
Abstract


Throughout the Veterans Health Administration (VHA), registered nurses in the outpatient setting are the clinicians who work most closely with veterans with diabetes. The VHA deals with an especially high burden of type 2 diabetes. Approximately 25% of the nation’s 8.92 million veterans are diagnosed with this form of the disease. The increased incidence of type 2 diabetes—relative to the US population at large—reflects in part the fact that over 70% of veterans are classified as overweight or obese, and 44% are aged 65 or older. VHA nurses deliver diabetes care—diabetes self-management education (DSME), case management, and care coordination—in individual appointments and group classes conducted face-to-face, virtually, and by telephone.
Though nursing care delivery via the usual modes is often effective in improving the clinical outcomes for patients with diabetes, it is not always so. Such was the case at our Southern Arizona VHA Community Based Outpatient Clinic (CBOC) in Northwest Tucson where we found that in spite of our best efforts, there were insulin-treated patients with type 2 diabetes who were not achieving their A1C goals in response to individualized nursing case management. In hopes of engaging these patients, we decided to trial a group appointment for diabetes case management. This is a recurring monthly appointment offering DSME and medication management, with peer support and feedback during the appointment. This appointment was named the Shared Nursing Appointment (SNA) for diabetes case management and was implemented initially as a quality improvement (QI) project in 2010.
The VHA deals with an especially high burden of type 2 diabetes. Approximately 25% of the nation’s 8.92 million veterans are diagnosed with this form of the disease.
In the same year we implemented the SNA, the VHA inaugurated its version of the patient-centered medical home (PCMH) branded the Patient Aligned Care Team (PACT) initiative. The goal of PACT is to achieve team-based care, improved access, and effective care management for veterans nationwide. To meet these goals, primary care staff were reorganized into PACT teams consisting of a primary care provider (PCP, MD or NP), RN care manager, clinical associate, and clerk and assigned to a panel of approximately 1200 patients. Ancillary staff available to support PACT teams includes a clinical pharmacist, social worker, dietitian, and behavioral health clinicians. Additionally, there is a sophisticated technological network that includes an integrated computerized patient record system (CPRS) from which multiple tools can be accessed, including the Primary Care Almanac, containing a disease registry, and the PACT Compass, containing quality care measures on access, admission, and continuity of care. Central to PACT is the idea that staff should work to the top of their expertise and that in doing so they will be better able to improve clinical outcomes, such as glycemic control for patients with diabetes.
Throughout the SNA, the RN CDE promotes peer support and critical thinking by encouraging patients to share their stories, insights, and concerns and soliciting input from patients to troubleshoot problems encountered by group members.
The Shared Nursing Appointment
We conceived of the SNA for diabetes case management as a mode of care delivery that would be cost-effective, successful in improving clinical outcomes, valuable to patients, and allow for increased access to the RN CDE. Initially, the target population included only patients already known by the RN CDE with A1Cs above 8%. Over time, it has come to include patients identified via the PC Almanac as having A1Cs above 9%, as well as patients whose A1Cs were at goal but who were referred to the group by PACT PCPs for help with some other aspect of diabetes care.
The monthly SNA aims to improve clinical outcomes such as A1C; provide ongoing DSME; promote lifestyle change resulting in increased physical activity, improved nutrition, and weight loss; coordinate care between the patient and PCP to optimize treatment of lipids and blood pressure; and put patient concerns at the forefront in a clinical setting that is therapeutic and supportive. Patients are encouraged to attend as long as they deem the SNA beneficial. The number of patients at the SNA varies, but the goal is 4 patients per session. Group cohesion is fostered by keeping the same individuals together over time. Patients attending the SNA verbally consent to participate in a shared appointment with other patients but no family members and to protect the privacy of the individuals attending the appointment. The RN CDE facilitates all the SNAs and works to foster therapeutic alliances with and between the patients.
In preparation for the SNA, the RN CDE initiates a form for each patient (Figure 1). On this form, the RN CDE records data collected at the patient’s last SNA, including weight, blood pressure, and pulse; glucose-lowering medication and dosing; and physical activity regimen. In addition, recent lab values are recorded, and any actions that need to be taken (eg, update A1C) are noted. At check-in, the RN CDE weighs each patient, measures their blood pressure and pulse, and records the new data on the form. During the appointment, each patient updates their form by recording their most recent blood glucose readings, noting any changes since the last SNA to their medication dosing for both insulin and oral anti-hyperglycemic agents. Additionally, they update their physical activity regimen, calculate weight loss/gain, and list any concerns to be discussed at the SNA or to be communicated afterward to the PCP. To complete the form, the RN CDE addresses the treatment plan for each patient and adds any changes to the plan of care. These changes include, for example, revision of physical activity goals and adjustment of insulin dosing according to the nurse managed protocol in use at our facility.
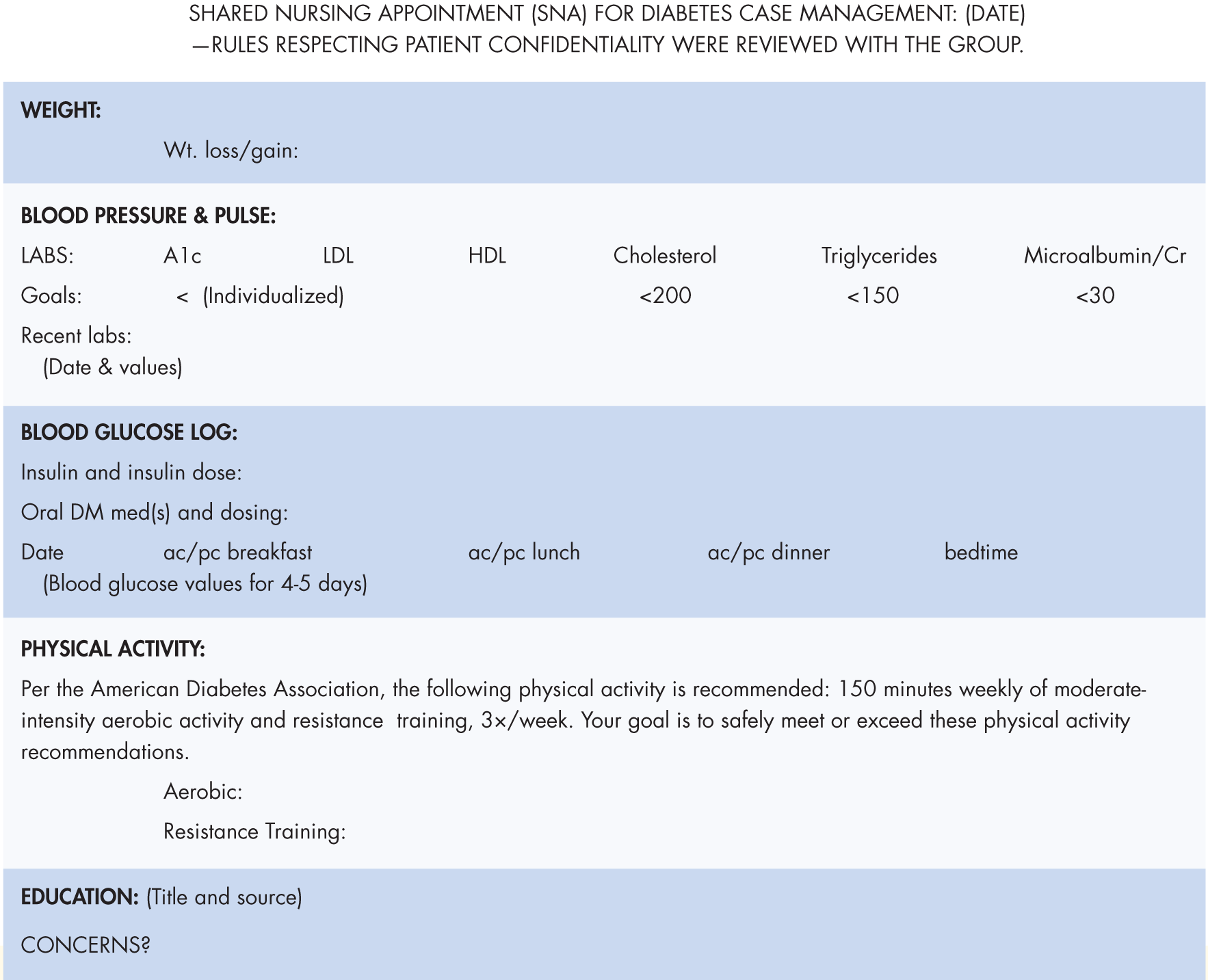
Patient record completed by the RN CDE and patient at the SNA.
Throughout the SNA, the RN CDE promotes peer support and critical thinking by encouraging patients to share their stories, insights, and concerns and soliciting input from patients to troubleshoot problems encountered by group members. In addition to what patients learn from sharing, there is also “formal” DSME featuring, for example, the discussion of brief articles on elements of the AADE7 Self-Care Behaviors™ as well as the use of AADE’s Diabetes Education and Diabetes Complications Prompt Decks. At the end of the SNA, the RN CDE makes a copy of the form and returns it to each patient. When charting, the RN CDE refers to the form to document the SNA in detail in CPRS. Finally, the CPRS note is always sent to the PCP for a co-signature and input on the plan of care.
Results
As mentioned, the SNA was implemented initially as a QI project in 2010. Data collected included information recorded on the patient form and was maintained in an Excel spreadsheet for future analysis. After 6 months of data were analyzed, and for those patients attending 3 or more SNAs during this time, outcomes were presented (Figure 2). Twenty patients attended at least 1 appointment, and 9 patients attended from 3 to 6 SNAs (average of 5 SNAs/patient). Patient feedback was positive, noting that the SNA “keeps me honest,” makes for “easy learning,” and is helpful because of the “support and sharing” through both RN CDE and peer feedback. At the commencement of the SNA, two-thirds of the patients were performing some routine physical activity. By the time the QI data were analyzed, all 9 patients were engaged in physical activity.
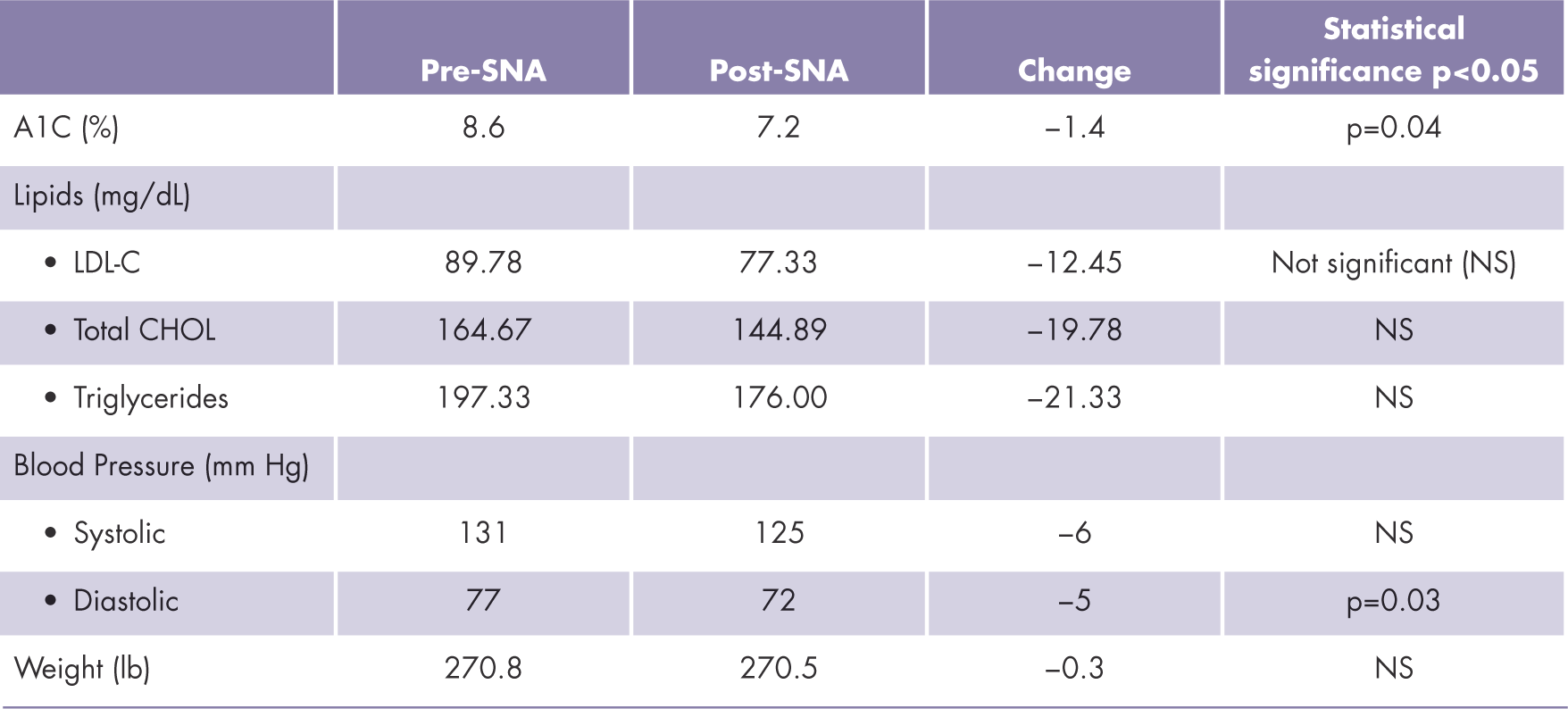
Pre- and Post-QI Project SNA Outcomes. Mean values for 9 patients who attended an average of 5 appointments (range: 3-6) during the first 6 months of the SNA.
Given the improvement in clinical outcomes and positive patient feedback, we made the decision to continue to offer the SNA as an alternative to the usual, individualized nursing case management for insulin-treated patients with type 2 diabetes. We have shared the results of our QI project in poster presentations with the parent facility and the other facilities in our Veterans Integrated Service Network (VISN), and we continue to collect data for further analysis.
Shared Medical Appointments Versus Shared Nursing Appointments
In the national discussion of “group appointments” for diabetes care, it is the shared medical appointment (SMA), not an SNA, that is cited as an example of care delivery capable of improving patient outcomes, increasing access, and reducing costs. In an SMA, groups of patients—typically from 8 to 20—are seen over time by a multidisciplinary team in a 1- to 2-hour appointment to address aspects, including the ABCs—A1C, blood pressure (BP), and cholesterol—of diabetes management. Patients meet with educators for DSME and practitioners with prescribing privileges for medication management.
A recent systematic review on SMAs for chronic medical conditions included 19 studies—16 of which specifically addressed patients with diabetes, including 13 randomized controlled trials (RCTs)—conducted in “non–real-world” settings such as vertically integrated systems like the VHA, as well as in academic and other government settings. 2 The visit frequency for diabetes SMAs was from every 3 weeks to every 3 months. Outcomes were assessed at the end of the SMA intervention, anywhere from 4 to 48 months later. The review found that patients with diabetes attending SMAs experienced improvements in intermediate clinical outcomes, namely, statistically significant improvements in A1C and systolic blood pressure and a modest but statistically insignificant reduction in LDL-C (Figure 3).

Reported Effects on Intermediate Outcomes of Two Modes of Outpatient Care Delivery for Adults with Chronic Conditions: The Shared Medical Appointment (SMA) and Nurse-Managed Protocols (NMP)
Though SMAs for persons with diabetes are promising, they are not yet prevalent in the VHA. For the majority of veterans, PCPs continue to address the routine follow-up care in 1:1 face-to-face and phone appointments. PACT RNs provide, at a minimum, DSME and glycemic management. RNs usually teach DMSE in a group setting. They typically provide glycemic management using approved insulin titration protocols via individualized counseling in either face-to-face visits or via phone appointments or secure email messaging.

Support for the Shared Nursing Appointment
Unlike the SMA, there are no published studies of what we call an SNA, per se. However, there have been 2 recent studies addressing the effectiveness of 2 components of the SNA—namely, nursing case management of chronic disease and DSME in a group setting.
In the systematic review and meta-analysis, “Effects of Nurse-Managed Protocols in the Outpatient Management of Adults With Chronic Conditions,” the authors sought to determine if RNs could effectively lead the management of chronic disease in an outpatient setting where, due to a shortage of primary care physicians and an increase in the demand for health care, new models for managing chronic diseases are needed. 3 Of the 18 studies included in the analysis, 15 were done on patients with diabetes, of which 10 were RCTs. The nurse-managed protocol (NMP) interventions were delivered in the clinic and by phone over a period of 6 to 36 months. The analysis concluded that RNs using physician-designed NMPs to adjust medications for diabetes, hypertension, and hyperlipidemia achieved a “consistently positive effect on chronically ill patients.” Compared to patients receiving the usual care, patients receiving the NMP intervention experienced decreases in intermediate outcomes including A1C, systolic and diastolic blood pressures, and total cholesterol and LDL-C levels (Figure 3). As the management of these conditions is relatively straightforward, the implication is that RNs are capable of an expanded role in which they can increase the reach and effectiveness of chronic care management.
In the study “Diabetes Education Through Group Classes Leads to Better Care and Outcomes Than Individual Counselling in Adults: A Population-Based Cohort Study,” which was conducted in “real-world” settings on the education of adults with diabetes (predominantly type 2) by nurses and dietitians, the authors determined that DSME taught in a group setting was superior to that obtained via individualized counseling. 4 Patients who received group education, typically in class sizes of 5 to 10 patients plus family members, were less likely to visit the emergency department or be hospitalized for treatment of hypoglycemia, hyperglycemia, foot ulcers, or cellulitis. 5 Such patients were also more likely to be prescribed statins and obtain timelier testing of A1C and lipids. In summary, the study concluded that DSME in a group setting was more resource efficient and productive of better patient outcomes and processes of care than individualized counseling.

The SNA for diabetes case management employs both group DSME and NMP in a group setting to provide an alternative mode of care delivery to insulin-treated patients with type 2 diabetes. It offers patients ongoing support and guidance from peers and the RN diabetes educator to sustain efforts required over time to achieve often difficult goals, such as weight loss or establishment of routine physical activity. The SNA offers patients routine follow-up with their nurse case manager, an element of chronic care management that is especially important for high-risk, vulnerable patients. Elderly patients with type 2 diabetes who use insulin or secretagogues, for example, are at higher risk for hypoglycemia and glycemic over treatment, which may result in emergency department visits and hospitalizations. A recent study suggests that the elderly often feel they are kept out of the decision loop in their own care, leading to feelings of marginalization. 6 As a patient-centered mode of care delivery providing monthly follow-up and facilitated communication with a patient’s PCP, the SNA could go far in safeguarding the elderly from harm, increasing their perception as being active and valued participants in their health care, mitigating social isolation, and curtailing the evolution of small problems into bigger ones.
Finally, the ease with which an SNA can be implemented in the VHA is appealing. Unlike an SMA, an SNA is not resource intensive. It does not require coordination of the schedules, time, and roles of multiple clinicians. It costs less for an RN to provide care than it does for a team of clinicians. Case management and education are 2 roles that fall squarely within the domain of the PACT RN. Veterans sharing the common bond of military service in addition to the diagnosis of type 2 diabetes may be more comfortable participating in an SNA. And in the VHA there is no financial obstacle to the implementation of an SNA as may exist in the community where fee-for-service prevails.
Conclusion
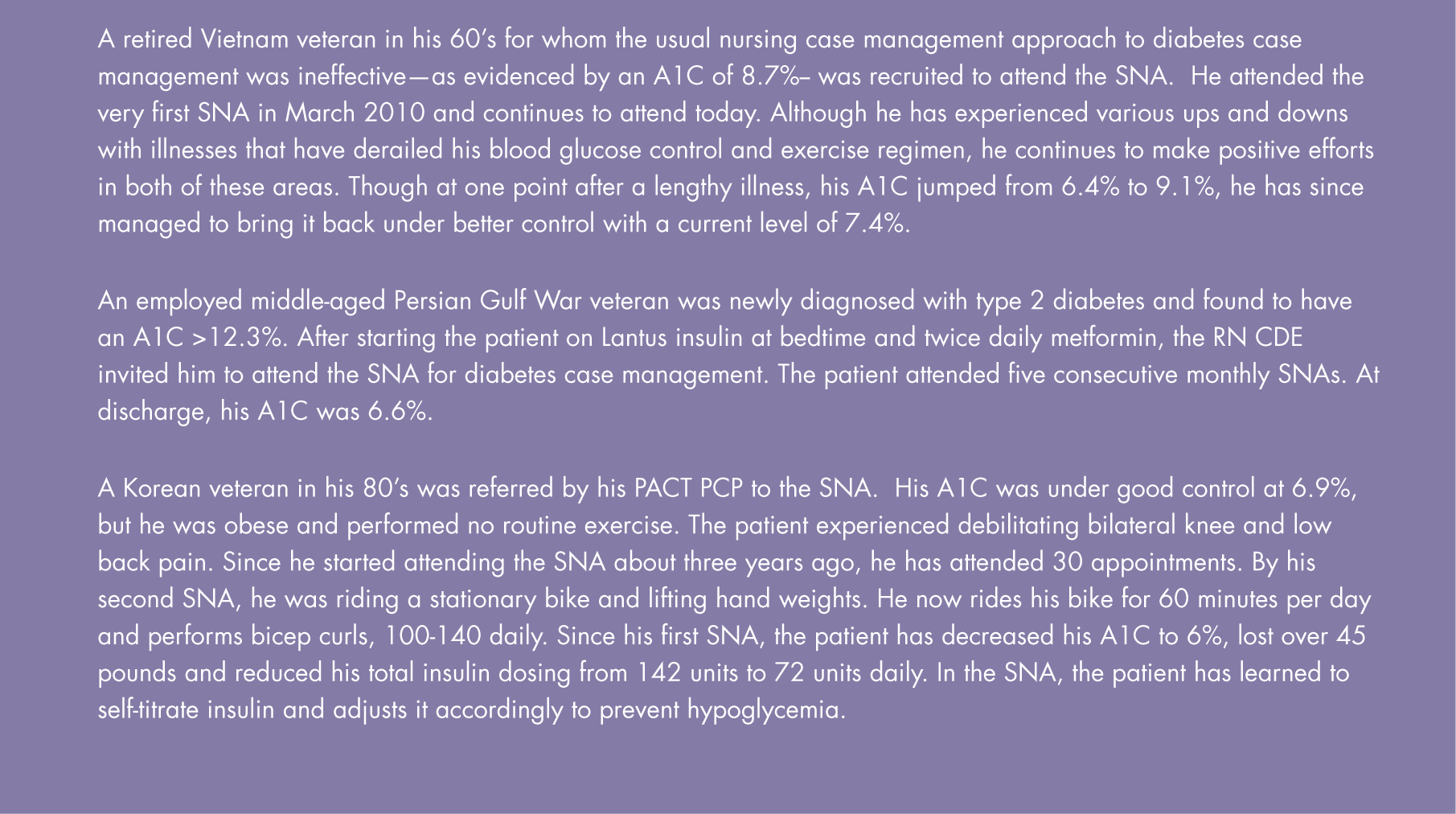
Initiated in 2010, the SNA at the NW CBOC is ongoing. There are patients who have been attending monthly since its inception (Figure 4), and because they find the SNA helps them to sustain the effort needed to successfully manage their chronic disease, they have no plans to stop. We have learned that the SNA meets a previously unmet need among our insulin-treated patients with type 2 diabetes. In spite of the success of the program and the enthusiasm of its attendees, there are challenges we face in recruiting patients for the SNA. At this time in our clinic, limited space inhibits expansion of the program, and this restriction necessarily limits the number of patients we can enroll in the SNA. The time it is offered is problematic for patients who work as well. Because of this, the patients who continue to attend the SNA monthly are those who no longer have to work due to retirement or disability. Extended hours would be helpful in recruiting working patients to the SNA. In addition, there are providers who do not yet understand that RNs can successfully implement NMPs to manage medications for not only glycemia but hypertension and lipids as well. Bridging this misunderstanding would allow more active participation by the RN to expand case management of diabetes care to also encompass that of hypertension and hyperlipidemia.
Clinical Vignettes
Changing the culture takes time. Clearly, the recent research demonstrating the value of NMPs will advance the case that RNs are capable of performing at a higher level. The research also suggests that given the burden of chronic disease such as diabetes on the health care system, it is a misuse of resources not to use NMPs more widely. The approach to chronic care management also needs to change. In spite of the understanding that episodic care fails to promote effective management of chronic disease, there is resistance to the SNA because the frequency of appointments is seen as excessive. However, lifestyle changes such as the development of routine physical activity regimens that lead to weight loss and improvement in clinical outcomes such as A1C are more difficult to sustain in programs that are limited to a few visits.

With the emergence of Accountable Care Organizations (ACOs) and bundled care payments, implementation of an SNA for diabetes case management may soon become more tenable in the community as well. The evidence shows that RNs can and should play a more decisive role in the delivery of chronic care management through implementation of NMPs and that the education they provide in a group setting is more effective than that provided via individualized counseling. In our experience at the NW CBOC in Tucson, the synthesis of group diabetes education with nurse case management employing NMP in the SNA has proven effective in engaging and improving the outcomes of insulin-treated patients with type 2 diabetes. ■
Footnotes
Anna Fletcher, BSN, BA, MS, RN, CDE, and Susan Lohse, BSN, BS, RCP, RN-BC, are diabetes educators with the Southern Arizona Veterans Health Care System, Northwest Community Based Outpatient Clinic, in Tucson, AZ.