
Abstract
Purpose:
This study examined factors associated with Italian healthcare practitioners’ clinical skills when working with lesbian, gay, bisexual, transgender, and queer (LGBTQ) patients across primary, sexual and reproductive, and mental health domains.
Methods:
A cross-sectional sample of 165 practitioners completed measures assessing clinical skills, heteronormative beliefs, and prejudice against sexual and gender diversity, along with sociodemographic and professional variables, between May 2024 and June 2025.
Results:
Participants (44 assigned male at birth, 121 assigned female at birth; mean age = 39.3 ± 11.4 years; 163 cisgender, 2 nonbinary; 49 identifying as LGBTQ) yielded significant differences across healthcare domains: primary care practitioners reported lower overall clinical skills, more negative attitudes and prejudice than mental health practitioners, as well as the lowest attendance at LGBTQ specific training among groups. Across the whole sample, greater clinical skills were associated with lower heteronormative beliefs and prejudice, attendance at LGBTQ training, and having at least one LGBTQ person among friends or relatives.
Conclusions:
These findings underscore the need for comprehensive educational interventions aimed at enhancing both knowledge and attitudinal components of LGBTQ clinical skills. Policy efforts should prioritize mandatory, experiential, and context-specific training programs and promote inclusive guidelines to reduce heteronormativity in Italian healthcare. Strengthening practitioners’ LGBTQ clinical skills can foster more equitable, compassionate, and accessible health services across all domains of care.
Introduction
Lesbian, gay, bisexual, transgender, and queer (LGBTQ) individuals consistently report poorer health outcomes than their heterosexual and cisgender counterparts across multiple healthcare settings. In primary care, they face higher risks of cancer,1,2 cardiovascular,3,4 respiratory,5,6 diabetes, 7 and other chronic illnesses.8,9 For instance, a 2022 press release from the Italian National Institute of Health 10 reported that in Italy, where the present study was conducted, only 20% of transgender individuals assigned female at birth undergo Pap tests for preventive cancer screening, compared to 79% of women in the general population.
Similarly, in the sexual and reproductive healthcare domain, LGBTQ populations report significantly higher rates of sexually transmitted infections. For example, lesbian, gay, bisexual, and transgender adults and youths reported higher rates of sexual transmitted infections than heterosexual and cisgender individuals.11,12 Specifically concerning transgender and nonbinary adults, lower cervical and prostate cancer screening rates are observed among those assigned female and male at birth, respectively.13,14 In mental health, elevated rates of depression, anxiety, suicidality, and substance-related problems have been reported by LGBTQ youths 15 and adults,16,17 with these disparities observed across diverse identities, age groups, and contexts. 18
Despite the enhanced risk for several health issues among different healthcare contexts, LGBTQ youths and adults access health services less frequently than the general population due to several social determinants of health, including socioeconomic status, education, employment conditions, and housing stability,19–22 as well as structural and interpersonal barriers.23,24 Structural barriers refer to systemic and institutional obstacles that limit LGBTQ individuals’ access to adequate healthcare, including high uninsured rates, lack of coverage for LGBTQ specific services, and limited availability of providers offering LGBTQ informed care. Interpersonal barriers include obstacles emerging within direct interactions between LGBTQ individuals and healthcare professionals, staff, or others involved in care.
Such barriers are often characterized by prejudice, discriminatory behaviors, negative attitudes, and insufficient cultural competence on the part of healthcare providers. These factors further hinder LGBTQ individuals from accessing health services due to the anticipation of stigmatizing interpersonal patterns.25,26 In the Italian context, where the present study was conducted, research documents shortages of providers, gaps in clinical knowledge about LGBTQ-specific needs, experiences of homophobic and transphobic discrimination, and lower levels of cultural compassion, all of which limit access to appropriate services.27–34
The Health Equity Promotion Model (HEPM) 35 offers a multidimensional framework for understanding LGBT health that goes beyond deficit-based views. Integrating behavioral, social, psychological, and biological pathways, it emphasizes how health trajectories are shaped by structural conditions, individual resources (e.g., healthy/unhealthy behaviors, rich/poor social networks, positive/negative identity management, adaptive/disadaptive coping strategies), and intersecting social positions (e.g., age, ethnicity, gender identity, socioeconomic status). The model highlights both risk and resilience processes—acknowledging that, alongside the harms of stigma and discrimination, LGBTQ communities cultivate coping strategies and supportive networks that promote well-being.
Expanding on the Minority Stress Model36,37 and the Psychological Mediation Framework, 38 the HEPM adopts an intersectional and life course perspective that addresses previous models’ tendency to overpathologize LGBTQ experiences and overlook resilience and structural influences. The HEPM offers a useful framework for understanding how healthcare professionals can either reinforce or reduce health inequalities. By acknowledging that LGBTQ health is influenced by structural and interpersonal factors, the model underscores clinicians’ role as agents of equity. This involves not only mitigating risks but also promoting resilience and inclusion through culturally competent care, respectful communication, and advocacy for systemic change.
Discriminatory practices in healthcare may be intentional or unintentional, often reflecting heterosexist or cisnormative assumptions.39–44 In this vein, in addition to heteronormativity, healthcare environments may also be influenced by binary social norms that assume the existence of only two discrete, biologically determined, and mutually exclusive genders aligned with sex assigned at birth. Such binary frameworks can marginalize transgender, nonbinary, and gender-diverse individuals by rendering their identities unintelligible within standard clinical categories and documentation systems. 45 These norms may subtly inform clinical interactions, intake procedures, and communication styles, reinforcing exclusion even in the absence of overt prejudice.46,47
Moreover, many practitioners lack awareness of LGBTQ individuals’ needs, partly due to insufficient training; sociodemographic factors—such as age, sex assigned at birth, LGBTQ identification, and having LGBTQ friends or relatives—may also shape attitudes and knowledge.48,49 These gaps can function as barriers to care for LGBTQ people, sustaining persistent disparities. In this vein, the Culturally Competent Compassion Model, 50 as adapted for LGBT populations, 27 highlights how gaps in clinical skills among healthcare professionals can reduce LGBTQ patients’ likelihood of seeking care. Papadopoulos 50 defines culturally competent compassion as the human capacity to recognize others’ suffering and address it through interventions that are sensitive to individuals’ cultural beliefs, behaviors, and needs. This approach can be fostered in healthcare and social care professionals via targeted training to improve both understanding and practical clinical skills.
Building on these premises, the present study examined Italian healthcare practitioners’ clinical skills in working with LGBTQ patients across primary care, sexual and reproductive health, and mental health domains, and explored the factors associated with such skills. As previously reported, 51 clinical skills can be conceptualized as an umbrella construct encompassing three core components identified across major health and mental health professional guidelines. These include clinical preparedness (i.e., the practical ability and confidence to provide appropriate care), attitudes (i.e., awareness and management of personal and societal biases toward LGBTQ individuals), and knowledge (i.e., familiarity with relevant psychosocial and health issues). Together, these dimensions reflect the competencies considered necessary to deliver ethical, effective, and culturally responsive care to LGBTQ patients.
In the present study, sociodemographic (age, sex assigned at birth, LGBTQ identity, contact with LGBTQ friends or relatives), clinical (years of experiences, attendance at LGBTQ-focused trainings), and attitudinal variables (heteronormative beliefs, prejudice toward sexual and gender diversity) were investigated as potential correlates of participants’ clinical skills. Based on prior research,48,49,52 it was hypothesized that practitioners from different healthcare domains would differ in clinical skills and attitudes, with mental and sexual and reproductive health providers showing higher competence and more affirmative attitudes than those in primary care. Moreover, stronger heteronormative beliefs and prejudice were expected to correlate negatively with clinical skills, whereas LGBTQ identity, personal contact with LGBTQ individuals, and prior LGBTQ-specific training were hypothesized to be positively associated.
Methods
Participants and procedure
A cross-sectional sample of 165 practitioners working in primary, sexual and reproductive, and mental health care was recruited. This study received ethical approval on May 15th, 2024 from the Ethical Committee of the University of Naples “Federico II” (protocol no. 10/2024) and the Territorial Ethics Committee Lazio Area 2 (protocol no. 197.24 CET2 utv) and was conducted in accordance with the EU General Data Protection Regulation. Participation was voluntary and could be discontinued at any moment. All participants were required to provide informed consent prior to participation. Written informed consent was obtained from all participants. Eligible participants had to meet the following criteria: working as a healthcare practitioner; being at least 18 years of age; residing in Italy; and having a fluent comprehension of the Italian language.
Data collection took place between May 2024 and June 2025 using an online survey hosted on the Qualtrics platform. Recruitment was conducted nationwide across Italy through multiple channels, including posts on social media groups and professional networks (e.g., Facebook, Instagram), institutional outreach within the National Health System, and snowball sampling through professional contacts. For the institutional outreach, major national scientific societies and professional associations representing healthcare professionals in primary care, sexual and reproductive health, and mental health were identified. The Principal Investigator contacted these organizations via email, outlining the main aims of the study and providing the survey link, with a request to disseminate it among their members.
To protect participants’ privacy and maintain voluntary participation, no formal feedback was requested regarding which associations ultimately distributed the link or which members completed the survey. No directly identifiable personal data were collected; although sociodemographic and professional information was obtained, responses were recorded without personal identifiers and analyzed in aggregate form in accordance with data protection regulations. Participation was voluntary, and respondents completed the questionnaire individually.
Measures
Sociodemographic and clinical activity information. Sociodemographics and clinical activity information were collected through an ad-hoc questionnaire. Sociodemographic information included age, sex assigned at birth (i.e., female, male, or other), gender identity (i.e., cisgender male, cisgender female, transgender male, transgender female, nonbinary, and other), sexual orientation (i.e., heterosexual, gay, lesbian, bisexual, other), LGBTQ identity (i.e., yes, no), ethnicity (i.e., White [Caucasian, European], Black or Afro-American, Hispanic or Latin, Asian, and other), relationship status (i.e., single, in a relationship, cohabiting partner, married, separated, divorced, widowed, and other), mean annual income (i.e., less than 15,000€, between 15,000€ and 28,000€, between 28,001 and 50,000€, ≥ 50,001€), and known LGBTQ persons among personal relationships (i.e., none, at least 1). Collected clinical activity information included professional experiences (i.e., less than 1 year, between 1 and 5 years, between 5 and 10 years, between 10 and 20 years, more than 20 years), having previously treated LGBTQ patients (i.e., yes, no, it is possible that I was not aware of their sexual orientation and/or gender identity), and having attended trainings on specific LGBTQ issues and needs (i.e., yes, no).
Clinical skills. The Lesbian, Gay, Bisexual, and Transgender Development of Clinical Skills Scale (LGBT-DOCSS) 51 is a self-report questionnaire composed of 18 items on a 7-point Likert scale, from 1 (strongly disagree) to 7 (strongly agree). The LGBT-DOCSS was translated into Italian using a back-translation procedure. The original items were translated into Italian and then independently back-translated into English by bilingual researchers. Discrepancies were discussed and resolved to ensure semantic and conceptual equivalence with the original instrument. The questionnaire measures practitioners’ Clinical Preparedness, Attitudes, and Basic Knowledge, as well as a clinical skills total score. Cronbach’s α for Clinical Preparedness, Attitudes, Basic Knowledge, and the Total score were 0.85, 0.80, 0.73, and 0.79, respectively.
Heteronormative beliefs. The Heteronormative Attitudes and Beliefs Scale (HABS) 53 is a self-report questionnaire composed of 16 items on a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), composed of two subscales: Essential sex and gender, assessing individuals’ beliefs that only two sexes exist corresponding exclusively to a matching gender; and Normative behavior, assessing attitudes toward stereotypical male and female roles. Cronbach’s α was 0.86 for the Essential sex and gender scale, and 0.80 for the Normative behavior scale.
Prejudice against sexual and gender diversity. The Prejudice Against Sexual and Gender Diversity Revised (PASGD-R) 54 is a unidimensional self-report measure composed of 18 items on a Likert scale ranging from 1 (completely in disagreement) to 5 (completely in agreement); it evaluates individuals’ explicit and subtle prejudices against lesbian, gay and bisexual orientations, trans identities and gender nonconformity. The PASGD-R was translated into Italian following a back-translation procedure. After the initial translation, an independent bilingual researcher performed a back-translation into English, and any inconsistencies were reviewed and reconciled to preserve the meaning of the original items. The scale yielded a Cronbach’s α of 0.92.
Data analysis
Analyses were conducted using the jamovi software (version 2.4.11) and the GAMLj3 statistical package. Group differences on sociodemographic, clinical information, and study variables were tested via chi-square for categorical and analyses of variance for continuous variables. Multivariate analyses of variance (MANOVAs) were planned to be run to assess the main effects of and the interaction between group and sociodemographic variables that yielded significant differences, on clinical skills, heteronormative beliefs, and prejudice against sexual and gender diversity as dependent variables. For MANOVAs, effect sizes were calculated as partial eta-squared, and pairwise comparisons were Bonferroni-corrected.
To assess which factors are associated with practitioners’ clinical skills in working with LGBTQ patients, bivariate correlations (Pearson’s r, 2-tailed) were run between study LGBT-DOCSS, HABS, and PASGD-R in the entire sample. In addition, a general linear model was implemented with the LGBT-DOCSS total score as the dependent variable, and Group, heteronormative beliefs, and prejudice against sexual and gender diversity as independent variables. Participants’ age, sex assigned at birth, LGBTQ identity, known LGBTQ persons, and attendance at LGBTQ trainings were also included in the model.41,42
Results
Primary health practitioners included 11 nurses, 14 neurologists, 13 dentists, 4 preventive medicine specialists, 7 pediatricians, 3 anesthetists, 6 internal medicine specialists, 1 physiotherapist, 1 geriatrician, 1 oncologist, 1 gastroenterologist, 1 pulmonologist, 1 food science specialist, 1 plastic surgeon, 1 rehabilitative medicine specialist, 1 emergency physician. Sexual and reproductive practitioners included 1 urologist, 9 gynecologists, 5 endocrinologists. Mental health practitioners included 67 psychologists/psychotherapists, 4 child neuropsychiatrists, 12 psychiatrists. Table 1 displays complete participants’ characteristics. Group comparisons are reported in Table 1.
Group Descriptives and Differences on Sociodemographic, Clinical Activity, and Study Variables (N = 165)
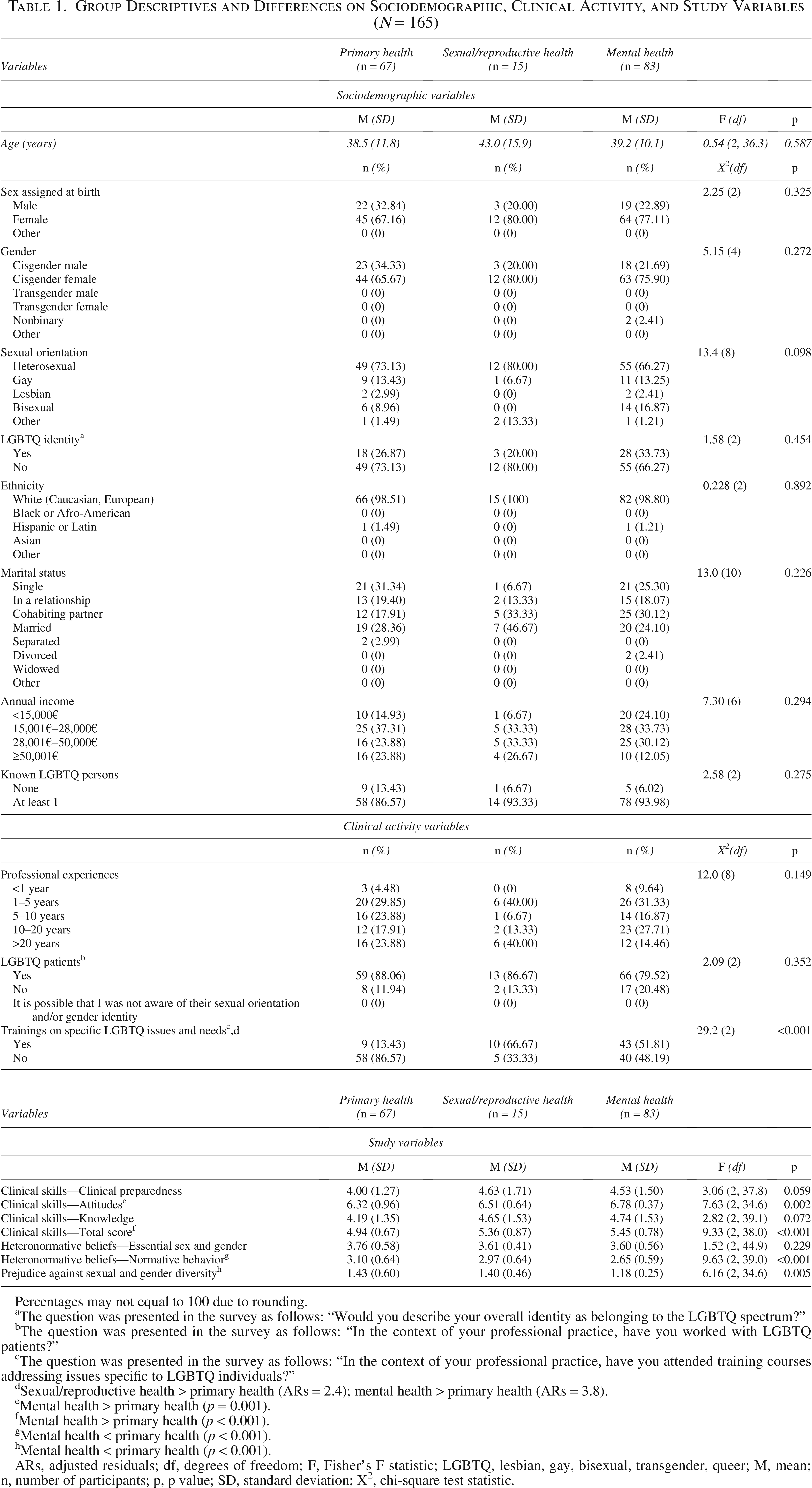
Percentages may not equal to 100 due to rounding.
The question was presented in the survey as follows: “Would you describe your overall identity as belonging to the LGBTQ spectrum?”
The question was presented in the survey as follows: “In the context of your professional practice, have you worked with LGBTQ patients?”
The question was presented in the survey as follows: “In the context of your professional practice, have you attended training courses addressing issues specific to LGBTQ individuals?”
Sexual/reproductive health > primary health (ARs = 2.4); mental health > primary health (ARs = 3.8).
Mental health > primary health (p = 0.001).
Mental health > primary health (p < 0.001).
Mental health < primary health (p < 0.001).
Mental health < primary health (p < 0.001).
ARs, adjusted residuals; df, degrees of freedom; F, Fisher’s F statistic; LGBTQ, lesbian, gay, bisexual, transgender, queer; M, mean; n, number of participants; p, p value; SD, standard deviation; Χ2, chi-square test statistic.
The 3 groups were comparable in all the sociodemographic and clinical information variables, except for the attendance at LGBTQ trainings; sexual/reproductive and mental health practitioners reported a significantly higher frequency of attendance at previous trainings than primary health practitioners. The 3 groups did not differ in terms of clinical preparedness, knowledge, and essential sex and gender heteronormative beliefs. However, primary health practitioners displayed significantly worse attitudes and lower total clinical skills in working with LGBTQ patients, as well as higher normative behavior heteronormative beliefs and prejudice against sexual and gender diversity than mental health practitioners.
A MANOVA was further implemented to assess the main effects of and the interaction between Group and attendance at LGBTQ trainings on study variables (Table 2 and 3). A main effect of training emerged, with practitioners who have attended previous LGBTQ trainings showing better clinical preparedness, basic knowledge and total clinical skills. A significant group x training interaction also emerged: mental health practitioners who have attended LGBTQ trainings display lower normative behavior beliefs than mental health practitioners who have not attended trainings. In addition, primary health practitioners who have attended LGBTQ trainings were characterized by higher normative behavior beliefs than mental health practitioners who have attended similar trainings.
Group x Trainings Interaction on Practitioners’ Clinical Skills (N = 165)
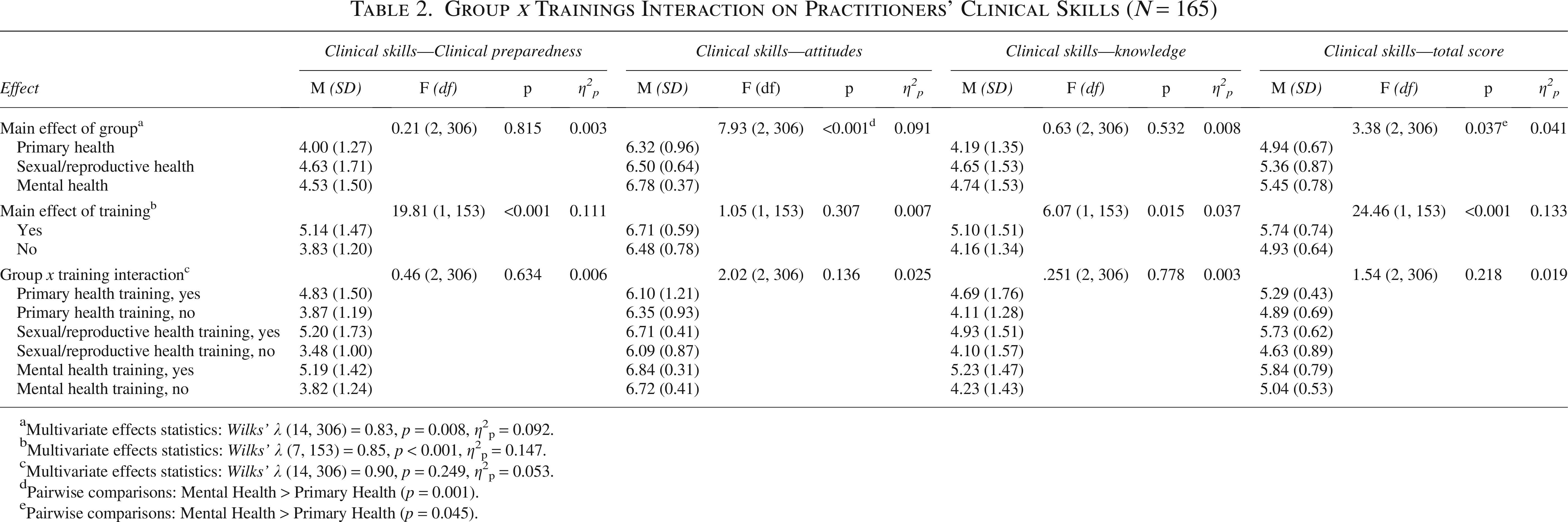
Multivariate effects statistics: Wilks’ λ (14, 306) = 0.83, p = 0.008, η2p = 0.092.
Multivariate effects statistics: Wilks’ λ (7, 153) = 0.85, p < 0.001, η2p = 0.147.
Multivariate effects statistics: Wilks’ λ (14, 306) = 0.90, p = 0.249, η2p = 0.053.
Pairwise comparisons: Mental Health > Primary Health (p = 0.001).
Pairwise comparisons: Mental Health > Primary Health (p = 0.045).
Group x Trainings Interaction on Practitioners’ Heteronormative Beliefs and Prejudice (N = 165)
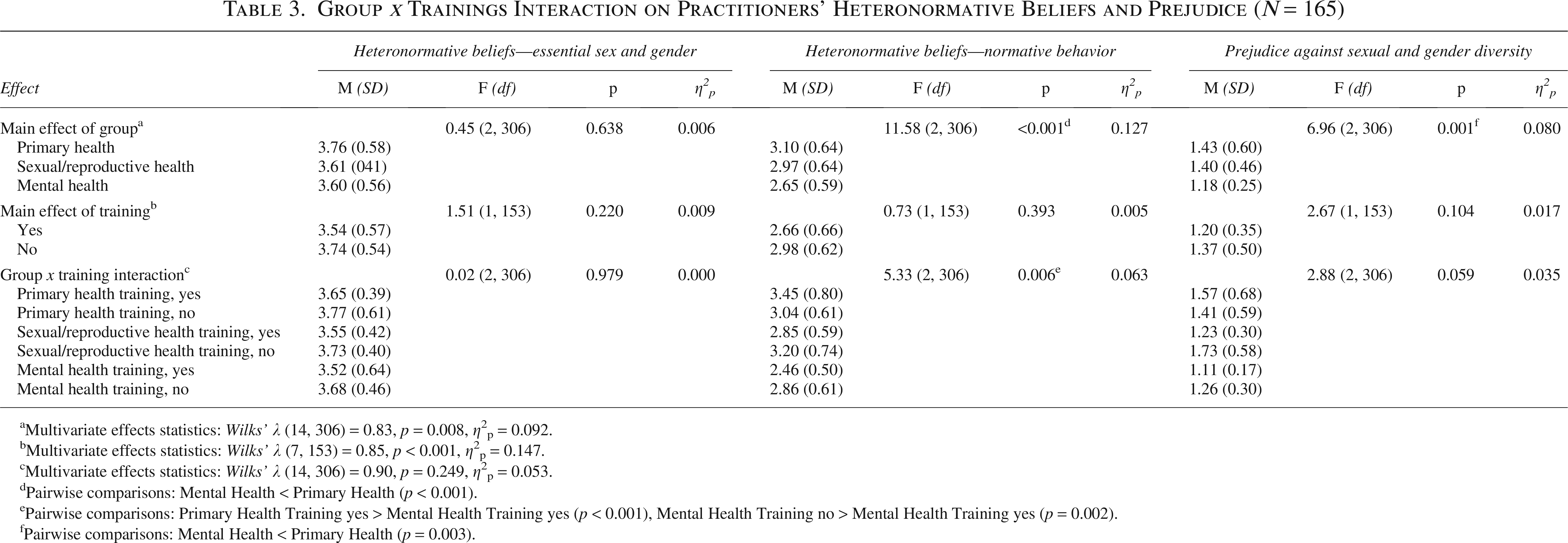
aMultivariate effects statistics: Wilks’ λ (14, 306) = 0.83, p = 0.008, η2p = 0.092.
bMultivariate effects statistics: Wilks’ λ (7, 153) = 0.85, p < 0.001, η2p = 0.147.
cMultivariate effects statistics: Wilks’ λ (14, 306) = 0.90, p = 0.249, η2p = 0.053.
dPairwise comparisons: Mental Health < Primary Health (p < 0.001).
ePairwise comparisons: Primary Health Training yes > Mental Health Training yes (p < 0.001), Mental Health Training no > Mental Health Training yes (p = 0.002).
fPairwise comparisons: Mental Health < Primary Health (p = 0.003).
Bivariate correlations are reported Table 4. Among the entire sample, negative attitudes, as well as lower knowledge and total clinical skills were associated with higher heteronormative beliefs and prejudice against sexual and gender diversity. Notably, within clinical skills, more positive attitudes were associated with higher knowledge. The general linear model with the clinical skills total score as the dependent variable was significant (p < 0.001) and explained 43.9% of the observed variance. Better clinical skills in working with LGBTQ patients were significantly associated with practitioners’ lower essential sex and gender heteronormative beliefs and prejudice against sexual and gender diversity, having at least 1 LGBTQ person in one’s own personal relationships, and having attended LGBTQ trainings. The full model estimates are reported in Table 5.
Associations among Clinical Skills, Heteronormative Beliefs, and Prejudice in the Entire Sample (N = 165)
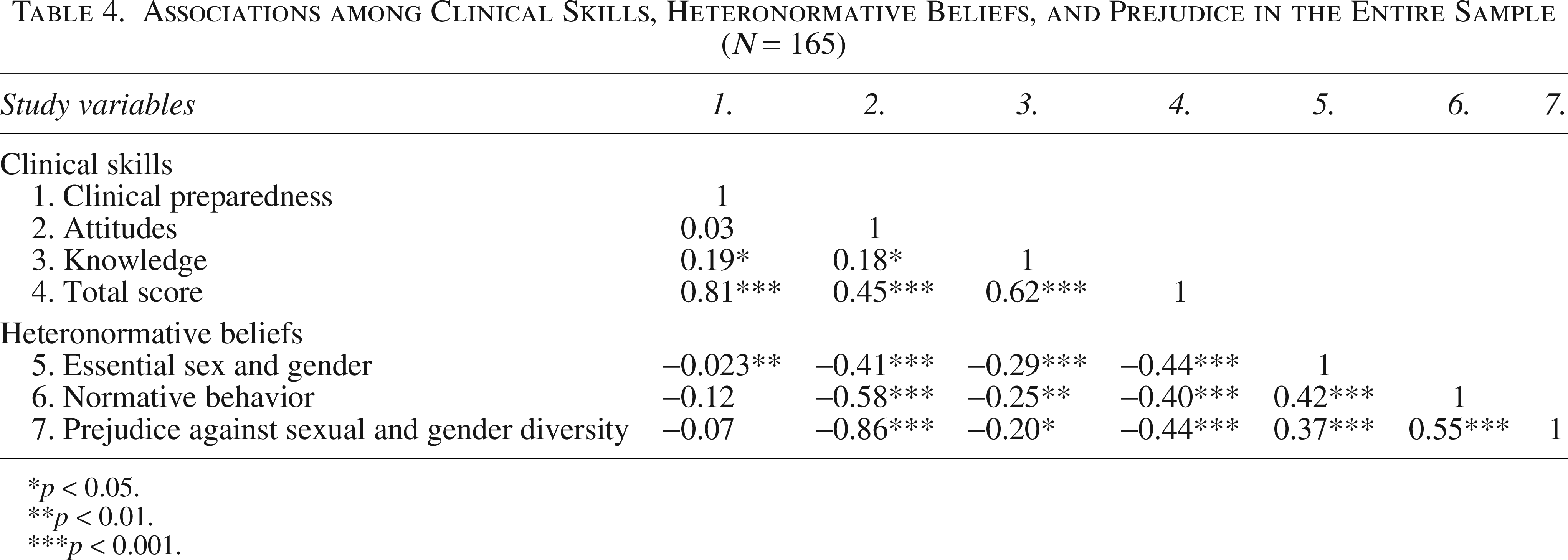
p < 0.05.
p < 0.01.
p < 0.001.
Factors Associated with Practitioners’ Clinical Skills in Working with Lesbian, Gay, Bisexual, Transgender, and Queer Patients (N = 165)
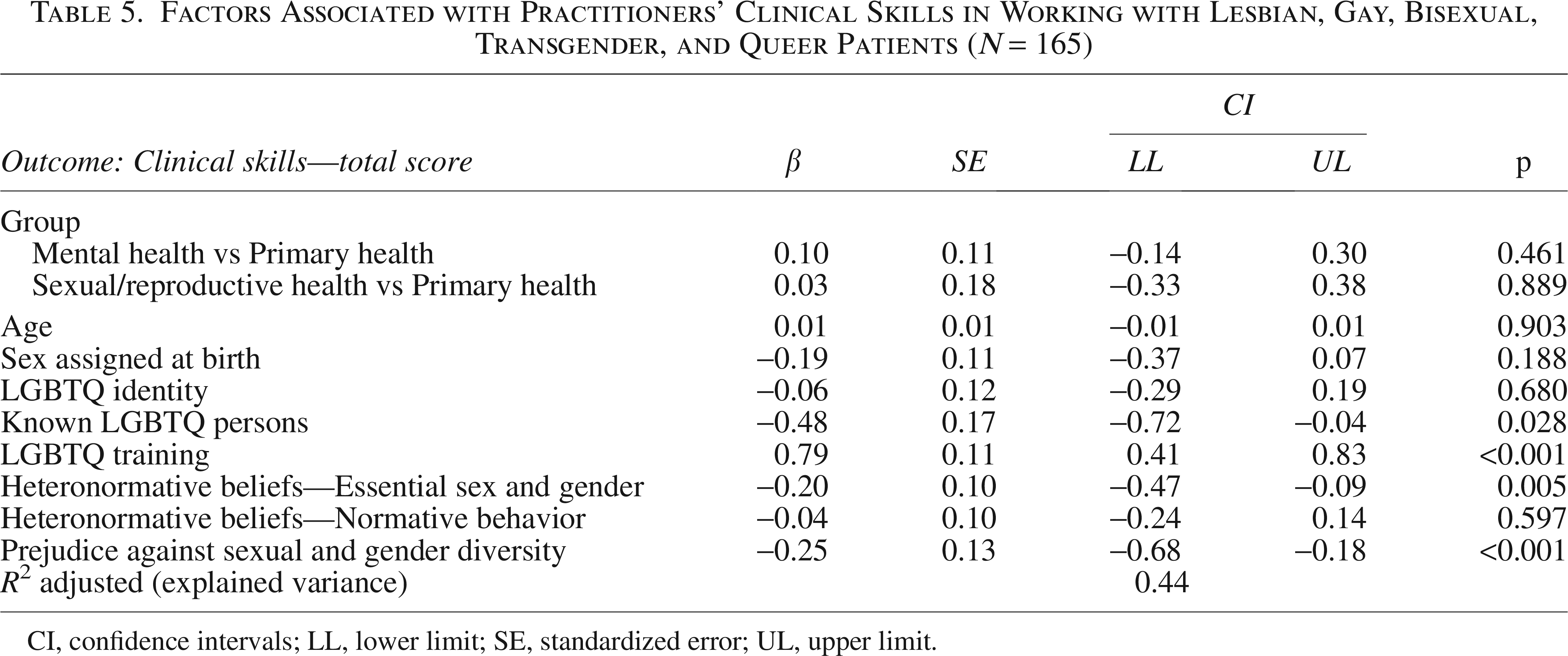
CI, confidence intervals; LL, lower limit; SE, standardized error; UL, upper limit.
Discussion
The present study provided a preliminary exploration of Italian healthcare practitioners’ clinical skills in working with LGBTQ patients across primary, sexual and reproductive health, and mental health care, and examined sociodemographic and personal factors associated with such skills. Primary health practitioners displayed significant worse attitudes and lower total clinical skills in working with LGBTQ patients, and higher heteronormative beliefs concerning normative behavior and prejudice against sexual and gender diversity than mental health practitioners. Primary health practitioners received the lowest amount of LGBTQ training among the three groups. Among the whole sample, better clinical skills were significantly associated with practitioners’ lower heteronormative beliefs and prejudice against sexual and gender diversity, with having attended trainings on specific LGBTQ issues and needs and with having at least 1 LGBTQ person in one’s own personal relationships.
Regarding group differences, primary healthcare practitioners exhibited more negative clinical and general attitudes toward LGBTQ individuals compared to mental health providers. Clinical attitudes, encompassing openness, adaptability, and communicative sensitivity, play a pivotal role in shaping the quality of healthcare interactions. Such dispositions, which function as both personal and professional competencies, influence patients’ trust, adherence, and willingness to seek care. Conversely, attitudes marked by discomfort or avoidance may compromise therapeutic relationships and discourage patients from disclosing relevant information or engaging in treatment.
In this vein, prior work shows that primary healthcare practitioners express varying levels of agreement about proactively asking adult and youth patients about sexual orientation and gender identity.55,56 They also often report discomfort or feeling unprepared to address LGBTQ issues and needs.56,57 A review further indicates that, in an effort to avoid making assumptions, many practitioners adopt a stance of “professional neutrality”; however, LGBTQ patients report that such neutrality can inadvertently reproduce heterosexist and cisnormative dynamics. 58
Nevertheless, not all primary healthcare practitioners may be characterized by more negative clinical attitudes toward LGBTQ patients. For instance, studies on oncology healthcare providers59,60 found that, despite low clinical preparedness, participants showed globally positive clinical attitudes toward assessing patients’ sexual orientation or gender identity-related issues, are characterized by generally favorable beliefs about patients’ sexual orientation and gender identity, and also reported being comfortable treating these populations. In this vein, it is possible that negative clinical attitudes may be a reflection of broader individuals’ negative attitudes towards LGBTQ people, rather than a specific connotation of a healthcare category.
In line with this hypothesis, along with clinical attitudes, primary healthcare practitioners also showed higher levels of negative attitudes towards LGBTQ communities at a broader level. These attitudes included more rigid heteronormative assumptions and enhanced levels of prejudice against sexual and gender diversity, than mental health professionals. These findings accord with prior research documenting lower explicit and implicit biases against lesbian women and gay men in mental health than primary care practitioners. 61
One explanation may pertain to the centrality of therapists’ subjective variables in clinical work.62–64 In this vein, psychological mindedness (i.e., active engagement in making sense of one’s own and others’ psychological experiences)65,66 and mentalization (i.e., the capacity to understand oneself and others in terms of underlying mental states, both implicitly and explicitly) 67 may predispose providers to adopt more open, accepting, and inclusive stances toward LGBTQ patients. A second explanation relates to the widespread practice of therapists’ personal psychotherapy, whether required by training institutes or pursued voluntarily. Such work encourages critical reflection on personal histories, biases, and internalized prejudices, increasing awareness and mitigation of potential discriminatory attitudes.68–72
Primary care respondents also reported lower rates of LGBTQ training than both sexual and reproductive health practitioners and mental health practitioners. These results align with a recent U.S. survey of trainees across health disciplines, 73 in which medical and nursing students reported fewer hours and lower-quality LGBTQ-specific education than psychology students. Together, these findings underscore the need to increase both the quantity and quality of LGBTQ-specific training across health professions. Expanding curricular hours and improving content breadth and depth has the potential to foster more inclusive attitudes, reduce prejudice, and enhance providers’ knowledge and confidence in addressing LGBTQ health concerns, ultimately strengthening clinical skills, improving patient communication, and promoting more equitable care.74–76
In this vein, it is noteworthy that in the present study attendance at LGBTQ trainings was linked to greater clinical knowledge and preparedness across all groups, but not to changes in clinical attitudes or broader measures such as heteronormative beliefs and prejudice. This exploratory pattern observed in the current sample likely reflects the largely knowledge-focused nature of training in Italy regarding the health of lesbian, gay, bisexual, and transgender individuals. 77 These trainings may strengthen competence without addressing cultural, relational, or attitudinal dimensions, highlighting the need for curricula that integrate experiential and culturally competent components.26,77 These results resonate with the Culturally Competent Compassion Model,27,50 which emphasizes the integration of knowledge, self-awareness, relational sensitivity, and active efforts to counteract bias in promoting effective cross-cultural care.
The finding that LGBTQ training was associated primarily with knowledge and preparedness, but not with attitudinal dimensions, highlights a possible gap between factual competence and the deeper relational and reflective components central to culturally competent compassion. In line with the Culturally Competent Compassion Model, strengthening clinical skills requires not only the transmission of information but also structured opportunities for reflexivity, emotional engagement, and examination of implicit biases. To this end, curricula should incorporate interactive and experiential components, including case discussions, focus groups, role-plays, and direct involvement of LGBTQ individuals through testimonies and co-facilitated workshops, to enhance empathy, surface implicit biases, and promote culturally sensitive practice.78,79
These observations were further confirmed, as LGBTQ training emerged as a significant positive predictor of clinical skills. Moreover, higher clinical skill was significantly associated with lower heteronormative beliefs and prejudice, as well as with having friends or relatives who identify as LGBTQ. Regardless of specialty, practitioners with strong heteronormative beliefs and negative prejudices have been shown to create interpersonal barriers to care for lesbian, gay, bisexual, and transgender patients, reflecting deficits in appropriate attitudes and knowledge.18,23 Conversely, fostering affirming attitudes is crucial: such attitudes are linked to better patient outcomes and higher-quality care across healthcare settings80–89 and to improved clinical outcomes and more effective therapeutic processes in mental health practice.85–87 Nevertheless, these associations should be interpreted as preliminary, as they rely on measures not yet fully validated in the Italian context.
From a theoretical standpoint, these findings can be interpreted in light of the HEPM, 35 which posits that health outcomes among lesbian, gay, bisexual, and transgender individuals are shaped not only by structural stigma and minority stress but also by protective and affirming contextual factors. In this framework, healthcare providers’ attitudes and competencies represent crucial structural and interpersonal determinants that may either mitigate or exacerbate health disparities.23,24 The observed associations between lower heteronormative beliefs, reduced prejudice, greater training exposure, and enhanced clinical skills may tentatively suggest that providers’ cultural competence may function as a protective factor within Italian healthcare settings, potentially contributing to more equitable and affirming care trajectories for LGBTQ patients.
Having LGBTQ friends or relatives was associated with enhanced clinical skills among practitioners, likely reflecting the benefits of direct, meaningful contact. Consistent with the contact hypothesis, 88 intergroup interactions that combine personal exposure with educational content can reduce prejudice, challenge stereotypes, and foster empathy.89,90 Key conditions for lasting effects include equal status, common goals, authoritative support, and minimal conflict,91,92 conditions naturally present in personal relationships but also replicable in structured training by incorporating direct testimonies, case discussions, or participatory activities, to promote inclusive clinical skills and more affirmative attitudes toward LGBTQ patients.
Contrary to our hypotheses, LGBTQ identity was not significantly associated with clinical skills, reflecting mixed evidence in prior research.57,58,62,93–96 Many null findings arise from samples of mental health practitioners, suggesting that field-specific dispositions (e.g., psychological mindedness, mentalizing capacity) and personal psychotherapy experiences may promote affirmative attitudes and adequate knowledge irrespective of identity. Rather than identity itself, co-occurring factors characterizing LGBTQ individuals, such as lower heteronormative beliefs and prejudice,53,54 greater ties with LGBTQ peers,97,98 and a more respectful approach toward LGBTQ communities,99,100 may lead to higher clinical skills, consistent with the preliminary patterns observed in the present data.
Limitations
The present study has several limitations. Methodologically, participants were recruited through nonrandom procedures, and sexual and reproductive health practitioners were underrepresented relative to the other groups, which may limit generalizability. Limited generalizability of the present results could be affected also by the low or absent representation of specific healthcare professionals, including urologists, endocrinologists, plastic surgeons, and emergency medicine specialists; future studies are warranted to include healthcare professions that were under-represented or absent in the present study.
In addition, the surveyed sample was predominantly composed of cisgender participants. Previous literature has pointed to better clinical knowledge and attitudes among practitioners holding an LGBTQ identity48,49; however, the present results showed no associations between participants’ LGBTQ identity and their clinical skills in working with LGBTQ patients; it is possible that the almost complete absence of practitioners with transgender identities could have overshadowed a possible effect. Further studies are required with larger and more representative samples to strengthen the generalizability of the findings. Accordingly, the results of the present study should be considered preliminary and exploratory.
Another limitation of the present study concerns the use of instruments that have not yet been formally validated in Italian (LGBT-DOCSS and PASGD-R). In the present study, a rigorous back-translation procedure was applied and internal consistency indices in the current sample were acceptable to good. However, the absence of validated Italian versions may limit the comparability of findings with other studies and calls for future research aimed at establishing the psychometric properties of these measures in larger Italian samples. This issue also raises the need to consider the results from the present study as preliminary and exploratory, due to measurement limitations. More specifically, the lack of full psychometric validation may affect construct validity, as it cannot be fully assumed that the instruments capture the same latent dimensions in the Italian cultural and linguistic context as in the original versions. This may in turn influence the interpretation of associations observed in the data and limit direct comparability with findings from studies conducted in other countries using validated versions of the same measures.
An additional limitation of the employed survey relates to the use of the term “other” in the collection of participants’ sociodemographic information. Although the intention was to provide the participants with the opportunity to personally select denominations that better represented their status (e.g., regarding gender identity, sexual orientation, ethnicity) than the provided options, we acknowledge that this wording may inadvertently contribute to feelings of marginalization. A formulation such as “I don’t see myself here” would likely have represented a more inclusive and person-centered alternative.
Another limitation concerns the assessment of LGBTQ training, which was measured dichotomously (attendance vs. no attendance) without detailed information on duration, content, satisfaction, or quality. As training opportunities may differ substantially across professional specialties, future studies are invited to assess this variable more in depth across healthcare groups. Self-report measures also introduces potential self-presentation (social desirability) bias, suggesting that future work should include implicit measures of beliefs and prejudice. In addition, the cross-sectional design precludes causal inference, underscoring the need for longitudinal studies. A further limitation is the lack of detailed information about the type and content of LGBTQ-related training received, which may differ across provider groups. Relatedly, we did not assess practitioners’ training needs or interest in additional training, factors that may be associated with clinical skills.
Conclusions
Limitations notwithstanding, and bearing in mind the exploratory nature of the findings, the present results offer preliminary indications that may inform training and service organization, pointing to the need for targeted educational programs to strengthen clinicians’ competence with LGBTQ patients, with particular attention to reducing heteronormative beliefs and prejudice. The positive associations between clinical competence, LGBTQ-specific training, and personal contact suggest that experiential, awareness-raising interventions may be especially effective. Moreover, differences across healthcare domains indicate that training could be tailored to professional context to ensure consistent, inclusive practice.
The results also carry tentative implications for health policy. Embedding LGBTQ-inclusive competencies and guidelines into national and regional standards may contribute to promoting equitable and sensitive care. Policymakers may consider encouraging regular LGBTQ cultural-competency training and incentivize institutions to adopt inclusive practices. Partnerships with LGBTQ communities can support evidence-based policymaking and evaluation. Overall, strengthening LGBTQ competence at the policy level has the potential to enhance care quality, reduce disparities, and foster a more equitable healthcare system.
Ethical Considerations
The present study was approved on May 15th, 2024 by the Ethical Committee of the University of Naples “Federico II” (protocol no. 10/2024) and the Territorial Ethics Committee Lazio Area 2 (protocol no. 197.24 CET2 utv) and was conducted in accordance with the EU General Data Protection Regulation.
Consent to Participate
All participants signed a written informed consent to participate in the study.
Consent for Publication
All participants authorized the use of anonymized data for future publications.
Authors’ Contributions
G.C.: Conceptualization (equal); data curation (lead); formal analysis (lead); investigation (equal); methodology (lead); software; writing—original draft (lead). M.Q.: Investigation (equal); writing—review and editing (equal). S.M.: Investigation (equal); writing—review and editing (equal). C.S.: data curation (supporting); funding acquisition (supporting); resources (equal); writing—review and editing (equal). N.C.: Conceptualization (equal); data curation (supporting); formal analysis (supporting); funding acquisition (lead); methodology (supporting); resources (equal); supervision (lead); writing—review and editing (equal). All authors have approved the final article.
Footnotes
Declaration of Conflicting Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Statement
This work was supported by funding from the Italian Ministry of University and Research (MUR) under the call Progetti di Rilevante Interesse Nazionale (PRIN) 2022 (Project number 2022YYL4RE; Project title: Intersectional Stigma and Health Equity Promotion for LGBT People in Primary, Sexual/Reproductive, and Mental Health Care Settings; Principal Investigator: Nicola Carone; CUP: F53D23004920001; PNRR for the Mission 4, investment 1.1., funded by the European Union–NextGenerationEU).
Data Availability
Research data supporting the findings of the current study are available upon reasonable request to the corresponding author.
Disclaimer
The content of the present article is solely the responsibility of the authors. Funders had no role in the study design; collection, analysis, and interpretation of data; writing of the article; or decision to submit the article for publication.