
Abstract

The Centers for Disease Control and Prevention has estimated that there are 29.1 million people in the United States with diabetes. Not only is diabetes prevalent in the community but also in the correctional setting. According to the US Department of Justice, in 2011 and 2012, 9% of inmates reported having diabetes compared to 6.5% of people in the general population.
Historically, nurses and dietitians have provided diabetes education. As the benefits of diabetes self-management education (DSME) became more widespread and the educational needs of the diabetes population increased, more and more disciplines began providing DSME services. Pharmacists are now among the leading providers of DSME. They are highly skilled and trained to provide educational and medication management services to patients with diabetes.
In 2011 and 2012, 9% of inmates reported having diabetes compared to 6.5% of people in the general population.
There are many examples of pharmacists providing DSME services in federal agencies. For example, Tran, Rapp, and Zielinski describe how the Veteran’s Administration (VA) utilizes clinical pharmacy specialists to provide diabetes management services to patients upon referral from primary care providers. They report a 1.5% mean decrease in A1C from baseline for study participants. However, the literature is lacking for DSME in the federal correctional setting.
Introduction
The purpose of this article is to describe how the national DSME standards and the DSME standards for pharmacists were applied to enhance the performance and outcomes of an interdisciplinary diabetes clinic at the Federal Medical Center at Devens (FMC Devens), a prison hospital owned by the Federal Bureau of Prisons (BOP). A pharmacist at FMC Devens created the clinic in March 2012 after conducting a needs assessment and finding that there were several inmates with uncontrolled diabetes that could benefit from specialized care.
The national DSME standards are evidence-based and were created for diabetes educators by a task force of diabetes experts from the American Association of Diabetes Educators (AADE) and the American Diabetes Association (ADA). Both agencies published their version of the National DSME Standards. This article references both the AADE and ADA standards.
The National Standards for Diabetes Self-Management Education and Support were created in an effort to standardize diabetes education. They act as a rubric for educators to teach patients how to manage their diabetes in order to avert or delay the complications with which it is associated. There are 10 standards that provide guidance for a successful DSME program. Haas et al define these as internal structure, external input, access to diabetes education, instructional staff, program coordination, curriculum, individualization, ongoing support, patient progress, and quality improvement.
When inmates achieve two consecutive A1Cs less than 7.5%, they are discharged from the clinic.
Standard 1: Internal Structure
Standard 1 says that the success of a DSME program is dependent on the implementation of 3 key elements—a mission statement, organizational structure, and goals.
A clearly defined mission statement specifies the target population, describes what the program intends to achieve, explains the reason for the service, and ascertains if the service has been provided.
Standard 1 states that a DSME program should record its organizational structure and define the channels of communication involved. There is a consensus among health care and business professionals that this will enhance communication and lay the foundation for optimal diabetes education.
Goals provide a sense of direction for programs. Pollack explains that goals help an organization to see what needs to be done in order to accomplish the mission, and they help to measure success. A successful DSME program has goals that are feasible, relevant to the needs of the organization, have practical application, and can be easily maintained. Without goals, the program cannot effectively meet the needs of patients.
Prior to launching the DSME program at FMC Devens, the mission, organizational structure, and goals of the clinic were established. The mission of the DSME program at FMC Devens is to provide diabetes education and management services to help inmates achieve their diabetes goals.
The organizational structure of the program fosters communication between the local leaders at FMC Devens and the leaders at the central office of the BOP. Before the program could be implemented, it had to be approved locally and centrally. The pharmacist developed a protocol for the management and evaluation of the DSME program and submitted it for approval from the Chief of Clinical Pharmacy at the BOP. The pharmacist also established a collaborative practice agreement with the Clinical Director at FMC Devens to prescribe and manage diabetes therapy for inmates who are enrolled in the clinic. The Chief of Clinical Pharmacy also approved the collaborative practice agreement and kept a copy on file in the Central Office of the BOP.
Outcomes for the diabetes clinic are reported to the Chief of Clinical Pharmacy annually. The pharmacist who manages the clinic reports to the Chief Pharmacists and Clinical Director at FMC Devens and to the Chief of Clinical Pharmacy at the Central Office of the BOP. The pharmacist collaborates with other members of the interdisciplinary team to provide diabetes education and management services and with Quality Improvement personnel to track patient outcomes.
The primary goal of the pharmacist-managed clinic is to have less than 15% of the diabetes population at FMC Devens with an A1C of 9.0% or greater. This goal aligns with the BOP’s Performance Measure Data. When inmates achieve 2 consecutive A1Cs less than 7.5%, they are discharged from the clinic.
Standard 2: External Input
The national DSME standards require a program advisory committee. The committee can include people with diabetes, health professionals, and members or representatives of community interest groups. It gives the providers a relevant perspective of the community’s needs.
FMC Devens currently does not have an advisory board. Adding an advisory group would help to raise awareness on issues such as culture, race, and ethnicity in managing diabetes. Given the restrictive nature of the prison environment, it would be easier to create an advisory board from within the facility. The advisory group could be comprised of social workers, case managers, and other correctional staff that are not involved in the clinic who could provide insight on how the DSME program might further meet the needs of inmates.
Standard 3: Access to Diabetes Education
Many people with diabetes have limited access to diabetes education due to socioeconomic or cultural factors. Some of the ways in which diabetes educators can improve access to DSME is through identifying the specific population to be served, conducting a needs assessment for the population in question, and identifying and overcoming barriers to access.
Prior to starting a diabetes clinic at FMC Devens, the pharmacist reviewed A1Cs and noticed that there were several inmates with an A1C above the BOP A1C goal of less than 7.5%. Due to the large number of patients that were above goal, it would have been difficult for the pharmacist to manage them independently while performing her traditional pharmacist duties. The Chief Pharmacist decided that they should focus on those with the highest A1Cs and set the cutoff at 9.5% or higher. The team providers continued to manage those with A1Cs above goal but did not meet the criteria for the pharmacist-managed diabetes clinic. Starting the diabetes clinic at FMC Devens improved the inmates’ access to diabetes care.
FMC Devens Interdisciplinary Diabetes Program
One of the strong points of the BOP is that it provides inmates with equal access to care regardless of their race, ethnicity, education, socioeconomic background, or culture. While access is important, Betancourt et al conclude that other social determinants can also affect patient care. The CDC identifies these determinants as age, sex, gender, discrimination, income, personal behavior, and living environment.
Another way to improve health outcomes is by developing cultural competence. Cultural competence describes the amalgamation of similar behaviors, attitudes, and policies in a system, an agency, or among professionals. The US Department of Health and Human Services maintains that cultural competence is important because it helps to significantly diminish disparities. The pharmacist managing the diabetes clinic applies the principles of cultural competence as many of the inmates who are enrolled in the clinic faced health disparities prior to incarceration.
Standard 4: Program Coordination
The role of the coordinator includes planning, implementing, and evaluating the educational services that are being provided. The pharmacist managing the FMC Devens DSME program fills the role of coordinator and meets the requirements of Standard 4.
Standard 5: Instructional Staff
Since diabetes is a multifaceted disease that can be very complex to manage, patients benefit from the expertise of several disciplines to help them manage their disease. Standard 5 focuses on instructional staff. It requires the staff members to a certified diabetes educators or to obtain up-to-date education and training in diabetes education and management.
Options for preparation include becoming a Certified Diabetes Educator (CDE), achieving board certification in advanced diabetes management (BC-ADM), and enrolling in a graduate program. In addition, instructors are required to complete continuing education credits in diabetes management on a regular basis.
The pharmacist who manages the diabetes clinic at FMC Devens obtained a certificate in diabetes management from the American Society of Health Systems Pharmacists and completed the master’s degree program at Teachers College, Columbia University.
Even with advanced training, an educator may not be able to cover everything. Therefore, when a need arises that is beyond the scope of the educator, he or she can have a referral system in place to provide patients with access to individuals who are trained and licensed to provide the education that is needed.
Although the diabetes clinic at FMC Devens is managed independently by the pharmacist, the care is provided by an interdisciplinary team. The team consists of primary care physicians and midlevel providers, an ophthalmologist, a contract endocrinologist, 2 dentists, a psychologist, the pharmacist, 2 dietitians, 2 physical therapists, a nurse, and the recreation department staff. The pharmacist refers patients to other members of the team based on individual needs. A subset of the interdisciplinary team meets weekly to discuss patients that are seen in the clinic.
Although the diabetes clinic at FMC Devens is managed independently by the pharmacist, the care is provided by an interdisciplinary team.

Standard 6: Curriculum
Standard 6 sets the parameters for designing a DSME curriculum. Adopting a standard curriculum that follows the existing evidence and clinical practice guidelines can lead to positive outcomes.
At FMC Devens, 1 of the dietitians organized an interdisciplinary teaching curriculum for inmates who need guidance in managing their diabetes. Currently, experts in nutrition, physical therapy, pharmacy, ophthalmology, dentistry, and psychology teach topics related to their disciplines and provide comprehensive information sessions for these inmates. For instance, the pharmacist provides information about the different types of diabetes medications (oral and injectable) that are used at the prison. Inmates get an overview of their uses, benefits, side effects, and interactions. While the curriculum was not developed specifically from the DSME standards, it aligns with AADE7, which focuses on teaching self-care behaviors.
Standard 7: Individualization
This standard has had the biggest impact to date on the diabetes clinic at the prison because it highlights the importance of the patient-centered approach. This standard acknowledges that the patient has the difficult task of managing his or her diabetes on a daily basis. It is the educator’s responsibility to make diabetes management easier for the patient. In addition to the national DSME program standards, the AADE created the Scope and Standards of Practice of Diabetes Education for Pharmacists. Prior to utilizing these standards, the pharmacist at FMC Devens focused primarily on medication management and has since shifted to a patient-specific approach.
Standard 7 calls for the instructor to conduct a thorough assessment of the person with diabetes. The purpose of an assessment is to recognize the patient’s needs and facilitate the selection of appropriate educational and behavioral interventions and self-management support strategies guided by evidence. In order for an assessment to be successful, both the patient and the educator must be in agreement with it.
According to the AADE scope and practice guidelines, the pharmacist is responsible for reviewing current medications, which include prescription and over-the-counter medications and alternative therapies. They also evaluate the patient’s lifestyle habits including diet, exercise, tobacco, and alcohol use. In addition, they assess medical conditions, financial issues, and the effect of therapeutic interventions.
The pharmacist is also tasked with assessing the patient’s understanding, willingness, and ability to change behaviors in order to achieve their goals. As with any other discipline, the pharmacist can use an empowerment approach such as motivational interviewing (MI). Motivational interviewing is defined by DiLillo and Smith West as a “client-centered, collaborative counseling strategy designed to help people explore and enhance motivation to change behavior while supporting autonomy and self-efficacy.” Motivational interviewing encourages the use of tools such as empathy, affirmation, and open-mindedness. The DSME pharmacist at FMC Devens uses MI to conduct patient assessments. The pharmacist shows empathy for the inmates by acknowledging that diabetes self-management is difficult, affirming the inmates when they make an effort to improve their diabetes, and including them in the decision-making process when changing their therapy. The pharmacist at FMC Devens also utilizes MI to encourage inmates to make changes to their diet, level of physical activity, and commissary purchases and to help improve medication adherence.
The most important part of an assessment is determining the readiness of the patient to accept and follow the recommendations. Decoste and Maurer emphatically expressed this point: While the education approach may be well matched to a person or population being served, if those on the receiving end are not ready to receive information or if the information is unimportant to them at the time, learning will likely be compromised.
When the client is in agreement with the plan and is ready to change, the plan can be implemented. The DSME standards for pharmacists encourage the use of MI during the implementation phase. The goal is to create an atmosphere that is conducive to the client sharing the pros and cons of the behavior in question. The pharmacist reviews drug therapy information with the patient, including side effects and adverse reactions. When a referral is necessary, the pharmacist may submit a referral request to members of the collaborative team such as dietitians, exercise physiologists, or behavior interventionists to assist the patient in making behavior changes.
Another individualized approach that is being utilized at FMC Devens is outcome identification. The pharmacist can educate the patient about diabetes and its comorbidities and assist the patient in understanding the benefits that can be achieved from utilizing drug therapy and other educational interventions. During the 1-on-1 initial visit, the pharmacist encourages inmates to set specific, measurable, attainable, realistic, and timely (SMART) goals for improving their diabetes outcomes. A typical SMART goal is to achieve a target A1C at goal within a 6-month period. These goals are reinforced at subsequent appointments.
Planning is a collaborative process based on current practice guidelines that includes the team of providers, the patient who has or is at risk for diabetes, and other members who provide support. The medical model often eliminates the patient from the decision-making process. Anderson and Funnell suggest that when health care providers empower their patients, they provide an opportunity for patients to make critical, independent, and educated decisions. Patients are usually experts on themselves; therefore, it is prudent to include them in the decision-making process.
Using the empowerment method has been effective in helping inmates to more effectively manage their diabetes. Inmates in the DSME program are included in decision making regarding their disease management.
The final component of individualization is evaluation. The AADE has stated that the pharmacist is responsible for monitoring and evaluating patients with diabetes on an ongoing basis. The evaluation process involves gathering and interpreting outcomes information from patients and health care providers. At FMC Devens, the pharmacist tracks A1Cs and monitors the patient’s flow-sheet to observe trends in plasma glucose. This is helpful in tracking adverse events such as hypoglycemia and aids in making adjustments in therapy.
Standard 8: Ongoing Support
Follow-up and ongoing diabetes self-management support (DSMS) is an essential component of DSME because it helps to reinforce new habits. There are many creative strategies that can be employed to help patients stay motivated and succeed in managing their diabetes. Maryniuk and Siminerio suggest that support services may be provided through nurse case managers, disease management programs, trained peers and health community workers, community-based programs, use of technology, ongoing education and support groups, and medical nutrition therapy. At FMC Devens, the inmates receive ongoing education and support through group sessions, peer bonding, and religious services.
At FMC Devens, the inmates receive ongoing education and support through group sessions, peer bonding, and religious services.
There is no evidence that 1 DSMS approach is superior to another. Brownson et al point out that it is prudent to utilize a wide range of approaches to facilitate different needs and preferences and to improve program access.
The DSME pharmacist at FMC Devens holds monthly individual follow-up appointments and hosts quarterly DSMS group meetings with the inmates. The group sessions serve a dual purpose. They provide an opportunity for inmates to share their concerns about diabetes, and they also serve as a forum for the pharmacist to provide diabetes information and hand out certificates of achievement to those who are eligible for discharge from the clinic. Inmates feel accomplished when they receive the certificates. Witnessing inmates receive the certificates inspires other inmates to try harder to improve their diabetes outcomes. In addition, the dietitian provides diabetes education classes throughout the year for inmates, which helps to reinforce self-management behaviors.
While DSMS is essential for continued success, without documentation it would be difficult to track and to assess its efficacy. Therefore, as Maryniuk and Siminerio assert, it is incumbent on educators to document follow-up methods, how frequently they occur, and the manner in which they are delivered. Using simple language in documentation provides clarity and reinforces the sentiments of the team, according to Fisher et al.
All patient encounters in the FMC Devens diabetes clinic are documented in the BOP electronic medical record (BEMR) system. These medical records can be accessed by providers throughout the BOP in the event the inmate is transferred to another facility.
Standard 9: Patient Progress
In order to determine if the DSME program is effective, there must be systems in place to measure the patient’s progress. Standard 9 states that those who provide DSME and DSMS services should utilize the right instruments to measure the efficacy of the educational tools in assisting patients with attaining their individualized diabetes self-management goals and outcomes and determine the efficacy of the education program.
Program outcomes need to be reported, and the protocols for the program need to be revisited and revised continually in response to knowledge enhancements, changes in treatment approaches, education updates, psychosocial interventions, fluctuations in consumer trends, and the ever-changing health care environment. FMC Devens’s DSME program outcomes are reported to the BOP’s Chief of Clinical Pharmacy Programs. Figures 1, 2, and 3 show the diabetes clinic outcomes for January to December 2014.
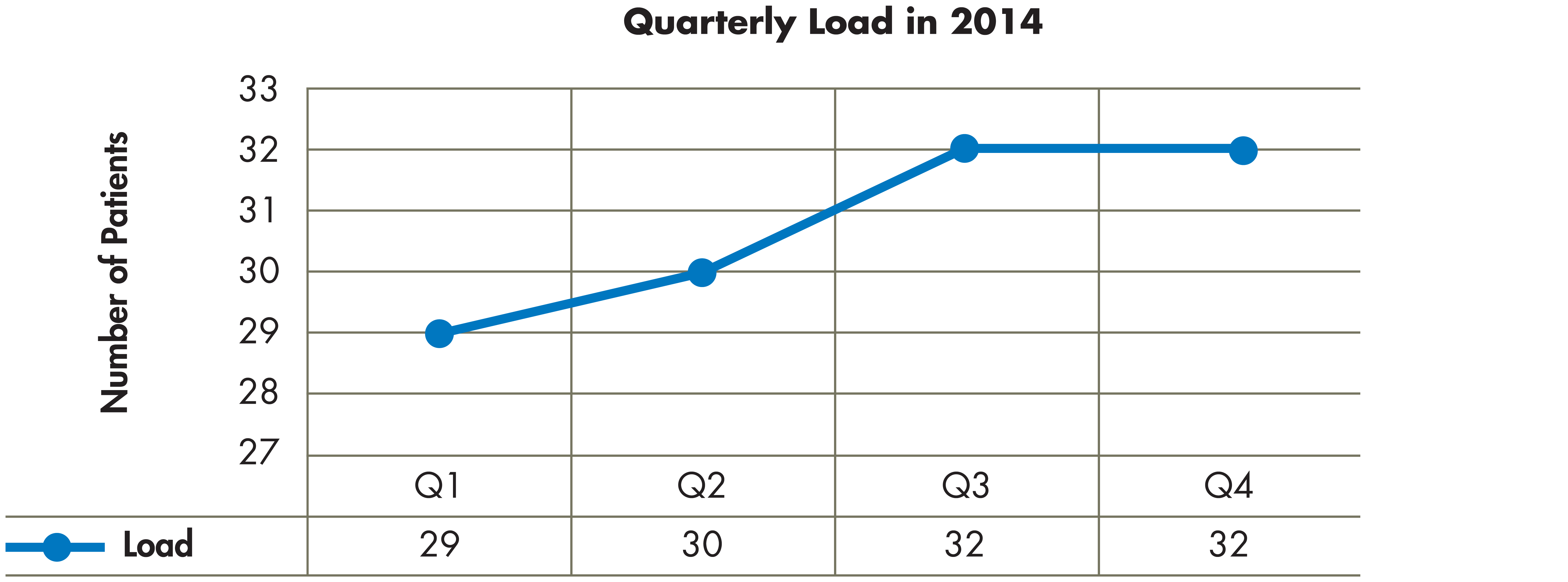
Number of patients seen at FMC Devins diabetes clinic, January-December 2014.
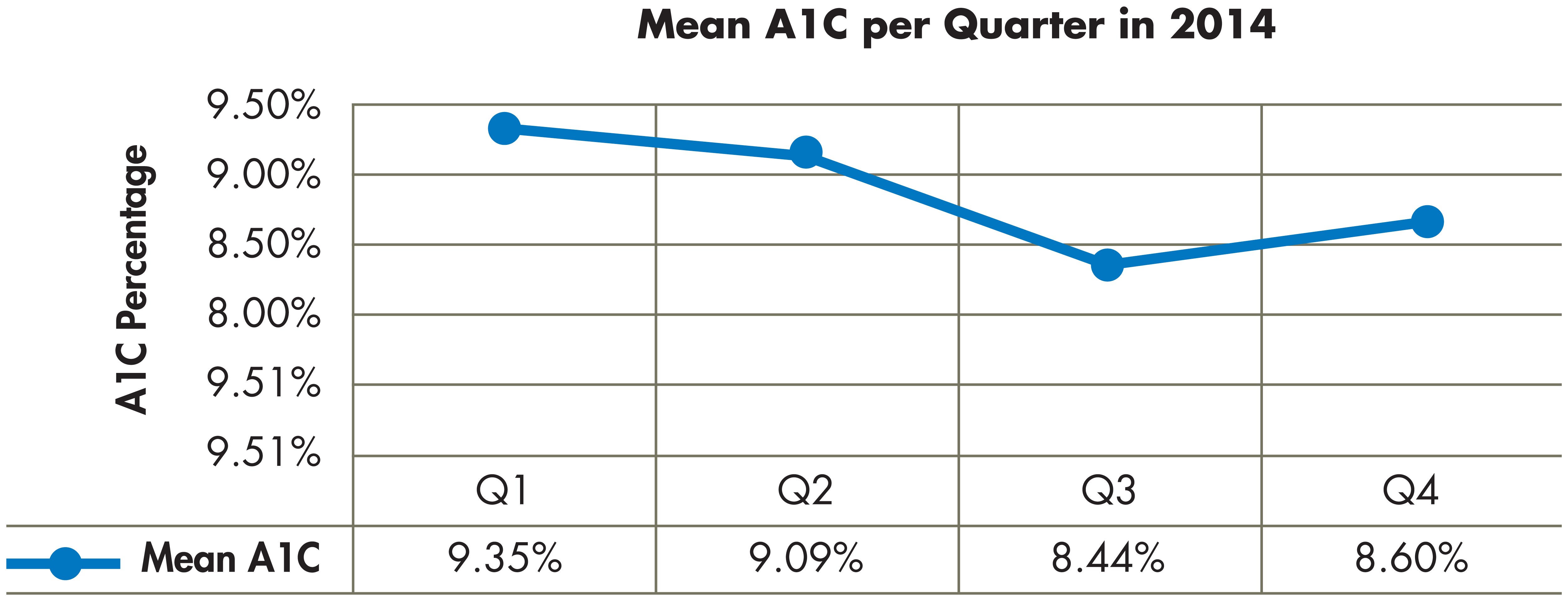
FMC Devins diabetes clinic mean A1C, January-December 2014.
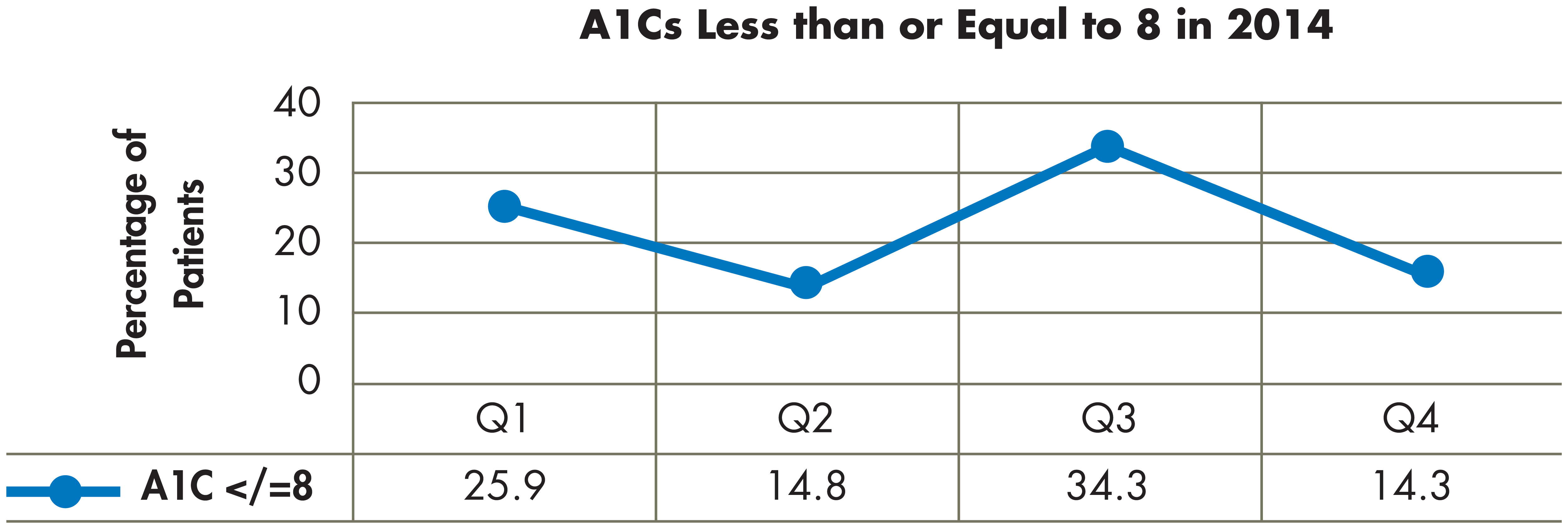
FMC Devins diabetes clinic A1C outcomes, January-December 2014.
The data show that patient load increased steadily in quarters 1 and 2 but remained constant in quarters 3 and 4. The percentage of inmates with an A1C less than or equal to 8% fluctuated throughout the year, with the most notable increase occurring in the third quarter. The mean A1C for all inmates in the clinic decreased steadily in the first, second, and third quarters but increased slightly in the fourth quarter. In 2014, 16 inmates were discharged from the clinic. Three inmates were not included in the data because they left before an ending A1C could be drawn.
Inmates are formally discharged from the clinic when they achieve 2 consecutive A1Cs less than 7.5%, transfer to another institution, die, or complete their sentence. Inmates who are not ready to change their behavior are returned to their provider for management.
In 2014, inmates who were discharged had a mean baseline A1C of 10.62% and a mean ending A1C of 7.35%. On average, A1Cs decreased 3.27 percentage points from baseline (Figure 4). This has helped FMC Devens to meet the BOP goal of having less than 15% of the diabetes population with an A1C of 9% or higher. The biannual performance measure data for FMC Devens revealed that the percentage of inmates with an A1C greater than 9% decreased from 14% (22/160) in July 2014 to 9% (14/158) in December 2014.
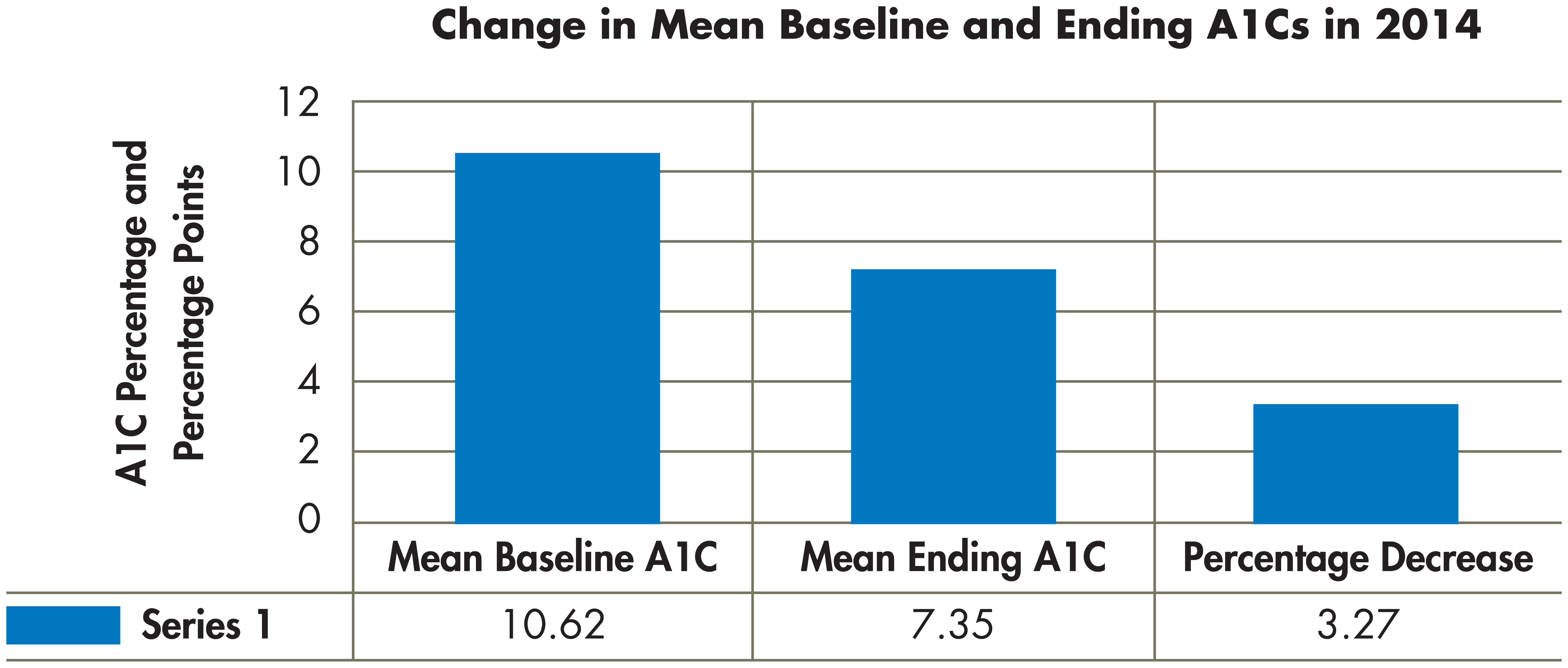
FMC Devins diabetes clinic baseline and discharge A1Cs, January-December 2014.
Standard 9 lists behavior change as the most valuable outcome as it provides guidance for assessment and documentation. AADE7 outlines 7 essential behaviors to assess in a DSME program. They include physical activity, healthy eating, taking medication, monitoring blood glucose, diabetes self-care–related problem solving, reducing risks of acute and chronic complications, and psychosocial aspects of living with diabetes. The DSME program at FMC Devens does not report outcomes on all these behaviors because there is currently no tool in place to evaluate patient progress in all areas. It will be helpful to create a self-care behavior questionnaire that can be given at baseline and readministered prior to discharge.
Standard 10: Quality Improvement
According to Haas et al, DSME providers conduct a systematic review of process and outcome data to determine if the educational and support services were effective. They also seek out opportunities to enhance the program, highlight areas for improvement, and evaluate the quality of services for efficacy, inconsistencies, and inferiority.
At FMC Devens, the diabetes team has made improvements to the program since its inception. Originally, inmates were enrolled with an A1C of 9.5% or higher, but it was changed to 9% and above to further improve the outcomes. The new Clinical Director at FMC Devens recently formalized the diabetes team, and a subset of the team meets weekly to discuss the patients that were seen during that week. The long-term goal of the DSME program is to become AADE accredited. This would help to optimize the educational experience for the inmates and continue to improve outcomes.
Conclusion
While there is an abundance of literature on pharmacist-managed DSME programs in various federal agencies such as the VA, the literature is lacking for DSME programs in federal prisons. More and more pharmacists are creating DSME programs at various federal correctional facilities. This article provides insight on how applying the national standards can help to create or enhance DSME programs at other federal facilities.
The DSME program at FMC Devens meets Standards, 1, 3, 4, 5, 6, 7, 8, and 10 of the National DSME Standards. However, it is deficient in Standards 2 and 9. Standard 2 requires the establishment of an advisory board. Establishing an advisory board would help to identify patient needs that may not be obvious to the DSME team. The DSME program is deficient in Standard 9 because there is currently no instrument in place to track changes in self-care behaviors. Developing an instrument such as a questionnaire that addresses the 7 self-care behaviors may be beneficial in evaluating behavioral outcomes.
The DSME program at FMC Devens meets the DSME Standards for Pharmacists. Since its inception, there have been notable improvements to the program. Providers in the program now manage inmates with an A1C of 9% or higher, they formalized the team, and they meet weekly to discuss inmates.
The long-term goal of the clinic is to become AADE accredited. Meeting all of the standards will help to prepare the FMC Devens DSME program for accreditation. ■
Footnotes
Juliet R. Jordan, PharmD, MSDEDM, NCPS, is a pharmacist and leads the diabetes clinic at Federal Medical Center at Devens in Devens, MA. The author would like to thank Jane Dickinson, RN, PhD, for her advice and expert opinion about the manuscript.