
Abstract


NYU Winthrop Hospital, certified by the Joint Commission in Advanced Inpatient Diabetes Care, is a 591-bed major teaching hospital located in a suburban setting. As part of a post-discharge, hospital-wide insulin safety initiative that involved calling patients after discharge, a disturbing pattern emerged. Patients were not filling prescriptions for blood glucose monitoring supplies and insulin due to insurance-related issues and were not receiving outpatient instruction concerning use of the devices.
The transition from the inpatient setting to home was identified as a risk point representing a potential discontinuity in care for the patient. To facilitate and improve patient education concerning use of diabetes-related devices from hospital to home, NYU Winthrop implemented a collaborative inpatient diabetes education program. Through the efforts of pharmacists and nurses, the objectives for this service include increasing patient confidence upon discharge regarding use of diabetes-related devices and eliminating meter- and insulin-related prescription problems.
Description
As an American Nurses Credentialing Center Magnet-recognized organization, the philosophy of nursing care at NYU Winthrop supports direct care nurses providing total care for their patients, including diabetes self-management education. Diabetes Nurse Clinicians, who are Certified Diabetes Educators, provide expertise, staff education, and management oversight but are not responsible for educating patients in the hospital. The structure of this collaborative service combines the expertise of direct care nurses, a preceptor pharmacist, and postgraduate (year 1) pharmacy practice residents. This service is strengthened by the participation of pharmacy residents who are assigned to a monthly rotation with a focus on improving their patient education and counseling skills.
Available daily from 8 am to 9 pm, the pharmacist delivers focused skills-based training and education reinforced by direct care nurses for patients who have not been treated with insulin therapy prior to hospitalization and need to learn how to use diabetes devices, such as a blood glucose meter, insulin pen, or insulin vial and syringe.
A unique aspect of the collaborative diabetes education program involves the pharmacist’s skill in navigating the prescription drug and durable device formularies to assist the provider in prescribing devices covered by the patient’s insurance. Because there is no universal, accurate, and easily accessible system that identifies which diabetes-related devices and medications are covered under an individual’s insurance plan, the pharmacist procures and documents this information in the electronic health record.
A unique aspect of the collaborative diabetes education program involves the pharmacist’s skill in navigating the prescription drug and durable device formularies to assist the provider in prescribing devices covered by the patient’s insurance.
Funding was secured so that each patient requiring education about blood glucose monitoring receives a blood glucose meter prior to discharge. In this way, the patient can learn how to use the actual meter that will be used at home. The meters are purchased by the hospital, paid for by donations, and given to patients at no charge to them. These meters are recorded into a pharmacy log that includes patient identification, meter brand and serial number, and the date the meter was accessed, in the event of recall.

Once the specifics of insurance coverage are determined, the pharmacist assesses the patient’s learning needs and teaches the patient how to use a meter and insulin delivery device, addresses patient fears regarding self-injection, and reviews blood glucose targets as well as hyperglycemia and hypoglycemia management. Educational tools include a teaching kit that consists of demonstration insulin pens, normal saline vials, syringes, an injection pad that feels like human skin, and supporting handouts. Direct care nurses continue skills-related teaching and reinforce educational content throughout the hospitalization following the initial education session. As needed, family members and caregivers are included in the education process. The pharmacist assesses the patients’ competency and learning by having them teach back what they have learned. Home care referrals are made when appropriate.
Evaluation and Survey
To evaluate the impact of the program, we solicited patient feedback through post-discharge telephone survey calls. This pilot survey consisted of 9 questions assessing the patients’ fears and confidence after their diabetes-related device education, difficulties in filling prescriptions at the pharmacy, and feedback regarding what they found beneficial and what they would change about their education sessions. Patients were considered lost to follow-up based on 3 unsuccessful telephone attempts or greater than 1 month since discharge. This pilot phase consisted of 51 post-intervention telephone surveys that informed the design of our quality improvement (QI) project.
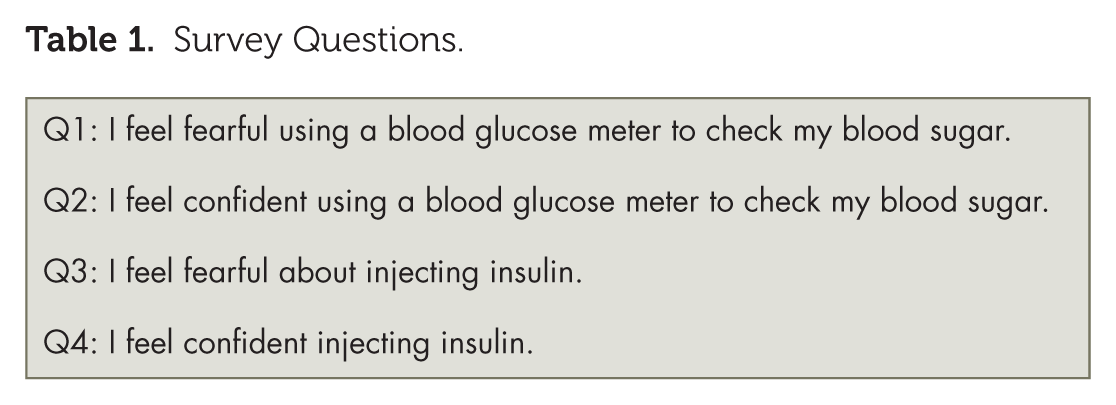
The QI project included a pre- and post-intervention survey intended to evaluate patients’ change in fears and confidence regarding use of devices before and after education (Table 1). Both surveys consist of 2 questions identifying patients’ fear and confidence using a blood glucose meter and 2 questions identifying patients’ fear and confidence injecting insulin. The post-intervention survey also identifies patients’ difficulties in filling prescriptions for diabetes-related devices following discharge. Participant responses were rated using a Likert scale corresponding to agree, neutral, or don’t agree. A Wilcoxon signed-rank test was used to determine significant differences between pre- and post-education responses.
Survey Questions.
Results
Between December 2017 and April 2018, 49 patients participated in education about diabetes-related devices, and 27 of these patients completed pre- and post-education surveys. Table 2 describes the baseline characteristics of the participants. Participation in insulin injection instruction included 26 patients (answered questions 3 and 4), and 17 patients participated in learning how to use a blood glucose meter (answered questions 1 and 2).
Participant Characteristics.
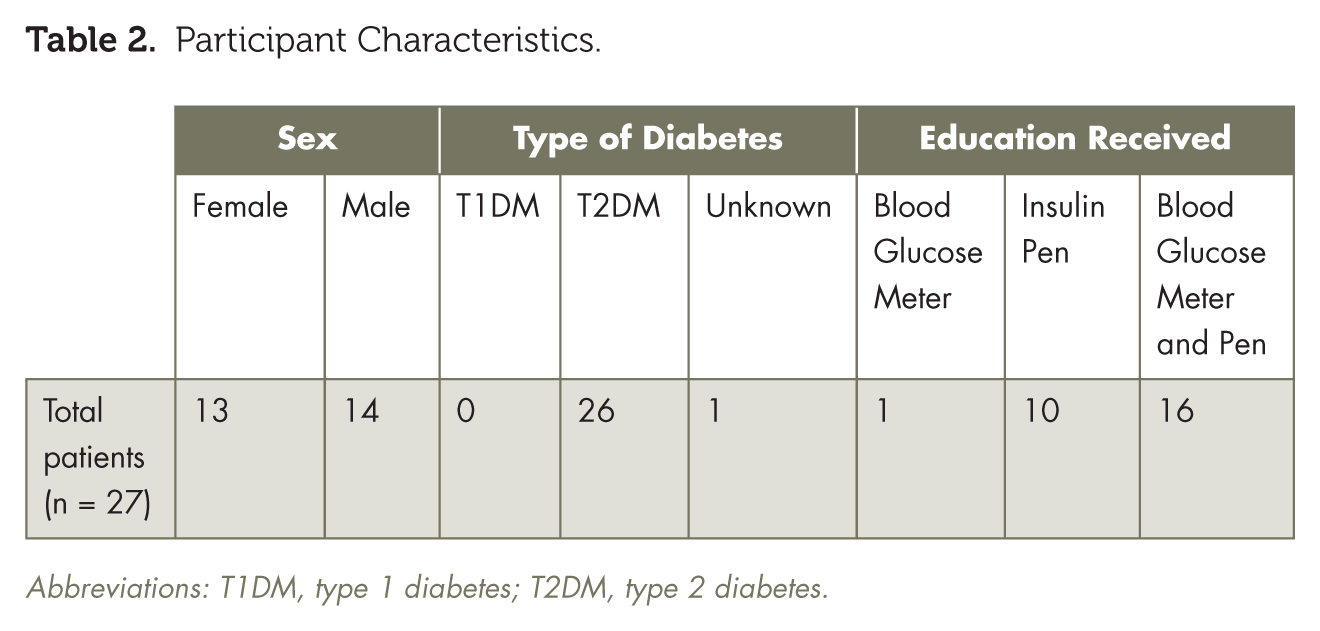
Abbreviations: T1DM, type 1 diabetes; T2DM, type 2 diabetes.
The post-education response results demonstrate that both those who learned how to use a blood glucose meter (n = 17) and those who learned about insulin injection (n = 26) were significantly more confident and less fearful, as shown in Table 3.
Wilcoxon Signed-Rank Test Results.
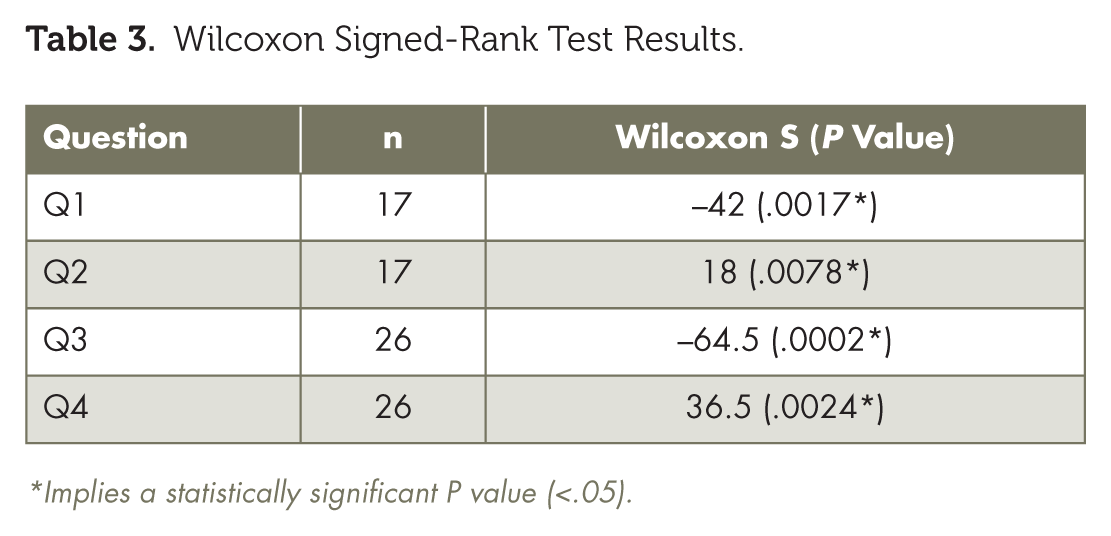
implies a statistically significant P value (<.05).
The efforts of the pharmacist to verify each patient’s insurance benefit resulted in the correct match of both the brand of meter and insulin prescribed with the patient’s insurance coverage. However, before the e-prescribe system was equipped to include pen needles, 2 patients lacked pen needle prescriptions following discharge. One patient was surprised to learn at the point of purchase of an extremely high deductible associated with the insurance company formulary’s preferred brand of insulin. Specific details regarding deductibles and coinsurance are particularly difficult to acquire in the inpatient setting. In addition, the increasing need for prior approval of insulin prescriptions is a demanding challenge to manage.
Limitations
Our statistical analysis was not able to estimate the exact effect education had on fear and confidence due to the small sample size. The survey tool was not tested for reliability and validity and did not capture participants’ previous exposure to blood glucose meters and insulin injections, which may have particularly influenced the individuals who felt confident prior to instruction.
The possibility of sample bias exists in that those who chose to answer the post-intervention survey may have valued the education and wanted to participate. Some patients may have also had conflicting answers regarding fears and confidence, perhaps due to response error.
Discussion
Across the country, we continue to struggle with the lack of a universal system for electronically identifying the diabetes-related products and medications that are part of an insurance plan’s formulary and the associated deductible, copay, or need for prior authorization. As our program has demonstrated, the time-consuming process of calling the patient’s insurance plan and verifying the preferred products and copays cannot completely eliminate all delays in securing the prescribed products or medications as an outpatient.
Patients return home knowing how to use blood glucose meters covered by their insurance plans and how to competently administer insulin. Providing both diabetes education and the supplies required for self-management strengthens the transition from hospital to home.

The collaborative inpatient diabetes education program, fully integrated into patient care, has filled the gaps in care related to diabetes-related device teaching. This service has increased patient confidence and reduced fear. Patients return home knowing how to use blood glucose meters covered by their insurance plans and how to competently administer insulin. Providing both diabetes education and the supplies required for self-management strengthens the transition from hospital to home. ■
Footnotes
Victoria J. Polla, PharmD, RPh; Virginia Peragallo-Dittko, RN, BC-ADM, CDE, FAADE, FAAN; Kara K. Foldes, PHARMD, RPH; and Melissa J. Fazzari, PHD, are with NYU Winthrop Hospital in Mineola, NY.