
Abstract
Purpose:
This study reviewed the U.S. insurance landscape for gender-affirming surgery (GAS) and examined how regional, legislative, and health care infrastructure factors influence coverage patterns to inform policy reform and advocacy.
Methods:
Policies from the top three insurers in each state, identified via the National Association of Insurance Commissioners, were analyzed in November 2024. Coverage was compared across census regions, and criteria concordance with the World Professional Association for Transgender Health (WPATH) Standards of Care, Version 8, was assessed. GAS fellowship availability, policy information accessibility (7-point Likert scale), and legislative favorability (Movement Advancement Project scores) were also evaluated. Coverage rates were compared across procedures using analysis of variance with post hoc Tukey tests. Poisson regression identified predictors of coverage, and ordinal logistic regression assessed predictors of policy information accessibility. All analyses were conducted in R 4.4.1.
Results:
We included 144 state insurance policies, representing 77% of the U.S. market. Overall GAS coverage was 67.7%, with significantly lower rates for fertility cryopreservation (6.6%), facial feminization (37.3%), and GAS reversal (65.7%). GAS fellowship presence positively predicted coverage (p < 0.001). States with fair (p = 0.041) or medium legislative favorability (p = 0.004) had higher coverage compared with negatively rated states. Only 61.9% of policies were concordant with WPATH guidelines. Coverage information access was uniformly limited and was more limited in Southern states than in other regions (p < 0.001).
Conclusion:
Insurance coverage for GAS was inconsistent and strongly influenced by political and health care infrastructure factors rather than medical necessity. The lack of guideline concordance and systematic information barriers highlights the need for targeted reforms.
Keywords
Introduction
The annual number of gender-affirming surgeries (GAS) in the United States increased fivefold, from 421 procedures in 2016 to 2224 procedures in 2021. 1 GAS is recognized as medically necessary by major professional organizations, including the World Professional Association for Transgender Health (WPATH), when patients meet established clinical criteria, such as persistent gender dysphoria and required evaluations. 2 However, overall procedural volume remains relatively low compared with other elective surgical categories, and access continues to be constrained by geographic and insurance-related barriers. In response to evolving evidence and patient needs, WPATH released the eighth version of the Standards of Care (SOC-8) in 2022. 2 This marked a shift in the field by declaring facial feminization surgery (FFS) a medical necessity, whereas previously it was considered cosmetic and denied coverage. 2
However, insurance enrollment does not necessarily equate to meaningful access to care. Although many patients rely on insurance to cover surgical expenses, restrictive coverage criteria or high costs in the absence of coverage limits access. 3 This is further impeded by inconsistencies across insurance companies and state legislative restrictions. 4 As of November 2024, 26 states have enacted legislation limiting gender-affirming care for adolescents, prompting many patients to seek care out-of-state. 5 A study of 1735 patients demonstrated that individuals seeking GAS travel a median distance of 191 miles, further inflating the financial and logistic burdens of care. 6
Prior studies of commercial insurance have assessed coverage by procedural category but did not perform current procedural terminology (CPT)-level analyses or evaluate health care infrastructure and legislative climate.7–9 Coverage has also not been examined in relation to local transgender health care infrastructure, including the availability of GAS fellowships providing specialized care. Currently, 16 GAS fellowships exist across 12 states, with four states (California, Illinois, New York, and Ohio) hosting two programs each. Legislative favorability toward LGBT-related policies also varies by state.
Given these gaps and the rapidly changing sociopolitical landscape, we analyzed procedural-level insurance coverage for GAS across the top insurers in every U.S. state, as defined by the National Association of Insurance Commissioners (NAIC) market share report, which includes commercial private insurance, Medicare Advantage, Medicare Supplement, and Medicaid managed care plans administered by these carriers. In addition, we examined the relationship between insurance coverage patterns and key factors, including adherence to WPATH SOC-8, the availability of specialized GAS fellowships, and state legislative favorability. 2 Through this multifaceted approach, our findings aimed to inform advocacy efforts, guide policy reform, and enhance equitable access to medically necessary GAS.
Methods
The institutional review board (IRB) at Beth Israel Deaconess Medical Center determined that this study did not constitute human subjects research (IRB protocol #2024D000690; August 21, 2024), as it involved analysis of publicly available insurer policy documents without interaction with human subjects or the use of identifiable private information.
Insurer selection
The three largest U.S. health insurers in each state were selected based on the NAIC market share report. 10 A systematic online search was conducted in November 2024 to review these companies’ GAS policies. In cases where policy details were not available online, the companies were contacted via phone interview for further information. If information remained unavailable after follow-up telephone inquiries, the company was excluded from the analyses. To focus on national structural coverage patterns rather than comparisons between individual carriers, insurer names were not reported but are available upon request, consistent with prior aggregate analyses of insurance coverage in this field.
Policy analysis and classification
We defined “top surgery’” as mastectomy for chest masculinization and breast augmentation for chest feminization, and “bottom surgery” as genital gender-affirming surgeries, including vaginoplasty, vulvoplasty, orchiectomy, phalloplasty, and metoidioplasty. Each GAS policy was individually evaluated for coverage of gender-affirming procedures using CPT codes, as well as explicit statement of coverage for fertility preservation procedures and GAS reversal. The CPT codes included in this study were derived from the literature as well as consensus of multiple expert plastic and gender surgeons at our institution (R.P.C., B.T.L., S.J.L., A.M.T., and M.A.K.).9,11–14 A summary of the CPT codes included in the analysis is provided in Table 1.
Summary and Definition of Procedure Codes
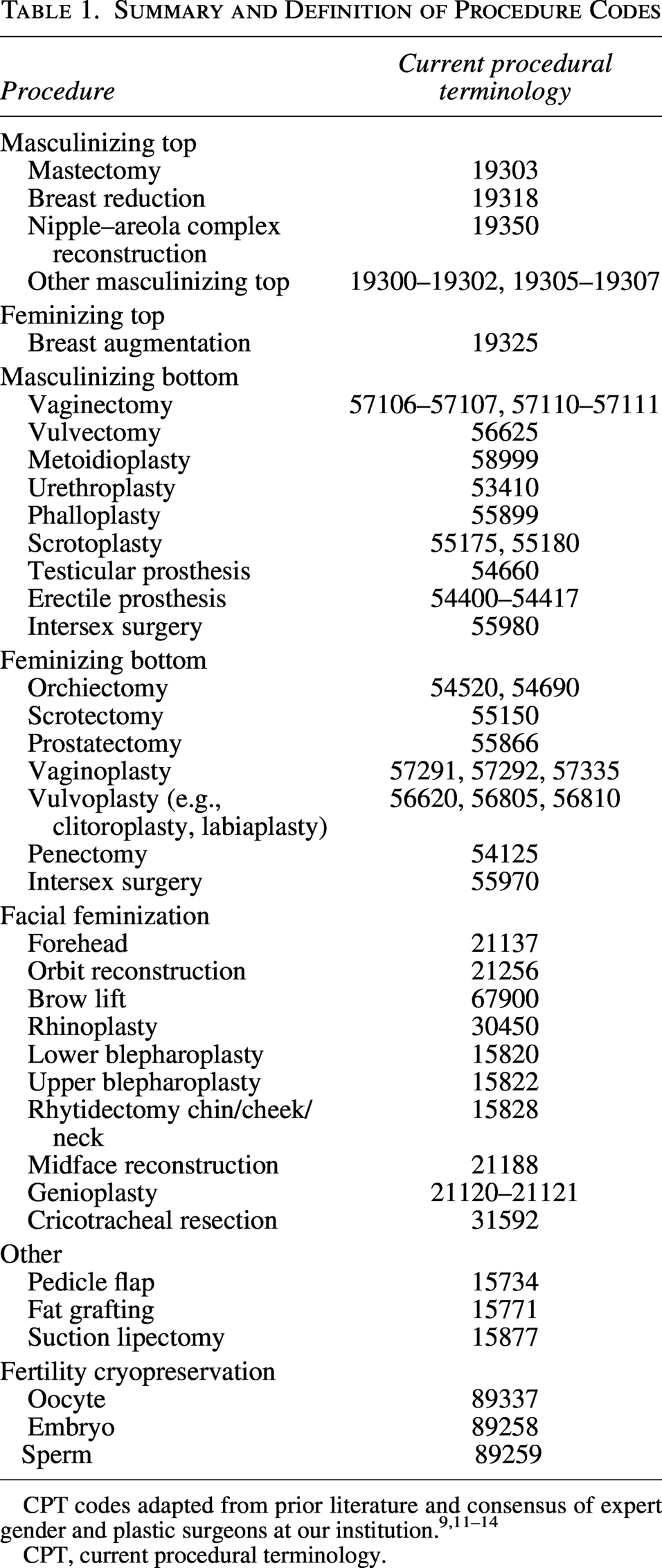
CPT codes adapted from prior literature and consensus of expert gender and plastic surgeons at our institution.9,11–14
CPT, current procedural terminology.
The policies were classified based on previously published methodologies: requiring preauthorization, covered case-by-case, never covered, and covered without restriction.7–9,15–17 Specifically, “requiring preauthorization” indicated coverage contingent upon fulfillment of specified medical necessity criteria (Covered Meeting Criteria), “covered case-by-case” reflected the absence of standardized criteria with individualized review (Covered Evaluating Case), “never covered” denoted explicit exclusion, and “covered without restriction” indicated explicit coverage without stated eligibility prerequisites beyond standard plan enrollment. Percentage of coverage was compared across U.S. Census regions. 18
Inclusion and exclusion criteria
Coverage was confirmed when a policy explicitly stated that a procedure was medically necessary and eligible for coverage. Similarly, a policy was classified as providing no coverage if it explicitly stated that the procedure was not covered. To be included in the analysis, a policy had to originate from an insurer operating within one of the 50 U.S. states and rank among the top three providers in that state based on market share. “Policy” referred to the publicly available medical coverage policy issued by the insurer governing GAS benefits. We evaluated carrier-level medical policy documents, as medical necessity criteria are typically determined at the insurer level. Companies were excluded if they did not offer primary comprehensive health care coverage or if their coverage details were unavailable online and could not be obtained via telephone inquiries. A flow chart of policy inclusion is provided in Figure 1.
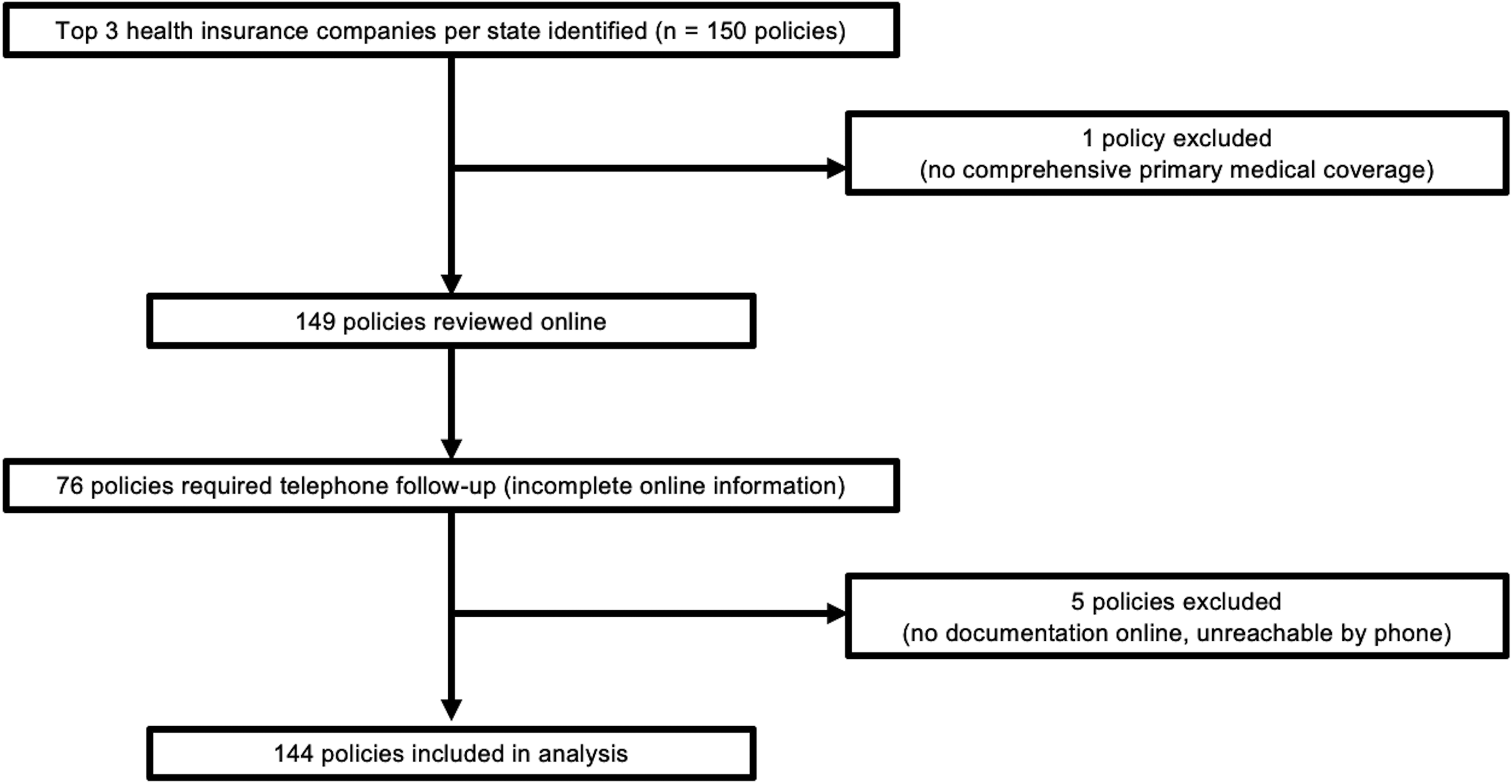
Flowchart of insurance policy inclusion.
Medical necessity criteria
Medical necessity criteria for gender-affirming procedures were abstracted from each publicly available policy. Coverage criteria were assessed for their concordance with the WPATH SOC-8 guidelines, which detail necessary conditions for gender-affirming treatment, as outlined in Table 2.2,19 Key domains assessed included age requirements (e.g., age of majority), duration of documented gender dysphoria, hormone therapy prerequisites, continuous living requirements (i.e., mandated duration living in affirmed gender role), and required health care provider referral letters. Investigators (M.M., T.M.R., M.Y., M.T., A.N.P., and L.F.) collected coverage data, which were independently reviewed by the first two authors (M.M. and J.H.L.).
Summary of World Professional Association for Transgender Health Standards of Care Version 8 Criteria for Gender-Affirming Surgery
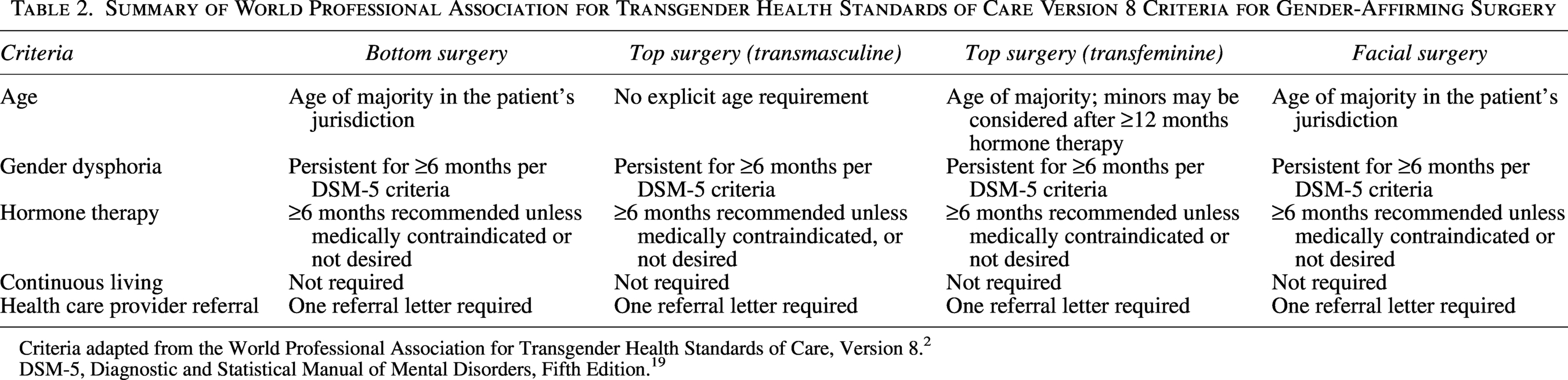
Criteria adapted from the World Professional Association for Transgender Health Standards of Care, Version 8. 2
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. 19
Measure of accessibility of coverage information
Publicly searched online materials included insurer medical policy bulletins and explicit clinical coverage guidelines published by the insurer specifically for gender-affirming surgery. In instances where predefined policy elements were not explicitly stated in publicly available online documents, a telephone inquiry was conducted using the publicly listed customer service numbers available on each insurer’s website for the state under review. For example, to ensure methodological consistency, insurers were contacted to confirm coverage of specific CPT codes of interest when policies broadly indicated coverage of a procedure but did not specify whether the CPT codes assessed in this study were explicitly included.
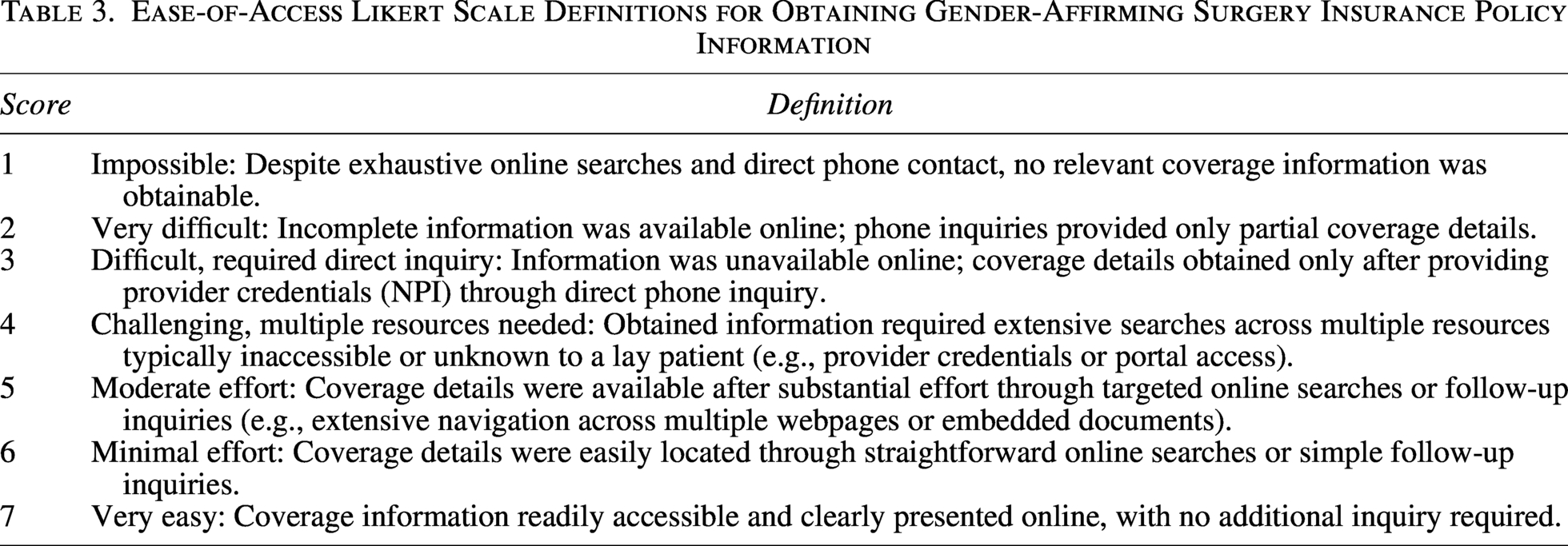
Additional clarification was limited to predefined variables, including medical necessity criteria, reversal procedures, and fertility preservation coverage. The specific information that was missing from the online policy materials, the response received via telephone attempt, and whether complete details were subsequently obtained were systematically recorded. Two authors (M.M. and T.M.R.) independently evaluated the ease of accessing coverage information using a validated 7-point Likert scale (higher scores indicated greater ease; Table 3).15,20 Scores distinguished between information publicly available without login credentials (5–7) versus information requiring provider-level portal access, provider credentials, and/or direct telephone inquiry (1–4).
Ease-of-Access Likert Scale Definitions for Obtaining Gender-Affirming Surgery Insurance Policy Information
Legislative favorability
Legislative favorability was assessed using Movement Advancement Project (MAP) scores, which rate each state on 50 sexual and gender minority laws across seven domains (e.g., nondiscrimination, health care, criminal justice). 21 States earn positive points for protective laws and negative points for discriminatory laws. Based on the percentage of total possible points, states were categorized as negative (<0%), low (0%–24.9%), fair/medium (25%–74.9%), or high (75%–100%). Previous literature has endorsed the usage of the MAP score, and the methodology of score calculations can be found on the MAP website.7,22–25
GAS fellowship availability and regional coverage analysis
To analyze the relationship between availability of transgender health care infrastructure and regional insurance coverage patterns, we quantified the association between the availability of GAS fellowships in each state and regional coverage rates. GAS fellowships were identified through national professional society directories and targeted keyword searches using keywords “gender-affirming surgery fellowship,” “GAS fellowship,” and “transgender surgery fellowship.” To evaluate the potential influence of GAS-specific fellowships at the state-level, we characterized fellowship presence as a binary indicator based on whether it was located within that particular state.
Statistical analyses
Means, proportions, and measures of variance were calculated using standard mathematical methods. A Poisson regression was used to evaluate predictors of coverage, and ordinal logistic regression was used to assess predictors of ease of access to coverage information. Covariates included region, legislative climate (MAP score), and fellowship presence. Results were reported using risk ratios and odds ratios with 95% confidence intervals (CIs). Pairwise comparisons of coverage among procedural categories were conducted using analysis of variance and Tukey’s honest significant difference test. Interrater reliability of ease-of-access Likert scores were evaluated using Cohen’s kappa. Statistical analyses were performed using R version 4.4.1 (Boston, MA, USA), and significance was evaluated using a two-tailed test at an alpha level set at 0.05.
Results
A total of 144 state insurance policies were included in this study, representing 77% of the U.S. market share. Six policies (<3% cumulative market share) were excluded: one lacked primary medical coverage, and five lacked available online documentation and could not be reached via telephone.
Gender-affirming surgery insurance coverage
Overall coverage was 67.7%, with 61.8% offering coverage if criteria were met (prior authorization) and 5.9% coverage on a case-by-case basis. In total, 32.3% of procedures had no policy coverage. Coverage breakdown and regional differences are illustrated in Figures 2 and 3, respectively. Procedural category differences were statistically significant (Fig. 4). Fertility cryopreservation had the lowest coverage, with an average of 93.4% of insurance policies offering no coverage, followed by FFS, for which 62.7% offered no coverage, and reversal surgery procedures, for which 34.3% offered no coverage (Supplementary Table S1).
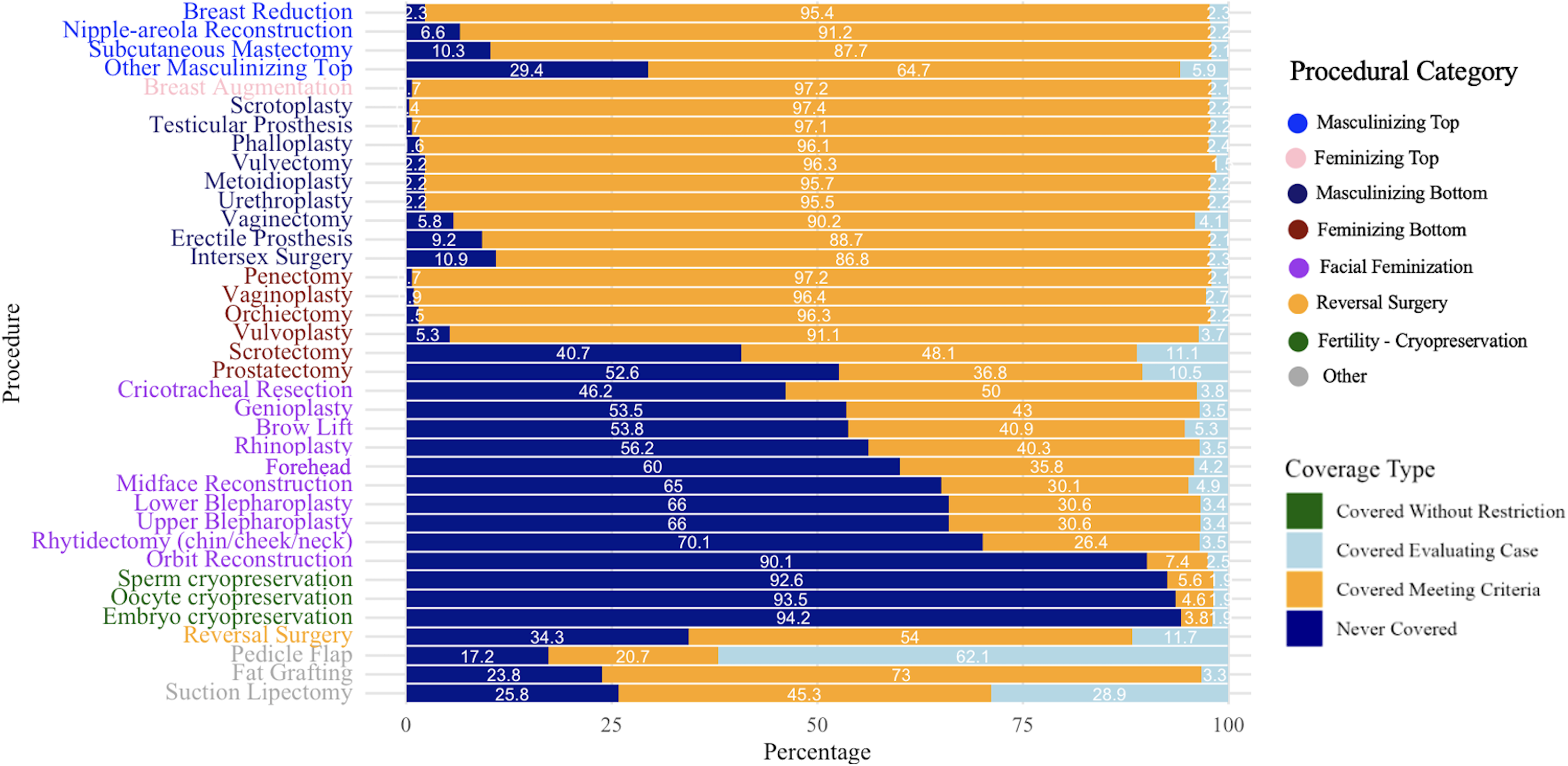
Gender-affirming care procedural coverage.
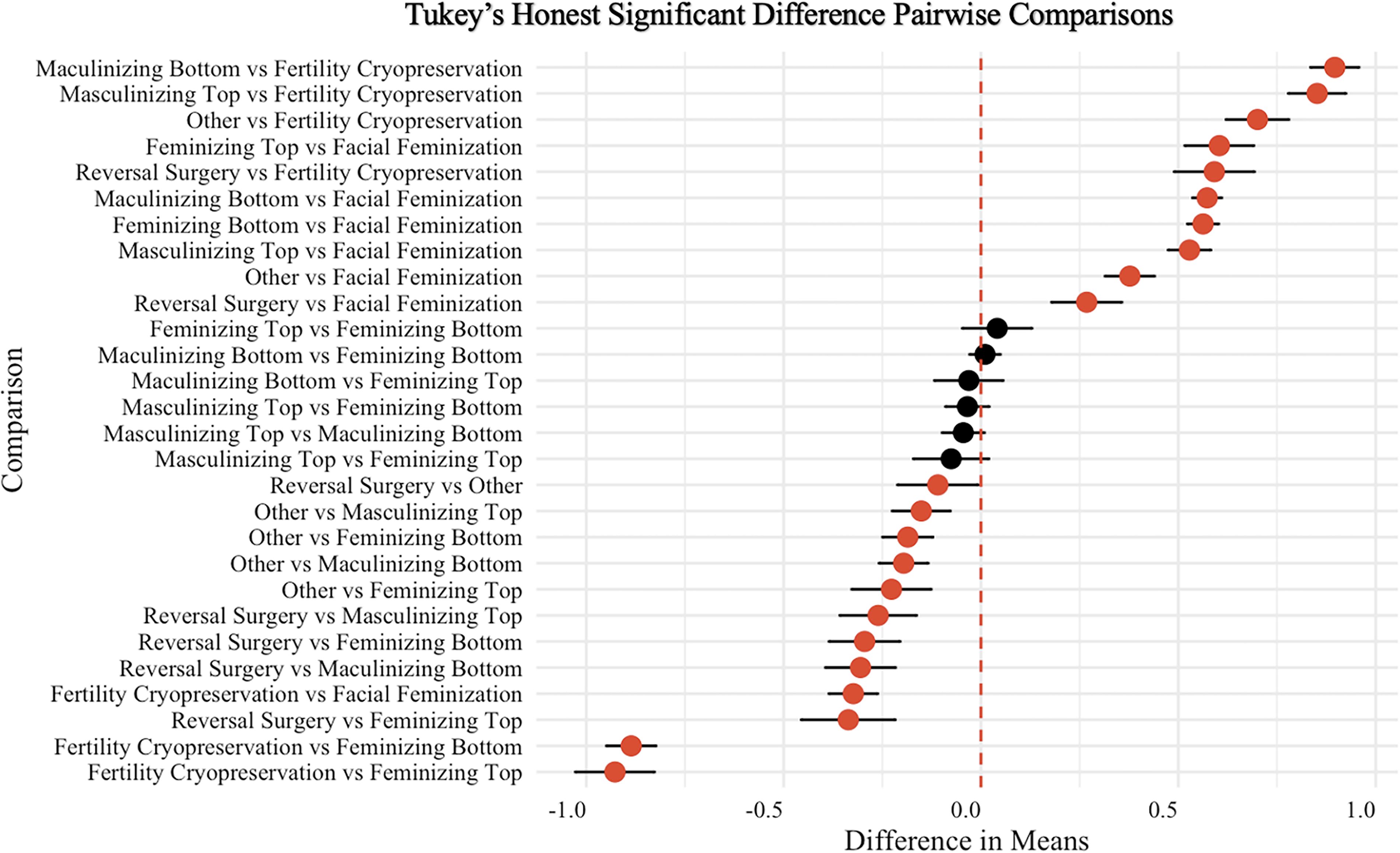
Pairwise comparisons of insurance coverage by procedural category. Other = pedicle flap, fat grafting, suction lipectomy.
The presence of a fellowship in a state was associated with higher coverage rates (adjusted risk ratio [aRR]: 1.10, 95% CI: 1.06–1.14, p < 0.001). Fair (aRR: 1.08, 95% CI: 1.00–1.17, p = 0.041) and medium (aRR: 1.05, 95% CI: 1.03–1.15, p = 0.004) overall policy scores were also associated with higher GAS coverage rates compared with negative scores. Neither low nor high overall policy scores, nor region, were significant predictors of coverage rates (Table 4). On subsection analysis by procedural category, the presence of a fellowship was a significant predictor of insurance coverage for FFS (aRR: 1.51, 95% CI: 1.31–1.74, p < 0.001) and fertility cryopreservation (aRR: 11.56, 95% CI: 2.85–47.00), p < 0.001) (Supplementary Table S2).
Poisson Regression Model of Gender-Affirming Surgical Insurance Coverage
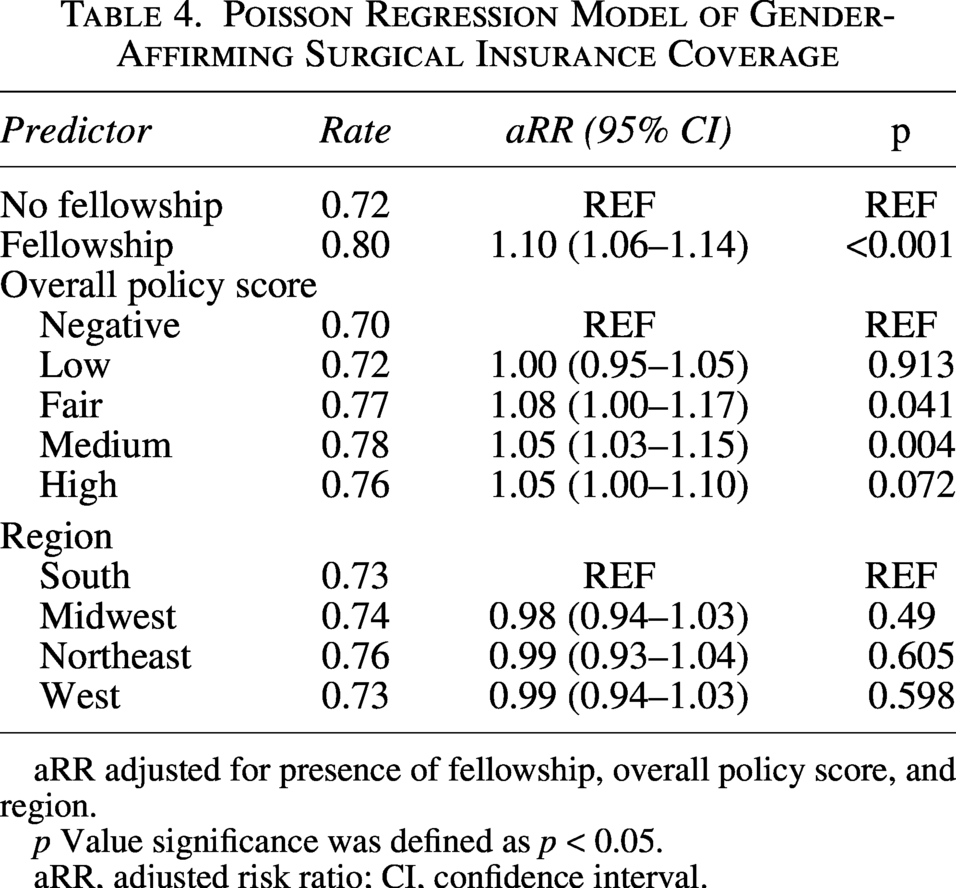
aRR adjusted for presence of fellowship, overall policy score, and region.
p Value significance was defined as p < 0.05.
aRR, adjusted risk ratio; CI, confidence interval.
Ease of obtaining insurance coverage policies
The mean Likert score was 3.58, indicating “challenging” or “difficult” access requiring multiple resources or phone inquiry. Only 52.1% (75/144) of policies were classified as accessible to patients (Likert score ≥ 5). There was high interreliability between the two raters (κ = 0.75). Coverage policies in the Northeast were easiest to obtain, with the highest mean Likert score (3.96 ± 1.86), followed by the West (3.84 ±1.53), Midwest (3.55 ± 1.83), and South (3.24 ± 1.64) (Supplementary Table S3 and S4). Seventy-six follow-up calls were made to insurance companies, with the majority 80.3% (61/76) of calls made to ask about CPT codes, 13.2% (10/76) of calls clarifying policy-specific criteria, and 6.6% (5/76) of calls were made as there was no information available online.
The ordinal logistic regression model demonstrated that high (adjusted odds ratio [aOR]: 3.96, 95% CI: 3.47–4.53, p < 0.001), medium (aOR: 1.61, 95% CI: 1.38–1.87, p < 0.001), and low (aOR: 1.74, 95% CI: 1.54–1.97, p < 0.001) overall policy scores were more likely to have scored in higher Likert score categories than negative overall policy scores. Fair overall policies had lower odds of scoring in higher Likert score categories than negative overall policies (aOR: 0.78, 95% CI: 0.62–0.97, p = 0.024). Insurance policies in the West (aOR: 2.27, 95% CI: 2.02–2.54, p < 0.001), Northeast (aOR: 2.49, 95% CI: 2.13–2.92, p < 0.001), and Midwest (aOR: 1.86, 95% CI: 1.64–2.11, p < 0.001) were more likely to have higher Likert scores compared to insurance policies in the South (Table 5).
Ordinal Logistic Regression Model of Likert Score Grading Ease of Obtaining Insurance Coverage Policies
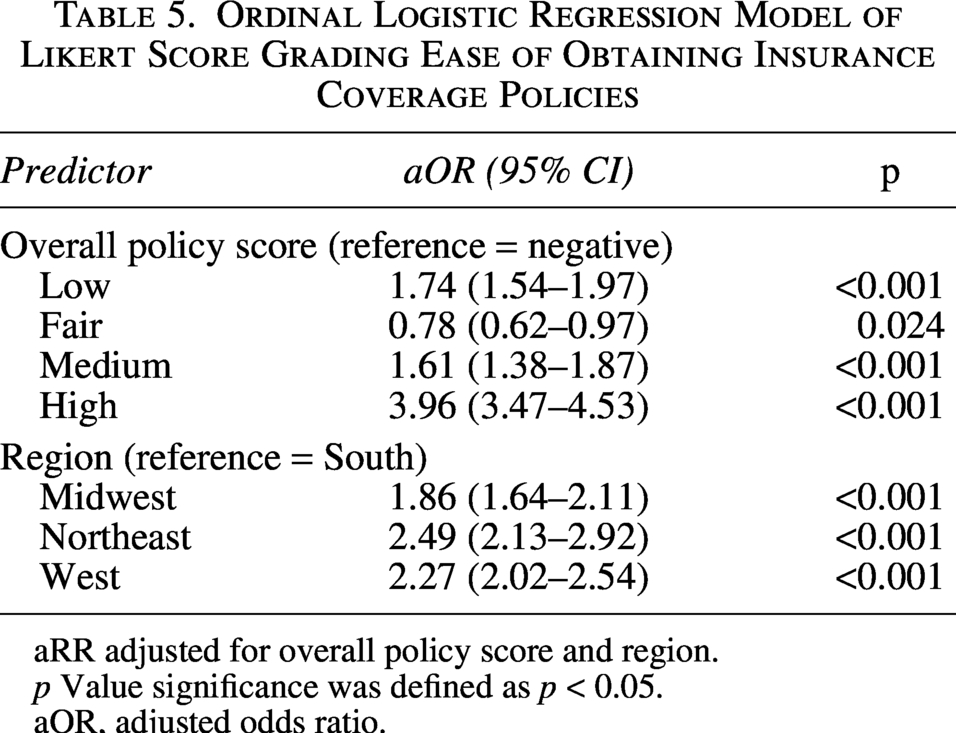
aRR adjusted for overall policy score and region.
p Value significance was defined as p < 0.05.
aOR, adjusted odds ratio.
WPATH concordance
Overall, 61.9% of policies were WPATH concordant. In terms of surgical treatment, FFS procedures were the most likely to be WPATH concordant (73.1%), followed by bottom surgery (61.7%) and top surgery (57.5%). The most common requirements by which gender-affirming surgery insurance policies were not WPATH concordant were continuous living requirements (93.5%), followed by hormone therapy requirements (67.0%), and minimum age requirements (49.0%).
Notably, among mastectomy for chest masculinization and breast augmentation for chest feminization insurance policies, 90.5% were not WPATH concordant with relation to minimum age requirements (Fig. 5). Despite age not being a WPATH criteria for coverage of mastectomy for chest masculinization and breast augmentation for chest feminization coverage, most policies (83.9%) required a minimum age of 18 years. WPATH concordance criteria are further detailed in Supplementary Figure S1.
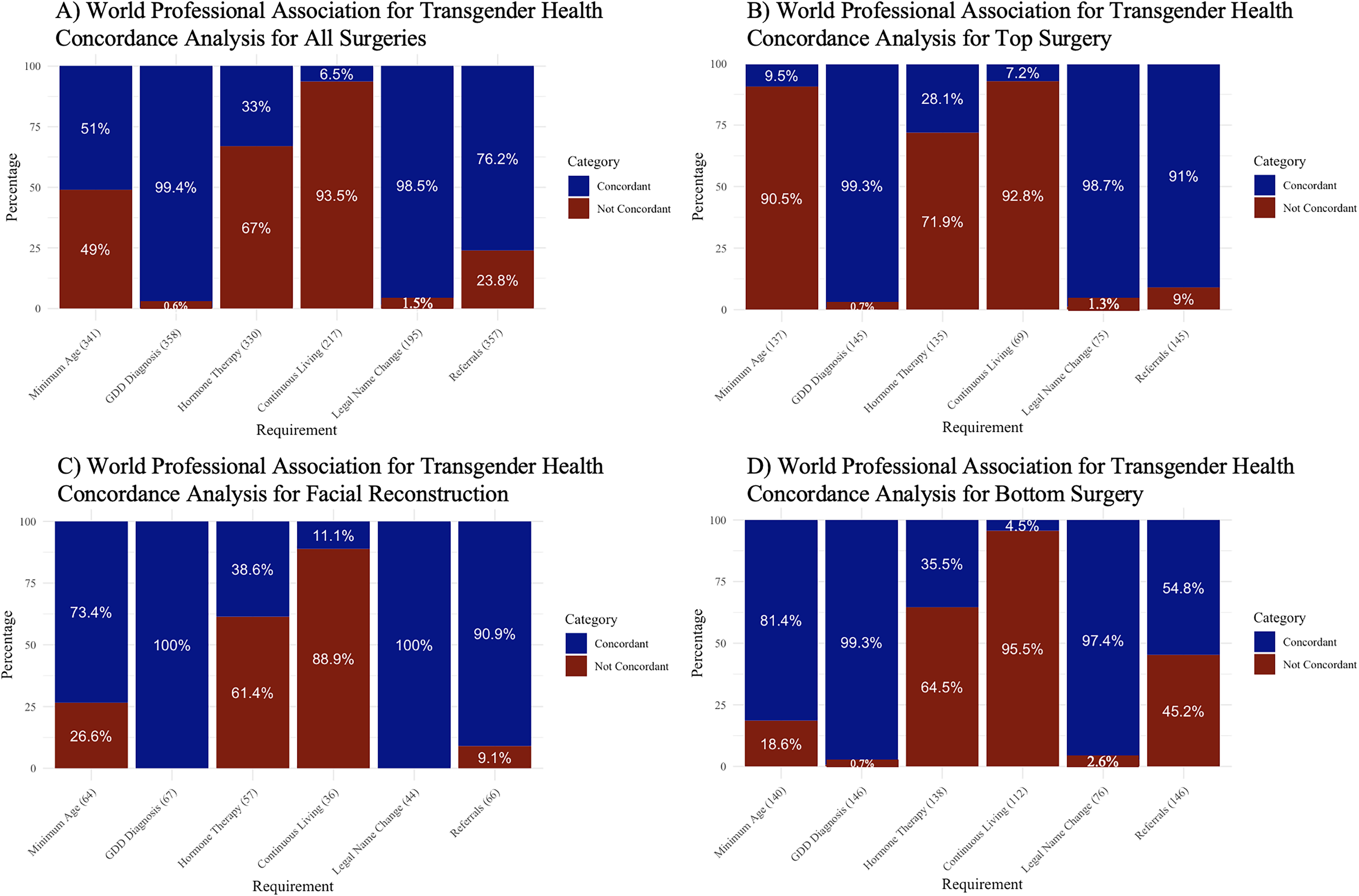
World Professional Association for Transgender Health Version 8 Concordance by Procedural Category.
2
Discussion
This national study found moderate overall coverage rates for GAS in the United States, with variation by geographic region, legislative climate, and procedural category, as well as a positive association with the presence of GAS fellowships. In addition, nearly 40% of GAS policies contained criteria discordant with current WPATH SOC, and coverage information was frequently difficult to access. 2 Together, these findings highlight persistent gaps in policy transparency and guideline alignment that limit meaningful access to care.
Amid ongoing federal health policy discussions—including potential changes to Medicare and Medicaid funding—it is important to establish a baseline understanding of current insurer-issued coverage policies. Although this study does not directly analyze federal fee-for-service programs, many large commercial carriers administer Medicare Advantage and Medicaid managed care plans, and broader policy shifts may influence how coverage criteria evolve across payer types.
Regions with more favorable policy environments related to gender identity, as well as those with a greater number of GAS fellowships generally had higher rates of coverage for GAS. Even when procedures were covered, specific information about coverage was often difficult to access. Investigators needed to reach out to over half of the study sample to manually verify or obtain additional coverage information. Patients may consult public sources for GAS information, and poor accessibility imposes further care barriers.3,23,26 Limited transparency may delay care-seeking, discourage consultation, or result in unexpected financial burden.
Compared with a 2019 study that similarly evaluated coverage among the top three largest commercial insurers in each state, our analysis revealed markedly improved insurance coverage for GAS procedures such as nipple–areola complex reconstruction (93.4% vs. 20%), chest feminization (99.3% vs. 29%), penile prosthesis (90.8% vs. 40%), and vulvoplasty (94.8% vs. 21%). 27 This likely reflects increased recognition of medical necessity and ongoing advocacy efforts. Finally, while a 2024 study reported higher coverage for masculinizing versus feminizing chest surgeries, likely due to a higher burden of proof for procedures with cosmetic overlap, our analysis revealed no significant differences. 7 This discrepancy may indicate a positive shift toward equity in coverage between masculinizing and feminizing procedures.
Coverage rates were especially low for FFS and fertility cryopreservation. FFS demonstrated low but improved FFS coverage (∼37% coverage) compared to prior reports of 18% and 24%.7,15 The low coverage rate for FFS likely reflects the higher burden of proof for procedures with cosmetic overlap, as well as historical ambiguity in prior WPATH guidelines regarding medical necessity. Low coverage for fertility preservation has also been reported. 9 Although cryopreservation is generally undercovered across populations, lack of coverage for transgender patients represents another critical barrier for patients seeking to preserve biological fertility prior to irreversible interventions.28,29
GAS is associated with improved mental health and quality-of-life outcomes, underscoring the implications of limited coverage.30–32 In addition, many procedures may appear to be covered qualitatively but are largely inaccessible to patients in practice due to restrictive criteria that are misaligned with current WPATH guidelines.2,33,34 Specifically, we observed substantial nonconcordance related to continuous living requirements, hormone therapy duration, and minimum age requirements across all procedures, consistent with findings from a prior study. 34
Guideline nondiscordance may reflect adherence to outdated SOC-7 standards, including longer hormone therapy and continuous living requirements. 35 Our results highlight that payers have not universally adapted to the more inclusive SOC-8 guidelines.2,36 These discordant criteria serve as substantial barriers and reinforce the idea that nominal coverage alone does not equate to adequate patient access to care.8,34
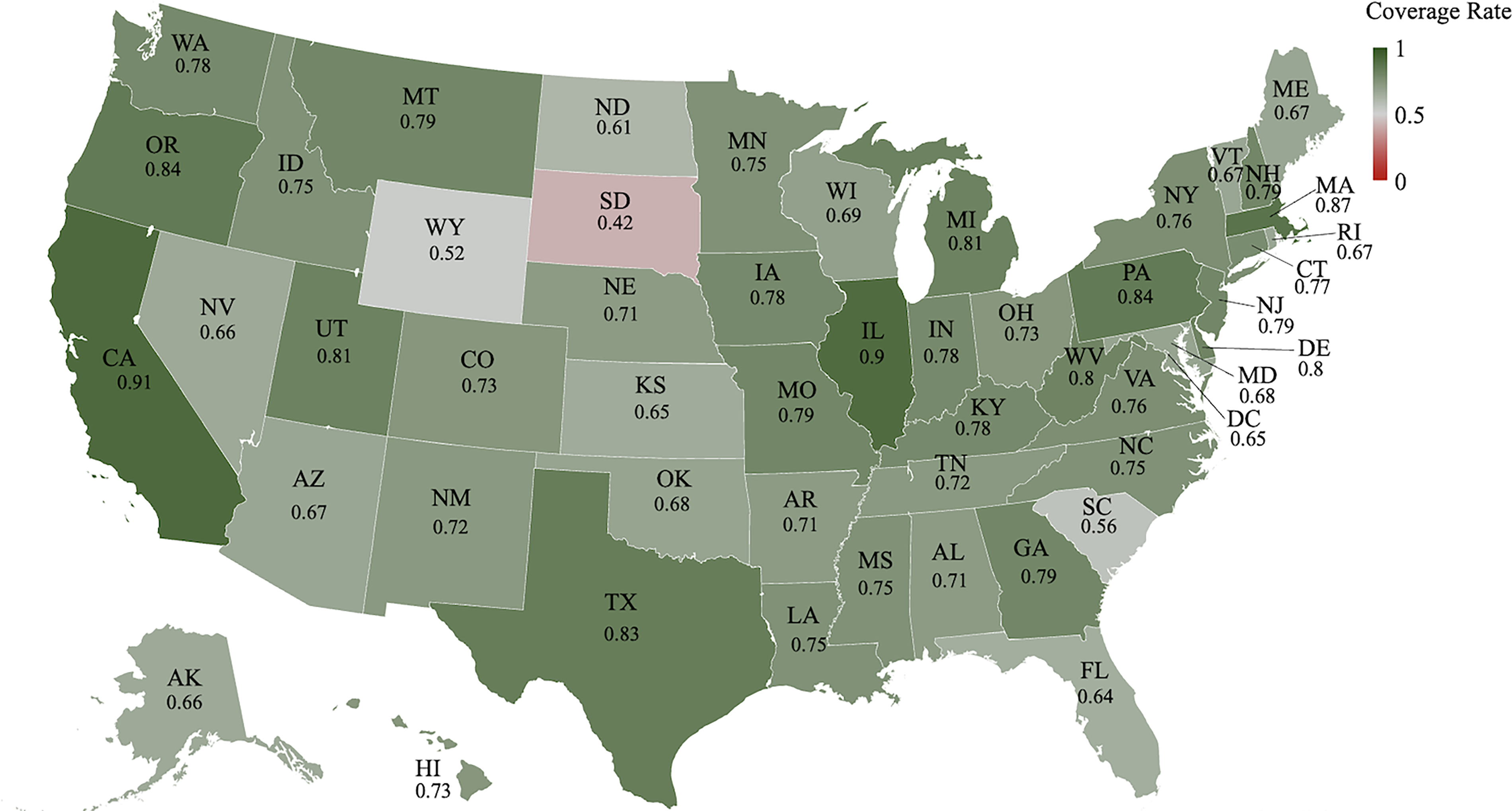
Heatmap of gender-affirming surgery insurance coverage.
Cost remains a major barrier, and lack of insurance coverage forces transgender patients to forgo medically necessary treatments or incur high out-of-pocket costs.3,37,38 These barriers have only worsened in the context of recent federal actions rescinding protections on the basis of gender identity under health care nondiscrimination laws.4,39–42 Addressing gaps in coverage and aligning coverage policies with evidence-based guidelines are critical to preserving equitable access to care.
We also observed higher overall rates of procedures based on geographic region and state-level policy scores. Importantly, greater legislative favorability related to gender identity was a strong predictor of GAS coverage. There was also evidence that state-level availability of GAS fellowships–a proxy for specialized transgender health care infrastructure–was associated with higher procedural coverage rates. These findings suggest that coverage policies for GAS are driven more by political environments and sociocultural attitudes toward transgender populations rather than medical necessity.32,34
Our analysis focused on policies issued by the largest health insurance carriers in each state. Therefore, the findings most directly reflect coverage patterns affecting individuals enrolled in commercial and employer-sponsored plans, as well as those covered through Medicare Advantage and Medicaid managed care administered by these carriers. As such, the populations most impacted by the policies examined in this study likely include employed transgender adults, their dependents, and publicly insured individuals enrolled in managed care products offered by major insurers.
Importantly, policies were abstracted and analyzed at the state-policy level rather than the parent company level. Although some parent organizations operated across multiple states, the 144 policies represented 32 unique parent companies, and we observed variation in policy language across states within the same parent organization. Although some residual intra-insurer correlation may exist, coverage determinations are implemented through state-specific regulatory frameworks and demonstrate substantial intra-insurer variation. These findings supported treating policies as independent state-level observations in our analyses.
Limitations
This study has several limitations. The cross-sectional analysis reflects policies at a single time point and cannot assess temporal trends or causality. In addition, although insurers represented 77% of market share, the findings may not generalize to all plans. Coverage policies issued by large commercial carriers may not necessarily hold in traditional fee-for-service Medicare or state-administered Medicaid programs, which have been the focus of prior studies. 43 Public insurance is often governed by federal or state-level statutory mandates and Centers for Medicare & Medicaid Services coverage determinations, which may differ structurally from commercial insurer medical policy frameworks. Moreover, written policy language may not fully reflect real-world coverage decisions.
Downstream access factors, such as network adequacy, provider availability, geographic distribution of qualified surgeons, or patient cost-sharing obligations (e.g., deductibles, coinsurance), were not captured in this study. Therefore, policy coverage as reported herein does not necessarily equate to practical access to care. Although coverage determinations via telephone inquiry were based on formal written medical policies and would be expected to remain consistent across representatives, variability in customer service processes may also have influenced the ease with which information was obtained, potentially affecting accessibility scoring.
Conclusion
Our national analysis demonstrates significant and ongoing disparities in insurance coverage for GAS across the United States. Coverage rates remain influenced more by political climate and geographic factors than by standardized, evidence-based medical criteria. Notably, substantial nonconcordance with current WPATH SOC-8 guidelines persists, reflecting outdated policies that remain major barriers to care, as well as systematic barriers to information access regarding coverage. 2 Aligning insurer criteria with evidence-based standards and improving the accessibility of coverage information are critical to ensuring meaningful access to care.
Authors’ Contributions
M.M.: Conceptualization, data curation (lead), investigation, methodology, project administration, resources, supervision, validation, visualization (supporting), formal analysis (supporting), and writing—original draft (equal) and review and editing (equal). J.H.L.: Data curation (supporting), formal analysis (lead), resources, software, validation, visualization (lead), and writing—original draft (equal) and review and editing (equal). M.L.: Validation, visualization (supporting) and writing—original draft (equal) and review and editing (equal). T.M.R.: Investigation and writing—original draft (equal) and review and editing (equal). M.Y., M.T., A.N.P., and L.F.: Investigation and writing—review and editing (equal). M.A.K.: Validation and writing—review and editing. A.M.T.: Validation and writing—review and editing (equal). S.J.L., B.T.L., and R.P.C.: Validation, supervision, and writing—review and editing (equal).
Ethical Considerations
This article does not contain any studies with human or animal participants. The Institutional Review Board (IRB) at Beth Israel Deaconess Medical Center determined on August 21, 2024 that this study did not constitute human subject research (IRB protocol #2024D000690), as it involved analysis of publicly available insurer policy documents without interaction with human subjects or use of identifiable private information.
Consent to Participate
Not applicable. There are no human participants in this article, and informed consent was not required.
Consent for Publication
Not applicable.
Data Availability
The data that support the findings of this study are available upon request from the corresponding author.
Footnotes
Declaration of Conflicting Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.