient outcomes.
Our cases illustrate a well-recognized diagnostic challenge: abdominal and PT can closely mimic CD, and abscess formation may further obscure the diagnosis. Early recognition supported by imaging, targeted sampling, and microbiological or molecular testing is critical to initiate appropriate therapy and to avoid inappropriate immunosuppression. These cases serve as a practical reminder to maintain clinical vigilance in endemic regions or in at-risk populations.
Conclusion
These cases underscore the diagnostic complexities posed by PT with abscess formation, particularly in atypical locations such as the psoas muscle and iliac fossa. Timely identification through a combination of modern imaging, invasive sampling techniques, and molecular diagnostics enables effective treatment and recovery. Awareness of such presentations is critical for clinicians managing abdominal masses or collections in regions with a high tuberculosis prevalence or in patients at risk.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI in Scientific Writing
Generative AI (chat GPT) was used for the correction of spelling mistakes of the final version of the manuscript.