
Abstract
Purpose:
We conducted a scoping review to map peer-reviewed literature on HIV research concerning sexual minority women (SMW).
Methods:
Following guidance from Arksey and O’Malley’s framework and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews, we searched PubMed, Embase, PsycInfo, Sociological Abstracts, and CINAHL from inception through May 2023. Eligible studies were English language, peer-reviewed studies, containing disaggregated HIV-related data on SMW. Studies were systematically screened, and relevant data were extracted and then summarized.
Results:
Our search identified 7615 studies; 187 met eligibility requirements. Most studies were quantitative (82%), cross-sectional (74%), used survey data (80%) obtained via convenience sampling (61%), and conducted in the United States (65%). Annual publications increased over time. Overwhelmingly, studies did not report engaging the community in the research process (93%). Demographic reporting in studies varied; about half reported age (52%) and race (52%), two-thirds reported sexual orientation (68%), and only 25% focused exclusively on SMW. Diverse HIV-related findings were addressed: sexual risk behaviors (64%), HIV testing, prevalence, and risk perception (47%), substance use (43%), sexually transmitted infections (29%), health care access (21%), intimate partner violence (17%), mental health (15%), stigma (10%), and incarceration (9%).
Conclusions:
Our review highlights key methodological and topical gaps. Future SMW HIV research guidance includes focusing on structural-level factors and biomedical interventions; researching understudied regions highly impacted by HIV; including qualitative and quantitative approaches; establishing standardized procedural and reporting guidelines; and increasing research and practice resources to focus on SMW’s unique HIV-related health strengths and vulnerabilities.
Introduction
Sexual minority women (SMW)—women with a minoritized sexual orientation or identity such as lesbian, gay, bisexual, or queer, as well as women who are sexually attracted to or romantically/sexually partner with other women—are an often-overlooked population in the extant human immunodeficiency virus (HIV) literature.1–4 Although disparities in HIV outcomes among women by sexual orientation are largely unexplored, some have been found among (sub)groups of women. For example, among women who inject drugs, HIV rates are higher in SMW versus heterosexual women (13.3% vs. 3.9%). 5
HIV transmission is influenced by the aggregation of multiple HIV vulnerabilities6–10—that is, factors associated with HIV risk such as sex work engagement,11–14 substance use,15–17 housing instability,18–20 and low health care service utilization.21,22 The growing SMW health literature has documented greater HIV vulnerabilities among SMW compared with their heterosexual counterparts,23,24 including sexual risk behaviors,23,25 illicit drug use,26,27 housing instability, 28 sex exchange,23,29 incarceration status, 30 violence, 23 reduced health care access, 31 stigma, 32 and HIV comorbidity with other sexually transmitted infections (STIs). 33 These data indicate that SMW have unique and exacerbated HIV risk, warranting greater public health attention.
The paucity of research on SMW’s HIV risk and outcomes is due to both methodological limitations and research priority setting. Many large HIV-related studies do not collect or report data on sexual orientation among women.34–36 Further, health and HIV studies among sexual minority populations have historically focused on cisgender men or multigender samples.37–40 Among studies that include multigender samples, data disaggregation is often limited, thus obscuring potentially significant gender differences.23,41,42
Research on HIV risks, prevalence reporting, and prevention programming has primarily focused on “key populations” considered to be at higher risk of HIV acquisition, such as gay, bisexual, and other men who have sex with men (GBMSM), transgender women, people who use drugs, and sometimes women who exchange sex.23,41,42 The volume of published research on these populations is remarkable; from 1980 to 1999, GBMSM were included in 95% of published articles related to STI research (including HIV). In contrast, SMW were included in only 6% of articles in the same period. 43 Although the high impact of HIV on key populations is unrefuted, greater attention to other vulnerable (sub)groups remains warranted.
A common rationale for the de-prioritization of SMW in HIV research and prevention efforts is that rates of HIV transmission from woman-to-woman sex are low.1,44 Although this may be true regarding oral/vaginal sex between cisgender women, concluding that SMW have low risk is a mistake, as it fails to consider other psychosocial and behavioral factors that influence HIV transmission risk. Such conclusions rest on a series of false assumptions. First, sex between women can happen in a range of ways and is not limited to oral/vaginal sex. Second, not all women have vaginas; transgender women can have various genitalia depending on their gender goals and journey. Third, SMW, even lesbian-identifying women, do not necessarily have sex with other women exclusively23,24,45–47; assuming overlap between sexual identity and behavior is a common error. Finally, HIV transmission among SMW can occur not only via sex but also via injection drug use. The prevailing narrative of HIV invulnerability among SMW poses a significant threat to HIV research and prevention efforts and further reinforces the systematic neglect of SMW’s needs in sexual and reproductive health services.2,48
Even less HIV research attention is paid to SMW with other minoritized or stigmatized social positions and identities, such as minoritized racial and ethnic populations. The concepts of intersectionality, coined by Kimberle Crenshaw 49 and applied to HIV research by numerous contemporary scholars,1,50–53 and minority stress, detailed by Dr. Virginia Rae Brooks in her seminal work on sexual minority stress theory among SMW,54,55 posit that intersecting forms of stigma and discrimination (e.g., sexism, homophobia, racism, transphobia) experienced by stigmatized groups result in deleterious physical and mental health outcomes.
Applied to the current topic, these theories suggest that SMW’s HIV risk is impacted by intersecting structural powers, which lead to disparate negative health outcomes among and between SMW (sub)groups. Applications of intersectionality theory to HIV research are still evolving, 56 and while measures of structural discrimination are becoming more available in published literature, much of the historic literature has used demographic categories as proxies for these structural forces, and even that work is limited in the field of SMW HIV research. 57 For example, little attention is paid to intersections of gender modality (i.e., cisgender and transgender) and sexual orientation (e.g., homosexual, heterosexual, bisexual) among women. Although there is now a sizable evidence base on HIV risk among transgender women, sexual orientation is rarely considered in that literature. 58 More work is needed to explore how structural-level power dynamics impact SMW HIV risk.
Minimal collated research describes HIV outcomes and the effect of syndemic HIV risk factors among SMW, despite a range of evidence suggesting the need for such insights. To address this gap, we conducted a scoping review to systematically map peer-reviewed literature concerning HIV among SMW globally. Knowledge gained from this endeavor can inform the future direction of HIV research and practice with SMW—including necessary descriptive research with understudied (sub)populations—and promote public health practice that is inclusive of SMW concerns and needs.
Methods
This scoping review followed the framework outlined by Arksey and O’Malley 59 and guidance from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 60 Institutional review board approval was not required as this review employs a secondary data analysis of published literature. No protocol was registered for this study.
Eligibility criteria
Eligible studies included peer-reviewed health research that contained disaggregated data on SMW and reported any findings related to HIV (e.g., HIV testing, prevalence, or any risk factors defined by the study authors as HIV-related). Eligible studies were published in English and were not limited by time frame or geographic location. We defined SMW individuals as any woman, cisgender or transgender, identifying with any sexual minority identity (e.g., lesbian, bisexual, queer), reporting ever having sex with women, or reporting same-gender attraction. Exclusion criteria included: gray literature (e.g., conference abstracts, dissertations), risk factors that are commonly recognized as HIV-related but not discussed in the article in the context of HIV (e.g., substance use), and including SMW in the sample but not providing disaggregated findings for SMW participants.
Data sources and search strategy
The search strategy included terms for HIV and SMW (Supplementary Table S1). Five databases were searched to identify peer-reviewed literature: PubMed (PubMed.gov), Embase (Elsevier), PsycInfo (EBSCO), Sociological Abstracts (ProQuest), and CINAHL (EBSCO). The search was run from inception to May 8, 2023, and restricted to English language items.
Screening process
References were managed and deduplicated in Covidence, a systematic review production tool. 61 During title and abstract screening and full-text review, each record was independently reviewed by two team members. Reviewers were blinded to each other’s decisions, and conflicts were resolved through discussion with the study’s principal investigator.
Data collection process
Data extraction was independently conducted for each record by two researchers; consensus was organized in Covidence, and conflicts were resolved by the research team in regular meetings. A template was designed to extract the following data: funding, study design, study location, sampling design, population demographics, sexual minority status measurement, gender measurement, data sources, community engagement, and key findings. Consistent with existing guidance on scoping reviews,60,62 formal risk-of-bias appraisal was not conducted.
Analysis and synthesis of results
Systematic narrative synthesis 63 was used to summarize and present study data, both within and between included studies. Microsoft Excel was used to calculate counts and percentages, which are always presented relative to the full sample size. 64 Excel’s “Geography” and “Map Chart” functions were used to analyze and map geographic frequencies (Fig. 2). 64
We modified a three-dimensional sexual orientation model 65 to analyze sexual orientation data operationalization including (1) identity (e.g., lesbian and bisexual identities), (2) behavior (e.g., women who have sex with women [WSW], women who have sex with women and men [WSWM]), and (3) attraction (e.g., attraction to other women), and added a “another operationalization” category for all other approaches.
For the race/ethnicity analysis, we used a modified version of the “Combined Race/Ethnicity” measure presented by Howell and Emerson. 66 Our categorization structure included (1) White, Caucasian, or European American; (2) Black or African American; (3) Hispanic/Latinx; (4) Asian or South Asian; (5) Biracial/Multiracial; (6) American Indian, Alaska Native, Native American, Aboriginal, and Torres Strait Islander; (7) Native Hawaiian or Other Pacific Islander. For studies that included racial or ethnic groups outside of this framework, we categorized them as (8) “Another race/ethnicity” and provided detailed reporting on the specific classifications observed within this category. When discussing studies, we use “SMW” population language regardless of language used by study authors,* and we offer insights on (sub)populations when available.
Team positionality
The research team included a principal investigator, an informationist, and five research team members supporting data collection, management, analysis, and article development. Our study team includes a diversity of identities, experiences, and perspectives. Five identify as cisgender women, four as LGBTQ+ (lesbian, gay, bisexual, transgender, queer, intersex, and asexual), three as SMW, and two as transgender/nonbinary people (identities not mutually exclusive). Most of the authors identify as White, hold graduate degrees in public health, and are U.S.-based. Team members were motivated by personal and professional interest and identification with the research topic and sample population. All team members were invited to bring their unique perspectives and lived experiences into the research process, which most likely influenced our study procedures and literature interpretation.
Results
Search results
The search returned 11,834 references, which were imported for screening. After identifying and removing duplicates, 7615 studies remained and were then screened against the title and abstract. Of those, 6967 studies were excluded, and 648 studies were assessed for full-text eligibility. Subsequently, 461 studies were excluded. Figure 1 illustrates the flowchart of article selection. 67 Ultimately, this review included 187 records.2,4,5,19,23,25,30,33,34,46,47,68–242
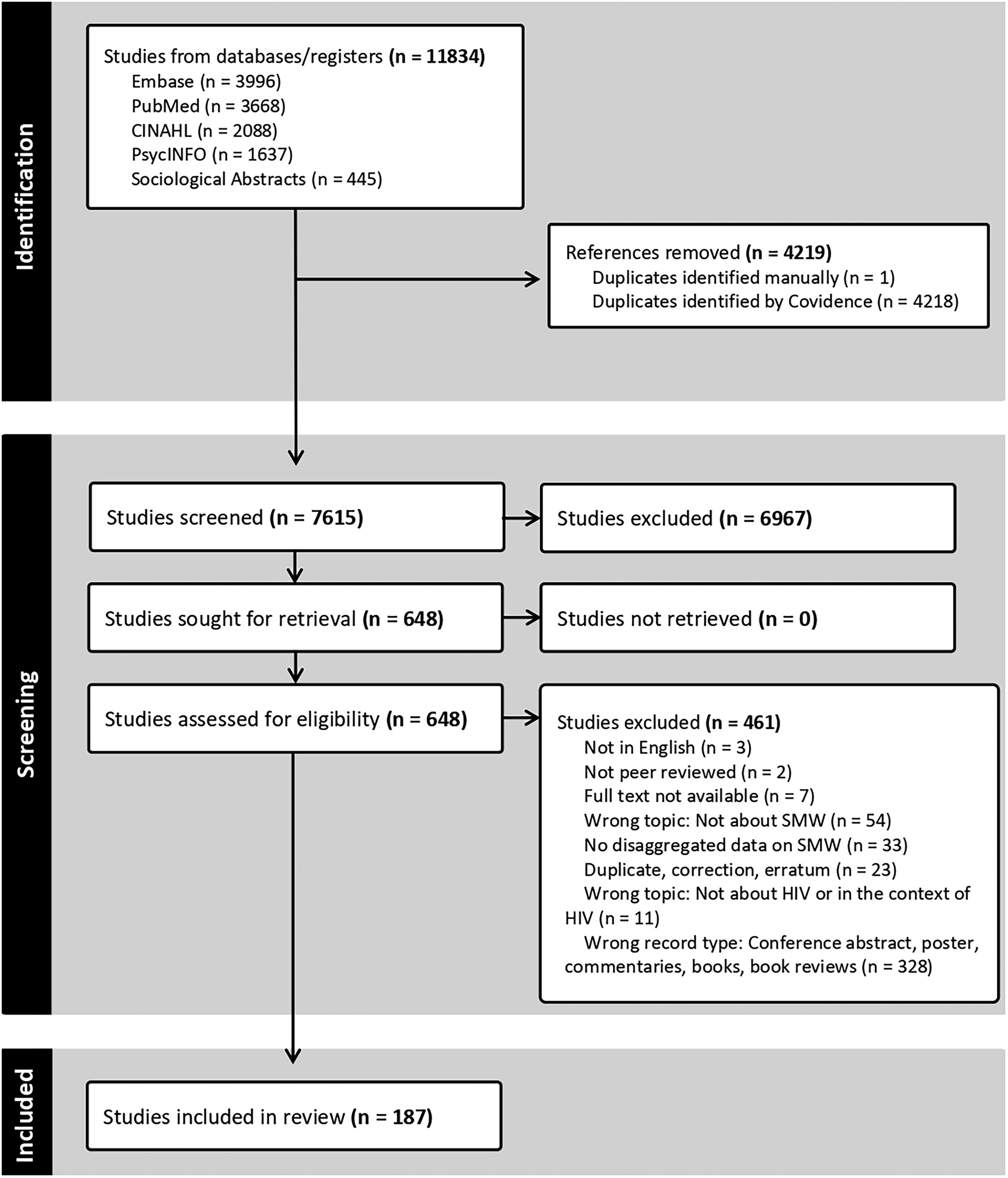
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart. 60
Study locations
The geographic representation of included studies varied: 121 studies were conducted in the United States (65%), 11 studies in Canada (6%), and 9 studies in Australia (5%). Further, five studies were conducted in Brazil (3%), four in the United Kingdom (2%), and three in China (2%). One study (0.5%) was conducted across both the United States and Canada. Six studies (3%) were conducted across Southern African countries: two studies were conducted in Lesotho, two were conducted across Botswana, Namibia, South Africa, and Zimbabwe, and one study each was conducted in South Africa and in a multicountry combination of Namibia, South Africa, and Zimbabwe. One study (0.5%) was conducted in each of the following countries: Chile, Czech Republic, Germany, Israel, Italy, Kenya, New Zealand, Norway, Philippines, and Spain. Notably, nine studies (5%) did not state their study location (Fig. 2).
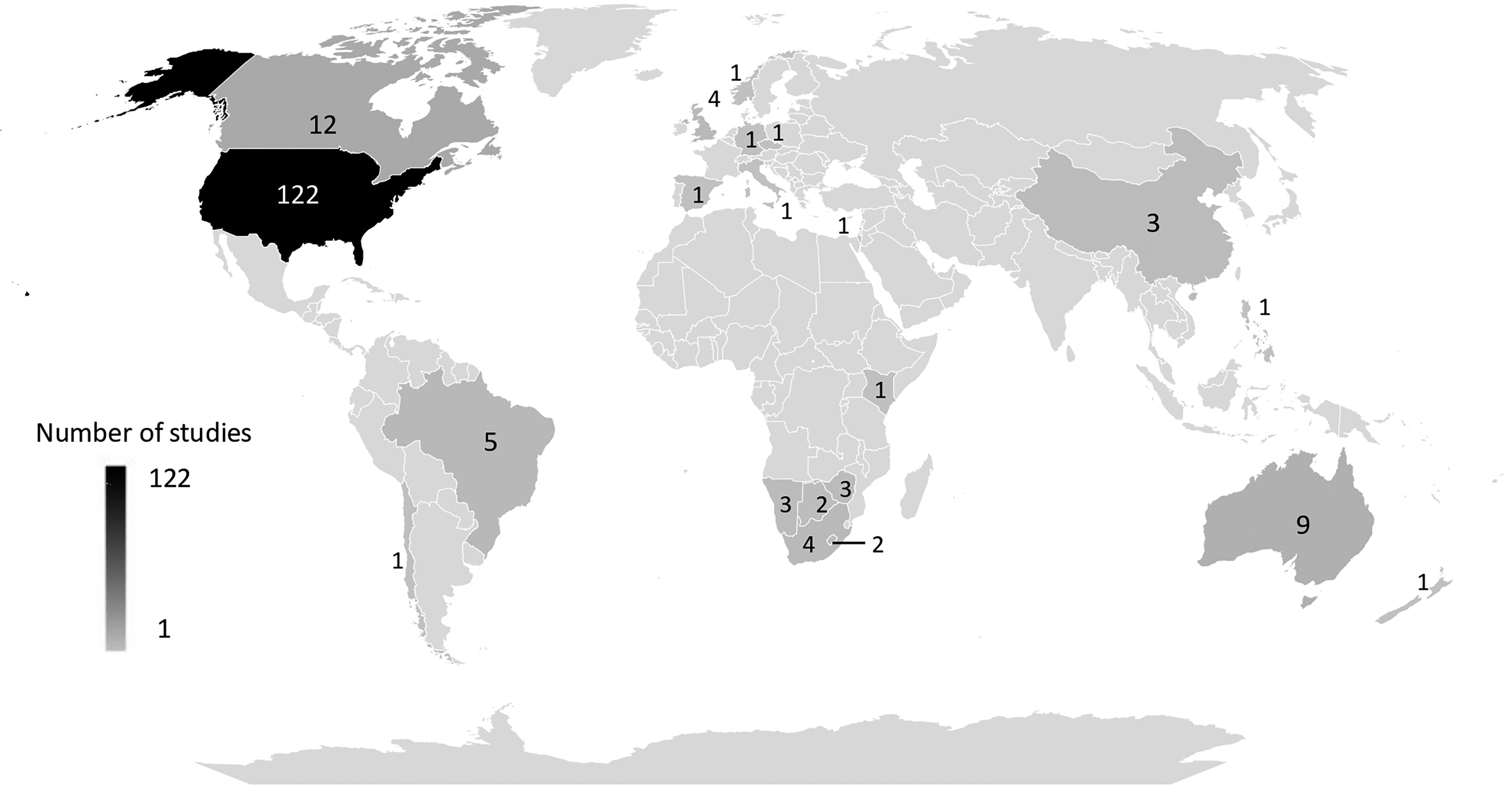
Map of number of studies by country.
Among the eight review studies included in our sample, three (2%) did not state a location of focus, three focused on a Southern African context (1: Botswana, Namibia, South Africa, and Zimbabwe; 2: South Africa; and 3: Southern Africa; 0.5% each), one (0.5%) on India, and one (0.5%) listed “Low- and Middle-Income Countries” as their location of focus. Study-level counts are reported in the text. In contrast, Figure 2 presents country-level data, in which studies conducted across multiple countries are counted in each applicable country.
Publications over time
The 187 included studies were published between 1990 and 2023. The annual volume of publications ranged between 0 (0%; 2004) and 13 (7%; 2022). Overall, there was an upward publication trend over time, as shown in Figure 3.

Chart of number of studies by year.
Methodological approach and study type
The included studies primarily employed quantitative methodology (n = 154, 82%). Most (n = 139, 74%) were cross-sectional, some (n = 14, 7%) were longitudinal cohort studies, and 1 (0.5%) was an ecological study. Twenty studies were qualitative (11%), eight were reviews (4%), and five were mixed- or multimethod studies (3%). Overwhelmingly, studies did not report community engagement in their studies (n = 173, 93%).
Most studies were observational (n = 175, 94%) followed by eight reviews (4%), three interventions (2%), and one (0.5%) that included both observational and intervention components.
Data sources and sampling
Most studies (n = 138, 74%) used only one data source, 44 (24%) used two, and five (3%) used three. Most data sources were surveys (n = 150, 80%), followed by study-related clinical examinations (n = 36, 19%), interviews (n = 20, 11%), focus groups (n = 12, 6%), and (electronic) medical records (n = 8, 4%). Other sources included ethnographic mapping (n = 2, 1%), surveillance data (n = 2, 1%), field notes (n = 1, 0.5%), and online posts (n = 1, 0.5%).
Forty-seven studies (25%) performed secondary analysis of previously collected survey data. These source studies include: National HIV Behavioral Surveillance (NHBS; n = 3, 2%), Women’s Interagency HIV Study (WIHS; n = 3, 2%), Youth Risk Behavior Survey (YRBS; n = 3, 2%), Protect and Respect study/Project (n = 2, 1%), National Health and Nutrition Examination Survey (n = 2, 1%), An Evaluation of Sex Workers’ Health Access (n = 2, 1%), and the Healthy Living Project (n = 2, 1%). In addition, in some cases, multiple articles were written about a single study; 26 (14%) articles included separate analyses coming from 12 distinct source studies. More specifically, for six source studies, two articles were written, and for one source study, three articles were written.
Most studies used only one type of sampling design (n = 141, 75%), whereas 27 studies (14%) used two. The majority of studies (n = 115, 61%) used nonprobability, non-population-based sampling designs, followed by probability sampling (n = 31, 17%), purposive or targeted sampling (n = 27, 14%), population sampling/census data (n = 16, 9%), and nonprobability, population-based sampling (n = 5, 3%). Eleven studies (6%) did not state their sampling design, eight (4%) were reviews, and one (0.5%) had varying samples across surveys (Table 1).
Summary of Study Characteristics
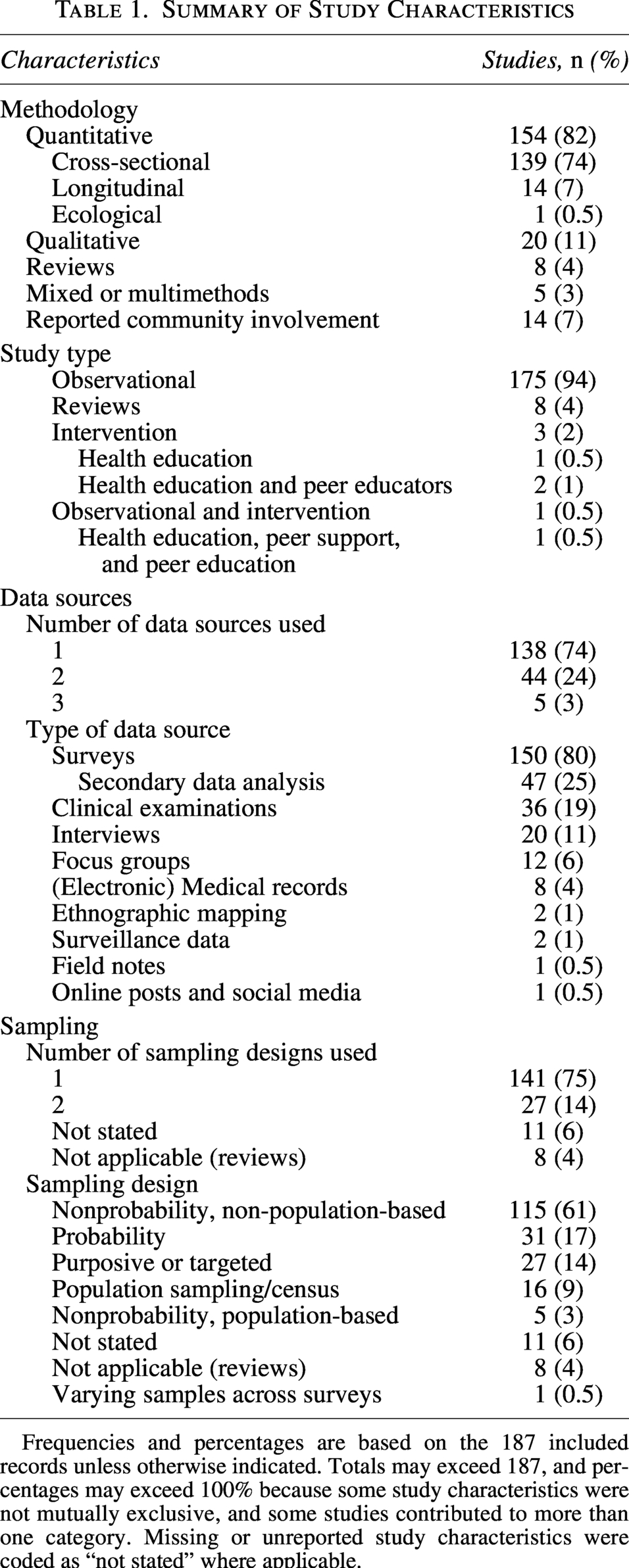
Frequencies and percentages are based on the 187 included records unless otherwise indicated. Totals may exceed 187, and percentages may exceed 100% because some study characteristics were not mutually exclusive, and some studies contributed to more than one category. Missing or unreported study characteristics were coded as “not stated” where applicable.
Language used to describe SMW
The included studies used a variety of words to describe SMW; “bisexual” was the most common (n = 130, 70%), followed by “lesbian” (n = 118, 63%). Further, 60 studies (32%) used “women who have sex with women,” and 32 (17%) used the word “gay” to describe SMW. Figure 4 visually illustrates the frequency of SMW words used.
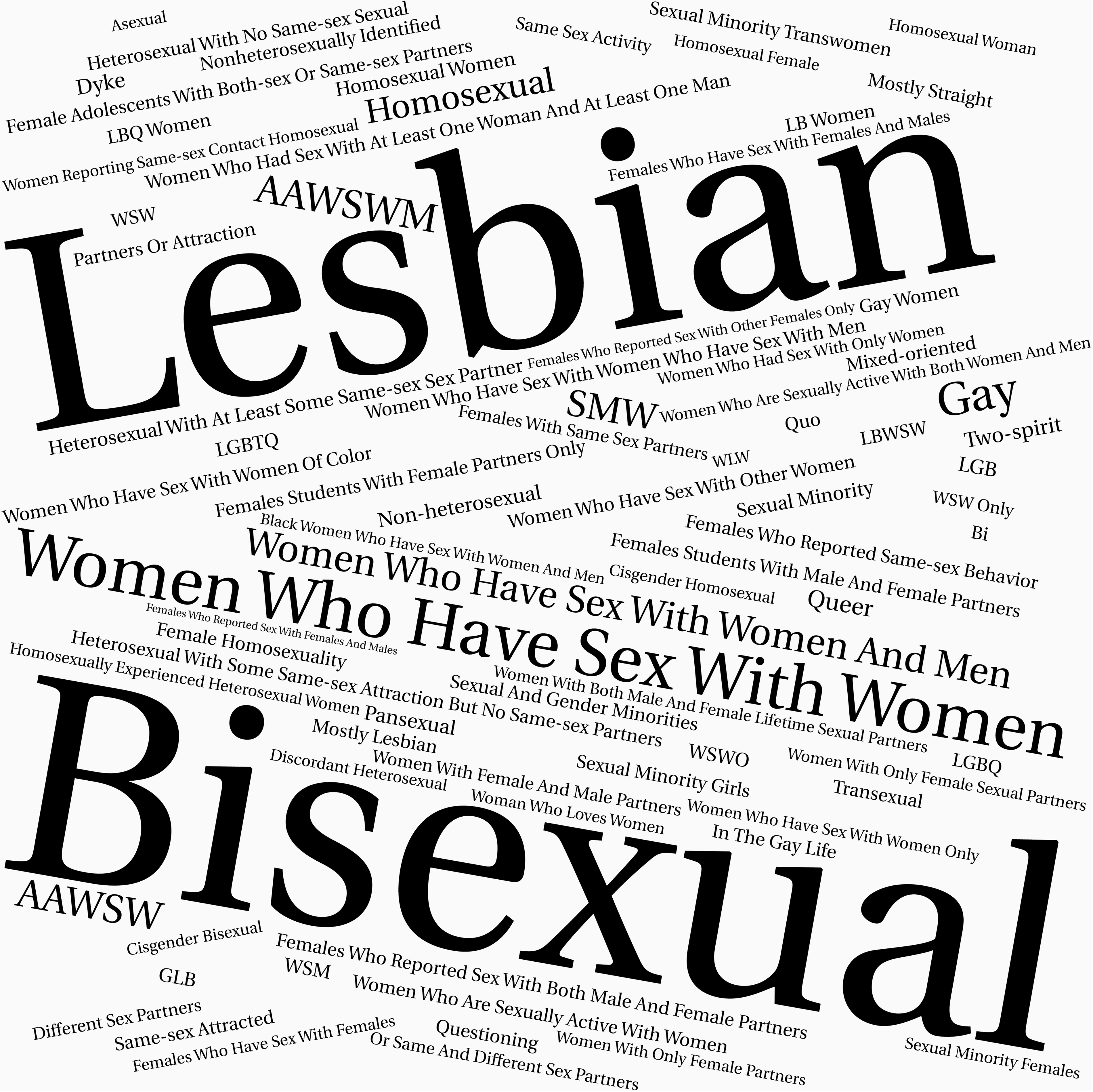
Word cloud of language used to describe sexual minority women (sub)samples by frequency; larger words were used most often.
SMW (sub)sample: Sociodemographic characteristics
SMW sample sizes
SMW (sub)sample sizes were reported by 169 studies (90%). SMW participants comprised the entire sample in 46 studies (25%) and most of the sample (between 50% and 83%) in 10 studies (5%). For the remaining studies, SMW participants comprised the sample minority, with 44 studies (24%) having <10% of their total. Participant sample size was not applicable to nine studies (5%) as they were reviews (n = 8) or based on social media posts (n = 1). Further, nine studies (5%) did not report the SMW (sub)sample size. An analysis of studies that included 50% or more SMW in their sample showed no clear trends in terms of publication year, geography, methodological approach, or study focus.
Sexual orientation
Among included studies, 128 (68%) reported detailed sexual orientation data among their SMW (sub)sample. Seventy-nine studies (42%) measured identity to characterize and report sexual orientation data, 30 studies (16%) used both identity and behavior, and 19 studies (10%) used only behavior. Further, five (3%) also used attraction to characterize sexual orientation.
Studies that operationalized sexual orientation by identity included participants who were bisexual (n = 92, 49%), lesbian (n = 86, 46%), gay (n = 29, 16%), heterosexual/straight (n = 20, 11%; reported having sex with other women), homosexual (n = 18, 10%), queer (n = 13, 7%), and those of another sexual orientation (n = 41, 22%; e.g., unsure, unidentified, pansexual, Two Spirit, same-gender-loving, asexual, dyke).
SMW (sub)populations operationalized with behavior data include WSW (n = 29; 16%) and WSWM (n = 29; 16%). Four studies (2%) included women who have sex with men only (identified with an SMW identity). Further, 12 studies (6%) defined their population based on recency of same-sex behavior, three (2%) used a sexuality spectrum, and four (2%) described same-sex behavior using alternative terminology (e.g., “homosexually experienced heterosexual,” “same-sex partners”).
Race/Ethnicity
Only 98 (52%) studies reported the racial and/or ethnic characteristics of SMW (sub)samples. Eighty-one studies in our sample included Black or African American participants (43%), 73 included White, Caucasian, or European American participants (39%), 58 included Hispanic/Latinx participants (31%), 36 included Asian or South Asian participants (19%), 30 included American Indian, Alaska Native, Native American, Aboriginal, or Torres Strait Islander participants (16%), 18 included Biracial/Multiracial participants (10%), and 9 included Native Hawaiian or Pacific Islander participants (5%).
Further, 58 (31%) studies included participants of another race/ethnicity. In most of those cases (n = 42, 22%), studies just listed “Other” for participant race/ethnicity, with no further details. However, 16 studies (9%) in this category used categories that fell outside our framework. These included studies that reported having “non-White” participants without providing further information (n = 6; 3%), “non-Aboriginal” participants (n = 3; 2%; conducted in Australia), participants of Jewish descent (n = 2; 1%), “Colored” participants (n = 2; 1%; conducted in Botswana, Namibia, South Africa, and Zimbabwe), and participants classified as Middle Eastern (n = 1; 0.5%), African Caribbean (n = 1; 0.5%), and “Mulatto” (n = 1; 0.5%; conducted in Brazil).
Age
Among the studies that reported SMW (sub)sample age (n = 98, 52%), reporting method varied, including: mean age (n = 60; 32%), age groups (n = 26; 14%), age range (n = 25; 13%), median age (n = 10; 5%), and another age measurement (n = 8; 4%). Further, 74 studies (40%) included only adults (
Key findings
The included studies covered diverse HIV-related findings (Table 2). Across topics, most studies reported overall prevalence among SMW and frequently conducted comparative analyses between SMW and other groups (e.g., heterosexual women, men) and sometimes between SMW (sub)groups.
Summary of Findings Regarding HIV and Sexual Minority Women, Globally
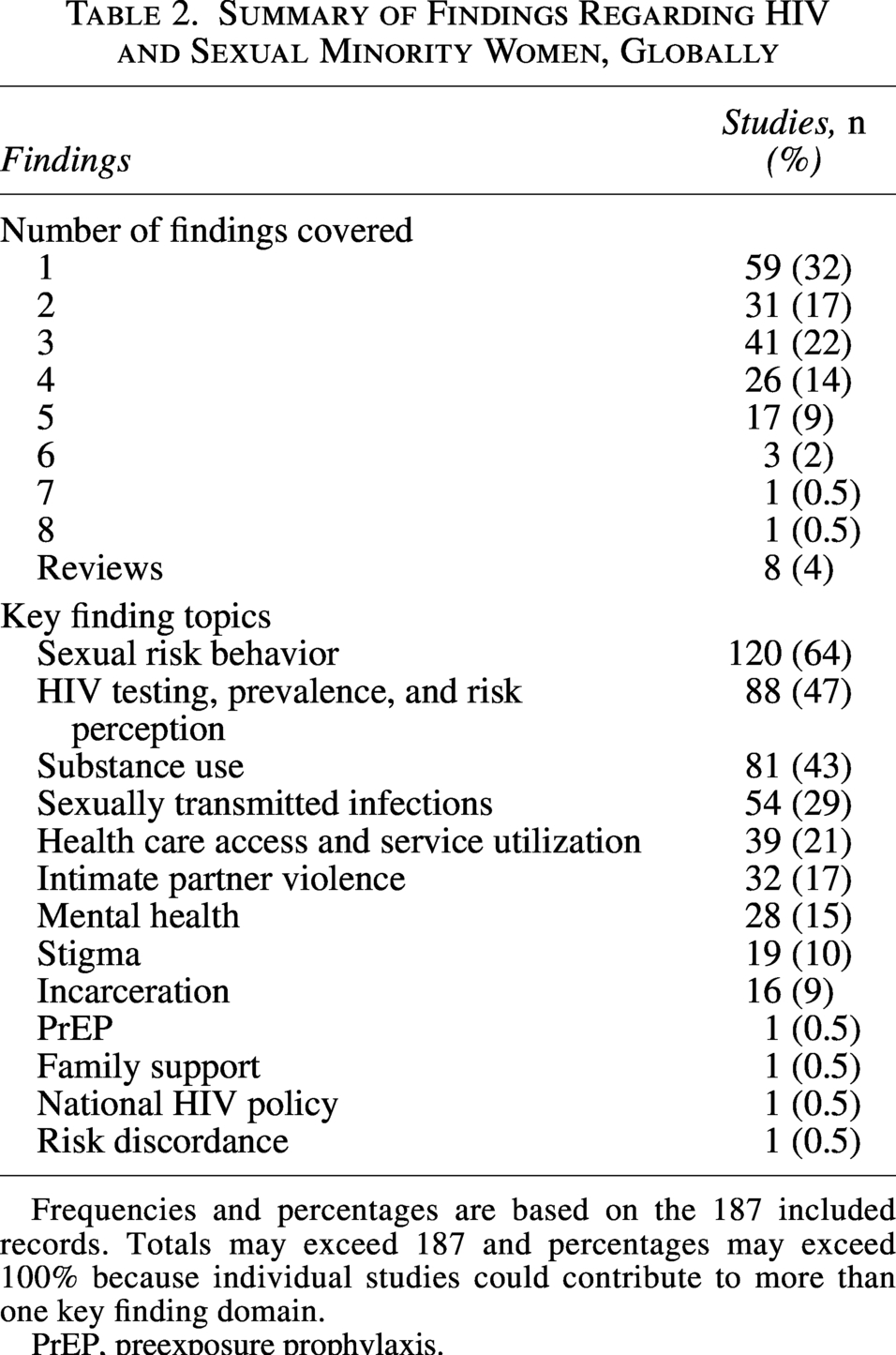
Frequencies and percentages are based on the 187 included records. Totals may exceed 187 and percentages may exceed 100% because individual studies could contribute to more than one key finding domain.
PrEP, preexposure prophylaxis.
Most studies reported findings related to sexual risk behaviors (n = 120; 64%), consistently describing variation in partnership patterns among SMW, including partner gender, partner number, concurrency, relationship duration, and diverse barrier use practices.2,5,19,23,25,46,47,74,77,78,81,82,86,87,91,94–96,102,104–106,109–111,113–117,119,121–128,130–143,145,148–150,152,154–157,159,161–168,171–175,177,179,183,186–193,196,199–203,205–209,211–213,215–222,224–228,231–234,237,240 Compared with heterosexual women, SMW (particularly bisexual and WSWM) were often reported to have higher partner counts, greater exposure to partners with elevated HIV/STI vulnerability, higher rates of concurrency, and, in some studies, more casual or short-term partnerships. Barrier use was frequently inconsistent (and often absent), with wide variation across studies; qualitative findings indicated that trust, relationship context, and gaps in inclusive sexual health education shaped protection decisions more than formal risk assessment. Across studies, elevated risk behaviors frequently co-occurred with structural vulnerabilities such as stigma, violence, and substance use.
Eighty-eight studies addressed HIV testing, prevalence, and risk perception among SMW (47%).5,23,25,33,46,47,69–73,76,79,82,83,87,89,91,95,97,99,104–107,109,110,113,115,117,118,121,127–131,134–138,141–143,145,148,150,156–159,161,166–171,173,175,176,178,184,185,188,190,193,196–199,201,205–208,212–218,222,229,233,240 HIV testing was generally high; SMW, particularly bisexual and WSWM, often reported higher testing engagement than heterosexual women, although disparities persisted by race and geography. SMW perceived themselves at low or no risk for HIV; several studies documented a disconnect between behavioral exposure (e.g., high partner counts) and perceived vulnerability. A few studies discussed HIV fear-driven testing avoidance and unequal access to HIV education.
Eighty-one studies covered substance use (43%), consistently reporting elevated alcohol and drug use among SMW compared with heterosexual women, although patterns varied substantially by subgroup.5,23,25,74,75,77,78,81,82,85,87,89,94–96,98,99,104,105,110,111,115,118,120–123,125,126,128–130,132,135,137,140–143,145,148,152,156,157,163,164,171,173,175–177,181,183,184,186–188,190,196,197,199–202,205,208–210,212,213,215–217,219–221,224,227,229,231,238 Heavy drinking, injection drug use, and noninjection drug use were frequently concentrated among bisexual women, WSWM, and racially and economically marginalized SMW. Across substances, qualitative and quantitative findings linked substance use to intersecting vulnerabilities (e.g., violence exposure, incarceration, unstable housing) and to sexual risk contexts; drugs and alcohol shaped partner dynamics and protection decisions.
Fifty-four studies discussed STIs (29%), showing wide variation in prevalence across infections, and consistent disparities between SMW subgroups.5,25,46,71,72,76,79,81,82,106,111,115,116,121,126–128,130,135,136,142,143,149,150,157,158,163,164,168,171,173,176,177,180,182,184,190,193,199,200,204–206,208,212,214,215,222,229–231,233,234,240 Bisexual women and WSWM were more likely than lesbian women and WSW to report bacterial and viral STI experiences, and to have partners with known STI histories; SMW experiencing racial, economic, or violence-related marginalization were the most impacted. STI screening and vaccination uptake were reported across studies but varied widely, with subgroup comparisons producing mixed findings.
Thirty-nine studies addressed health care access (21%), showing inequities among SMW that were strongly shaped by stigma rather than insurance or provider availability.5,33,71,76–80,99,115,117,127,131,132,134,135,137,143,147,148,150,153,157,159,160,170,173,190,193,194,211,212,229,233,236,238,240–242 Although many studies reported high rates of insurance coverage and primary care access, utilization of routine preventive services varied widely, and lesbian women/WSW were often less likely to receive routine testing (e.g., STIs, Papanicolaou), mental health counseling, or contraceptive services than their bisexual and heterosexual counterparts. Across studies, fear of discrimination, provider heteronormativity, and confidentiality concerns consistently discouraged disclosure and health care engagement. The findings indicate that structural barriers, not just individual behavior, constrained where and how SMW received care.
Thirty-two studies discussed intimate partner violence (IPV; 17%), consistently showing elevated exposure to violence (e.g., sexual assault, physical abuse, childhood abuse) among SMW relative to heterosexual women.5,23,71,72,77,78,93,96,99,100,108,123,125,126,128,148,163,170,171,177,183,186,194,196,197,200,212,213,221,222,224,235 Reported prevalence frequently exceeded one-third of participants, with bisexual/WSWM participants often facing the highest burden. Violence also included coercive control, emotional abuse, and social isolation, underscoring the relational and structural nature of risk. The single intervention study suggested that SMW-specific programming improved engagement.
Mental health topics were reported by 28 studies (15%), showing consistently worse depression, distress, anxiety, suicidality, and psychiatric hospitalization outcomes among SMW compared with heterosexual women.25,87,89,90,94,96,97,99,100,118,121,123,138,140,141,148,149,169,176,184,195,197,200,212,227,229,231 Depression and distress studies showed that bisexual women experienced the greatest burden, whereas studies concerning suicidal ideation and suicide attempts showed that transgender SMW faced particularly elevated risk. Across studies, mental health disparities were connected with substance use, violence exposure, and structural marginalization.
Nineteen studies addressed stigma (10%), which shaped both risk and care access for SMW.2,70,77,78,88,139,146,147,149,150,156,170,191–193,212,234,238,242 Studies documented specific manifestations of sexuality-related stigma, including antibisexual discrimination, lesbian stigma, and SMW invisibility in sex education, with many SMW reporting direct discrimination experiences. HIV-related stigma was linked to avoidant coping and compounded vulnerability through intersecting marginalizations. One study emphasized resilience, arguing that prevention efforts should build on SMW strengths rather than focus solely on risk.
Sixteen studies reported SMW incarceration experiences (9%), with descriptive analyses indicating that a substantial proportion of SMW had prior arrests or jail.5,25,30,68,105,121,123,128,130,145,152,156,163,171,209,212 Comparative analyses consistently showed higher incarceration among SMW than heterosexual women; bisexual women were the most impacted. Qualitative findings described incarceration intersecting with relationship dynamics and sexual networks, including the maintenance of existing partnerships, the formation of new or concurrent relationships during incarceration, and, in some cases, the simultaneous incarceration of partners.
One study (0.5%) covered each of the following: preexposure prophylaxis (PrEP), 132 family support, 84 national HIV policy, 103 and risk perception discordance. 144 Notably, no studies focused on antiretroviral therapy (ART), vaccine trials, or explicitly strengths-based factors.
Discussion
This is the first global scoping review, to our knowledge, to systematically identify and synthesize scientific literature regarding the state of HIV research, inclusive of SMW. Other reviews related to SMW and HIV have been broader in terms of population (e.g., LGBTQ+ people), 243 restrictive in time period, 4 focused on a specific location,112,170 sexual health-related but not HIV-specific, 34 or have focused on specific health outcomes that may be HIV-related, but were not conducted in an HIV context.239,244
Our review identified 187 studies, most of which were conducted in the United States and utilized quantitative methods, most commonly cross-sectional designs, using survey data obtained via nonprobability, non-population-based convenience sampling methods. Overwhelmingly, studies did not report community engagement in the research process. Only about a quarter of studies focused exclusively on SMW. Publications show an upward trend over time. Inclusion of demographic data on SMW (sub)samples varied; about half of the studies reported on age and race, and about two-thirds reported on sexual orientation, limiting the potential for disparity analyses. Study foci ranged, with most research centering on sexual risk behavior and HIV testing, prevalence, and risk perception. Our review offers insights on a range of key methodological and topical gaps in the current literature related to SMW HIV risk, which can inform future research and practice efforts to improve HIV-related outcomes among SMW.
Although our final sample of included studies (n = 187) can seem considerable, the breadth of HIV literature related to other populations puts this number into perspective. Our search included all studies, anywhere, since the beginning of the epidemic (40+ years), related to HIV and SMW. In contrast, a systematic review of HIV testing and incidence among men who have sex with men (MSM) in Africa included 152 studies, comparable with our final sample, despite their more restrictive inclusion criteria (e.g., 2005–2023; Africa only). 245 An HIV prevalence systematic review among MSM in China included 355 studies, nearly double our sample, again despite restrictive inclusion criteria (e.g., 2001–2018; China only). 246 Given the vastness of the HIV literature, the epidemic status of HIV globally, and the heightened yet invisibilized risk among SMW, our comprehensive review highlights a critical need for increased HIV research among SMW.
The included studies commonly focused on sexual risk behaviors, HIV epidemiology, and substance use; a minority of studies focused on structural factors (e.g., stigma, incarceration) despite known association with HIV vulnerability.247,248 Findings across domains indicate consistently poorer outcomes among SMW when compared with heterosexual women, with disproportionate impacts on bisexual women and WSWM relative to lesbian women and WSW. Disparities also persisted for racially and economically marginalized SMW. Across domains, vulnerabilities commonly co-occurred and were shaped by sociostructural factors rather than isolated behaviors. Notably, no studies included SMW-inclusive research on ART or vaccine trials, only one focused on PrEP, and intervention studies were limited, despite the critical role of PrEP 249 and ART in HIV prevention and treatment. 250 Additional underrepresented topics include HIV prevention education, sociostructural interventions, living with HIV, resilience and strength-based factors, and social determinants of health. Our findings offer a research agenda roadmap.
The geographic representation of included studies shows a strong bias toward North American research. Few studies were conducted in Latin America, Africa (outside of Southern Africa), Europe, or Asia. However, global data highlight that HIV infection rates among women remain disproportionately high across contexts, with persistent disparities between (sub)groups of women. For instance, HIV incidence is decreasing slower for young women compared with men in Sub-Saharan Africa; HIV infections among transgender women are increasing in Latin America, Eastern Europe, and Central Asia; treatment coverage for HIV is especially low for women in the Middle East and Northern Africa; and overall acquired immunodeficiency syndrome (AIDS)-related deaths increased among women in Central America, whereas it decreased for the overall population. 251
The lack of diverse geographic research pertaining to (sub)groups of women is likely related to bias and stigma in both Western and non-Western countries. It can partially be accounted for by our neo-colonial global order and its associated socioeconomic power imbalances, which center the Global North 252 ; research agenda setting in Western nations, where most of the work and funding currently originate, may insufficiently allocate resources to SMW research. 253 This is especially salient in the current moment, when the U.S. federal government is systematically defunding LGBTQ+ research. 254
Sexuality-related stigma, rooted in homophobia and misogyny, is also operating within the Global South and may contribute to limited geographic diversity within SMW research; agenda setters and gatekeeper biases may prevent this research. 255 Further, in contexts where societal-level biases and stigmas persist, respondents may be reticent to participate in available studies or share sexual orientation data due to anti-LGBTQ+ policies and cultural norms. 256 Funding limitations for LGBTQ+ research in these locations could explain this underrepresentation. The lack of SMW-focused research in these highly impacted regions highlights an important literature gap and urgent need for investigations that consider regional and cultural contexts.
HIV studies with SMW have increased over time, potentially reflecting growing recognition of the need for this research. However, there was a notable drop in publications in 2021, potentially due to the impact of the COVID-19 pandemic, which disrupted research activities and diverted funding away from HIV-related research.257,258 Although an increase in studies over time suggests progress, the current body of literature remains insufficient to address the diverse needs of SMW globally.
A quarter of the studies included in this review focused exclusively on SMW populations. Among studies inclusive of but not focused on SMW, SMW participants comprised a minority of the sample. Demographic data of SMW (sub)samples were also lacking, making cross-study analyses difficult, especially in terms of examining (sub)group nuances, and limiting the possibility for intersectional analyses, even if using individual-level factors as proxies for structural forces. Although this review uses SMW as an umbrella term, we emphasize the importance of future research to disaggregate findings by SMW (sub)groups (e.g., lesbian women, bisexual women, WSW, WSWM) and to clearly define the populations under study. Additional health disparity analyses between SMW (sub)groups (e.g., defined by race, gender, or sexual orientation) are needed to better understand intersectional dimensions of HIV vulnerabilities and to inform responsive interventions.
Our review highlighted key methodological gaps in the existing literature. The overwhelming use of cross-sectional survey-based designs with convenience sampling provides an important orientation to relevant issues but limits finding generalizability. Future quantitative research should prioritize more complex designs, including longitudinal studies to investigate SMW HIV risk and outcome evolution over time, as well as more sophisticated sampling strategies to facilitate greater generalizability. In addition, future research could utilize pooled data or meta-analyses to derive insights across studies.
Although quantitative studies provide important prevalence and incidence data, qualitative approaches can offer deeper insights into barriers to care, stigma experiences, and structural factors influencing HIV risk. Qualitative research is underrepresented in this review, yet is essential for capturing the lived HIV risk, prevention, and care experiences of SMW. Further, there is a need for intervention studies to provide HIV-related and other support to SMW. Finally, SMW community-engaged research approaches are necessary to ensure relevant, accurate, and meaningful findings are generated.
In many instances, studies did not report important methodological factors (i.e., level of community engagement, sexual orientation operationalization). Although relevant data to describe study results and journal reporting requirements vary, this information is critical to contextualize the field and move toward better public health research practices. Taken together, the findings highlight the need for the establishment and adoption of transparent research implementation and reporting guidelines for SMW studies, similar to those developed for specific populations (e.g., transgender populations 259 ), study designs (e.g., PRISMA-ScR for scoping reviews, 60 Consolidated Standards of Reporting Trials for randomized controlled trials 260 ), and specific fields (e.g., Strengthening the Reporting of Observational Studies in Epidemiology for epidemiology 261 ).
Limitations
Our scoping review has some limitations. First, all searches potentially miss eligible articles; relevant articles may have been excluded because they were published in a language other than English. Further, we focused on peer-reviewed empirical publications, which omitted “gray literature” (e.g., doctoral dissertations, practice guidelines, government reports). Second, our choice to summarize the literature under the umbrella SMW term limits nuanced takeaways concerning (sub)group nuances. However, given the range of ways in which authors label and define SMW (sub)groups, and the goal of this scoping review, this choice still provided high-level summary data on the existing literature.
Conclusion
This scoping review of 187 studies provides insights into the current body of peer-reviewed, English language global research concerning SMW and HIV. We include an overview of study characteristics and research foci, offering rich insight into existing knowledge and highlighting key methodological and topical gaps. Specifically, further research on structural, level factors and biomedical interventions among SMW is needed. Expanding research efforts beyond North America should be prioritized, particularly in regions highly impacted by HIV, where SMW remain understudied. This research should include qualitative and quantitative approaches, with strengths-based lenses. Finally, the establishment of transparent and standardized procedural and reporting guidelines for SMW studies would enhance the comparability and utility of future research. Our study supports a need for increased resources for research and practice that focus on the unique HIV-related health strengths and vulnerabilities of SMW. These findings can inform future research agendas, policy development, and targeted public health interventions to help improve HIV-related outcomes for SMW globally.
Authors’ Contributions
J.L.G.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, and writing—original draft. M.S.: Data curation, formal analysis, investigation, project administration, visualization, and writing—review and editing. F.M.W.: Data curation, formal analysis, investigation, visualization, and writing—review and editing. M.N.: Data curation, formal analysis, investigation, visualization, and writing—review and editing.
Ethical Considerations
This study was a scoping review of published literature and did not involve human participants or primary data collection. As such, ethics approval was not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Data Availability
All data in this article are available on request to the corresponding author. No restrictions will be applied.
Footnotes
Acknowledgments
The authors thank Rebecca Fowler for her support in the early stages of this project, Lori Rosman for her technical support in developing and running the search, Katherine Banchoff for her support with data abstraction, Sara Malley for her support on early drafts of ![]() , Leanne Zhang for her academic editing, and Matthew Folse for expert support with reference formatting and citation review. The authors also thank the authors of the included studies and the women who participated in them.
, Leanne Zhang for her academic editing, and Matthew Folse for expert support with reference formatting and citation review. The authors also thank the authors of the included studies and the women who participated in them.
Declaration of Conflicting Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Statement
This publication resulted, in part, from research supported by the NIH/NIDA (
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.