
Abstract
Background
Combination of antiretroviral therapy (cART) has improved the life expectancy of HIV patients. Yet, it can also increase the risk of metabolic dysfunction, including dyslipidemia and diabetes mellitus (DM). Despite this, local data on the prevalence and risk factors for dyslipidemia and DM are limited. In addition, prognostic tools for regular monitoring and thereby the early detection of metabolic dysfunction have yet to be validated among cART-treated patients.
Methods
A hospital-based cross-sectional study was conducted at Nekemte Specialized Hospital (Western Ethiopia) from February to April 2025. A total of 176 cART-treated HIV patients were purposively selected for the study. Socio-demographic, anthropometric, and metabolic parameters were assessed, and their associations with dyslipidemia and DM were evaluated using univariate (bivariate) and multivariable regression analyses. The predictive performances of lipid index-based prognostic tools were assessed using receiver operating characteristic curve analysis.
Results
Dyslipidemia and previously undiagnosed DM were observed among 54.5% and 9.7% of participants, respectively. Significant risk factors included family history of DM (AOR = 4.5), frequent alcohol use (AOR = 5.2), age greater than 40 years (AOR = 3.4), sedentary lifestyle (AOR = 5.6), frequent consumption of traditional spiced milk butter (AOR = 5.2), elevated TyG-WC (AOR = 6.7), and high VAI (AOR = 8.7). TyG-WC had the highest predictive performance for dyslipidemia (AUC = 0.795) with an optimal cutoff of 434.1, followed by TyG-BMI (cutoff 128.5), LAP (cutoff 34.5), and VAI (cutoff 1.91).
Conclusion
Dyslipidemia and undiagnosed diabetes remain highly prevalent among cART-treated HIV patients compared to the general population. In addition to commonly recognized risk factors, frequent consumption of a high-fat, carbohydrate-restricted diet like Nitter kibbeh may influence metabolic outcomes in this sub-population, highlighting the need for further research. Lipid indices, particularly TyG-WC, appear to be feasible tools for routine monitoring and early prediction of metabolic dysfunction. Revising population-specific thresholds could further improve early detection in this group.
Plain Language Summary Title
Prevalence and Predictors of Dyslipidemia and Diabetes Mellitus Among cART-Treated HIV Patients in Western Ethiopia: A Cross-Sectional Study
Background
Combination of antiretroviral therapy (cART) has improved the life expectancy of HIV patients. Yet, it can also increase the risk of metabolic dysfunction; despite this, local data are limited.
Methods
A hospital-based cross-sectional study was conducted at Nekemte Specialized Hospital from February to April 2025. A total of 176 cART-treated HIV patients were purposively selected for the study. Socio-demographic, anthropometric, and metabolic parameters were assessed, and their associations were evaluated using univariate and multivariable regression analyses.
Results
Dyslipidemia and previously undiagnosed Diabetes mellitus (DM) were observed among 54.5% and 9.7% of participants, respectively. Significant risk factors included family history of DM, frequent alcohol use, age greater than 40 years, sedentary lifestyle, elevated TyG-WC, and VAI.
Conclusion
Dyslipidemia and undiagnosed DM remain highly prevalent among cART-treated HIV patients compared to the general population. This highlights the need for routine monitoring and screening for early detection.
Keywords
Introduction
The WHO reports that diabetes is among the top 10 global health challenges, affecting over half a billion people and causing more than 4 million deaths since 2018, with nearly two-thirds of the burden occurring in Africa. 1 Global healthcare spending on diabetes, estimated at USD 760 billion in 2019, is projected to rise to USD 845 billion by 2045. 2 The prevalence of undiagnosed DM in Ethiopia among health individuals ranges from 2.3% to 14.7%,3–6 among combination antiretroviral therapy (cART) treated patients was ranges from 7.9% to 11.4%,3,4,7 and 5.6% and 7.6% among naïve HIV patients.4,8 From different systematic reviews the overall prevalence of dyslipidemia among naïve and cART treated HIV patients was 61.46% and 69.74% 9 respectively and 56.6% among healthy individuals. 10
Although antiretroviral therapy (ART) has greatly improved the lifespan of HIV patients, it is linked to metabolic complications, particularly with nucleoside reverse transcriptase inhibitors (NRTI), non-nucleoside reverse transcriptase inhibitors (NNRTI), and protease inhibitors (PIs) based regimens.11–14 HIV infection itself can also contribute to these complications through viral factors, including accessory proteins such as Vpr, Nef, and Tat, which induce the release of inflammatory cytokines (IL-6, TNF-α, and IL-2). Additional host-related risk factors, such as smoking, alcohol consumption, unhealthy diet, and physical inactivity, further increase the likelihood of metabolic and cardiovascular complications,15,16 especially in the absence of early diagnosis.
Regular clinical follow-up of HIV patients receiving cART not only reduces the risk of metabolic complications but also provides substantial economic benefits by preventing the high direct and indirect costs of managing these conditions.17–19 Moreover, patients who develop diabetes or dyslipidemia face higher rates of antiretroviral drug resistance and ischemic heart disease compared with cART-treated individuals without such metabolic disorders, underscoring the clinical and economic value of early detection and intervention.9,13,14,20,21
Nekemte town has experienced increasing population mobility and urban pressures, contributing to lifestyle-related risk factors such as stress, substance use, and unsafe sexual practices.22,23 These conditions increase vulnerability to HIV infection, reflected in the town's estimated HIV burden of about 3.5%. 24 Such factors may also exacerbate metabolic complications—including dyslipidemia and glucose abnormalities—among HIV patients on cART, highlighting the need for strengthened screening and preventive care.
Therefore, this study investigates the prevalence and risk factors of undiagnosed diabetes and dyslipidemia among cART-treated HIV patients in western Ethiopia, addressing the critical gap in local data needed to guide early detection and targeted intervention strategies.
Methods
Study Design and Setting
A cross-sectional study was conducted from February to April 2025 at the ART clinic of Nekemte Specialized Hospital (NSH), and the study was reported in accordance with the STROBE statement guideline for observational studies. NSH is located in Nekemte town, the capital of East Wollega Zone, Oromia Region, Ethiopia. Since 2015, NSH has provided comprehensive HIV services—including diagnosis, treatment, and monitoring—for over 7200 patients on cART.
Study Population, Sample Size, and Sampling
The number of study subjects needed for this study was calculated from a study conducted in Jimma, which reported the prevalence of DM in cART-treated HIV patients as 11.4%. 25 Sample size was calculated using the single population proportion formula by using 0.05% expected margin of error, with 95% confidence interval (CI). Since the total population was less than 10,000, we used the correction formula. By adding 20% non-respondents, we finally got 176 study subjects. HIV-positive adults aged ≥18 years who had been on cART for at least 1 year and were registered at the ART clinic were eligible for this study, and pregnant Mothers, patients with known DM and Dyslipidemia before cART, and those with other metabolic disorders, such as thyroid disorder, Cushing's syndrome, were excluded from this study. A total of 176 consenting participants visiting NSH's ART clinic during the study period were recruited using a purposive sampling technique.
Data Collection and Laboratory Analysis
Data collection was conducted after obtaining ethical approval from the Departmental Research Ethics and Review Committee (DRERC) and permission from the Hospital's Medical Director. Socio-demographic and behavioral information was then gathered using an adapted structured questionnaire, following the acquisition of written informed consent from participants.
Operational Definitions
Dyslipidemia was defined according to the National Cholesterol Education Program Adult Treatment Panel III (NCEP–ATP III) 26 criteria which classify individuals as dyslipidemic if any of the following were present: TC ≥ 200 mg/dL, TG ≥ 150 mg/dL, HDL-C < 40 mg/dL, or LDL-cholesterol (LDL-C) ≥ 130 mg/dL.
Diabetes mellitus (DM) was defined using the World Health Organization (WHO) 27 diagnostic criteria as a fasting blood glucose concentration > 125 mg/dL.
Statistical Analysis
Data were entered into SPSS Version 27, cleaned, and checked for normality. Descriptive statistics summarized participant characteristics. Bivariate logistic regression assessed associations between dyslipidemia or DM and potential risk factors. Variables with P
Results
Scio-Demographic Characteristics
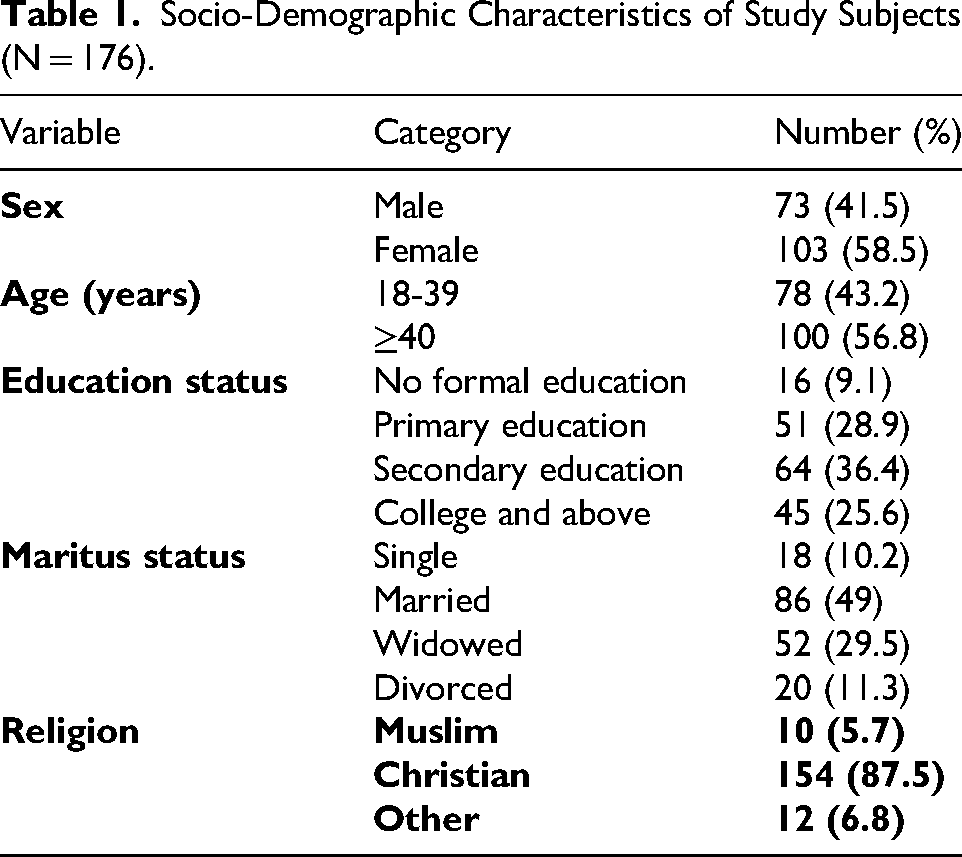
A total of 176 adults receiving cART were enrolled. The majority were female (58.5%), above the age of 40 (56.8%). Key socio-demographic characteristics are summarized in Table 1.
Socio-Demographic Characteristics of Study Subjects (N = 176).
Lifestyle and Socio-Behavioral Characteristics
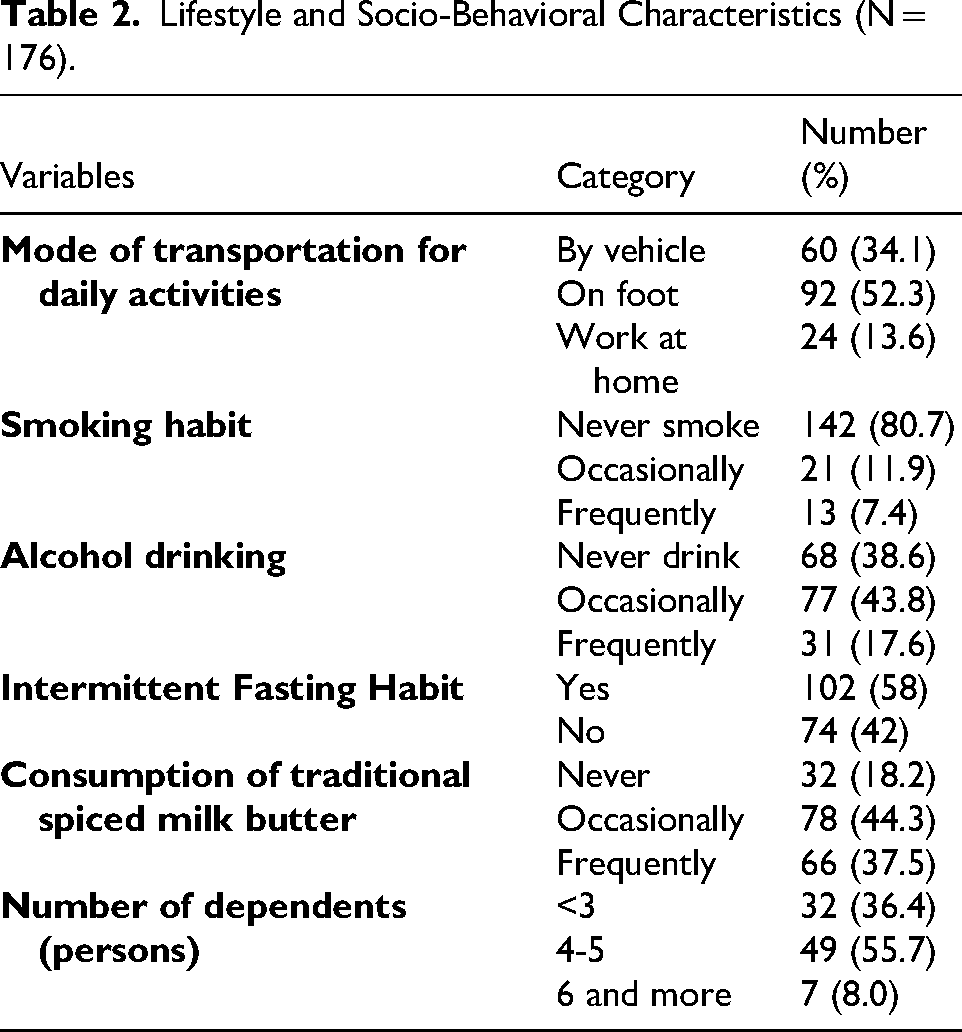
Most participants were non-smokers (80.7%), occasional alcohol drinkers (43.8%), and had an intermittent fasting habit (58%). Most of the subjects were primary breadwinners for 4-5 dependents (55.7%), reflecting both household responsibility and socio-economic pressures (Table 2).
Lifestyle and Socio-Behavioral Characteristics (N = 176).
Clinical and Metabolic Profiles
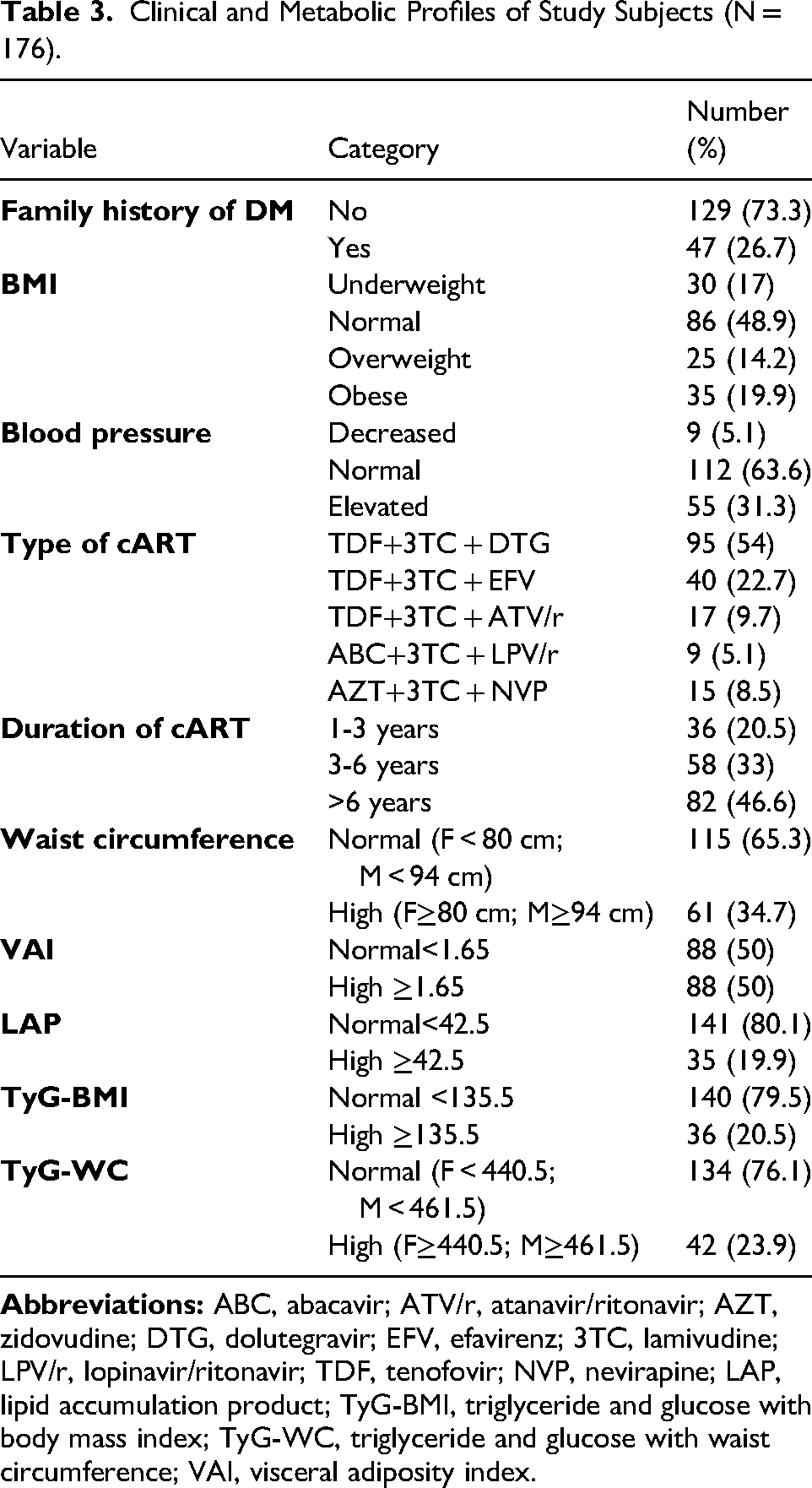
Among the 176 cART-treated HIV patients, 26.7% had a family history of diabetes. Nearly half had normal BMI (48.9%), while 34.1% were overweight or obese. Elevated blood pressure was observed in 31.3% of participants. Most patients were on a first-line cART regimen, TDF+3TC + DTG (54%), with 46.6% receiving cART for over 6 years. About one-third had high WC (34.7%), and half showed elevated visceral adiposity index (VAI ≥1.65). Most participants had normal lipid accumulation product (LAP <42.5, 80.1%) and TyG indices (TyG-BMI <135.5, 79.5%; TyG-WC <461.5 M/ < 440.5 F, 76.1%), highlighting key metabolic and anthropometric profiles relevant to diabetes and dyslipidemia risk (Table 3).
Clinical and Metabolic Profiles of Study Subjects (N = 176).
Prevalence of DM and Dyslipidemia
Among the 176 study participants, 17 (9.7%) subjects had undiagnosed DM, and 96 (54.5%) subjects had at least 1 abnormal lipid profile. Specifically, 39 participants (22.2%) had TC ≥200 mg/dL, 34 (19.3%) had TG ≥150 mg/dL, 63 (35.8%) had HDL cholesterol <40 mg/dL, and 24 (13.6%) had LDL cholesterol ≥130 mg/dL (Table 4).
Prevalence of Diabetes Mellitus and Dyslipidemia.
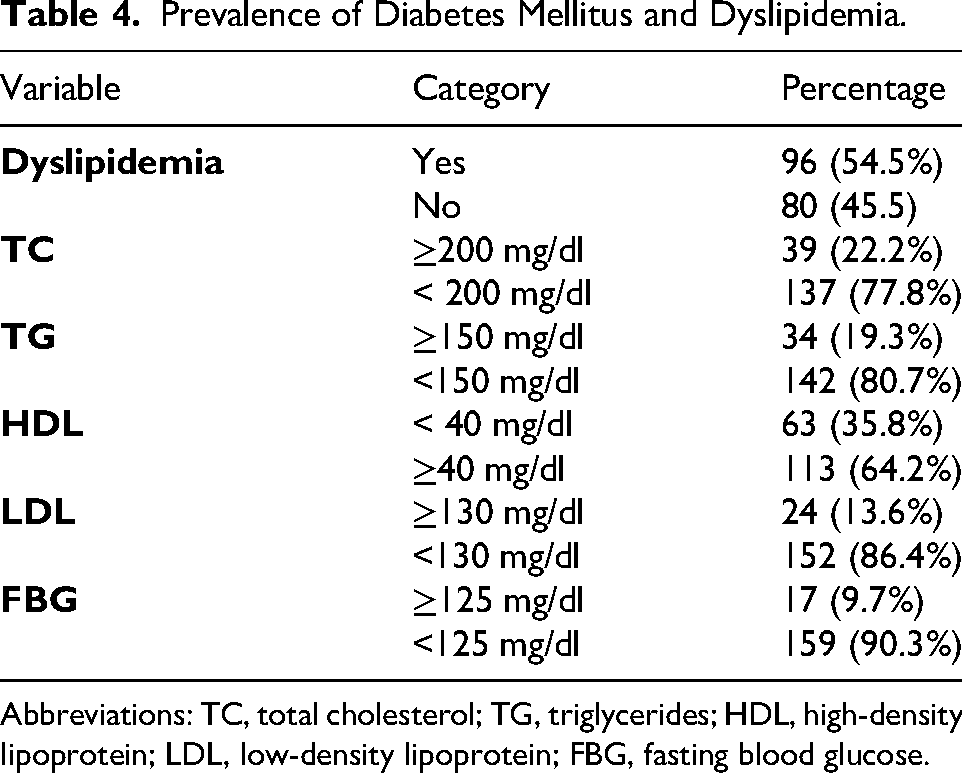
Abbreviations: TC, total cholesterol; TG, triglycerides; HDL, high-density lipoprotein; LDL, low-density lipoprotein; FBG, fasting blood glucose.
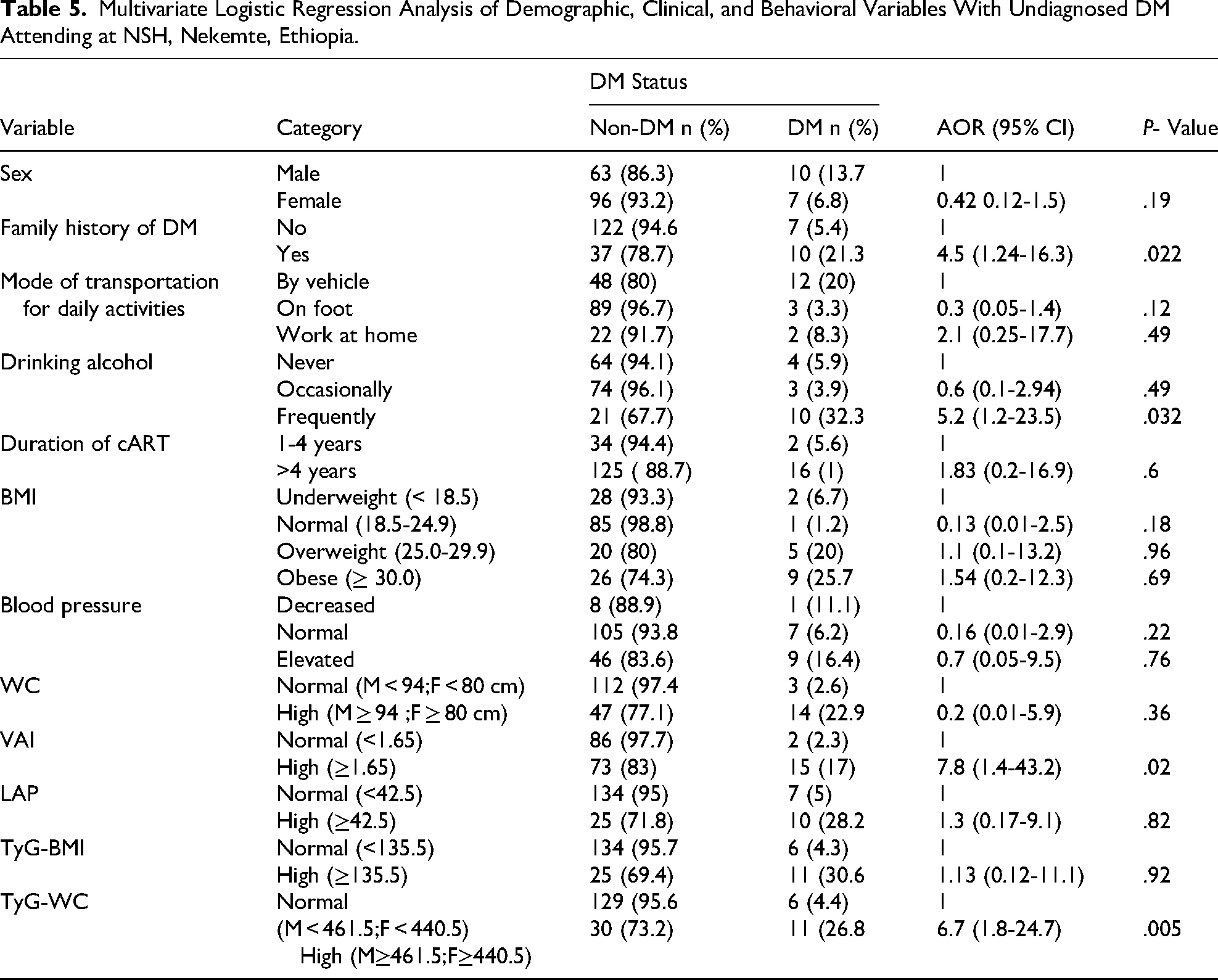
Risk Factors Associated With DM
After adjustment, 4 factors remained significantly associated with DM. Family history of diabetes had 4.5-times higher odds of developing DM (AOR = 4.5; 95% CI: 1.24-16.3; P = .022). Frequent alcohol consumption was also significantly associated with DM (AOR = 5.2; 95% CI: 1.2-23.5; P = .032). In addition, individuals with elevated VAI values had 7.8 times higher odds of DM (AOR = 7.8; 95% CI: 1.4-43.2; P = .02), while those with high TyG-WC showed a similarly strong association (AOR = 6.7; 95% CI: 1.8-24.7; P = .005) (Table 5).
Multivariate Logistic Regression Analysis of Demographic, Clinical, and Behavioral Variables With Undiagnosed DM Attending at NSH, Nekemte, Ethiopia.
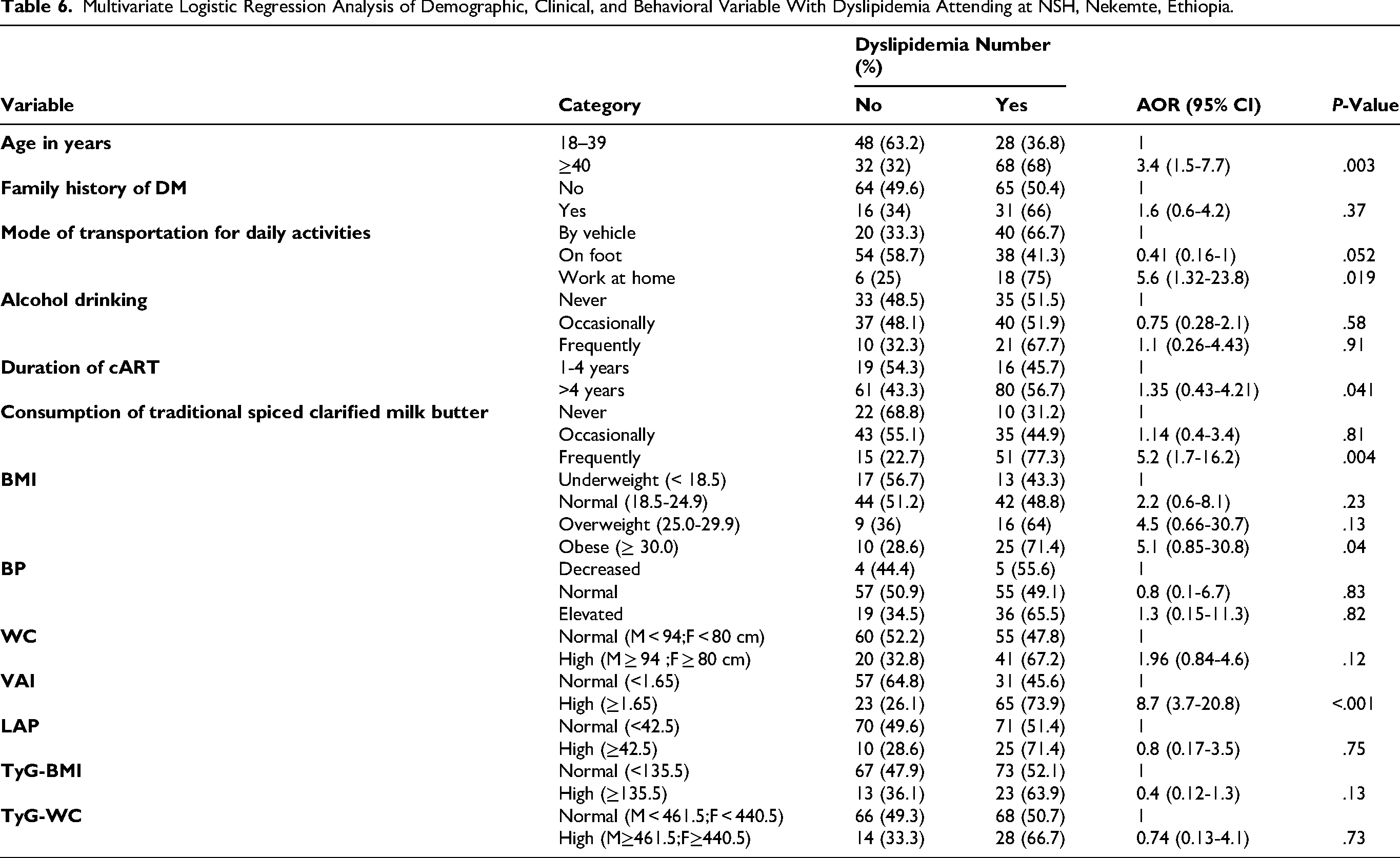
Risk Factor Associated With Dyslipidemia
In the multivariate model, participants aged ≥40 years were more likely to have dyslipidemia compared to those aged 18-39 years (AOR = 3.4; 95% CI: 1.5-7.7; P = .003). Those with a sedentary lifestyle, such as working at home, also had higher odds of dyslipidemia (AOR = 5.6; 95% CI: 1.32-23.8; P = .019). Frequent consumption of traditional spiced clarified milk butter was associated with increased risk (AOR = 5.2; 95% CI: 1.7-16.2; P = .004), and participants with a high VAI (VAI ≥1.65) had the strongest association (AOR = 8.7; 95% CI: 3.7-20.8; P < .001). Other variables, including BMI, blood pressure, WC, and lipid accumulation product (LAP), were not independently associated with dyslipidemia after adjusting for confounders (Table 6).
Multivariate Logistic Regression Analysis of Demographic, Clinical, and Behavioral Variable With Dyslipidemia Attending at NSH, Nekemte, Ethiopia.
Association of Lipid Indices With Lipid Profile and Fasting Glucose
Our Study Participants with longer duration of cART (>4 years) had slightly higher TG and lower HDL-C and LDL-C (P < .05). Higher BMI, WC, VAI, LAP, and TyG-BMI/WC were generally associated with elevated TC, TG, LDL-C, and FBS, while HDL-C tended to be lower in participants with higher visceral adiposity or lipid accumulation indices. Blood pressure and BMI categories also showed significant differences in TC, LDL-C, and FBS (P < .05). Overall, indices reflecting visceral adiposity and lipid accumulation were strongly associated with dyslipidemia and impaired glucose metabolism in this cohort (Table 7).
Median and 95% Reference Value for Lipid Profile Components (TC, TG, HDL-C, LDL-C) and Fasting Blood Sugar (FBS) Stratified by Clinical, Anthropometric, and Metabolic Indices.
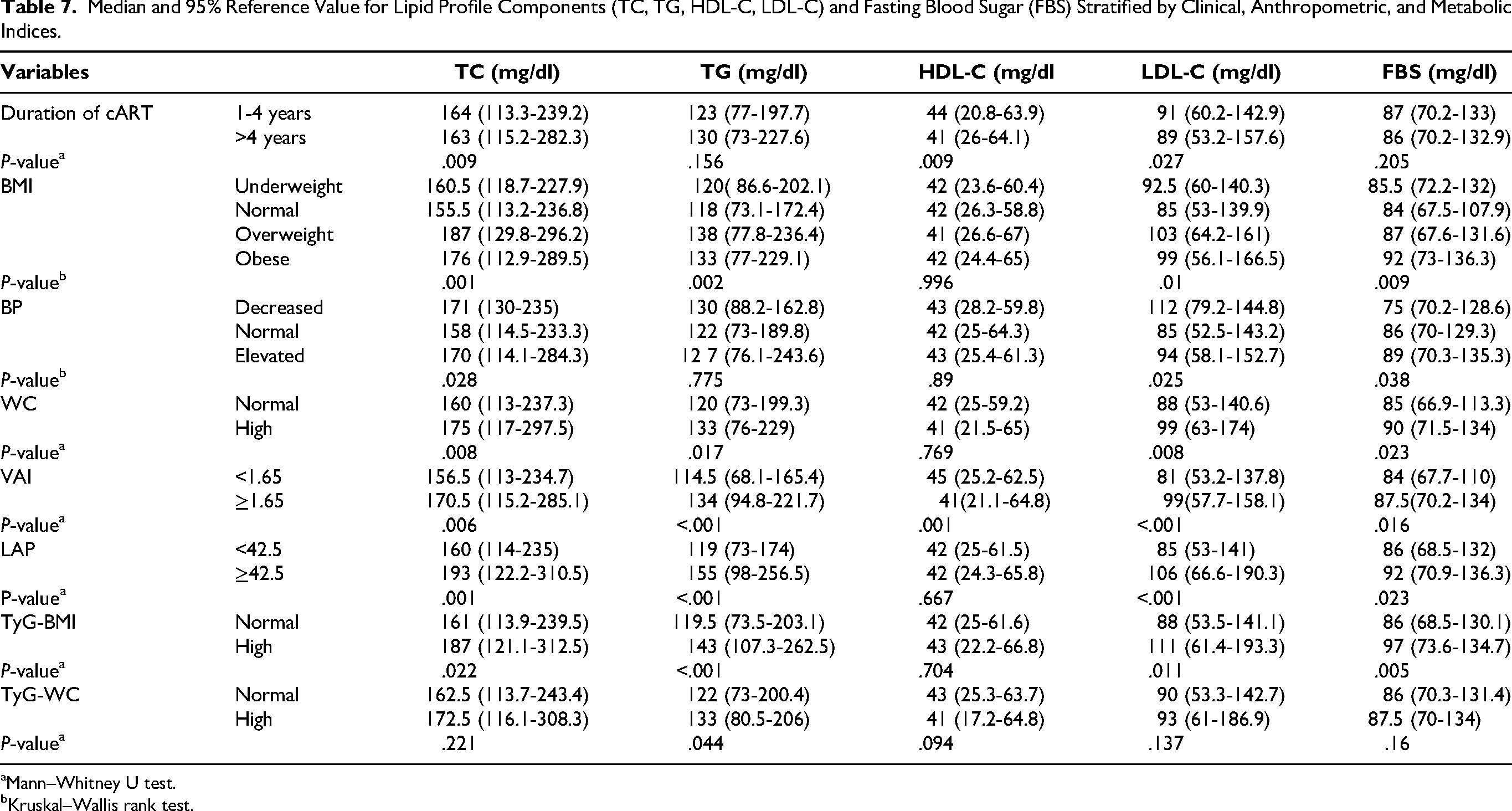
Mann–Whitney U test.
Kruskal–Wallis rank test.
Predictive Performance of Lipid-Related Indices for Dyslipidemia
Although textbook cutoffs for lipid-related indices are commonly used to flag metabolic risk, our results indicate that the optimal thresholds for this cART-treated population differ from conventional values. In this study, TyG-WC achieved the strongest diagnostic performance (AUC = 0.795) with an optimal cutoff of 434.1, higher than standard reference thresholds. TyG-BMI (cutoff 128.5) and LAP (cutoff 34.5) also showed strong predictive ability, while VAI required a slightly higher cutoff (1.91) than typically reported. These findings suggest that population-specific cutoffs may be necessary to accurately identify dyslipidemia in cART-treated individuals (Figure 1).
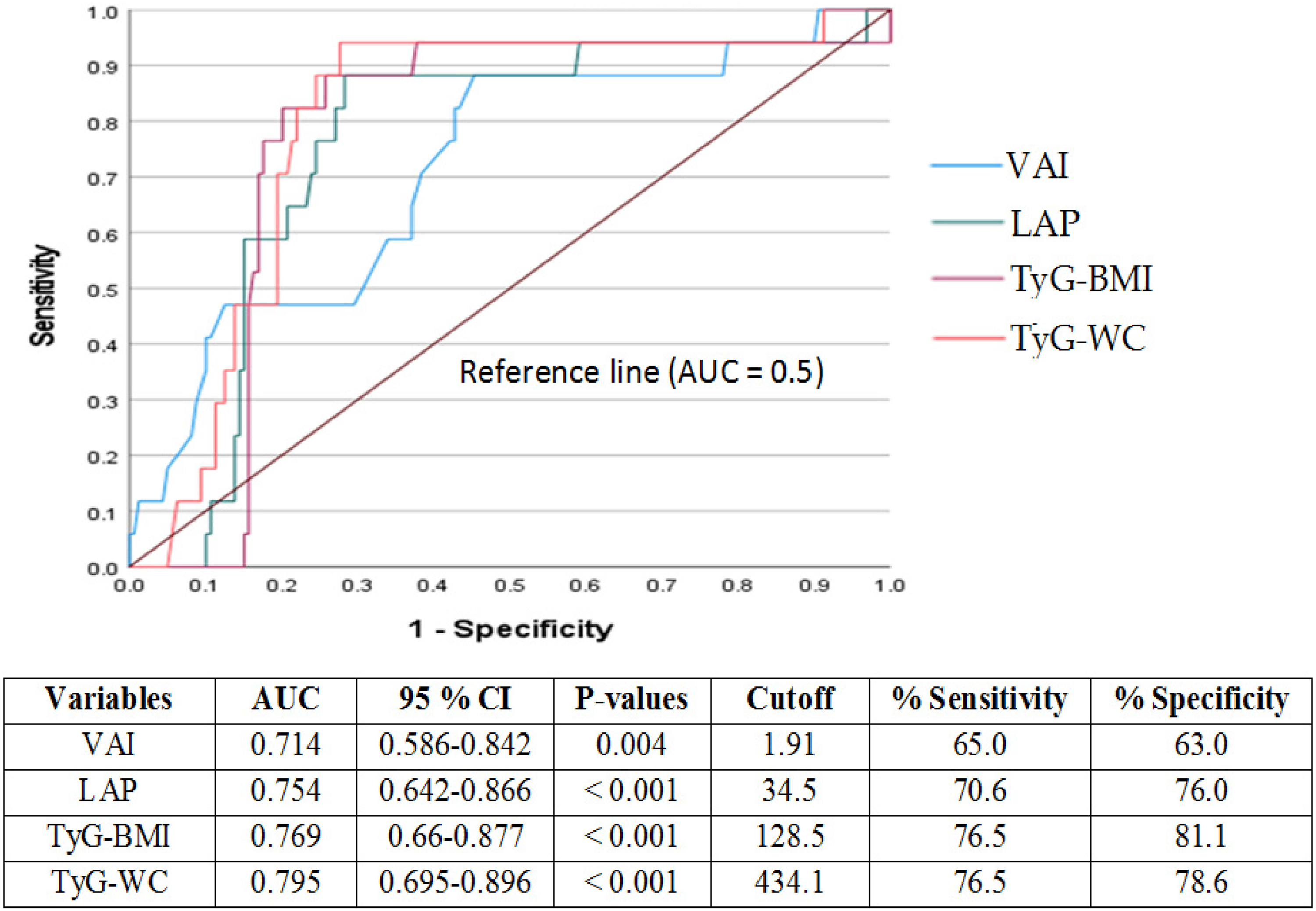
ROC-derived cutoffs for lipid indices (VAI, LAP, TyG-BMI, and TyG-WC).
Discussion
The overall prevalence of dyslipidemia in the current study was 54.5%. It was comparable with study conducted at Zewditu memorial hospital in Ethiopia 55.2% 28 in 2021, Mehal Meda north shoa in Ethiopia 59.9% 29 in 2018, in Addis Ababa at defence force hospital 63.6% 30 in 2014. But, some studies in Ethiopia has reported higher prevalence, in Addis Ababa at Armed force comprehensive specialized hospital 74.8% 31 in 2018, Debra Tabor hospital 73.7% 32 in 2020, the prevalence was even higher in neighboring countries like Uganda at Kampala hospital 81.5% 33 in 2012.
This discrepancy could result from variations in the components of cART, namely the different affinities of distinct PIs for human regulatory proteins. For example, some PIs, like lopinavir, exhibit molecular mimicry with proteins associated with the LDL receptor, which might hinder the clearance of TG. Furthermore, NNRTIs such as Efavirenz can promote hepatic lipogenesis, whereas ritonavir-boosted PIs may interfere with the proteasome-mediated breakdown of Apo lipoprotein B. These variances may also be caused by variations in study populations, treatment duration, study methodology, and baseline metabolic profiles.
Regarding the prevalence of DM in the current study was 9.7%, higher than a report in the an outskirts of Addis Ababa, Burayu health center (7.9%) in 2014, 4 northern part of the Ethiopia, Gondar university hospital 8% 7 in 2014. But other studies had reported even higher prevalence's; Southwest Ethiopia, Jimma public hospital 11.4% 25 in 2020. The report in neighboring African countries was much higher; Uganda at Kampala HIV clinic 16.3%. 33 This variation could be attributed to differences in the duration and type of HAART that block Glut 4 translocation, geographical settings which may lead to individual experience sedentary lifestyle and consumption of junk food, sample sizes differences, lifestyle such as regular drinking alcohol, smoking cigarettes, and others. According to our study, age (>40 years) was an independent risk factor for dyslipidemia among cART-treated HIV subjects (AOR, 3.4, P = .003). A similar result was reported from studies in the Malawi HIV clinic (AOR, 3.69, P <.001) 34 in 2014. Studies from Jimma public hospital, Mehal Meda, North Shewa, Ethiopia, suggested that long duration of cART is independently associated with the development of both dyslipidemia and DM.25,29 But, in our study, it was only associated with dyslipidemia (Table 6); there was a statistically significant difference of TC, HDL-C, LDL-C in reference to greater than 4 years on cART. Similarly, BMI was also statistically associated with lipid profile (Table 7). Similar results were reported; Uganda at Kampala Hospital (AOR, 1.4, P = .023), 33 Kenya (AOR, 1.9, P = .02), 35 in Ethiopia, Gondar University Hospital (AOR, 6.55, P = .001). 7
Another interesting habitual diet—spiced clarified milk butter (probably due to high livestock population, informal report)—in the local cART population was statistically associated with dyslipidemia. A similar report was from Uganda at Kalisizo Hospital in Kyotera district 36 in 2020, western Kenya at Kisumu Hospital 35 in 2018, but it was contradictory to a study from other areas.37,38 This may be caused by variations in the types of spices and their contents, such as garlic and ginger, which are rich in bioactive compounds with anti-inflammatory, antioxidant, lipid-lowering, and glucose-sensitizing qualities, as well as variations in ART types, such as PI directly linked to it. Family history of DM, frequent alcohol consumption (common in the area, personal objection) were risk factors of metabolic dysfunction, which was similarly reported in others.33,39,40 Overall, these findings underscore the importance of focused follow-up and counseling of this particular subpopulation.
Frequent monitoring using conventional biochemical tests might not be feasible in our study subjects, due to limited socioeconomic factors. Hence, we have evaluated inexpensive lipid indexes as a nearly too early detect with metabolic dysfunction, and thereby identify those at high risk for further in-depth biochemical tests. LAP, TyG-BMI, and TyG-WC had shown promising predictive power of dyslipidemia, which was similar to studies from the US and China.41–44 The ROC analysis compares the diagnostic performance of 4 variables (VAI, LAP, TyG-BMI, TyG-WC). TyG-WC and TyG-BMI showed the highest discriminatory ability with AUCs of 0.790 and 0.769, respectively, indicating good predictive performance. LAP had an AUC of 0.754, and VAI had the lowest AUC at 0.714. The optimal cutoffs provided balanced sensitivity and specificity, with TyG-WC achieving the highest specificity (84.0%) and TyG-BMI achieving the highest sensitivity (76.5%). All variables were statistically significant (P < .01). Although textbook cutoffs for lipid-related indices are commonly used to flag metabolic risk, our results indicate that the optimal thresholds for this cART-treated population differ from conventional values. In this study, TyG-WC achieved the strongest diagnostic performance (AUC = 0.795) with an optimal cutoff of 434.1, higher than standard reference thresholds. TyG-BMI (cutoff 128.5) and LAP (cutoff 34.5) also showed strong predictive ability, while VAI required a slightly higher cutoff (1.91) than typically reported.
Conclusion
In conclusion, our study demonstrates that dyslipidemia and undiagnosed diabetes are highly prevalent among cART-treated HIV patients in the study area. Beyond traditional risk factors, dietary patterns, including frequent consumption of high-fat, carbohydrate-restricted diets, like Nitter kibbeh, may modulate metabolic outcomes in this population, highlighting the need for further investigation. Simple, cost-effective lipid indices, particularly TyG-WC, showed robust predictive performance for early detection of insulin resistance and atherogenic dyslipidemia. These findings underscore the importance of establishing population-specific thresholds to accurately identify metabolic dysfunction in cART-treated individuals.
Limitation of the Study
We have not included ART naïve HIV positive subjects, small sample size, and the study design used was cross-sectional, which only identifies prevalence and associated factors. The sampling technique, purposive sampling, that we used couldn’t include all HIV patients.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261452325 - Supplemental material for Prevalence and Predictors of Dyslipidemia and Diabetes Mellitus Among cART-Treated HIV Patients in Western Ethiopia: A Cross-Sectional Study
Supplemental material, sj-docx-1-jia-10.1177_23259582261452325 for Prevalence and Predictors of Dyslipidemia and Diabetes Mellitus Among cART-Treated HIV Patients in Western Ethiopia: A Cross-Sectional Study by Nano Debele Gadisa, Mekdes Alem Baye, Halima Abdulkadir Hussein, Abebe Edao Nagesso, Mintewab Hussein, Afework Habtamu Aseme, Bezawit Fekadu, Demeke Jabesa Aga, Guta Tuna Edao, Gutama Diriba Tucho, Mikias Shitaw Tadese, Mitiku Deresa, Gobena Dedefo Dekebo, Mistire Wolde Gebre and Samuel Kinde Birru in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582261452325 - Supplemental material for Prevalence and Predictors of Dyslipidemia and Diabetes Mellitus Among cART-Treated HIV Patients in Western Ethiopia: A Cross-Sectional Study
Supplemental material, sj-docx-2-jia-10.1177_23259582261452325 for Prevalence and Predictors of Dyslipidemia and Diabetes Mellitus Among cART-Treated HIV Patients in Western Ethiopia: A Cross-Sectional Study by Nano Debele Gadisa, Mekdes Alem Baye, Halima Abdulkadir Hussein, Abebe Edao Nagesso, Mintewab Hussein, Afework Habtamu Aseme, Bezawit Fekadu, Demeke Jabesa Aga, Guta Tuna Edao, Gutama Diriba Tucho, Mikias Shitaw Tadese, Mitiku Deresa, Gobena Dedefo Dekebo, Mistire Wolde Gebre and Samuel Kinde Birru in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgment
We would like to thank the staff of NSH for their support during data collection. We want to extend our gratitude also to Nekemte public research and referral laboratory for materials, reagents, and expert support, and HIV patients for volunteering to participate in this study.
ORCID iDs
Author Contributions
Nano Debele Gadisa, Samuel Kinde Birru, and Mekdes Alem Baye conceived and designed the study. Nano Debele Gadisa, Samuel Kinde Birru, Mekdes Alem Baye, Demeke Jabesa Aga, Mitiku Derese, Gutama Diriba Tucho, Afework Habtamu Aseme, and Abebe Edao Nagesso collected and curated the data. Nano Debele Gadisa, Samuel Kinde Birru, Mistire Wolde Gebre, Gutama Diriba Tucho, Halima Abdulkadir Hussein, Mitiku Deresa, and Mikias Shitaw Tadese performed formal analysis. Nano Debele Gadisa, Samuel Kinde Birru, Guta Tuna Edao, Abebe Edao Nagesso, Halima Abdulkadir Hussein, Gobena Dedefo Dekebo, and Bezawit Fekadu developed the methodology. Nano Debele Gadisa managed the project and resources. Samuel Kinde Birru supervised the study. Nano Debele Gadisa, Samuel Kinde Birru, Mistire Wolde Gebre, Mintewab Hussein, and Abebe Edao Nagesso validated the results. Nano Debele Gadisa and Samuel Kinde Birru wrote the manuscript and performed review and editing.
Ethics Statement
The study protocol received ethical approval from the Departmental Research Ethics and Review Committee (DRERC) of the Department of Medical Laboratory Science, College of Health Sciences, Addis Ababa University (Ref. No. Mels/12/24, dated 27/12/24), and from the Medical Director of NSH. Written informed consent was obtained from all participants prior to enrollment. All study procedures, including sample collection, were conducted in accordance with the Declaration of Helsinki and relevant local guidelines for research involving human participants.
Consent Information
Prior to data collection, written informed consent was obtained from all study participants. Participants were fully informed about the study's objectives, procedures, potential risks and benefits, and their right to withdraw at any time without penalty. All personal identifiers were removed to ensure anonymity and confidentiality of the collected data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.