
Abstract
Background
Cervical cancer remains a major global health challenge, disproportionately affecting low- and middle-income countries. Women living with HIV are at increased risk due to weakened immunity. This study assessed cervical cancer screening utilization and associated factors among HIV-positive women attending antiretroviral therapy (ART) clinics in Gondar town, Northwest Ethiopia.
Methods
A multicenter institution-based cross-sectional study was conducted from November 1 to 30, 2025, using systematic random sampling. Data were collected through structured interviewer-administered questionnaires and analyzed using STATA 14. Bivariable and multivariable logistic regression analyses were performed, with P < .05 considered statistically significant.
Results
Screening utilization was 30.2%. Good knowledge (AOR = 3.44; 95% CI: 2.22-5.16), favorable attitude (AOR = 2.81; 95% CI: 2.28-6.61), and history of sexually transmitted infections (AOR = 2.22; 95% CI: 1.83-4.13) were significantly associated.
Conclusion
Screening utilization was low. Strengthening health education, improving ART counseling, and integrating screening into routine HIV care are recommended.
Plain Language Summary
Cervical cancer is one of the most common cancers affecting women worldwide. It is especially common in low- and middle-income countries. Women living with HIV have a higher risk of developing cervical cancer because their immune system is weakened. Regular cervical cancer screening can help detect early changes in the cervix and prevent the disease. However, many women living with HIV do not use these screening services. This study examined how many women living with HIV use cervical cancer screening services and what factors influence their use of screening. The study was conducted among women attending antiretroviral therapy (ART) clinics in public health facilities in Gondar town, Northwest Ethiopia. Data were collected using interviews with structured questionnaires. The results showed that only 30.2% of women living with HIV had been screened for cervical cancer. The study found that women who had good knowledge about cervical cancer, those who had a positive attitude toward screening, and those who had a history of sexually transmitted infections were more likely to use cervical cancer screening services. The findings indicate that cervical cancer screening among women living with HIV is still low. Improving awareness and knowledge about cervical cancer, providing better counseling services in ART clinics, and integrating cervical cancer screening into routine HIV care may help increase screening use. Strengthening these efforts could help detect cervical cancer earlier and reduce illness and death among women living with HIV.
Introduction
Cervical cancer (CC) continues to pose a substantial global public health challenge and ranks as the fourth most frequently diagnosed cancer among women worldwide. In 2020, approximately 604,000 new cases and 342,000 deaths were recorded globally. 1 Notably, more than 90% of these cases and deaths occurred in low- and middle-income countries, highlighting significant inequities in access to preventive, diagnostic, and treatment services. 1 Without intensified intervention strategies, the global burden is projected to increase further, with new cases expected to rise from 570,000 in 2018 to nearly 700,000 by 2030, and annual deaths increasing from 311,000 to about 400,000. 2 The disease disproportionately affects women who are socioeconomically disadvantaged, less educated, and residing in resource-limited settings. 2
Sub-Saharan Africa carries a particularly high burden of CC, with reported incidence, mortality, and prevalence rates of 25.2%, 23.2%, and 27.6%, respectively. 3 In Ethiopia, CC remains a major public health concern, with incidence and mortality rates of 17.3% and 16.5%, respectively, and an overall prevalence of 18.2%. 4 It ranks as the second leading cause of cancer-related death among women of reproductive age, after breast cancer. 4 Approximately 23 per 100,000 Ethiopian women are diagnosed with CC annually, emphasizing the urgent need to strengthen prevention and screening programs. 5
Women living with HIV (WLHIV) are at significantly higher risk of developing CC compared to HIV-negative women. Persistent infection with high-risk human papillomavirus (HPV), the principal cause of CC, is more common among immunocompromised individuals. The WLHIV are estimated to be about 6 times more likely to develop CC and often experience earlier disease onset.6-8 Moreover, immunosuppression accelerates the progression from precancerous lesions to invasive cancer, shortening the time to disease development. 1 Consequently, CC represents the most common malignancy among WLHIV.
Despite strong global advocacy for prevention, CC screening coverage remains insufficient in many low-income countries. The World Health Organization recommends routine screening and timely management of precancerous lesions. 9 Similarly, the United Nations promotes the integration of CC screening into HIV care services to improve the management of comorbid conditions. 10 However, only about 30% of low-income countries have established organized public-sector screening programs, compared with over 90% of high-income countries. 1 Similarly, HPV vaccination coverage remains limited, with only a quarter of low-income countries incorporating it into national immunization programs. 1
In Ethiopia, CC screening uptake among WLHIV remains consistently low. Studies conducted in Tigray, Gondar, Addis Ababa, and Adama have reported screening rates ranging from 8% to 26.9%.11-14 These figures are substantially below national and global targets, indicating persistent service delivery gaps.
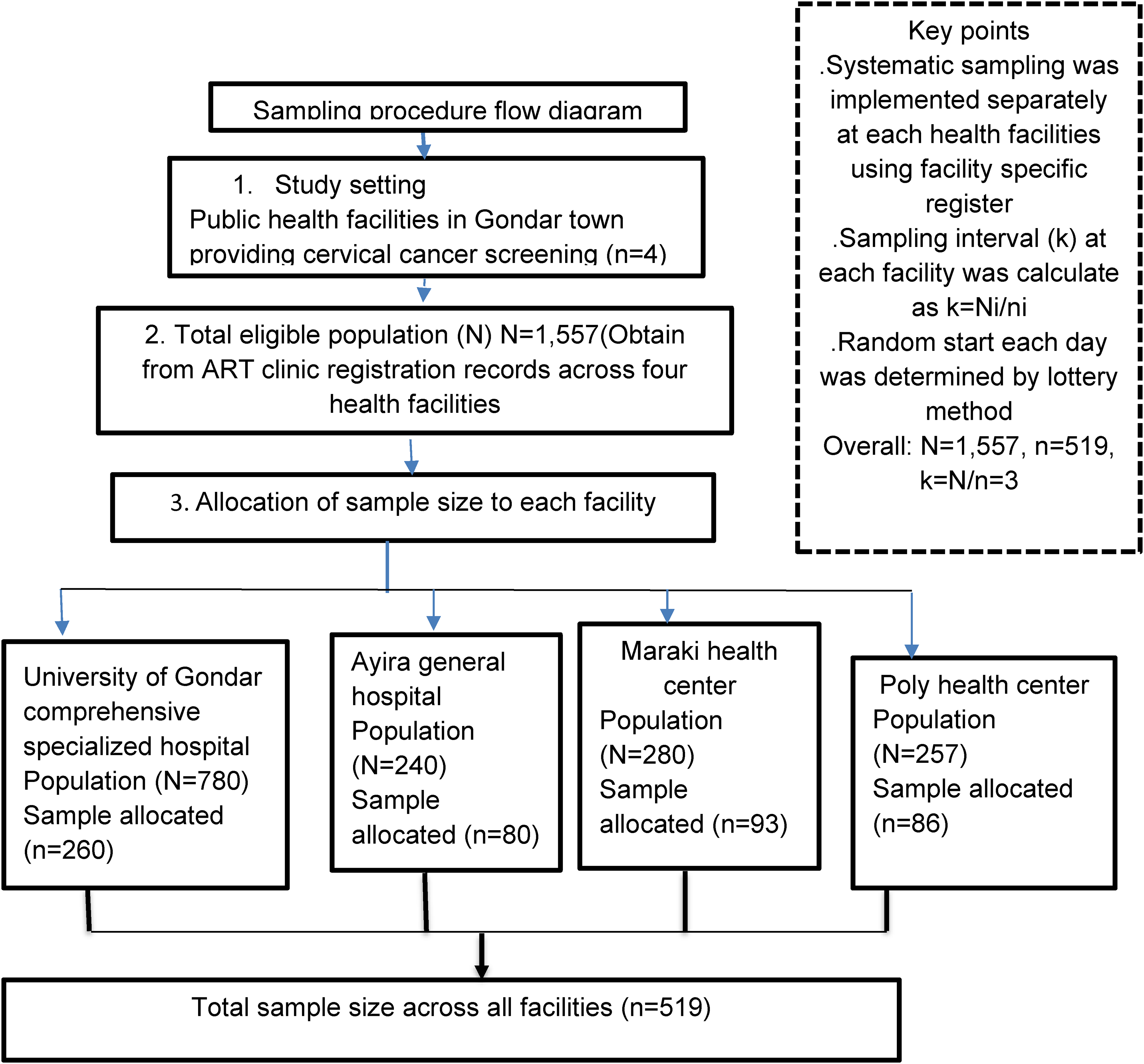
Sampling procedure flow diagram.
Several factors influence CC screening utilization. Sociodemographic characteristics such as age, education, and occupation affect health-seeking behavior. In addition, HIV-related and reproductive characteristics, including a history of sexually transmitted infections (STIs), having multiple sexual partners, early initiation of sexual activity, time since HIV diagnosis, and viral load status, have been linked to variations in screening utilization.5,14-16 In addition, limited knowledge, unfavorable attitudes, health system barriers, inadequate provider training, financial constraints, and restricted availability of screening facilities further reduce service utilization.5,14-16
To accelerate the elimination of CC as a public health concern, the World Health Organization introduced the global 90-70-90 strategy, which sets targets for 2030: vaccinating 90% of girls against HPV by age 15, screening 70% of women with a high-performance test, and ensuring that 90% of those diagnosed with cervical disease receive appropriate treatment. 1 In alignment with this global framework, Ethiopia has adopted context-appropriate and cost-effective screening approaches, such as Visual Inspection with Acetic Acid, to improve access in resource-limited settings. 17 The Ethiopian Ministry of Health has also set a national target to screen at least 80% of eligible women. 17 The Ethiopian Ministry of Health has also set a national target to screen at least 80% of eligible women. 18
Despite these initiatives, screening coverage among WLHIV remains suboptimal. Therefore, assessing the level of CC screening utilization and identifying associated factors among women receiving antiretroviral therapy (ART) is crucial to inform targeted interventions and strengthen integrated HIV and CC services.
Methods
Study Area and Period
The study was carried out in public health facilities in Gondar town, which is situated about 727 km northwest of Addis Ababa, the capital of Ethiopia. Based on information from the Gondar Town Health Office, the town has 1 comprehensive specialized hospital, 1 general hospital, 8 health centers, and 61 private health facilities.
Among the public health facilities, CC screening services are provided at the University of Gondar Comprehensive Specialized Hospital, Ayira General Hospital, Maraki Health Center, and Poly Health Center. These facilities were purposefully selected because they were the only public health facilities in Gondar town providing CC screening services during the study period. Accordingly, all 4 public health facilities providing CC screening in Gondar town were included in the study. Data collection for this study was conducted from November 1 to 30, 2025.
Study Design and Population
A multicenter, institution-based cross-sectional study was conducted among adult women aged 18 years and above living with HIV who were on ART in public health facilities of Gondar town. The source population included all HIV-positive women attending ART clinics during the study period.
Inclusion and Exclusion Criteria
All HIV-positive women aged 18 years and older who were on ART during the study period were eligible to participate. Exclusion criteria included women who were critically ill or unconscious at the time of data collection, those who had previously undergone total hysterectomy, and those with a prior diagnosis of CC.
Sample Size Determination and Sampling Procedure
The sample size was calculated using a single population proportion formula, assuming a 95% confidence level, a 4% margin of error, and a CC screening utilization rate of 26.9%, as reported by Adama Hospital Medical College (14). After accounting for a 10% nonresponse rate, the final sample size was determined to be 519 participants.
The average monthly attendance of women at ART clinics was estimated based on records from the previous 6 months. The sampling frame consisted of the daily ART clinic attendance register (appointment/visit logbook) of eligible women, which was used to identify and list participants attending follow-up visits during the data collection period. The total number of eligible women (N) in the sampling frame during the study period was obtained from ART clinic registration records.
A systematic random sampling method was used to select study participants. Eligible women attending follow-up visits were numbered sequentially according to their arrival. Every third woman (K = 3) was selected, starting from a randomly chosen first participant each day. This process was repeated daily until the target sample size was reached. To avoid including the same participant more than once, a marker was placed on the medical records of women who had already been enrolled in the study. To minimize the risk of periodicity or hidden patterns in the ordered list, the first participant each day was selected using a lottery method, and participant selection followed the natural sequence of clinic arrivals without any prior ordering or grouping based on clinical or demographic characteristics. A flow diagram illustrating the sampling procedure is shown in Figure 1.
Operational Definitions
Uptake of CC screening: HIV-positive women who had undergone screening at least once within the past 5 years. 15
Awareness of CC and screening: Participants who had ever heard about CC and its screening services. 12
Knowledge: Knowledge was assessed using 10 yes/no questions. Each correct response was scored as one point, and incorrect responses were scored zero. Participants scoring at or above the mean value were categorized as having good knowledge; those scoring below the mean were classified as having poor knowledge. 19
Attitude toward CC screening: Attitude was measured using 8 Likert-scale questions (1 = strongly disagree to 5 = strongly agree). Participants scoring at or above the mean were considered to have a positive attitude, while those scoring below the mean were categorized as having a negative attitude. 19 The internal consistency of the attitude scale was assessed using Cronbach α, and the scale demonstrated acceptable reliability (Cronbach α = 0.82).
Data Collection Procedures
Data were gathered using a structured interviewer-administered questionnaire, which was adapted from previously published studies.11,12,14,20-22 The questionnaire was initially developed in English, translated into Amharic, and then back-translated into English to ensure accuracy and consistency. It covered sections on sociodemographic characteristics, knowledge and attitudes toward CC screening, and reproductive health–related factors.
Six BSc midwives were recruited as data collectors, while 2 BSc midwives supervised the process. Three-day training was provided on sampling methods, interviewing techniques, and overall data collection procedures. Before the main study, a pretest was conducted on 5% of the sample at Bahir Dar Tibebe Gion Specialized Hospital, and adjustments were made based on the pretest results. During data collection, supervisors checked the questionnaires daily to ensure completeness and consistency. The principal investigator managed data coding, entry, and cleaning.
Statistical Analysis
Data were entered into EpiData version 3.1 and analyzed using Stata version 14. Descriptive statistics were used to summarize the data in the form of frequencies, percentages, means, and standard deviations.
Binary logistic regression analysis was performed to identify factors associated with CC screening utilization. Variables with a P-value <.2 in the Bivariable analysis were included in the multivariable logistic regression model to control for potential confounders. The goodness of fit of the final model was assessed using the Hosmer-Lemeshow test, with a P-value ≥.05 indicating an acceptable model fit. Multicollinearity was checked using the variance inflation factor (VIF); values greater than 10 were considered indicative of Multicollinearity. The mean VIF was 3.6, indicating no significant multicollinearity.
Result
Sociodemographic Characteristics of the Study Participants
A total of 504 HIV-positive women were included in the study, yielding a response rate of 97.1%. The mean age of the participants was 43.6 years (SD ± 4.8). Among them, 255 (50.6%) had completed primary education. Regarding marital status, the majority, 342 (67.9%), were married. Most participants, 376 (74.6%), were engaged in private employment. Finally, 316 (62.7%) of the respondents identified as followers of the Orthodox Christian faith (Table 1).
Sociodemographic Characteristics of HIV-Positive Women Attending Adult ART Clinics at Public Health Facilities in Gondar Town, Ethiopia, 2026 (n = 504).
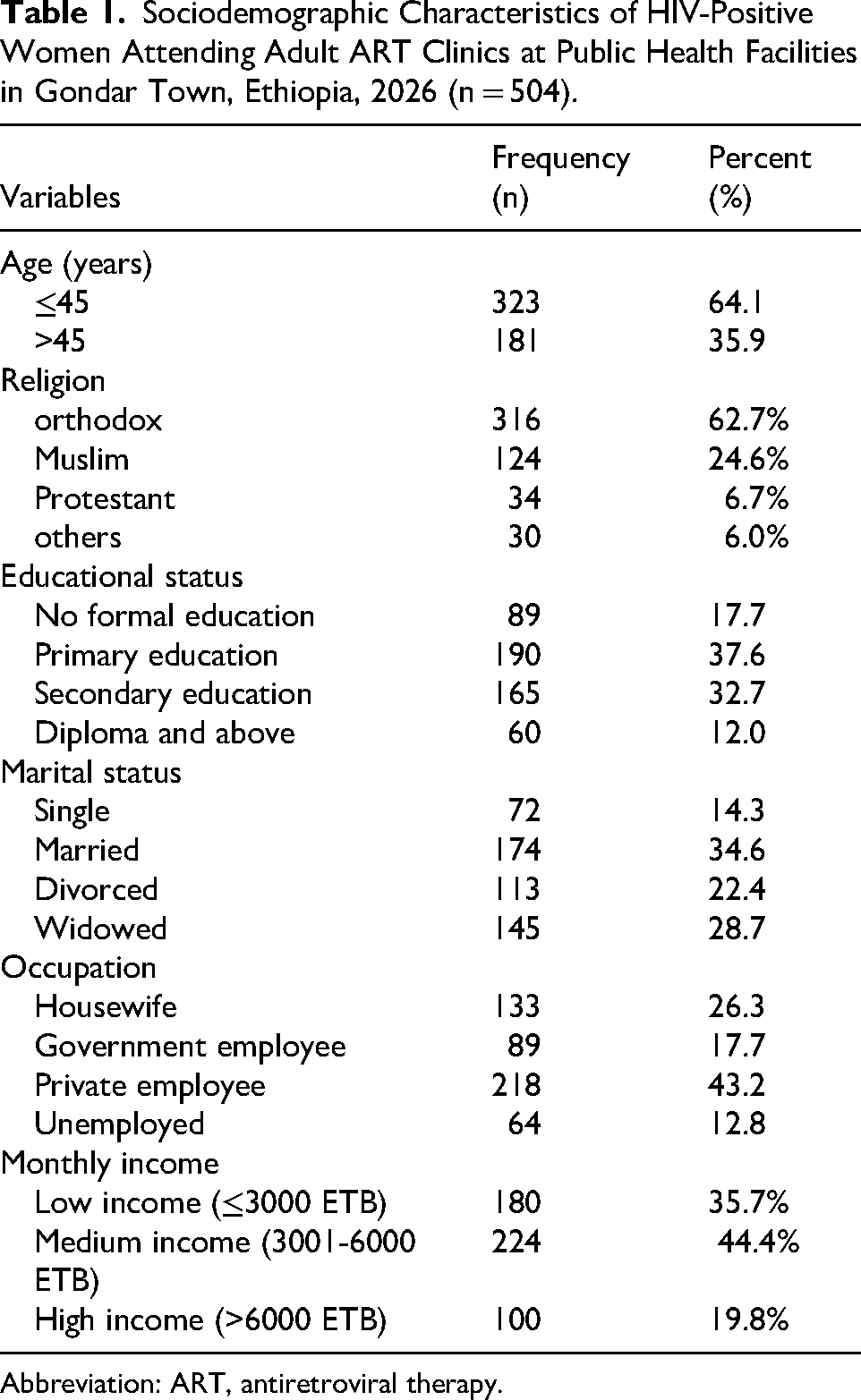
Abbreviation: ART, antiretroviral therapy.
Reproductive Health Characteristics
Regarding reproductive health characteristics, 84 women (16.6%) reported initiating sexual activity before the age of 18 years. A majority of participants, 446 (88.5%), had experienced at least one childbirth. Furthermore, 432 women (85.7%) reported current or past use of oral contraceptive pills, while 59 participants (11.7%) indicated having had multiple sexual partners in the past 3 years (Table 2).
Reproductive Health-Related Characteristics of HIV-Positive Women Attending Adult ART Clinics at Public Health Facilities in Gondar Town, Ethiopia, 2026 (n = 504).
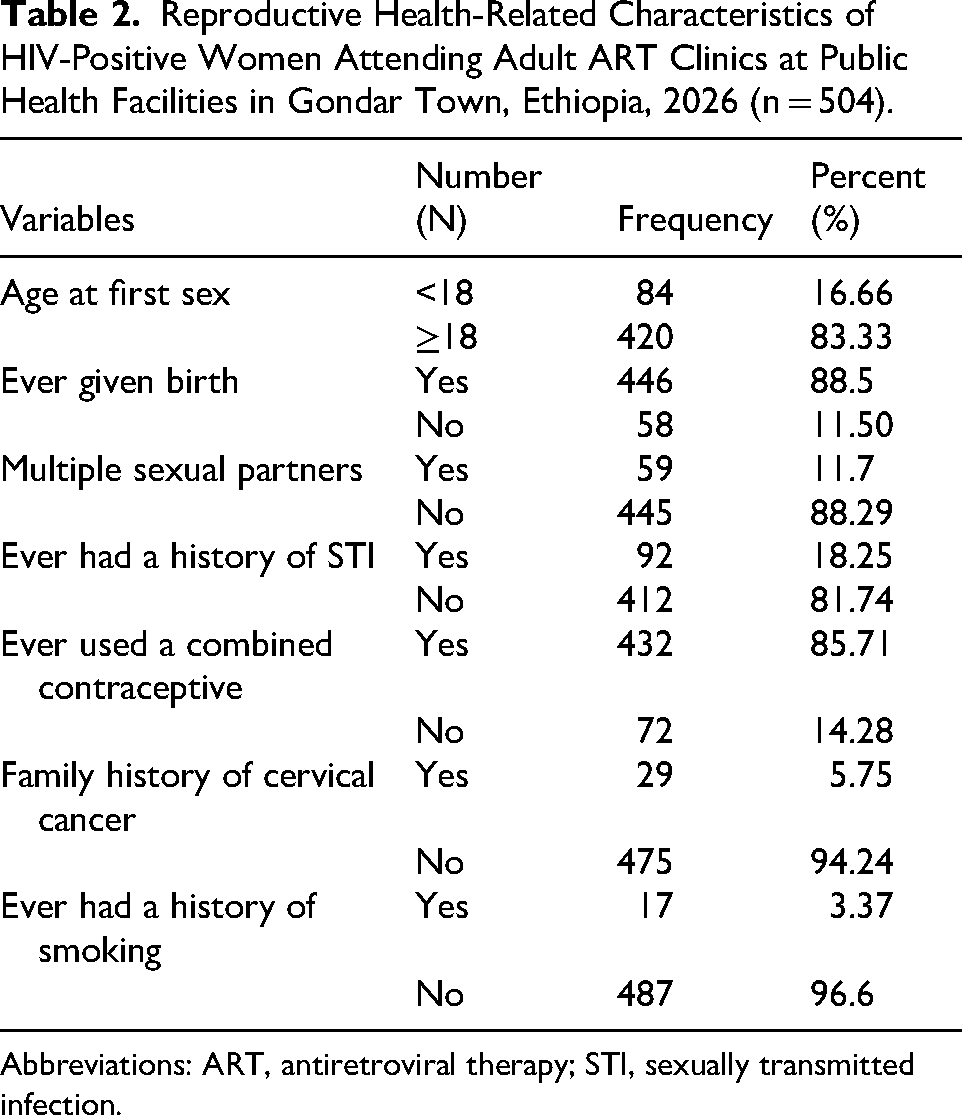
Abbreviations: ART, antiretroviral therapy; STI, sexually transmitted infection.
Knowledge About CC Screening
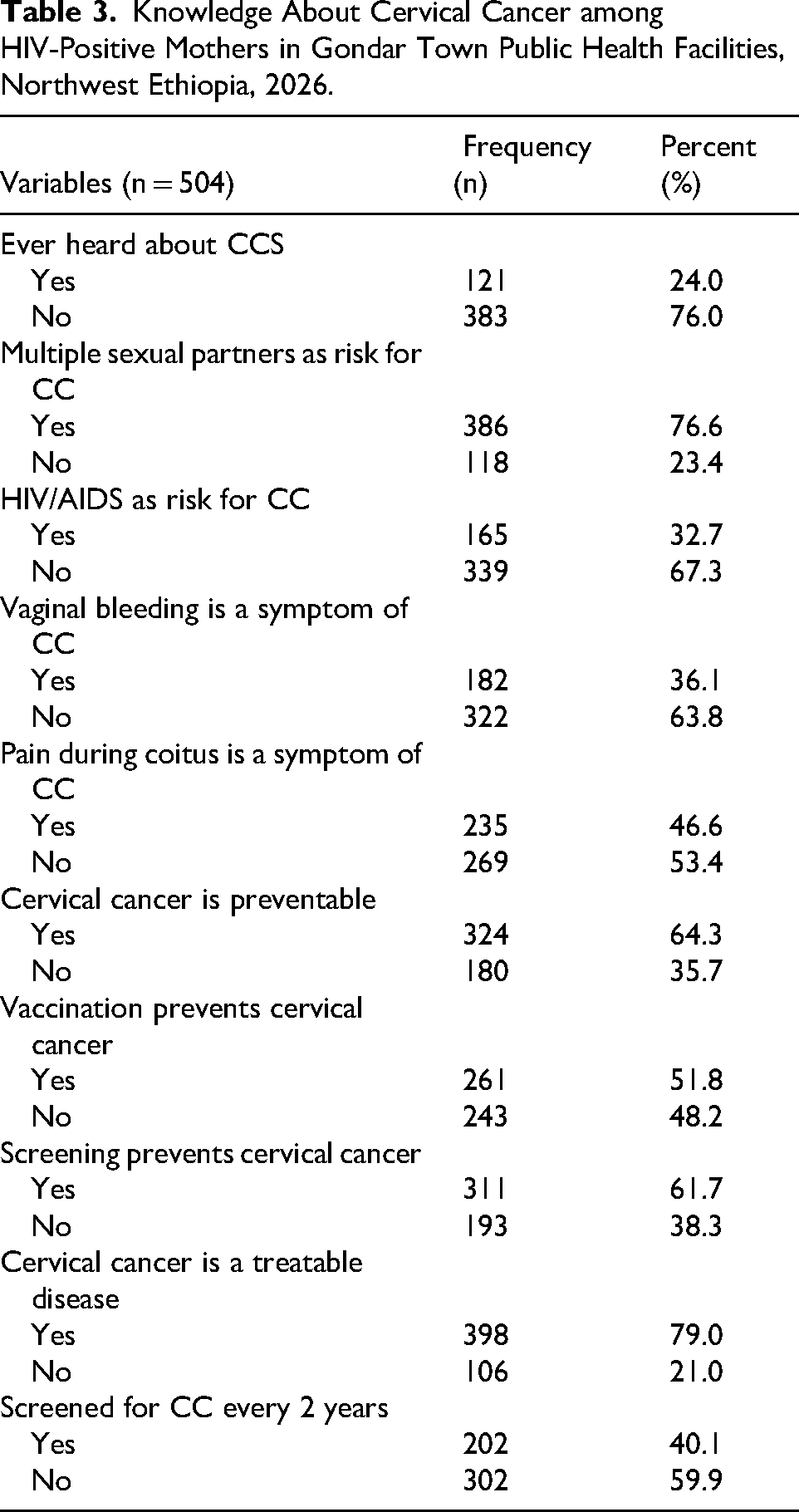
Among the study participants, 383 (76%) reported that they had never heard of CC, while 165 (32.7%) recognized HIV/AIDS as a risk factor for CC. In addition, 386 participants (76.6%) were aware that having multiple sexual partners increases the risk of CC. Regarding prevention, 261 women (51.8%) knew that vaccination can help prevent CC, and 324 participants (64.3%) understood that CC is a preventable disease.
Overall, 258 respondents (51.2%) demonstrated good knowledge about CC, whereas 246 (48.8%) had poor knowledge (Table 3).
Knowledge About Cervical Cancer among HIV-Positive Mothers in Gondar Town Public Health Facilities, Northwest Ethiopia, 2026.
Attitudes Toward CC Screening
Regarding attitudes, most participants recognized the importance of CC as a public health concern in Ethiopia, with 454 women (90.1%) acknowledging its significance. Additionally, 406 participants (80.6%) believed that early detection of CC allows for effective treatment.
Overall, 388 women (77.1%) exhibited a positive attitude toward CC screening, while 116 participants (23.0%) demonstrated an unfavorable attitude.
Magnitude of CC Screening Utilization
The overall prevalence of CC screening utilization among WLHIV receiving ART in Gondar Town was 182 (30.2%), with a 95% confidence interval of 26.2% to 34.2%.
Factors Associated with CC Screening Utilization
In the Bivariable logistic regression analysis, variables such as age, occupation, educational status, history of STIs, parity, knowledge, and attitude were found to have a P-value <.2 and were subsequently included in the multivariable logistic regression model.
In the multivariable analysis, 3 variables were significantly associated with CC screening utilization (P < .05): knowledge, attitude, and history of STIs. Women with a favorable attitude toward CC screening were nearly 3 times more likely to be screened compared to those with an unfavorable attitude (AOR = 2.81; 95% CI: 2.28-6.61). Similarly, participants with good knowledge about CC were more than 3 times more likely to utilize screening than those with poor knowledge (AOR = 3.44; 95% CI: 2.22-5.16). In addition, women with a history of STIs had higher odds of undergoing screening compared to those without such history (AOR = 2.22; 95% CI: 1.83-4.13) (Table 4).
Factors Associated with Cervical Cancer Screening Utilization among HIV-Positive Mothers in Gondar Town Public Health Facilities, Northwest Ethiopia, 2026.
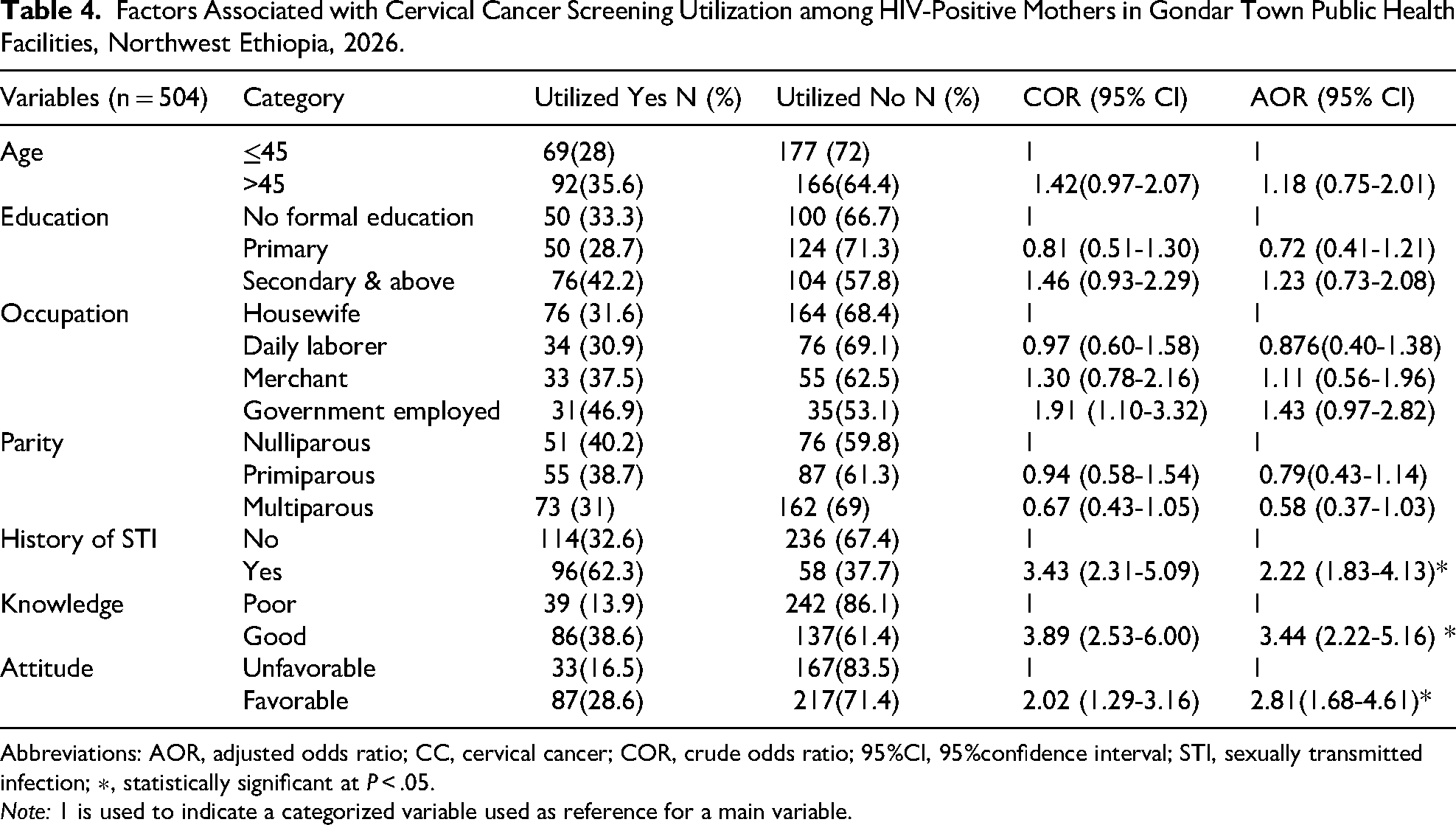
Abbreviations: AOR, adjusted odds ratio; CC, cervical cancer; COR, crude odds ratio; 95%CI, 95%confidence interval; STI, sexually transmitted infection; ∗, statistically significant at P < .05.
Note: 1 is used to indicate a categorized variable used as reference for a main variable.
Discussion
This study examined CC screening utilization and its associated factors among WLHIV who were receiving ART in public health facilities in Gondar town, Northwest Ethiopia. The overall CC screening utilization among participants was 30.2% (95% CI: 26.2-34.2). This finding is similar to studies conducted in Kenya (27.5%) 14 and Mekele, Ethiopia (29.8%), 23 but higher than reports from Morocco (9%), 24 Tanzania (22.6%), 25 Southern Tigray (8%), 11 Addis Ababa (11.5%), 26 and Hadiya zone, Hosanna (24.2%). 27
Conversely, the utilization rate in this study was lower than that reported in England (85.7%), 28 Catalonia (50.6%), 29 and Uganda (44%). 30 The observed low screening coverage remains below the World Health Organization's 2030 target of screening 70% of eligible women and Ethiopia's national goal of 80% coverage. 31 Differences in screening uptake may be explained by variations in participants’ sociodemographic and socioeconomic status, national income levels, limited awareness, cultural beliefs, fear of diagnosis, absence of routine screening reminders, and the availability and quality of screening services within healthcare facilities.32-34
Women who had good knowledge about CC were significantly more likely to utilize screening services. Specifically, they were 3.44 times more likely to undergo CC screening compared to women with poor knowledge. Similar associations have been reported in Tanzania, 35 Tigray, 11 and Hawassa. 15 This relationship is likely because women who are well-informed about CC, its risk factors, and the benefits of early detection are more inclined to adopt preventive health behaviors, including screening.
A history of STIs was also significantly associated with CC screening. Women reporting prior STIs were 2.22 times more likely to be screened than those without such a history, a finding comparable to results from Adama Hospital Medical College. 14 This may be explained by the increased interaction with healthcare providers among women experiencing STI-related symptoms, which often includes gynecological examination and counseling on CC and its prevention, thereby promoting screening uptake.
Furthermore, a favorable attitude toward CC screening was positively associated with utilization; women with a positive attitude were 2.81 times more likely to undergo screening than those with an unfavorable attitude. This result is consistent with findings from studies conducted in Malawi, 26 Hawassa, 36 and Finote Selam. 37 A positive attitude may increase willingness to participate in screening programs, as women perceive these services as important for early detection and prevention of CC.
Although factors such as age, educational status, occupation, and parity were associated with CC screening utilization in the Bivariable analysis, they did not remain statistically significant in the multivariable regression model. This suggests that behavioral and awareness-related factors may play a more important role than sociodemographic characteristics in influencing screening uptake among WLHIV in this setting.
Overall, the findings of this study underscore the need to enhance knowledge and attitudes toward CC screening in order to improve service utilization among WLHIV. Strengthening health education programs, integrating CC screening into routine ART services, and improving counseling by healthcare providers may help increase screening coverage.
Strengths and Limitations of the Study
This study has several notable strengths. It utilized a multicenter, institution-based design and included a relatively large sample with a high response rate, which enhances the reliability and generalizability of the findings for WLHIV attending ART clinics in Gondar town. The use of systematic random sampling helped reduce selection bias, while standardized data collection procedures conducted by trained data collectors ensured high data quality. Moreover, the study examined both behavioral factors (knowledge and attitude) and clinical characteristics, offering a comprehensive understanding of the determinants of CC screening utilization.
However, the study has some limitations that should be considered. The cross-sectional nature of the design limits the ability to establish causal relationships between the identified factors and CC screening utilization. In addition, the use of self-reported information may introduce recall bias or social desirability bias, particularly for reproductive history and screening practices. Furthermore, since the study was conducted only among women attending ART clinics in public health facilities, the findings may not be generalizable to women receiving care in private facilities or those not engaged in HIV services. Furthermore, the inclusion of only facilities providing CC screening services may limit the generalizability of the findings to other health facilities that do not offer such services.
Another potential limitation is the analytical approach. Although the study involved multiple health facilities, multilevel logistic regression was not performed due to the limited number of clusters (4 facilities), which may affect the ability to fully account for potential clustering effects at the facility level.
Conclusion
The findings of this study indicate that CC screening utilization among WLHIV remains low and is far below both national and global targets for CC prevention. Good knowledge about CC, a positive attitude toward screening, and a history of STIs were identified as significant factors associated with screening uptake. These results highlight the importance of enhancing health education and counseling services within ART clinics and strengthening the integration of CC screening into routine HIV care. Targeted interventions that improve awareness and encourage favorable attitudes among WLHIV may enhance screening coverage and help reduce the overall burden of CC.
Supplemental Material
sj-docx-1-jia-10.1177_23259582261460521 - Supplemental material for Cervical Cancer Screening Utilization and Its Associated Factors Among Women Living With HIV in Public Health Facilities of Gondar Town, Northwest Ethiopia
Supplemental material, sj-docx-1-jia-10.1177_23259582261460521 for Cervical Cancer Screening Utilization and Its Associated Factors Among Women Living With HIV in Public Health Facilities of Gondar Town, Northwest Ethiopia by Yeshiwas Ayale Ferede, Agerie Mengistie Zeleke, Worku Chekole Tassew, Ayanaw Dinku Abebe and Jember Ayelgne Beyene in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582261460521 - Supplemental material for Cervical Cancer Screening Utilization and Its Associated Factors Among Women Living With HIV in Public Health Facilities of Gondar Town, Northwest Ethiopia
Supplemental material, sj-docx-2-jia-10.1177_23259582261460521 for Cervical Cancer Screening Utilization and Its Associated Factors Among Women Living With HIV in Public Health Facilities of Gondar Town, Northwest Ethiopia by Yeshiwas Ayale Ferede, Agerie Mengistie Zeleke, Worku Chekole Tassew, Ayanaw Dinku Abebe and Jember Ayelgne Beyene in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The author would like to sincerely thank the College of Health Sciences for their continuous support throughout the development of this thesis. The author is also grateful to all study participants for their willingness to provide valuable information, as well as to the data collectors and supervisors for their dedicated efforts during the data collection process.
Ethics Approval,Confidentiality,and Informed Consent
Ethical approval for the study was granted by the Institutional Review Board of Debark University, College of Health Sciences (Reference No. DUHS/25074/2025). Due to the sensitive and potentially stigmatizing nature of HIV-related information, strict precautions were taken to maintain confidentiality and safeguard participants’ personal and health data. No personal identifiers were included in the data collection instruments, and only the principal investigator and supervisors had access to the study records. All documents were securely kept in a locked cabinet to prevent unauthorized access. Both written and verbal informed consent were obtained from each participant after clearly explaining the purpose of the study, the procedures involved, and the possible risks and benefits. Participants were also informed that their participation was voluntary and that they had the right to refuse or withdraw from the study at any time without facing any negative consequences. These ethical procedures were followed to protect participants’ privacy, promote trust, and ensure adherence to national and international ethical standards.
Author Contributions
Yeshiwas Ayale Ferede contributed to the conceptualization of the study, study design and methodology, data collection, formal data analysis, and data visualization. Agerie Mengistie Zeleke contributed to supervision, drafting the manuscript, and reviewing and editing the text. Worku Chekole Tassew contributed to methodology support, supervision, drafting the manuscript, and reviewing and editing. Ayanaw Dinku Abebe contributed to formal analysis, supervision, manuscript drafting, and review and editing. Jember Ayelgne Beyene contributed to supervision, drafting the manuscript, and reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All the materials used in this study will be made available by the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.