
Abstract
Objective
We examined the association between 18 covariates measuring women's self-reported positive experiences with their main HIV care provider/clinics, drawing on the Substance Abuse and Mental Health Services Administration “trauma-informed care” framework, and multiple HIV treatment/care outcomes.
Methods
Data (2014-2021) were drawn from a longitudinal community-based cohort with women living with HIV in Metro Vancouver (the Sexual Health and HIV/AIDS: Longitudinal Women's Needs Assessment) and analyzed using multivariable logistic regression with generalized estimating equations.
Results
Multivariable analysis suggested that principles of “safety and respect” (eg, feeling safe discussing sexual and/or reproductive health, confidentiality) and “strength-based collaboration” (eg, agency in scheduling, actively participating in one's own care) were significantly associated with higher odds of optimal HIV treatment/care outcomes.
Conclusions
Our study provides evidence for the benefit of incorporating and scaling up education, training and health systems policies that support women's positive experiences with their main HIV care provider/clinics in a trauma- and violence-informed framework.
Plain Language Summary Title
Safety, respect and collaboration in HIV care linked to achieving better treatment outcomes among women living with HIV
Plain Language Summary
Many women living with HIV have experienced trauma or violence, which can make it harder to stay engaged in HIV care and treatment. Health services that recognize and respond to these experiences, known as trauma- and violence-informed care, take into account the broader context of a person's life and the challenges they may face when accessing health services. This approach is gaining attention as a way to improve HIV treatment and care outcomes. We explored how women's experiences with HIV care providers and clinics were linked to their treatment and care outcomes, using principles from the Substance Abuse and Mental Health Services Administration trauma-informed care framework. We focused on 18 factors related to women's experiences of HIV care, such as safety, respect, collaboration, and choice. The study drew on data from 2014 to 2021 from the Sexual Health and HIV/AIDS Women's Needs Assessment community-based cohort of women living with HIV in Metro Vancouver. We used statistical methods to look at whether these 18 factors were connected with outcomes across the HIV care continuum. Outcomes included: being on antiretroviral therapy (ART); feeling confident in taking HIV medicine (self-efficacy); and consistently taking HIV medicine over different time periods (the last 2 weeks, month, and 3-6 months). Findings showed that women who reported positive HIV care experiences aligned with trauma- and violence-informed principles—particularly feeling safe, respected, and having a say in their care—were more likely to report positive HIV treatment and care outcomes. These outcomes included being on ART, having higher confidence in their ability to take medicines, and consistency in taking HIV medication over time. Our study provides strong evidence that integrating trauma- and violence-informed principles into HIV care experiences can improve treatment outcomes for women living with HIV. Supporting and scaling up services that prioritize safety, respect, and collaboration can play a key role in improving health and well-being.
Keywords
Introduction
Over the past decade, trauma- and violence-informed care and practice has been explored for its benefits across various fields, including within substance use and mental health care services provision. The Substance Abuse and Mental Health Services Administration (SAMHSA), an agency within the U.S. Department of Health and Human Services, has played a leading role in conceptualizing the role of trauma in influencing health outcomes, 1 including through the development of a National Center for Trauma-Informed Care in 2005. SAMHSA's “trauma-informed care” approach is guided by 6 key principles or values, which may be tailored according to the population and geographic setting and include: safety; trustworthiness and transparency; peer support; collaboration and mutuality; empowerment, voice and choice; and cultural, historical and gender issues. 1 There has been increasing research that aims to better understand how to incorporate trauma-informed care and practice into United States Ryan White HIV/AIDS Program (RWHAP) and other HIV clinic settings.
Increasingly, the term “trauma-informed” has been expanded on in order to more explicitly acknowledge the relationships between different sources of interpersonal (ie, physical, verbal, emotional, sexual acts of violence by perpetrators) and structural violence (ie, structural and systemic oppression and discrimination) and their impacts on all aspects of people's lives, including health and healthcare services access (“trauma- and-violence-informed”). For example, trauma- and violence-informed care is of 3 core dimensions in “Equity-Oriented Health Care,” an approach to care developed through research in our Canadian setting to address the needs of people experiencing substantial health and social inequities accessing primary and emergency care. 2 This model focuses on the development of safe healthcare environments within which trust can be built between patients and providers and the overall healthcare experience and health outcomes improved. 2 While SAMHSA uses the term “trauma-informed,” this article will continue to use the term “trauma- and violence-informed” alongside other current research in Canada and elsewhere.
In Canada and globally, women living with HIV, allies, and advocates have repeatedly called for improved healthcare experiences tailored to meet their needs. 3 It has been well-established that women living with HIV experience disproportionately high rates of structural and interpersonal violence and trauma throughout their lifetimes4,5 relative to general populations. These observations have been drawn on as part of a justification and call for incorporating trauma- and violence-informed principles into HIV care and practice.4,6 Trauma-and violence-aware care is also a key component of “women-centered HIV care,” a “comprehensive, holistic and flexible model” 7 of optimal care developed among women living with HIV in Canada, with global implications.7–9 All women living with HIV have experienced an HIV diagnosis, which in itself can be experienced as a trauma, depending on the context and circumstances and most women living with HIV have experienced HIV discrimination and stigma.10,11 Among all women living with HIV, there continues to be overrepresentation of women with marginalized and minoritized social identities, with structural and intersectional discrimination shaping access to health care services, health outcomes and quality of life. 12 In Canada and elsewhere, Indigenous women are overrepresented among women living with HIV as a result of historical and ongoing multigenerational colonial and other forms of structural violence.13–17
The negative health effects of trauma and physical and sexual violence (eg, intimate partner violence; sexual violence by nonpartners) are well-documented in multiple global reviews and include: mental health outcomes (eg, posttraumatic stress disorder, depression; anxiety); fatal and nonfatal injury and associated outcomes, including chronic pain; worse pregnancy outcomes (eg, low birth weight and prematurity); sexual health; and criminalized substance use.18,19 Women living with HIV who report lifetime or recent trauma including gender-based violence and HIV stigma have been more likely to report increased likelihood of posttraumatic stress disorder, depression, and anxiety symptoms; harmful alcohol and drug use; worse quality of life; and viral load nonsuppression; and less likely to report being on and having optimal adherence to antiretroviral therapy (ART).11,20,21
In an effort to bring attention to the urgent need to address gaps in access to health services and improve health among women living with HIV, much research with women living with HIV has sought to better understand how social and structural inequities are associated with reduced access along the HIV care continuum.5,22 Less research takes a strength-based approach to identify facilitators to better health and health services access outcomes, or positive experiences in health care that could mitigate the relationships between violence, stigma and suboptimal health services use and health outcomes, among women living with HIV. Several studies have identified better physician–patient relationships associated with optimal access along the HIV care continuum (eg, retention in care, ART use)23–25 and self-perceived women-centered HIV care has been associated with better health-related quality of life among women living with HIV. 26 Nevertheless, scarce evidence exists to guide the measurement or evaluation of trauma-and violence-informed principles in HIV practice in ours or other settings, nor to establish the potential positive health services access outcomes that having access to trauma-and-violence-informed HIV care could support. Our study therefore examined the association between 18 explanatory variables measuring characteristics of women's main HIV care provider/clinics and multiple outcomes related to HIV treatment/care continuum access. We drew on the SAMHSA work alongside community consultation to help guide our choice of survey items situating women's self-reported positive experiences with their main HIV care provider/clinics within 5 principles representing a trauma- and violence-informed practice framework.
Materials and Methods
Study Design and Sampling
Data were drawn from 7 years (September 1, 2014-August 31, 2021) of an open longitudinal community-based cohort of cisgender (cis) or trans WLWH who lived and/or accessed care in Metro Vancouver, Canada, which has been ongoing since 2014 (The Sexual Health and HIV/AIDS: Longitudinal Women's Needs Assessment [The SHAWNA Project]). SHAWNA is a partnership 10+ women's HIV and community service providers and is guided by a Community Stakeholder Advisory Board that meets annually, and a Positive Women's Advisory Board of WLWH that meets every 3-4 months. SHAWNA was developed based on over 6 months of community consultations with WLWH, HIV care providers and policy experts, with the main objective to longitudinally assess the HIV treatment and care and broader health needs and priorities identified by WLWH in Metro Vancouver.
Inclusion criteria for SHAWNA includes: living with HIV; self-identifying as a woman (cis or trans) at baseline interview; being ≥14 years and living and/or accessing HIV/AIDS services in Metro Vancouver. We use the term “community experts” to describe the people in our study rather than “participants,” as this is preferred by the community and reflects and honors lived and living experience and expertise. Community-based research principles guided our recruitment of community experts, including: self-referrals and referrals from HIV care providers, HIV/AIDS service organizations and clinical outreach (eg, Oak Tree Clinic), as well as word of mouth. Following obtaining informed consent for entry to the study, baseline surveys were completed, and community experts were invited to complete follow-up interviews every 6 months. Each semiannual study visit consists of (1) responding to a questionnaire administered by trained community researchers, including information on a variety of sociodemographic, structural, relational and healthcare access factors; and (2) an appointment with a sexual health research nurse, including laboratory blood testing, with CD4 counts and viral load measured as outcomes of the study. Sexually transmitted infections testing, education, and pap smears are also offered by the sexual health research nurse. Community experts receive an honorarium for their time and expertise. The honorarium has increased over the study period. At the study's inception in 2014, community experts received $50 for participating in the initial/baseline and each 6-monthly follow-up survey ($25 for the main questionnaire and $25 for the appointment with the sexual health research nurse). In September 2021, the honorarium increased to $80 for the initial/baseline survey and 65$ for each 6-monthly follow-up survey, and then in March, 2024 increased to $100 for initial/baseline survey and $80 for each 6-monthly follow-up survey. The honoraria for lab testing and appointment with the sexual health research nurse has remained at $25 throughout the study. SHAWNA holds ethical approval through the University of British Columbia/Providence Health Care Clinical Research Ethics Board (H14-01073).
Primary Covariates: Women's Experiences With HIV Care Providers/Clinics in a Trauma- and Violence-Informed Framework
Survey items on women's self-reported experiences with their main HIV care provider/clinics that reflected trauma- and violence-informed care principles relevant to HIV care were developed and grouped in themes building on an extensive literature review of existing principles and approaches, SAMHSA's trauma- and violence-informed framework 1 and further informed by our community consultation process. Item development was informed by the experience and expertise of our community and clinical partners, 27 staff, community researchers, Positive Women's Advisory Board (PWAB) and through piloting and testing with community experts and staff. Overall, 18 items were considered in this study. Each survey item could be responded to, in the context of whether or not community experts felt that their HIV care provider imbued the characteristics, as “agree” or “disagree.” To group our survey items as variables into themes, we drew on SAMHSA's 6 trauma- and violence-informed care principles, including: (1) Safety; (2) Trustworthiness and transparency; (3) Peer support; (4) Collaboration and mutuality; (5) Empowerment, voice and choice; and (6) Cultural, historical and gender issues. Following discussions with community and clinical collaborators, staff and following a workshop with PWAB, we grouped variables as follows: (1) Low-barrier accessibility; (2) Safety and respect; (3) Strength-based collaboration; (4) Peer support; (5) Gender/family-specific services.
Outcomes
We considered 5 outcomes representing different aspects of the HIV care continuum, including, among the full sample, self-reported being on ART (responding “yes” to currently being on ART vs “no”). Among those who self-reported being on ART, we also included positive HIV medication self-efficacy (among those on ART, categorized as “yes” if they responded that they were “extremely sure” or “very sure” to a survey item asking about if community experts were confident in their ability to take all or most medication as directed in the last 3 to 4 weeks, versus “somewhat sure” or “not sure at all”); taking all ART medication in the last 2 weeks (“yes” vs “no”); the last month (“yes” vs “no”); and the last 3 months (“yes” vs “no”).
Confounders
Potential confounders were chosen within the context of conceptual risk frameworks to explain suboptimal health services access and included time fixed variables: race/ethnicity (“Indigenous,” “other racialized person,” or “White”). The term Indigenous was used, recognizing this includes First Nations, Métis, and Inuit, 3 distinct groups of Indigenous peoples with a variety of cultures, traditions, languages, and geographical locations. In the response category of racialized women/women of color, possible responses included Black, East/Southeast Asian, Latinx, Middle Eastern, South Asian, and Other. While recognizing that aggregated racial/ethnic categories can mask diverse experiences, due to the small sample size of minoritized races/ethnicities, non-White and non-Indigenous responses to race/ethnicity were combined in the analysis to understand the experiences of non-Indigenous racialized community experts. Time-fixed variables also included im/migrant status (born in Canada vs not. All other variables were time-updated in the last 6 months. Additional variables included minoritized sexual identities (ie, as “gay,” “lesbian,” “bisexual,” “asexual,” “queer,” “other,” “Two-Spirit,” at any follow-up survey in the study as compared to “straight” at all study follow-ups) and minoritized gender identities (ie, “transgender,” “intersex,” “transexual,” “Two-Spirit,” “genderqueer,” “other” at any follow-up survey in the study as compared to “cisgender” at all study follow-ups). Given the variety of cultures and languages among Indigenous Peoples across Canada and Turtle Island, the term Two-Spirit is drawn on as a tool of community organizing to identify Indigenous peoples who have diverse sexual identities, gender identities, and gender expressions. 28 Prior to colonial contact, Indigenous peoples had terms specific to nations that referred nuanced gender identities and sexualities; the term Two-Spirit thus refers to a variety of nation-specific roles. Community experts could provide multiple answers for sexual and gender identities. Community experts with minoritized sexual identities and gender identities were combined respectively into categories, as there were small sample sizes of respondents in some responses. Further justification for combining responses into 2 categories is from research that has found that minority stress may impact both people with marginalized and minoritized sexual 29 as well as marginalized and minoritized gender 30 identities relative to heterosexual and cis people respectively, shaped by stigma and discrimination. Time-updated variables also included age, criminalized injection drug use frequency (daily, less than daily, vs none); criminalized noninjection drug use frequency (daily, less than daily, vs none); housing insecurity (any living situation aside from living in the same house/apartment for the last 6 months alone, with intimate partner, or shared with family, for example, homeless, living with family/friends, supportive housing, moving in the last 6 months); food insecurity (measured by a version of the Radimer/Cornell Hunger Scale; “often true” or “sometimes true” to at least one item versus “never true” or “not applicable” to all items. 31
Statistical Analysis
Descriptive statistics were calculated for the overall sample and included frequencies and proportions for categorical variables, and measures of central tendencies (ie, mean, medians, and interquartile ranges) for continuous data. Multiple imputations, which assume data is missing at random, were used to impute missing data in multivariable logistic regression models. Twenty datasets were imputed using “proc mi” function in SAS 9.4 (SAS Institute Inc., Cary, NC) with a discriminant function method for categorical binary variables with missing data and the predictive mean matching method for continuous variables. Data was imputed cross-sectionally for each follow-up time point. Variables used in the imputation models included the outcome variables and all other variables considered in descriptive analysis. Multivariable logistic regression models with GEE were fitted on each imputed dataset, with results pooled and averaged using Rubin's formula. We used a bivariate and multivariable logistic model approach using generalized estimating equation (GEE) with an exchangeable correlation structure. The utilization of logistic regression with GEE aided in accounting for time-varying variables, adjusting the standard error to accommodate correlations resulting from repeated measurements among the same community experts over time. All hypothesized confounders were included and results from full models are reported. Multicollinearity was assessed for the final models. Unadjusted (ORs) and adjusted odds ratios (AORs) along with 95% confidence intervals (CIs) were calculated. All P-values were interpreted as 2-sided, and statistical analyses were carried out using SAS software version 9.4 (SAS Institute Inc., Cary, NC).
Results
Of the total of 342 community experts and 2168 observations considered for inclusion in the study over 7 years of observation in this open cohort (September/14–August/21), there were 339 community experts and 2092 community expert observations where a main HIV provider in Metro Vancouver was reported. The minimum, maximum and median (interquartile range, IQR) number of follow-up surveys among community experts in the study was 1-14 and 6(IQR: 3–9) surveys, noting that this was an open cohort and community experts were enrolled at any point between September/14-August/21. Table 1 summarizes baseline characteristics of the study sample of 339 community experts with a main HIV provider. With respect to our 5 outcomes, 296 (87.3%) were on ART, and among those on ART, 269 (90.1%) had HIV medication self-efficacy in the last 3 to 4 weeks, 201 (67.9%) took ART every day for the last 2 weeks, 139 (47.0%) took ART every day for the last month and 116 (39.2%) took ART every day for the last 3 to 4 months. The median age of community experts in the study sample was 44 years (Interquartile range: 37-51 years). A total of 149 (44.1%) reported minoritized sexual identities, and 40 (11.9%) reported minoritized gender identities. Overall, 25 (7.4%) reported transfeminine identities and 9 (2.7%) reported nonbinary identities. There were 189 Indigenous women in the study (55.8%), and Indigenous women were overrepresented compared to the population of Indigenous women in BC; in 2021 approximately 3.0% of the total population of BC was Indigenous women, and 6.0% of women in BC were Indigenous. 32 Among Indigenous community experts, 28 (14.8%) reported Two-Spirit identities. The sample also included 116 (34.2%) White community experts, 20 (5.9%) Black community experts, and 14 (4.1%) other racialized women.
Selected Social-Demographic and Social–Structural Characteristics at Baseline/First Interview of a Study Sample of 339 Women Living With HIV Who Lived in or Access HIV Care in Metro Vancouver, Canada and Who Report Having a Main HIV Provider.
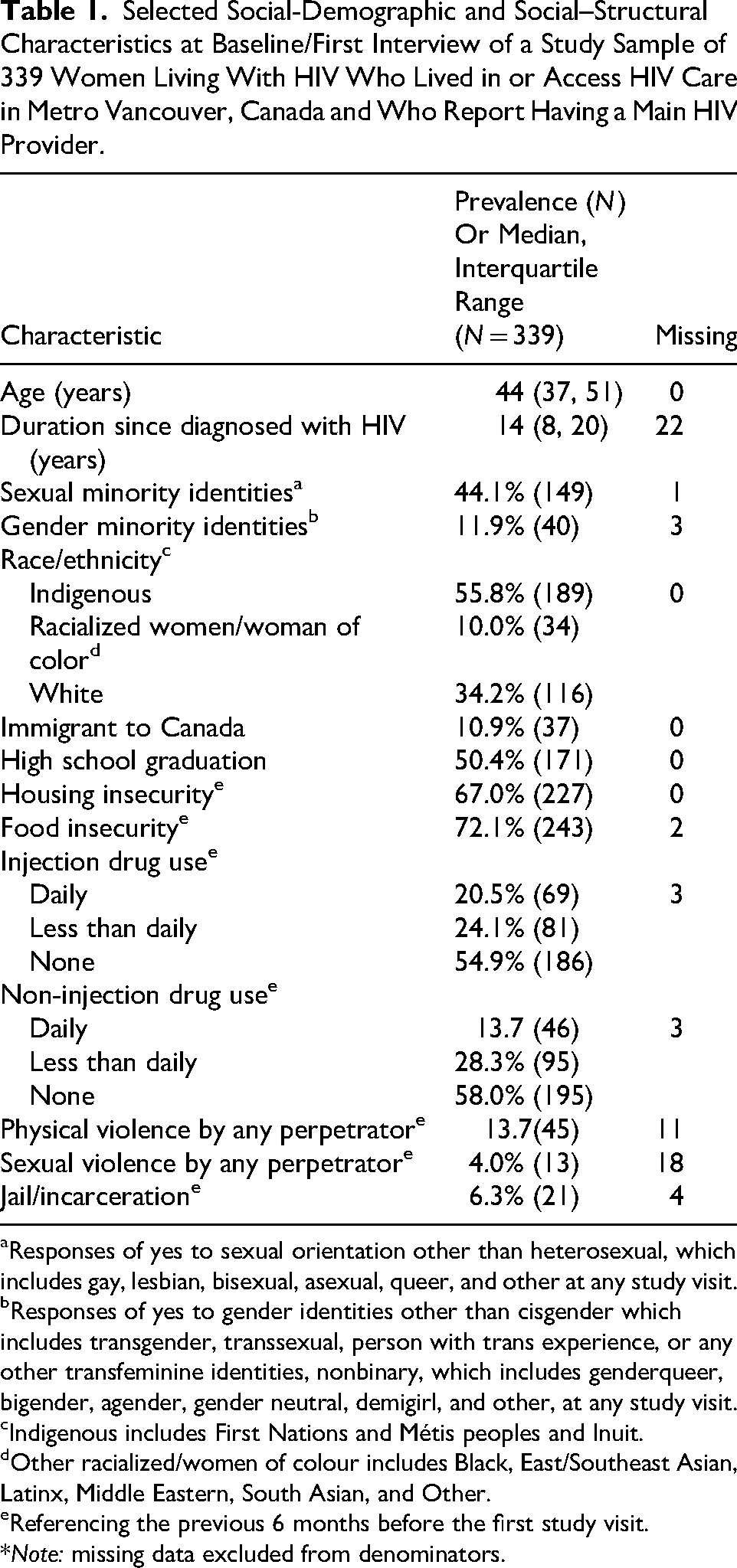
Responses of yes to sexual orientation other than heterosexual, which includes gay, lesbian, bisexual, asexual, queer, and other at any study visit.
Responses of yes to gender identities other than cisgender which includes transgender, transsexual, person with trans experience, or any other transfeminine identities, nonbinary, which includes genderqueer, bigender, agender, gender neutral, demigirl, and other, at any study visit.
Indigenous includes First Nations and Métis peoples and Inuit.
Other racialized/women of colour includes Black, East/Southeast Asian, Latinx, Middle Eastern, South Asian, and Other.
Referencing the previous 6 months before the first study visit.
*Note: missing data excluded from denominators.
Table 2 presents the prevalence of 18 variables representing characteristics of women's self-reported positive experiences with their main HIV care provider/clinics at baseline grouped into 5 principles within a trauma- and violence-informed practice framework. For nearly all of the variables, the majority of community experts reported that the care they received from HIV providers had positive characteristics with respect to trauma- and violence-informed practice principles, with the highest prevalence characteristics being: “I feel safe at the clinic” (93.0%, n = 304), “I feel respected by clinic staff” (92.0%, n = 301), and “I feel like other parts of my life besides HIV are treated as important” (91.7%, n = 298); while the lowest prevalence characteristics were: “My children are welcome at the clinic” (43.3%, n = 141) and “There are peer support/groups for people with my culture” (58.3%, n = 190).
Prevalence of Trauma- and Violence-Informed Characteristics of Current HIV Care Providers Among 339 Women Living With HIV in Metro Vancouver at Their Baseline/First Interview, All Variables Measured in the Last 6 Months.
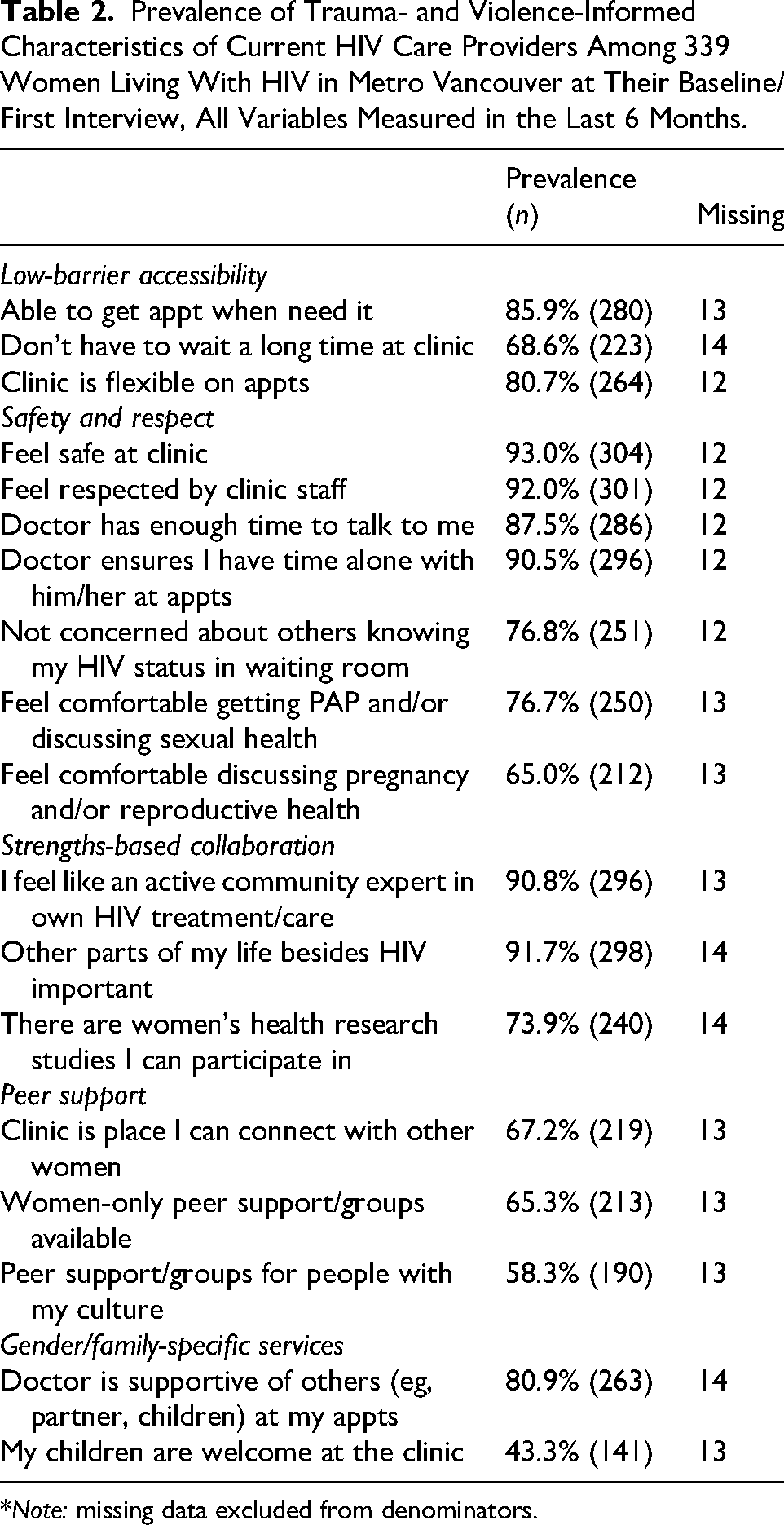
*Note: missing data excluded from denominators.
Table 3 presents results from multivariable logistic regression for the relationships between the 18 variables representing women's self-reported positive experiences with their main HIV care provider/clinics and the 5 HIV treatment and care outcomes, adjusted for confounders.
Adjusted Odds Ratios and 95% Confidence Intervals for the Relationship Between Women's Self-Reported Positive Experiences With Their Main HIV Care Provider/Clinics and Five Outcomes Representing Different Aspects of the HIV Care continuum.a
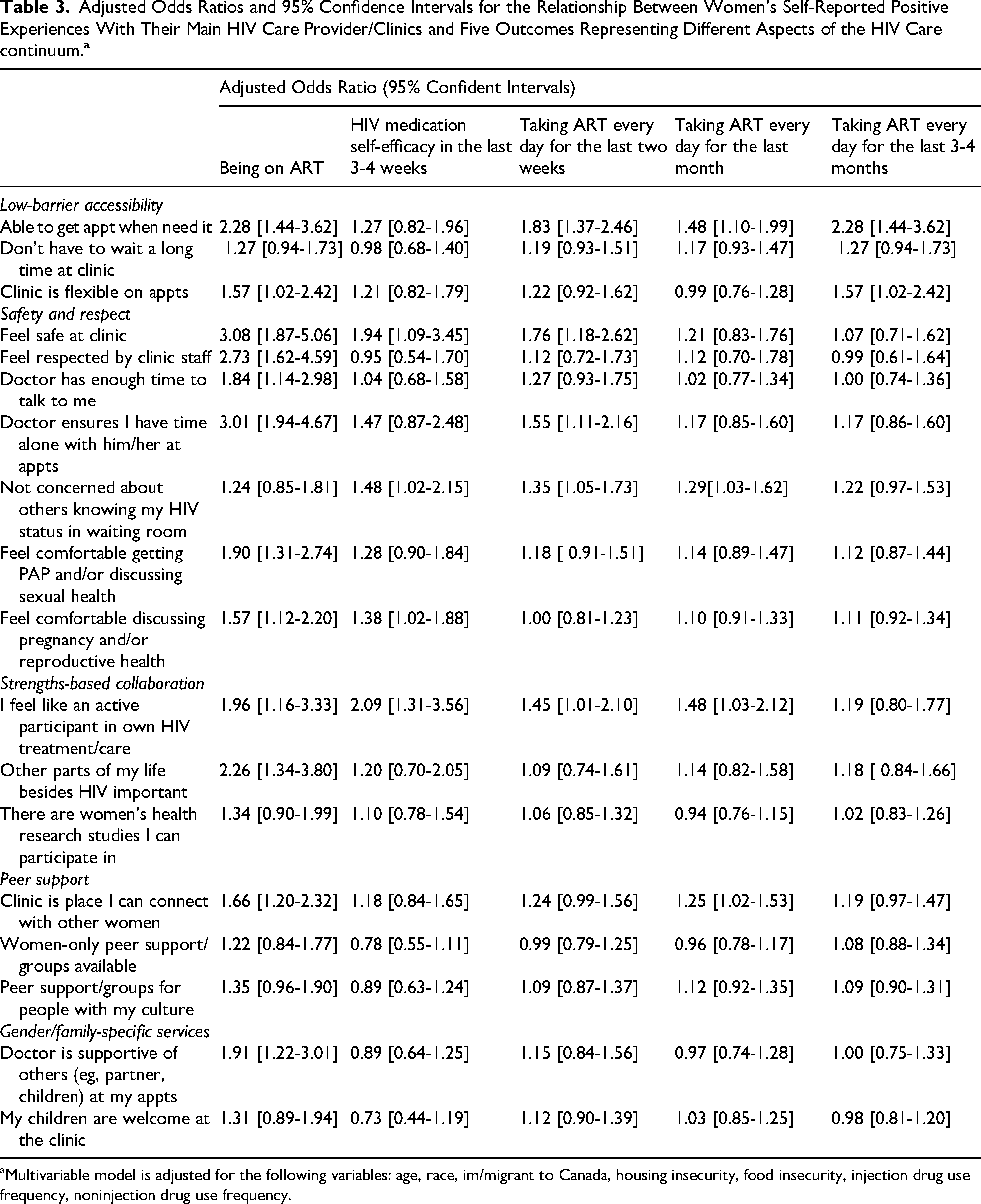
Multivariable model is adjusted for the following variables: age, race, im/migrant to Canada, housing insecurity, food insecurity, injection drug use frequency, noninjection drug use frequency.
Many variables were significantly associated with being on ART, including those grouped under “low-barrier accessibility” (“I am able to get an appointment when I need one,” AOR: 2.28 [1.44-3.62]; and “The clinic is flexible on appointments,” AOR: 1.57 [1.02-2.42]), “safety and respect” (“I feel safe at the clinic,” AOR: 3.08 [1.87-5.06]; “I feel respected by clinic staff, AOR: 2.73 [1.62-4.59]; “The doctor has enough time to talk to me,” AOR: 1.84 [1.14-2.98]; “I feel comfortable getting my pap and/or discussing sexual health,” AOR: 1.90 [1.31-2.74]); and “I feel comfortable discussing my pregnancy and reproductive needs” AOR: 1.57 [1.12-2.20]), “strength-based collaboration” (“I feel like an active community expert in my own HIV treatment/care,” AOR: 1.96 [1.16-3.33]; “Other parts of my life besides HIV are treated as important,” AOR: 2.26 [1.34-3.80]), “peer support” (“The clinic is a place I can connect with other women,” AOR: 1.66 [1.20-2.32]; and “gender/family-specific services” (“The doctor is supportive of others at my appointments,” AOR: 1.91 [1.22-3.01]).
Variables under the principles of “safety and respect” (“I feel safe at the clinic,” AOR: 1.94 [1.09-3.45]; “I am not concerned about others knowing my HIV status in the waiting room,” AOR: 1.48 [1.02-2.15]; “I feel comfortable discussing my pregnancy and/or reproductive health needs,” AOR: 1.38 [1.02-1.88]) and “strength-based collaboration” (“I feel like an active community expert in my own HIV treatment/care,” AOR: 2.09 [1.31-3.56]) were significantly associated with positive HIV medication self-efficacy.
The “low-barrier/accessibility” variable, “I feel able to get an appointment when I need it” was significantly associated with the 3 measures of consistency/regularity of ART use, including not missing ART in the last 2 weeks (AOR: 1.83 [1.37-2.46]), not missing ART in the last month (AOR: 1.48 [1.10-1.99]) and not missing ART in the last 3-6 months (AOR: 1.42 [1.07-1.89]). Variables under “safety and respect” and “strength-based collaboration” principles were associated with the former 2 outcomes, with “I am not concerned about others knowing my HIV status in the waiting room” and “I feel like an active community expert in my own HIV treatment/care” being associated with both not missing HIV medication in the last 2 weeks (AOR: 1.35 [1.05-1.73] and AOR: 1.45 [1.01-2.10], respectively) and not missing HIV medication in the last month (AOR: 1.29 [1.03-1.62]; and AOR: 1.48 [1.03-2.12]respectively). Finally, “I feel safe at the clinic” (AOR: 1.76 [1.18-2.62]) and “The doctor ensures I have time alone with him/her at appointments” (AOR: 1.55 [1.11-2.16]) were significantly associated with not missing HIV medication in the last 2 weeks and the “peer support” variable “The clinic is a place I can connect with other women” was significantly associated with not missing HIV medication in the last month (AOR: 1.25 [1.02-1.53]).
Discussion
Our study on women's self-reported positive experiences with their main HIV care provider/clinics provides evidence that incorporating key characteristics of trauma- and violence-informed practice within women's HIV care, particularly principles of “safety and respect” (eg, feeling safe, feeling respected at the clinic; feeling safe discussing sexual and/or reproductive health, confidentiality) and “strength-based collaboration” (eg, agency in scheduling, actively participating on one's own care) are associated with optimal HIV treatment and care.
In this study we have taken a set of 18 measures representing women's self-reported positive experiences with their main HIV care provider/clinics within 5 principles within a trauma- and violence-informed framework, drawing on foundational work by SAMHSA in developing principles related to trauma-informed care among people living with mental health conditions and addictions. 33 The choice to contextualize these measures within a trauma- and violence-informed framework was driven by community and advocates calls to acknowledge high levels of social and structural violence experienced by women living with HIV, including overlapping trauma, mental health and addictions. A trauma- and violence-informed approach aligns well with other principles and frameworks. In particular, person-centered care recognizes patients as persons with diverse backgrounds, knowledge, resources and abilities, rather than only focusing on the person's health conditions and associated biomedical treatment. Person-centered care acknowledges and prioritizes lived experiences alongside evidence-based practice and the importance of collaboration in health care plans between providers and patients. 34 Trauma- and violence-informed care and practice specifically acknowledges and elevates the critical role that lived experiences of trauma and violence may play in shaping health and social inequities and how people engage with others and in their treatment and care and suggests appropriate responses to support patients in accessing care. Many of the statements asked of community experts in our study, including those relating to relationship-based care (eg, “I feel respected by clinic staff”), involvement in decision-making (eg, “I feel like an active community expert in my HIV treatment and care”) and general care environments (eg, “I am able to get an appointment when I need one”), associated with optimal HIV care continuum outcomes, concurrently fit well as statements that represent best practices within both person-centered and trauma- and violence-informed care models. 35
Given these intersections, it is productive to map women's self-reported positive experiences with their main HIV care provider/clinics under multiple frameworks. Indeed, “person-centered” and “trauma- and violence-informed” care are frameworks that are increasingly used together. Importantly, the concept of “Women-Centered HIV Care,” developed over the last decade by Canadian researchers 7 to fill a critical gap in existing theory and practice of HIV care among women living with HIV, brings many core principles and ideas together under one comprehensive model for the optimal provision of care among women living with HIV. Drawing on a community-engaged approach, the Women-Centered HIV Care model has identified 6 key components of HIV care among women and gender-diverse people, with a foundation of trauma- and violence-aware and person-centered care, alongside sexual and reproductive health care and rights, mental health and addiction care, and peer support, leadership and capacity building. Our study findings fit well within this framework as well as previous research suggesting associations between person-centered and many positive health services access outcomes (eg, shorter duration of time in hospital stays, lower readmission rates, higher perceived quality of and satisfaction with healthcare). 36 Interestingly, while some measures related to safety and respect (eg, “I feel safe at the clinic,” “I am not concerned about others knowing my HIV status in the waiting room”) and strengths-based collaboration (eg, “I feel like an active community expert in HIV treatment and care”) were associated with shorter-term 100% ART use consistency (within 2 weeks, 1 month), only the statement “I am able to get an appointment when I need it” was associated with longer-term 100% ART use consistency (within 3 months). Future research should explore if and why some care provider characteristics are more likely to result in sustained optimal HIV treatment and care.
Promisingly, our results suggest that most women in our study access HIV care that have positive experiences with their main HIV care provider/clinics. This is something to celebrate, while also a reminder to continue to work toward the goal of having all women living with HIV being able to access care they perceive as positive. In our setting, Metro Vancouver, Canada, women living with HIV access HIV treatment and care from a variety of different providers, including nurse practitioners, family physicians and infectious diseases specialist physicians. The Oak Tree Clinic is the primary referral clinic for women living with HIV and provides a comprehensive model of women-centered and trauma- and violence-informed HIV care with women living with HIV in Metro Vancouver. 27 Other settings where women living with HIV access HIV care include community health clinics, hospital-based clinics and independent physician offices, all of which may incorporate trauma-and-violence-informed and aligned principles in various ways on a health provider- or clinic-level. A limitation of the use of conceptual approaches to healthcare provision is that they are not always accessible to providers in a meaningful and practical way. 36 There is increasingly practical guidance on how to operationalize trauma- and violence-informed principles into practice. For example, accessible training materials including workshops on how to implement a trauma- and violence-informed practice intervention among marginalized populations in 3 diverse emergency room settings is published publicly .37,38 In this intervention, evidence suggested nonsignificant trends toward improvement of patients’ experiences with discrimination and significant decrease in the percentage of patients who left without care being completed. 39 Extensive work has been undertaken to disseminate knowledge and recommendations of a toolkit outlining the Women-Centered HIV Care model, which includes core components of both person-centered and trauma- and violence-aware care. 9 Education, training and public webinars have been used to disseminate the toolkit.
According to the SAMHSA framework, 10 implementation domains (eg, governance and leadership, policy, physical environment, training and workforce development) need attention for clinics to effectively implement trauma- and violence-informed practice, 33 with many of these steps requiring substantial investment in time and resources. RWHAP clinics can access SAMHSA resources as well as the “Trauma- and Violence-Informed Approaches Toolkit,” a set of comprehensive resources developed by National Alliance of State and Territorial AIDS Directors. 40 However, research suggests that resource and financial constraints limit the ability of RWHAP and other clinics to implement trauma- and violence-informed care. 41 Recent studies of administrators, providers and staff in RWHAP clinics have identified that there is individual support for trauma- and violence-informed care and practice, with community experts perceiving this type of care as effective, preferred by and beneficial to patients, and timesaving over the longer term.41,42 Facilitators to systems-level support in RWHAP clinics are strong staff culture and resource availability and facilitators to personal- and systems-level support for implementation included stronger leadership support and reduced burnout. 41 Stress and burnout in particular in the context of high patient loads and lack of resources, alongside a lack of resources on self-care and how to provide appropriate care for patients who have experienced trauma have been identified in RWHAP clinics.42,43 Many of these challenges are echoed widely among health providers and settings across Canada and the United States. Individual- and systems-level support needs to be strengthened in clinics and health systems to implement site- and setting-specific trauma-and violence-informed practice.
This study had limitations as well as strengths. Our study's smaller sample size may not provide power to detect some associations. However, because we draw on multiple measurements over time in our longitudinal study approach, effective sample size is increased. Our study may not be representative of all women living with HIV in Metro Vancouver nor be generalizable to other settings. Given that our study population is highly marginalized and criminalized, our study sample is not a probability-based sample; the study was open for recruitment for its duration and study community experts were enrolled until the study ended. However, recruitment of study community experts for this study is achieved by broad coverage of diverse HIV community-based organizations and clinical settings, and we feel that our sample reflects the diversity of women living with HIV. Our study includes self-report data, which can be subject to social desirability bias, as well as recall bias. We are confident in the training and experience of our community and clinical research interviewers in safe and supportive interview approaches to minimize these biases. Finally, we can only draw on women's self-reported positive experiences with their main HIV care provider/clinics rather than observing interactions between HIV providers and patients, or measure experiences HIV providers themselves. Thus, from this study, we can only draw the conclusions about the association between patients’ positive experiences in health care and HIV outcomes, not the association between objective trauma- and violent-informed practices by providers and HIV outcomes. Nevertheless, elevating and centering women's self-reported experiences of care remains critical, as these accounts reflect how health care is actually received and interpreted by patients, shape trust and engagement with services, and represent meaningful indicators of whether care environments are experienced as safe, respectful, and responsive to trauma and violence.
Given the overrepresentation of Indigenous, Black and other racialized women/women of color relative to the overall population among women living with HIV and historical and ongoing colonial and structural violence that shapes access to health services, intersections with culturally safe and culturally appropriate care need also the be integrated alongside trauma- and violence-informed and person-centered practice. Future research should understand how trauma- and violence-informed HIV care and practice intersects with overlapping systems of oppression and violence to mitigate the effects of structural violence on suboptimal health access outcomes and seek to identify how approaches should be tailored to meet the needs of diverse women living with HIV. Research with women living with HIV and providers should be done to better understand, interpret and modify dimensions of trauma- and violence-informed and aligned HIV care principles, how these can be implemented into care and practice in practical ways.
Our study has important implications for HIV care and practice for women living with HIV in Metro Vancouver and beyond. We provide suggestions for how to consider women's self-reported positive experiences with their main HIV care provider/clinics within the SAMHSA trauma- and violence-informed care framework, which can be modified for other contexts and populations and considered alongside other frameworks. Our study results suggested that women's self-reported positive experiences with their main HIV care provider/clinics, particularly principles of “safety and respect” (eg, feeling safe discussing sexual and/or reproductive health, confidentiality) and “strength-based collaboration” (eg, agency in scheduling, actively participating on one's own care) were associated with multiple optimal HIV care continuum outcomes. Given high prevalence of trauma and violence experienced by women living with HIV in Metro Vancouver and globally, our study provides evidence for the benefit of incorporating and scaling up education, training and health systems policies that support women's positive experiences with their main HIV care provider/clinics in a trauma- and violence-informed framework.
Footnotes
Acknowledgments
First and foremost, we want to thank SHAWNA community experts/participants for sharing their experiences with us. We also want to thank our PWAB and our Community Advisory Board. We want to thank the current SHAWNA team of project and statistical staff and trainees including Elle Aikema, Wiebke Bartels, Suiqiong Fan, Parisa Kabir, Desire King, Beatrix Lehmann, Melanie Lee, Mika Ohtsuka, Rhiannon Owen, Sagar Pannu, Amanda Tallio, Colleen Thompson, Esteban Valencia, and Charlie Zhou. We also thank the current administrative/operations/knowledge translation staff supporting SHAWNA, including Esther Ibu, and Peter Vann. We also thank our Study Physician, Dr Mary Kestler.
Ethical Considerations
The data for this study were drawn from the SHAWNA Project, which is approved through the University of British Columbia/Providence Health Care Research Ethics Board (Reference No. H14-01073).
Consent to Participate
All participants provide informed consent to participate in this study, either written or verbal, if the interview is conducted over the phone/online.
Author Contributions
KD was responsible for writing, editing, and leading the conceptualization of the manuscript; DK, CT, and KS were responsible for contributing to some of the conceptual framing of the manuscript, editing, and giving feedback; DK and CT were further responsible for collecting and managing the data; HZ was the statistician/analyst on the project and conducted all analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SHAWNA research was supported by grants from the Canadian Institutes of Health Research (PJT—169119), the National Institutes of Health (1R01MH123349), and the Canadian HIV Trials Network (CTN-333). KD was supported through a Michael Smith Foundation for Health Research Scholar Award.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions related to confidentiality and the sensitivity of these data collected with a highly criminalized and marginalized population. These restrictions on sharing data beyond the study team are imposed by the Providence Health Care/University of British Columbia Research Ethics Board. Data are available on reasonable request and subject to approval by the Providence Health Care/University of British Columbia Research Ethics Board by emailing julie.hadden@ubc.ca.