
Abstract
Background
Despite global advances in HIV care, pediatric populations in Africa continue to experience suboptimal treatment outcomes. Dolutegravir (DTG)-based antiretroviral therapy (ART) offers improved efficacy and tolerability, however, its real-world impact on viral load suppression (VLS) and the uptake of DTG-based regimens from older ART to newly recommended DTG-based ART among children and adolescents in Africa has not been systematically quantified.
Objective
This systematic review and meta-analysis aimed to estimate the pooled viral load suppression after initiation of dolutegravir-based ART and the uptake of DTG-based regimens from older regimens to dolutegravir-based ART among children and adolescents living with HIV in Africa.
Methods
A systematic review and meta-analysis conducted in accordance with PRISMA 2020 guidelines. Comprehensive searches of PubMed, Google Scholar, ScienceDirect, Hinari, CORE, and DOAJ were performed from January 01-10, 2026. Studies reporting VLS after initiation of DTG-based ART and the uptake of DTG-based regimens among pediatric patients with HIV in Africa were included. Pooled estimates were computed using random-effect models. Heterogeneity was assessed using I2 statistics, and subgroup, sensitivity, and publication bias analyses were performed.
Results
out of 7,789 records screened, twenty-four studies comprising 119,292 participants were included. The overall pooled viral load suppression at six months after initiation of DTG-based ART was 82% (95% CI: 79-85%) and 70 (95% CI: 62-77%) among participants who were unsuppressed at baseline. The pooled uptake of DTG-based regimens was 77% (95% CI: 68-86%) based on 23 studies. Substantial heterogeneity was observed across outcomes (I2≥98%). Subgroup analysis indicated regional and study-design variation in the uptake of DTG-based regimens but not in viral suppression. No substantial publication bias was detected among the included studies.
Conclusion
DTG-based ART effectively suppressed viral load among pediatric patients in Africa, though adoption remains incomplete and below UNAIDS 95-95-95 targets. Significant heterogeneity highlights the influence of contextual and health system factors. Accelerated rollout, strengthened adherence support, and harmonized monitoring are needed to optimize pediatric HIV outcomes.
Plain Language Summary
Many children and adolescents living with HIV in Africa do not achieve optimal treatment outcomes. Dolutegravir (DTG) is a newer HIV medicine that is more effective and better tolerated than older treatment options. This study reviewed research from across Africa to assess the effectiveness of DTG in young people and to determine how many children are receiving DTG-based therapy after older regimens. We analyzed 24 studies including over 119,000 children and adolescents. Six months after starting DTG, 82% had viral suppression, and 70% of those who were previously unsuppressed achieved viral control. Approximately 77% of children received DTG-based therapy after older treatments. Results varied across regions and study designs, but overall, DTG was effective in achieving viral suppression in most children. Although DTG is effective, not all children are currently receiving it. Expanding access, strengthening adherence support, and improving routine monitoring could help more children achieve better health outcomes.
Introduction
Human immunodeficiency virus (HIV) remains a major global health challenge, with new infections continuing to occur despite substantial advances in prevention, diagnosis, and treatment1,2
In 2020, approximately 3.4 million children and adolescents aged 0-19 years were living with HIV worldwide, the majority of whom resided in the African region.5,6 Despite sustained global initiatives to expand access to antiretroviral therapy(ART), children and adolescents living with HIV(CALHIV) continue to face significant treatment gaps, 7 persistent structural disadvantages, 8 and pronounced regional inequalities. 9 By 2024, only 55-57% of children aged 0-14 years had access to life-saving ART, while treatment coverage among adolescents aged 10-19 years reached approximately 64%. Nevertheless, both figures remain substantially lower than the 77-78% ART coverage achieved among adults living with HIV. 10 Similarly, viral load suppression(VLS)among children and adolescents ranged from 46-64%, compared with 65-79% among adults, reflecting ongoing disparities in treatment effectiveness and outcomes.11,12 Collectively, these disparities highlight persistent inequality in HIV care and the need for targeted interventions to improve pediatric outcomes.8-11
Despite notable advances in pediatric HIV care, including rapid diagnosis, simplified ART regimens, and long-acting preventive therapies, HIV related mortality among children remains high, and durable viral suppression continues to be difficult to achieve. 13
Viral load suppression is defined as achieving and sustaining a viral load below 1,000 copies/mL of blood, which is essential for improving immune functions, reducing morbidity and mortality, and minimizing the risk of onward transmission
14
In response to the united nations member stats as part of the global effort to end AIDS, the joint united nations programs on HIV/AIDS (UNAIDS) 95-95-95 targets and the recognized limitations of older pediatric antiretroviral regimens including suboptimal efficacy, treatment related toxicity, and complex dosing, the World Health Organization (WHO) endorse dolutegravir-based (DTG) regimens as the preferred first-line therapy for people living with HIV. Dolutegravir, and integrase strand transfer inhibitor administered in combination with two nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs)15,16
Evidence from cohorts and large-scale programmatic rollouts across African settings demonstrates high viral suppression rates ranging from 90% to 92% among children and adolescents transitioned to dolutegravir-based regimens, including those who were previously unsuppressed, underscoring the effectiveness of DTG in routine clinical practice.21-24 As a result, DTG-containing regimens are projected to become the most widely used antiretroviral therapy globally, particularly in low-and middle-income countries, by 2025. 25 Notwithstanding these gains, significant disparities in viral suppression persist, and uptake of DTG-based ART remains below global targets, especially among younger children and those populations faced barriers to care, such as adherence difficulties and inconsistent retention in treatment programs.23,26,27
Although individual studies have reported encouraging outcomes, the overall impact of dolutegravir-based antiretroviral therapy on viral suppression and the uptake of DTG-based regimens among pediatric HIV patients in Africa has not been systematically quantified. Current existing evidence is fragmented, with wide variability in reported outcomes and a lack of comprehensive continent -wide estimates. In particular, data on the uptake of DTG-based regimens from NNRTI-based regimens to DTG-based art is a critical indicator of treatment optimization and program effectiveness have not been comprehensively synthesized. Therefore, this systematic review and meta-analysis aimed to estimate the pooled rate of viral suppression and the uptake of newly recommended DTG-based regimens ART among children and adolescents receiving DTG-based ART in Africa. The findings are intended to provide robust evidence to inform clinical practice guide policy formulations, support target interventions to enhance pediatric HIV care and outcomes, and promote health equity across the region.
Methods
Study Design
This systematic review and meta-analysis were employed to evaluate the effectiveness of dolutegravir-based antiretroviral therapy, measured by viral load suppression, and to assess the uptake of dolutegravir-based regimens among pediatric HIV patients in Africa.
Search Approach and Appraisal of Studies
This review was conducted in compliance with the 2020 PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) guidelines 28 (Supplementary file S1). This systematic review and meta-analysis was not registered in PROSPERO because the review process had already commenced before protocol registration was considered. A comprehensive literature search was undertaken between January 01 and January 10, 2026, to identify relevant published studies. Electronic search databases, including PubMed, ScienceDirect, Google Scholar, Hinari-Research4life, the Directory of Open Access Journals (DOAJ), and the CORE database, were systematically searched. Both Medical Subject Headings (MeSH) and relevant keywords were employed to ensure a thorough and structured retrieval of the literature. Additionally, targeted Google searches were performed to capture unpublished studies and other sources of gray literature.
Two reviewers (D.M and A.S) independently conducted the literature search and screened all eligible human studies published up to the final search date. Disagreements were resolved through consensus. The search strategy was guided by the COCO Pop framework (condition, context, and population), with the condition defined as viral load suppression following initiation of dolutegravir(DTG) and the uptake of dolutegravir-based regimens from older antiretroviral regimens to DTG-based antiretroviral therapy, the context as Africa, and the population as children and adolescents living with HIDTG-manuscript V.
A comprehensive search strategy was employed to maximize the retrieval of relevant studies. Boolean operators (AND, OR) were used to combine key search terms, including “viral load suppression,” “virologic suppression,” “VS,” “dolutegravir-based antiretroviral therapy,” “DTG,” and “DTG uptake”, or “ uptake of DTG-based ART,” along with population and region-specific terms such as “ children,” “adolescents,” and “Africa. “Search strategies were tailored to the indexing requirement of each database. In Google Scholar, the following search strings were applied. (“Dolutegravir-based antiretroviral therapy” OR “DTG-based ART”) AND (“viral load suppression” OR “virologic suppression” OR “VS”) AND (“pediatric HIV patients” OR “children” OR “adolescent”) AND Africa.
For PubMed and Hinari-Research4Life, a structured strategy was applied using a combination of Medical Subject Headings (MeSH) and free text terms. The search included terms related to dolutegravir, viral suppression, DTG uptake, HIV infection, and pediatric populations. The following search string was used: (“Dolutegravir’’ [MeSH Terms] OR “Dolutegravir’’ [Title/Abstract] OR “DTG-based ART’’ [Title/Abstract] OR “Dolutegravir-based antiretroviral therapy’’ [Title/Abstract]) AND (“viral load’’ [MeSH Terms] OR “viral load suppression’’ [Title/Abstract] OR “virologic suppression’’ [Title/Abstract]) AND (“DTG uptake’’ [Title/Abstract] OR “uptake of DTG-based ART’’[Title/Abstract] OR “switching to DTG-based ART’’[Title/Abstract]) AND (“HIV infection’’[MeSH Terms]) AND (“child’’[MeSH Terms]OR “adolescent’’[MeSH Terms] OR child* [Title/Abstract] OR adolescent* [Title/Abstract]) AND Africa[Title/Abstract].
Similarly, the Directory of Open Access Journals (DOAJ) was used using stepwise keyword strategies. A broad search using “dolutegravir AND HIV” identified 826 records. Refinement using “dolutegravir AND pediatric AND HIV” yielded 14 records. Then a highly specific search using “(dolutegravir OR DTG) AND (pediatric OR child OR adolescent) AND (viral load OR viral suppression) AND HIV*” identified two records. Due to database limitation, complex Boolean logic was applied cautiously, and results were supplemented by broader searches and for CORE database was searched using (“dolutegravir’’ OR “DTG”) AND (“pediatric” OR child* OR adolescent* OR infant*) AND (“HIV” OR “human immunodeficiency virus”) AND (“viral load” OR “viral suppression”) AND (switch* OR “uptake of DTG-based ART” OR “regimen change”), limited by year, research articles and English langue.
Additionally, we used (“dolutegravir” OR “dolutegravir-based antiretroviral therapy”) AND (“viral load suppression” OR “virological suppression”) AND (“uptake of DTG-based ART” OR “regimen switching”) AND (child* OR adolescent*) AND (each nation), restricted by select open access in the ScienceDirect database, was applied (Supplementary file S2). All retrieved records were imported into EndNote X9 reference manager software to remove duplicates and organize citations. This approach ensured a comprehensive search and identification of all relevant studies for inclusion in the systematic review and meta-analysis.
Outcome Measurement
This systematic review and meta-analysis aimed primarily to estimate the pooled prevalence of viral load suppression among children and adolescents living with HIV following initiation of dolutegravir-based antiretroviral therapy. As a secondary objective, the study assessed the pooled uptake of DTG-based ART among children and adolescent populations in Africa.
Operational Definitions
Study Selection
After removal of duplicate records, the abstracts of all retrieved studies identified through electronic database searches were screened by two reviewers (D.M and A.S). Articles deemed potentially eligible according to the predefined inclusion criteria were subsequently subjected to full-text review and independently assessed by a third reviewer (T.K). Any disagreement among reviewers was resolved through discussion and consulting with a fourth reviewer at any stage of the selection process. All studies excluded during the full-text review were recorded along with the reason for their exclusion.
Inclusion Criteria
This systematic review and meta-analysis incorporated both published and grey literature reporting data on viral load suppression following initiation of dolutegravir-based antiretroviral therapy, as well as outcomes related to uptake of DTG-based regimens, without restriction of publication date. Eligible study designs included randomized controlled trials, cross-sectional studies, and prospective and retrospective cohort studies.
Exclusion Criteria
Non-English language publications were excluded due to limited resources for translation. In addition, case reports, case series, qualitative studies, articles that did not report outcomes relevant to the objective of this review, and studies for which the full text was unavailable were all excluded.
Data Extraction
Data extraction was conducted independently by two reviewers (D.M and A.S) and subsequently verified by a third reviewer to ensure completeness and accuracy. Extracted variables included the first author’s surname, year of publication, study design, sample size, and number and proportion of children and adolescents achieving viral load suppression following initiation of dolutegravir-based antiretroviral therapy, and uptake of DTG-based ART among those previously receiving older ART regimens. All data were compiled using a standardized Microsoft Excel extraction form. Discrepancies between reviewers were resolved through discussion, and a third reviewer made the final determination when consensus could not be achieved. The data extraction process was carried out between January 16 and 25, 2026.
Data Quality Control Measures
The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal checklists, adopted for prevalence and incidence studies 31 as well as for retrospective and prospective cohort designs. 32 This appraisal tool is used to evaluate the methodological quality of the included studies and to assess the extent to which potential sources of bias in the study design, data collection, and analysis were assessed. Quality assessment was conducted independently by two reviewers (D.M and A.S) between January 11 and 15, 2026. Studies were categorized as low (>70%), medium (50-70%), or high (<50%) risk of bias. Studies meeting or exceeding the medium and low risk of bias were included, while those scoring high risk of bias were excluded. Discrepancies between reviewers were resolved through discussion (Supplementary File S3).
Grade Assessment
The certainty for each primary outcome was assessed using the Grade of Recommendations Assessment, Development and Evaluation (GRADE) approach. Evidence quality was evaluated across five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. The certainty of evidence for each outcome was classified as high, moderate, low, or very low based on the overall strength of the available evidence.33-35 Details of the GRADE assessment approach are provided in (Supplementary File S4).
Statistical Analysis
For analysis, data from each study were extracted into an Excel spreadsheet and subsequently imported into Stata 17.1. Findings were summarized narratively according to participants’ characteristics. Heterogeneity was assessed using the I2 statistic, with a fixed-effect model applied for low heterogeneity (I2<50%) and a random-effect model for higher heterogeneity (I2≥50%). Due to significant heterogeneity among included studies, the pooled estimate of viral load suppression following initiation of DTG-based ART and the pooled uptake of DTG-based regimens in children and adolescents were computed using a random-effect model. Subgroup analyses were conducted by geographical region, study design, and sample size to explore sources of heterogeneity and reduce random variation. Publication bias was evaluated using funnel plot symmetry inspection, the regression-based Egger test, and nonparametric trim-and-fill analysis. Sensitivity analysis was used to assess the influence of individual studies on the overall pooled estimate. Throughout, the PRISMA 2020 guidelines were followed to ensure transparency and appropriate handling of missing data.
Result
A comprehensive literature search was conducted from January 1 to 10, 2026, across multiple databases, including Google Scholar (n=1,410), PubMed (n=4,733), ScienceDirect (n=1,350), Hinari (Research4Life) (n=101), CORE (n=193), and the Directory of Open Access Journals (DOAJ) (n=2), yielding a total of 7,789 records. After removing 5,377 duplicates, 2,412 articles remained for screening. Title and abstract screening excluded 1,763 studies that did not meet the inclusion criteria. Of the 649 articles assessed in full text, 539 were excluded due to reporting outcomes unrelated to the review, 40 were conducted outside Africa, six were unavailable in full text, four used different viral load cutoff points to define suppressed viral load, one was a review article, and 35 were duplicates. Ultimately, 24 studies met the inclusion criteria and were included in this systematic review and meta-analysis (Figure 1). PRISMA flow diagram illustrating the identification, screening, eligibility assessment, and selection of studies included in the systematic review and meta-analysis of the impact of dolutegravir-based antiretroviral therapy (ART) on viral load suppression and switching rates among children and adolescents living with HIV in Africa.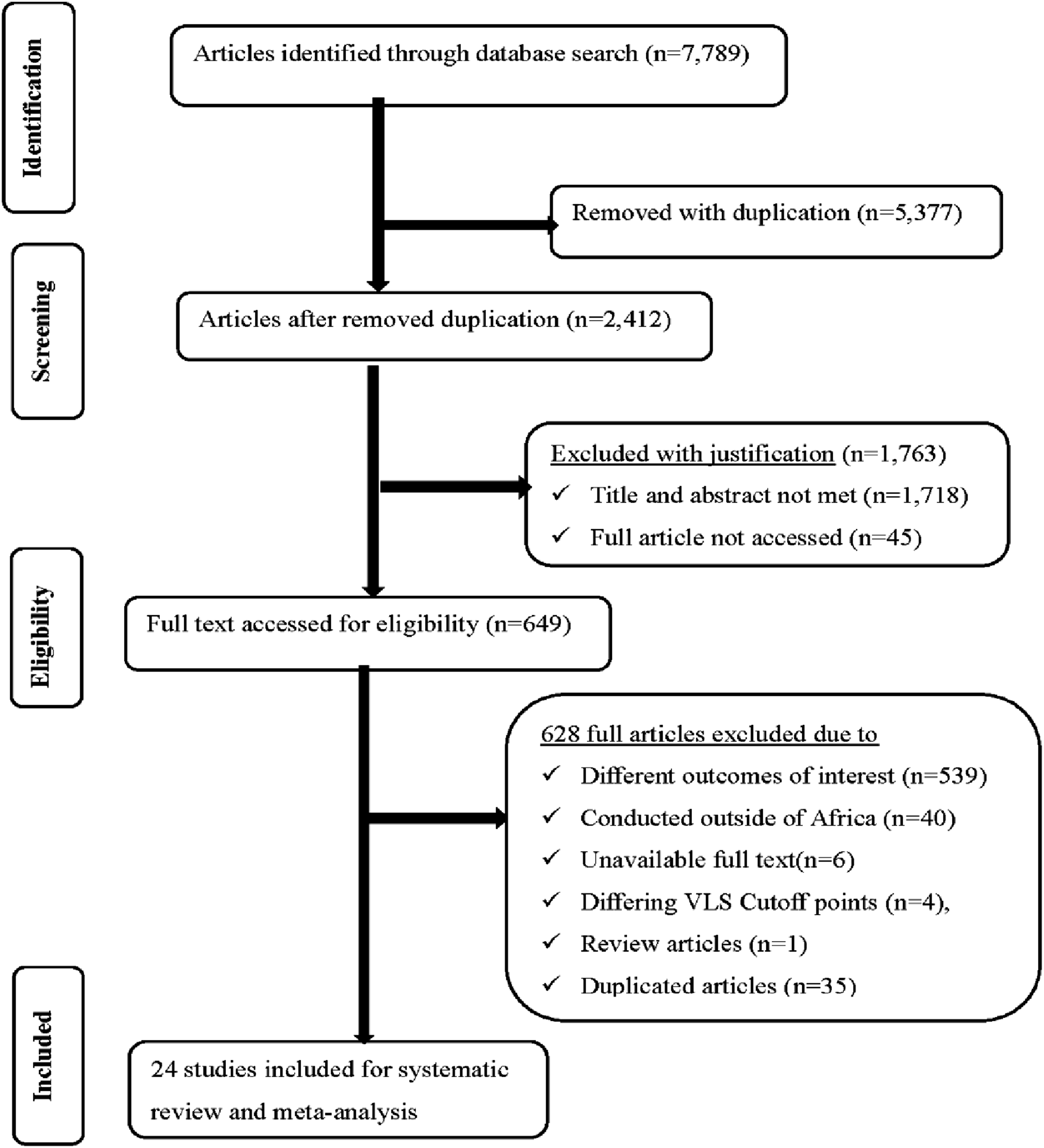
Characteristics of the Included Studies
This systematic review and meta-analysis included 24 primary studies investigating the impact of dolutegravir-based antiretroviral therapy on viral load suppression and uptake of DTG-based ART among children and adolescents living with HIV across Africa. This systematic review encompassed studies of participants with both initially unsuppressed viral load and those with viral load suppressed at baseline before the initiation of DTG-based ART. Fourteen (58%) studies specifically evaluated viral load suppression among children and adolescents who were initially unsuppressed, while the remaining studies assessed the effect of DTG regardless of baseline viral load.
All studies included in this systematic review and meta-analysis were published between 2020 and 2026 and were conducted in Cameroon,36-38 Kenya, 39 Malawi,40,41 Mozambique,23,26 Uganda,27,42-44 Lesotho,21,45 Nigeria,46,47 Tanzania,48-51 Ethiopia, 52 Zimbabwe, 53 Togo 54 and as well as one regional study done in eastern and southern countries. 22 Geographically, three studies originated from were conducted in West Africa,46,47,54 three in central Africa,36-38 ten in east Africa,27,39,42-44,48-52 seven in southern Africa,21,23,26,40,41,45,53 and one regional study spanning eastern and southern Africa. 22 The sample size ranged from 40 participants 21 to 15, 166 participants. 49
Viral load suppression rate varying from a minimum of 38.9% 52 to a maximum of 87.8% 27 among the studies assessing the effect of dolutegravir on viral load suppression, who were initially unsuppressed, whereas studies reporting overall viral load suppression following DTG-based regimens, regardless of baseline viral load, suppression rate ranged from 45.3% 47 to 94.7%. 45
Across studies assessing the impact of dolutegravir among children and adolescents who were unsuppressed at baseline, a total of 19,328 participants were included, of whom 12,586(65.1%) achieved viral suppression. In studies evaluating DTG-associated viral suppression irrespective of baseline viral load, 119,292 children and adolescents were included, with 104,968 (88.0%) achieving an overall suppression rate.
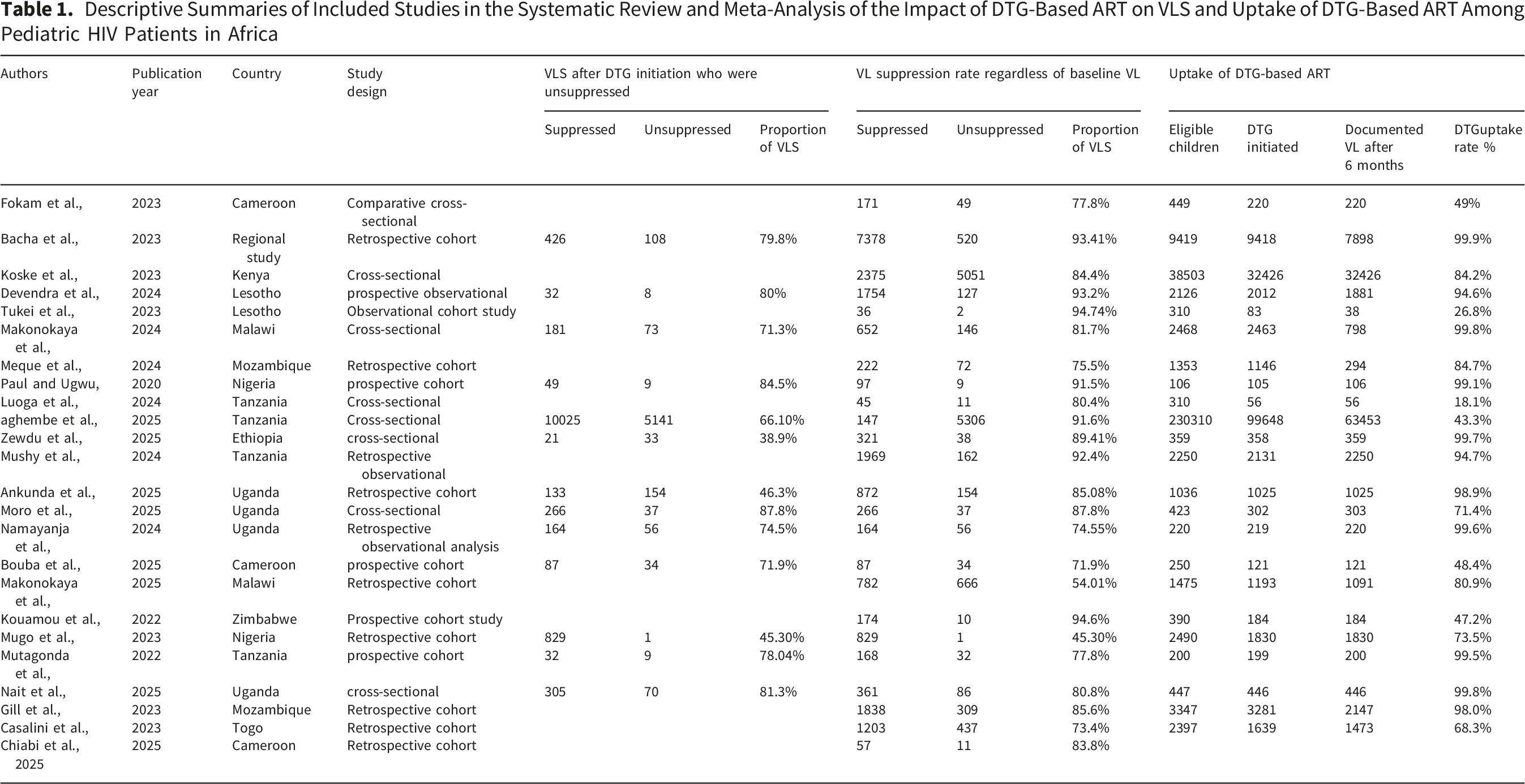
Descriptive Summaries of Included Studies in the Systematic Review and Meta-Analysis of the Impact of DTG-Based ART on VLS and Uptake of DTG-Based ART Among Pediatric HIV Patients in Africa
Pooled Viral Load Suppression After Initiation of DTG-Based Antiretroviral Therapy
This systematic review and meta-analysis included 14 primary studies21,22,27,34,38-41,43,44,46,48-50 comprising 19,283 HIV infected children and adolescents with baseline viral load exceeding 1000copies/mL before initiation of dolutegravir-based antiretroviral therapy. Following treatment initiation, 65.1% of participants achieved viral load suppression.
To estimate the pooled prevalence of viral load suppression following the initiation of dolutegravir-based ART, heterogeneity among the included studies was first assessed using the fixed-effect model. This assessment revealed substantial heterogeneity (I2 = 98.21%, P < 0.01), warranting a random-effects approach for the pooled analysis. Accordingly, the DerSimonian-Laird random effect model was applied, yielding a pooled viral load suppression rate of 70 %( 95% CI: 62-77%) after six months across the 13 studies (Figure 2). The certainty of evidence for this outcome was rated as low due to substantial heterogeneity and observational study designs. Pooled prevalence of viral load suppression after initiation of DTG-based antiretroviral therapy among children and adolescent HIV patients in Africa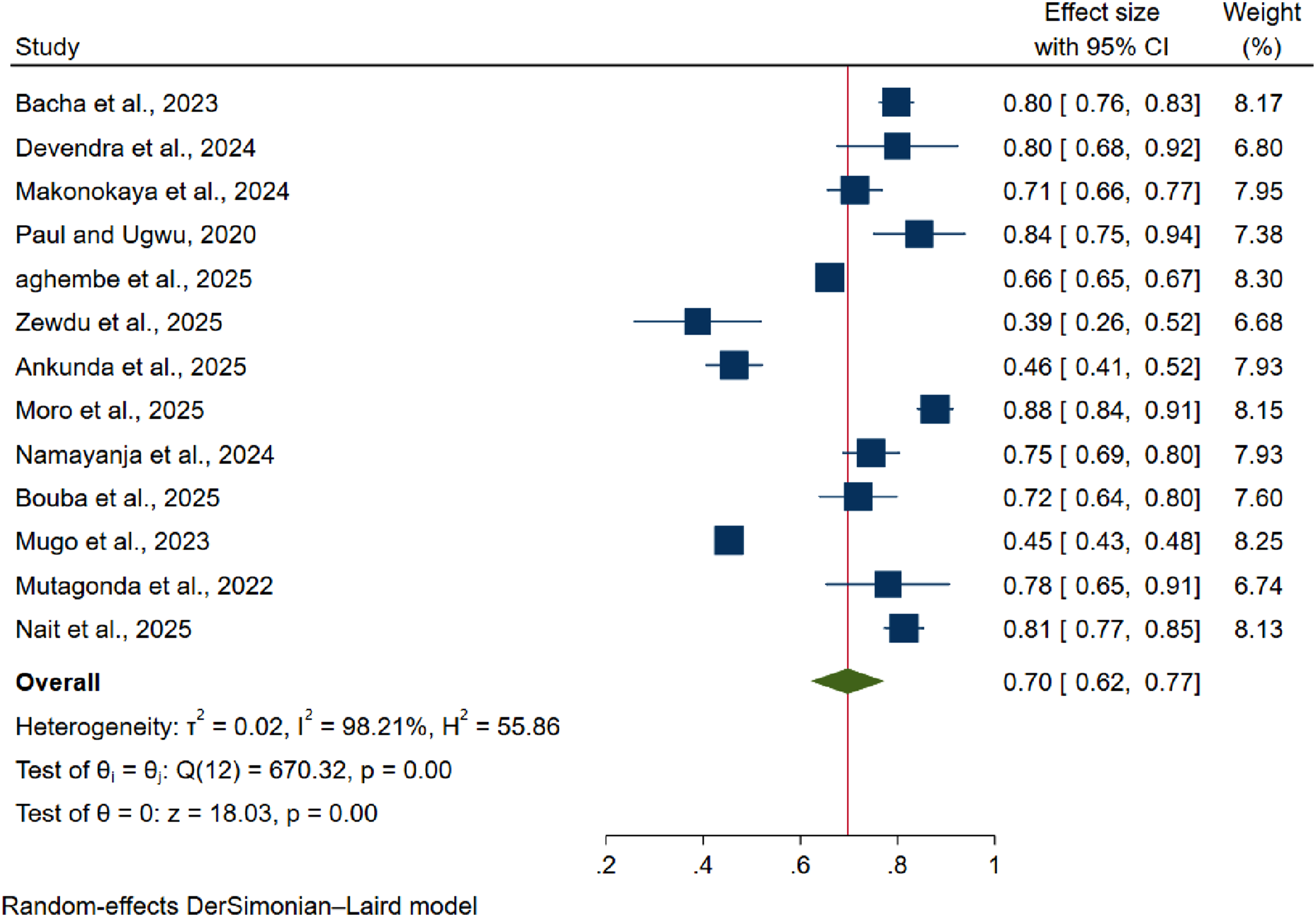
Pooled Viral Load Suppression Following DTG-Based ART Initiation, Regardless of Baseline Viral Load
To estimate the pooled viral load suppression following DTG-based ART initiation, regardless of baseline viral load, 24 studies involving 119,292 HIV-infected children and adolescents were analyzed. Among these, 104,968 (88.0%) achieved viral load suppression during the follow-up period. Heterogeneity among the included studies was first assessed using a fixed-effect model to estimate the pooled prevalence of viral suppression six months after initiation of DTG-based ART. This revealed variability was observed (I2=99.41%, p<0.001), leading to the application of a random-effect model for the pooled analysis. Using the DerSimonian-Laird random-effect model, after six months of DTG-based ART initiation irrespective of baseline viral status, pooled viral suppression was 82% (95% CI:79-85%) across the 24 studies (Figure 3). The certainty of evidence for this outcome was rated as low to moderate due to substantial heterogeneity and observational designs of included studies. Pooled prevalence of viral load suppression following DTG-based ART initiation, regardless of baseline viral load among children and adolescents with HIV in Africa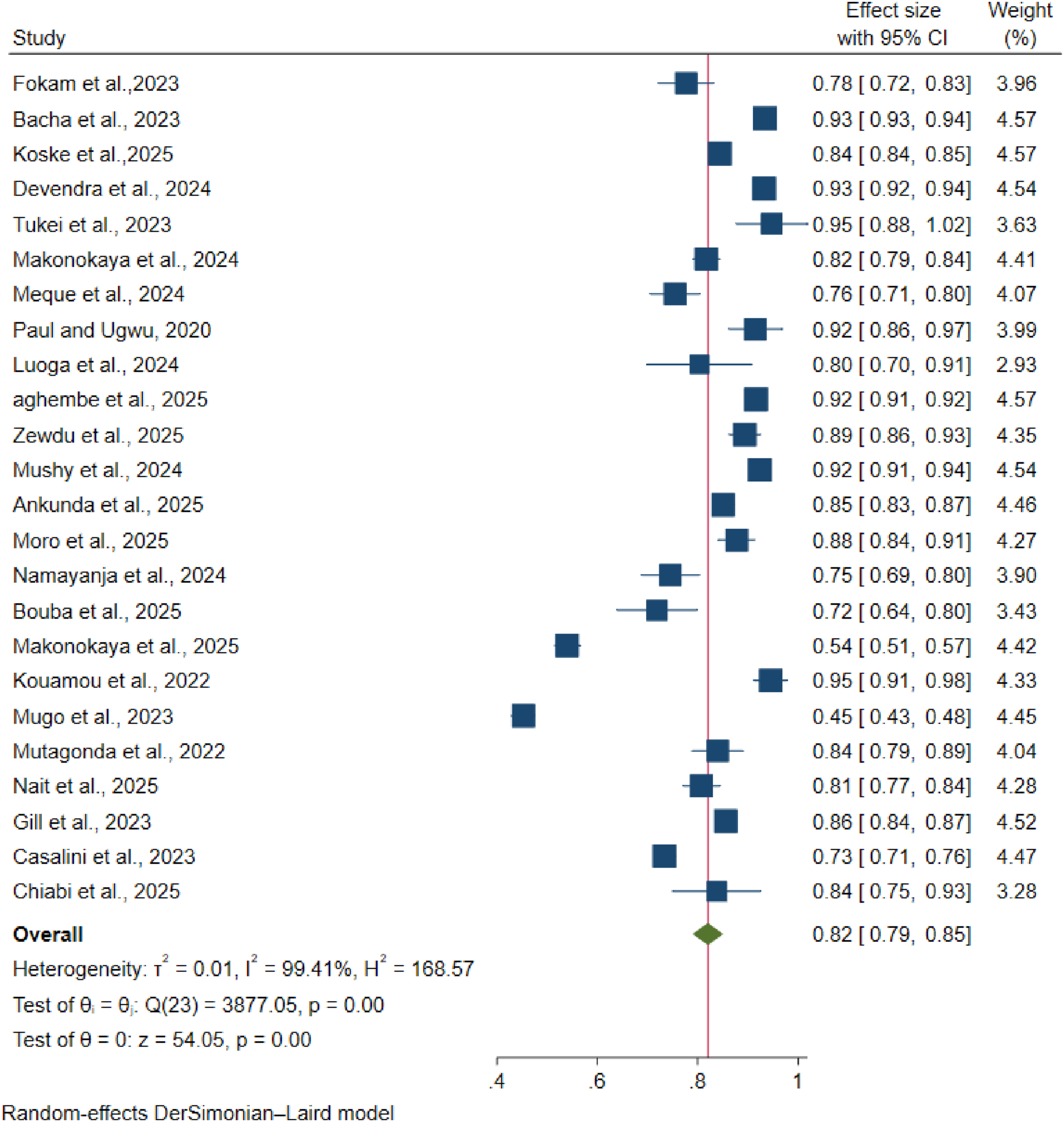
Pooled Uptake of Dolutegravir-Based ART Among Children and Adolescents
To estimate the pooled uptake of dolutegravir-based antiretroviral therapy among children and adolescents, 23 primary studies including 300,638 HIV-infected children and adolescents eligible for ART were analyzed. Of these, 160,505 (53.3%) initiated DTG-based ART, either as naïve treatment or transitioned from previous ART regimens. This proportion represents the simple arithmetic proportion across all included participants, whereas the pooled estimate derived from the meta-analysis reflects a weighted average that accounts for study-level variance and sample size.
To estimate the pooled uptake of the DTG-based ART regimen among children and adolescents in Africa, heterogeneity across the included studies was first assessed using a fixed-effect model. This analysis revealed substantial heterogeneity (I2=99.99, P<0.001), prompting the use of a random-effects model for the final pooled analysis. Using the DerSimonian-Laird random-effects approach, the pooled uptake of DTR-based ART regimens among 300,638 HIV infected children and adolescents in Africa was 77% (95% CI: 68-86%) (Figure 4). The certainty of evidence for this outcome was rated as very low due to extreme heterogeneity and variability in programmatic implementation across settings. Pooled uptake of dolutegravir-based ART among children and adolescent HIV patients in Africa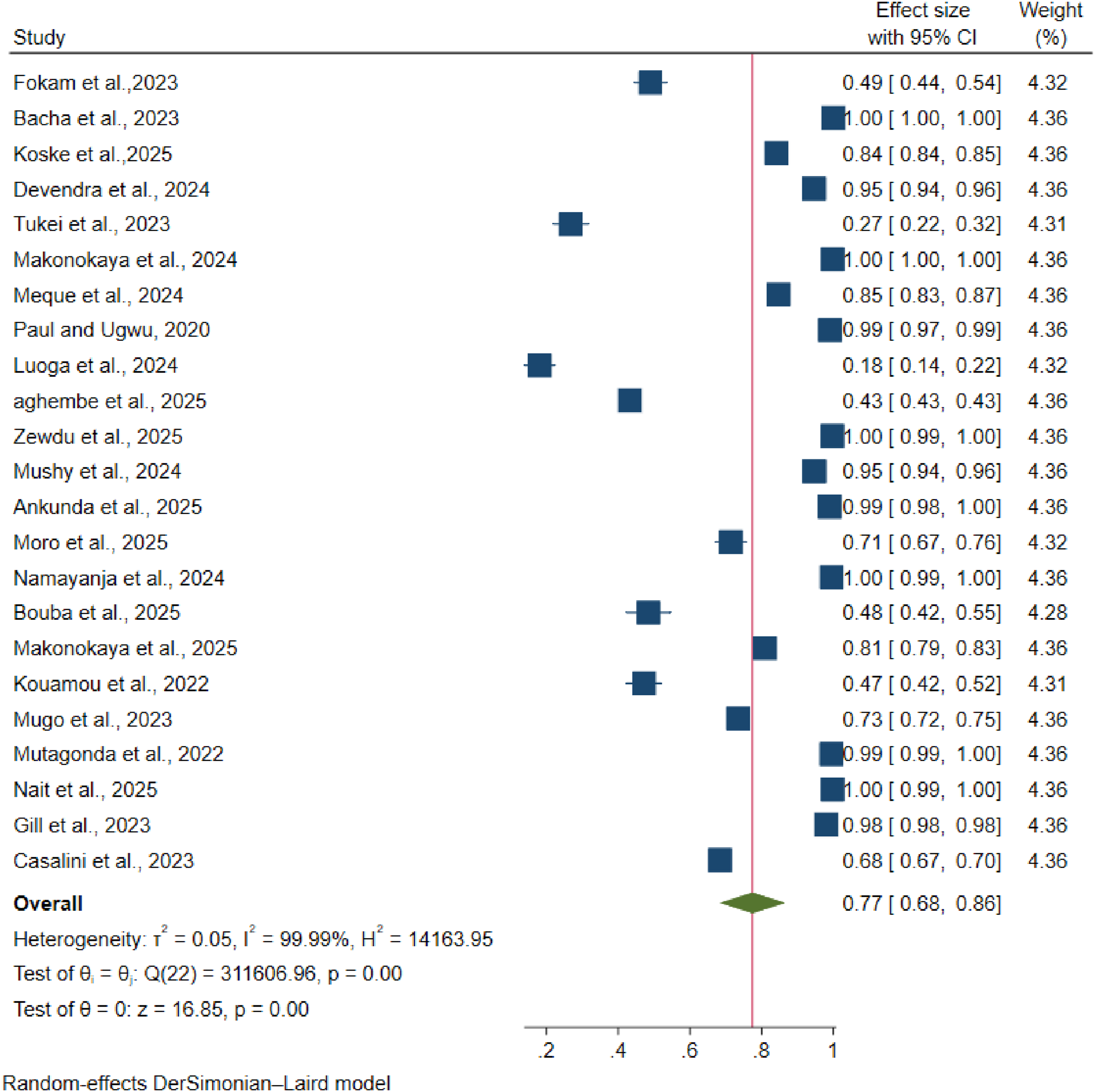
Subgroup Analysis of DTG-Based ART Outcomes Among Children and Adolescents in Africa
We used a random-effects model to carry out subgroup analyses of the three main outcomes following DTG-based ART in African children and adolescents: viral suppression (VS), VS regardless of baseline viral load, and uptake of newly endorsed DTG-based antiretroviral therapy. Subgroup analyses were stratified by geographic region, study design, and sample size.
Subgroup Analysis for VS After DTG-Based ART Among Children and Adolescents in Africa
The analysis of viral suppression after DTG-based ART among children and adolescents who were unsuppressed before initiation of DTG-based ART revealed high heterogeneity (I2=98.08%, τ2=0.02, p<0.001), demonstrating that discrepancies in VS estimates across studies are likely due to real variance rather than random effects. This diversity may be influenced by factors such as study design, demographic characteristics, VL test, and follow-up period. To identify potential sources of variability, we conducted subgroup analyses based on geographical region, design of the study, and sample size.
Subgroup Analysis of Viral Load Suppression After Initiation of DTG and Uptake of DTG-Based ART Among Children and Adolescents in Africa
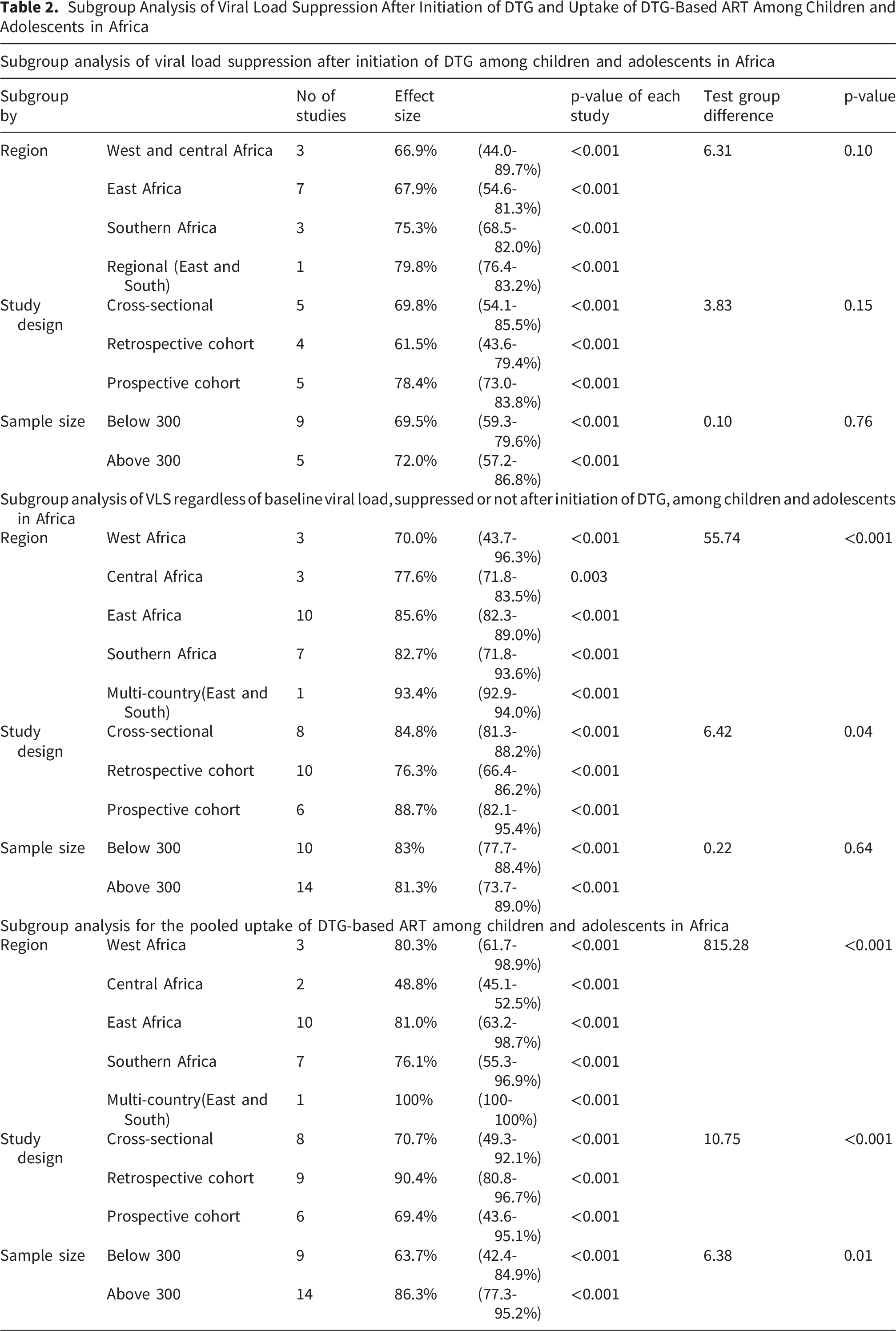
Similarly, subgroup analysis by study design revealed variation in pooled viral suppression estimates. Cross-sectional studies reported a pooled VS proportion of 69.8 %( 95% ci: 54.1-85.5%), while retrospective cohort studies demonstrated a lower pooled estimate of 61.5% (95% CI: 43.6-79.4%). In contrast, prospective cohort studies yielded the highest pooled proportion of 78.4% (95% CI: 73-83.8%). Despite these differences, the test for subgroup difference by study design was not statistically significant (Q=3.38, P=0.15), indicating no significant variation in VS across study design (Table 2).
Furthermore, VS estimations were comparable across investigations with varying sample sizes. Studies with fewer than 300 respondents found a pooled VS proportion of 69.5% (95% confidence interval: 59.3-79.6%), while studies with 300 or more participants reported a comparable estimate of 72% (95% CI: 57.2-86.8%). There was no statistically significant subgroup difference (Q=0.10, p=0.76), showing that sample size had no meaningful influence on VS results (Table 2).
Subgroup Analysis of VS After DTG-Based ART Initiation Regardless of Baseline VL Status Among Children and Adolescents
Using a random-effects model, subgroup analyses were performed to investigate VS outcomes after the introduction of DTG-based antiretroviral therapy among African children and adolescents, regardless of VS status before DTG initiation, stratified by geographical region, research design, and sample size.
Pooled viral suppression estimates varied significantly by geographic region, ranging from 70% in West Africa to 93.4% in a multi-country study from east and southern Africa, with significant regional variation(Q=55.54, P<0.001). when stratified by study design, VS was highest in prospective cohort studies (88.7%), followed by cross sectional studies (84.4%) and retrospective cohort studies (76.3%): these difference were statistically significant (Q=6.42, P=0.04). in contrast, VS rate were similar between studies with fewer than 300 participants (83%) and those with 300 or more participants (81.3%), with no evidence of subgroup difference (Q=0.22, P=0.64) (Table 2).
Subgroup Analysis of the Uptake of DTG-Based ART Among Children and Adolescents
The adoption of dolutegravir (DTG)-based antiretroviral therapy (ART) among African children and adolescents differed significantly across categories. The pooled uptake of DTG-based ART ranged from 48.8% in Central Africa to 100% in a multi-country study of Eastern and Southern Africa. Uptake rates were also high in West Africa (80.3%), East Africa (81.0%), and Southern Africa (76.1%), with statistically significant regional heterogeneity (Q = 815.47, p < 0.001).
Similarly, the transition from previous ART regimens to the newly recommended DTG-based therapy varied widely across study designs. Retrospective cohort studies had the highest pooled uptake (88.8%), followed by cross-sectional studies (70.7%) and prospective cohort studies (69.4%), with statistically significant differences (Q=10.75, p<0.001). Furthermore, sample size had a significant influence on uptake rates (Q=6.38, p=0.01); studies with 300 or more participants showed a greater pooled uptake (86.3%) than studies with fewer than 300 respondents (63.7%).
In general, DTG uptake differed significantly by geographical region, study design, and sample size, with a greater number of study participants consistently reporting higher uptake rates, indicating that contextual and methodological factors influence DTG uptake among African children and adolescents (Table 2).
Assessment of Publication Bias in Viral Load Suppression After DTG Initiation in Children and Adolescents in Africa
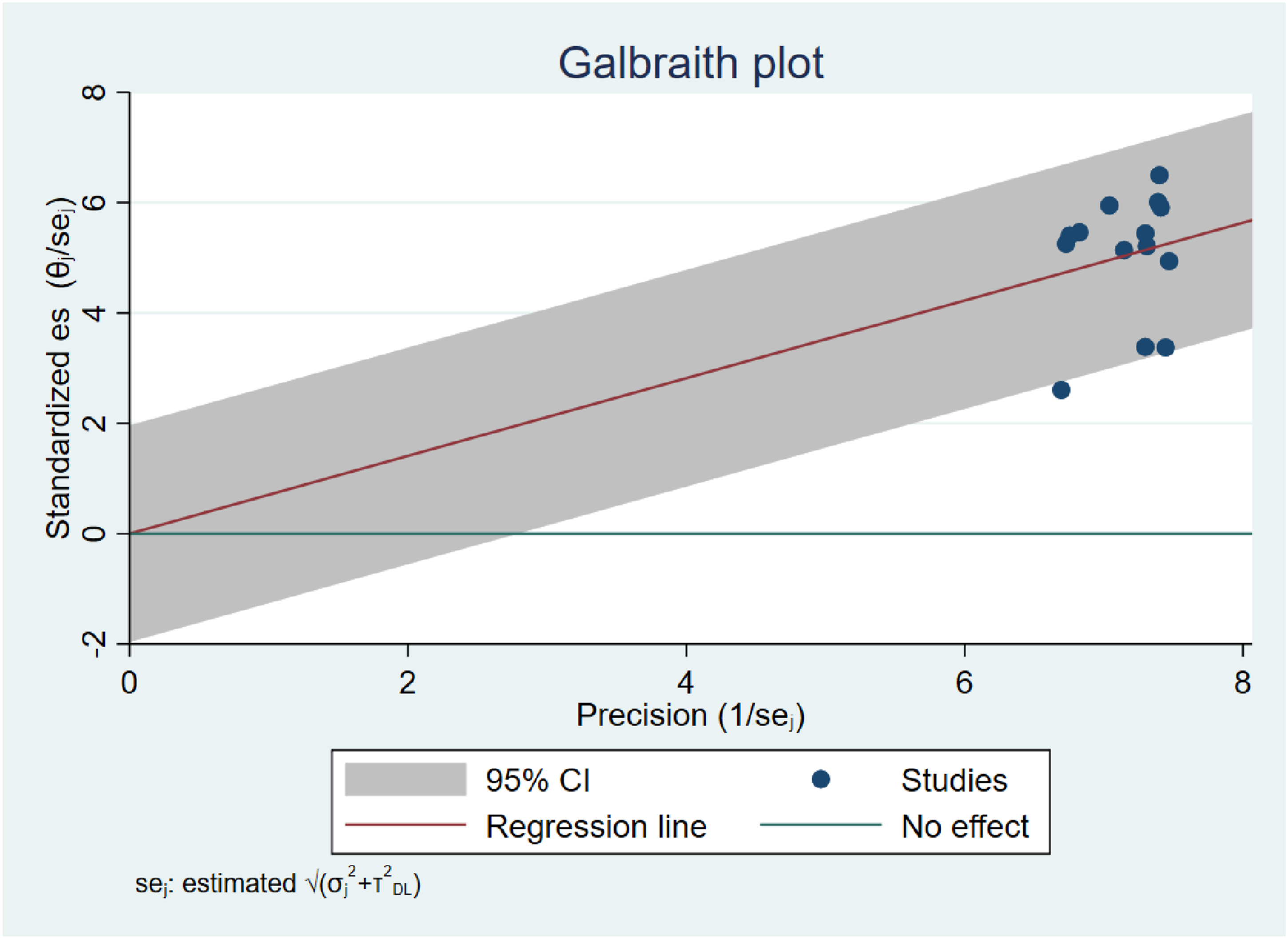
Visual inspection of the funnel plot, regression-based Egger test, and nonparametric trim-and-fill analysis were used to determine publication bias. Despite minimal asymmetry in the funnel plot (Figure 5), the Egger test for small-study effects was not statistically significant (β = 0.34, SE = 2.124, z =0.16, p=0.8718), revealing no evidence of such effects. Trim-and-fill analysis with a linear estimator did not impute any studies, and the pooled percent of viral load suppression remained at 66.1% (95% CI: 65.4-66.8%). Additionally, the Galbraith plot analysis confirmed there was no evidence of publication bias among the included papers (Figure 6). The plot showed that almost all studies were within the 95% confidence limits, with no noticeable outliers, indicating minor publication bias in the analyzed research. Assessment of publication bias in viral load suppression after DTG initiation in children adolescents HIV patients in Africa Galbraith plot test showing heterogeneity of viral load suppression after dolutegravir-based ART among children and adolescent HIV patients in Africa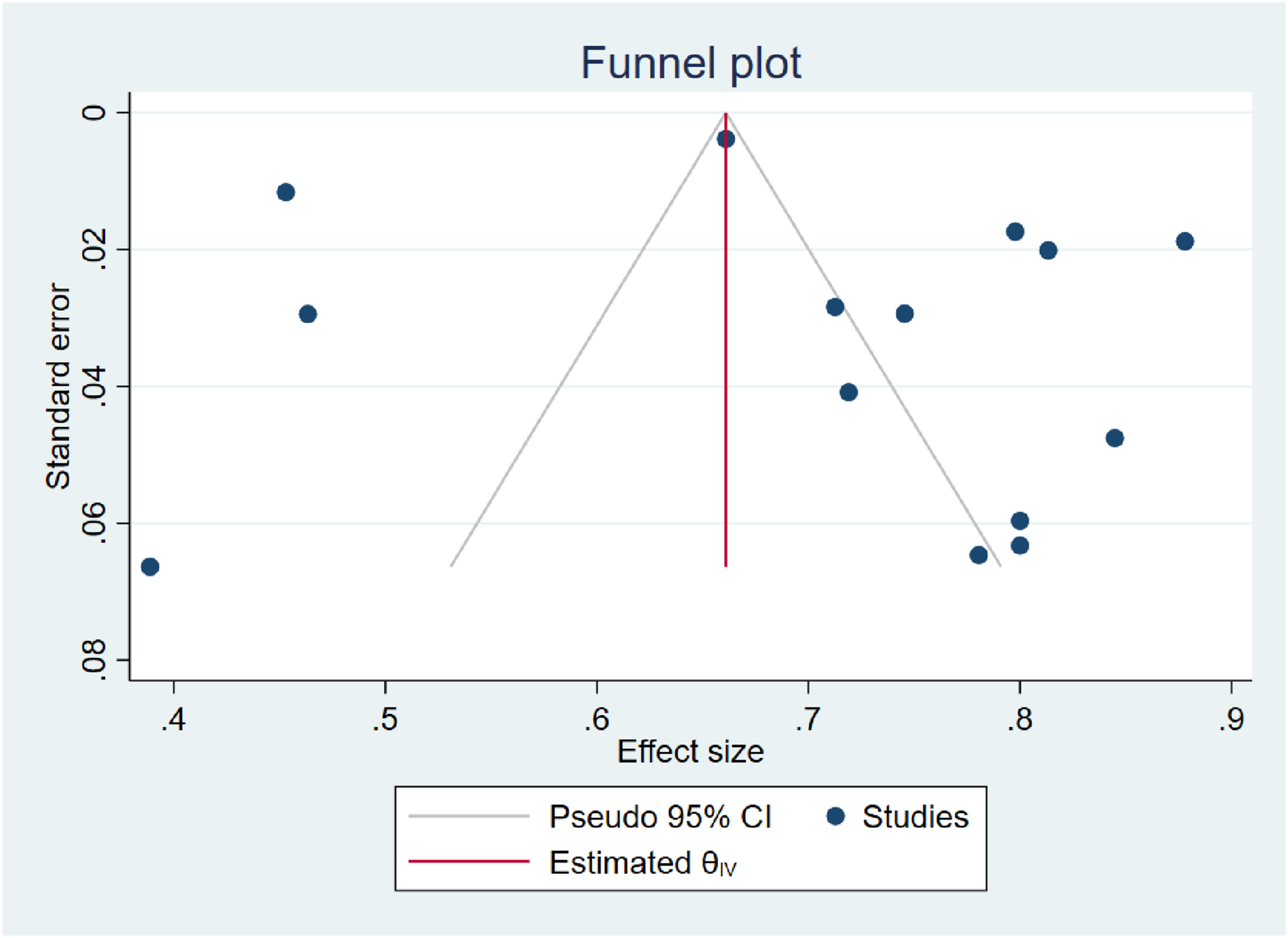
Assessment of Publication Bias for VS After DTG Initiation Irrespective of Baseline VL Status Among Children and Adolescents in Africa
Publication bias was assessed using visual inspection of funnel plot asymmetry, the regression-based Egger test, and nonparametric trim-fill analysis. The funnel plot (Figure 5) suggested potential asymmetry, indicating possible publication bias. However, the Egger test for small-study effect was not statistically significant (β=-0.97, SE=1.122, Z=-0.86, p=0.3876), providing no evidence of small- study effects. Consistently, the trim-and-fill analysis did not impute any studies, and the pooled proportion of viral suppression remained unchanged at 89.9 %( 95% CI: 89.9-90.1%).
Publication Bias Assessment for Uptake of DTG-Based ART Among Children and Adolescents in Africa
The possibility of publication bias in research findings reporting the proportion of children and adolescents initiating dolutegravir (DTG)-based ART in Africa was investigated using funnel plot inspection, Egger’s regression test, and nonparametric trim-and-fill analysis. Visual inspection of the funnel plot revealed some asymmetry (Figure 5), indicating potential small-study effects. The Egger test demonstrated a statistically significant difference (β=-20.70, SE=3.812, z=-5.43, p<0.001) between smaller and larger studies in terms of uptake. Therefore, a trim-and-fill analysis was used to determine the influence of these small-study effects on the pooled estimate. No studies were imputed, and the aggregated proportion of DTG uptake remained consistent at 99.3% (95% CI: 99.3-99.4%).
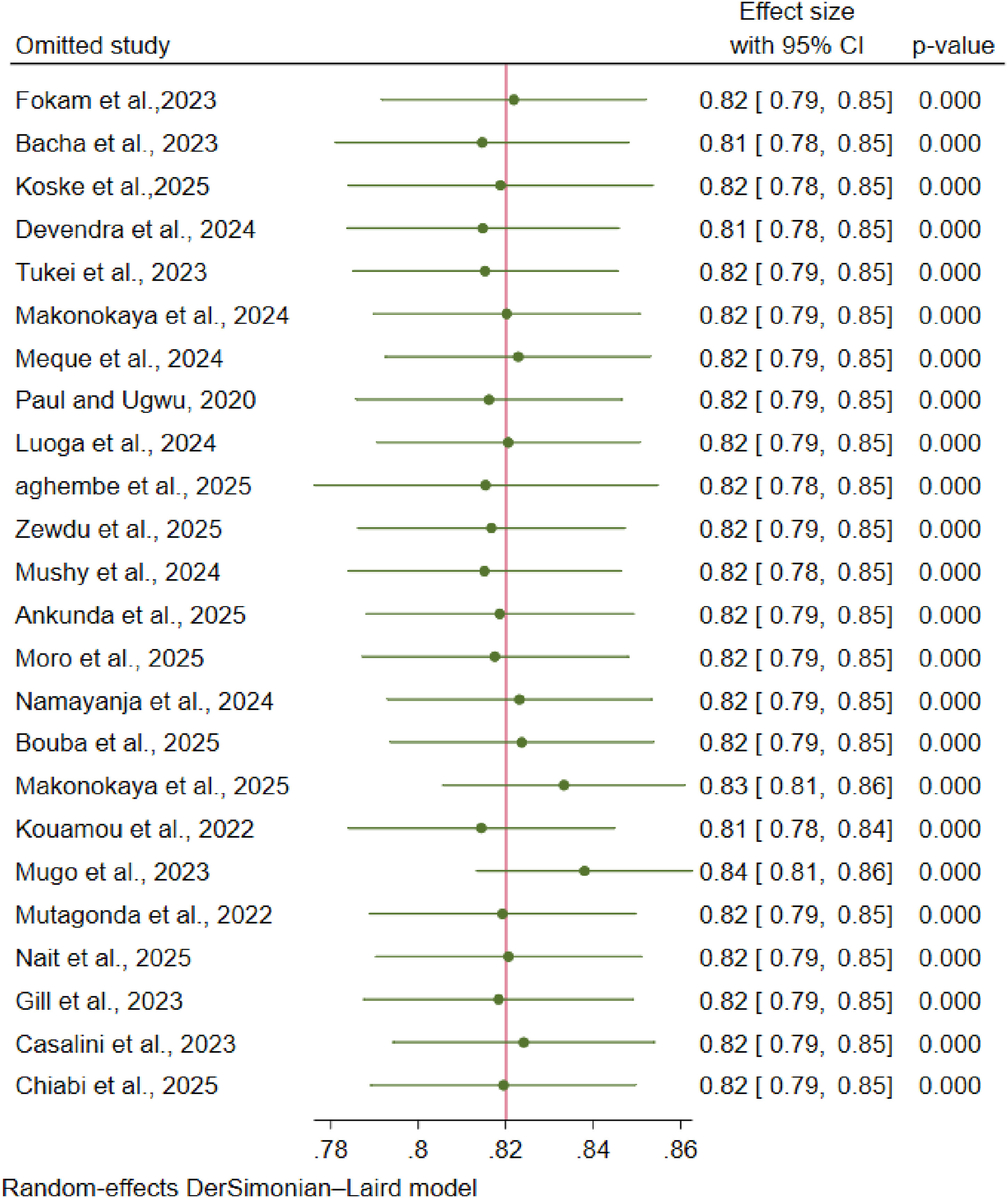
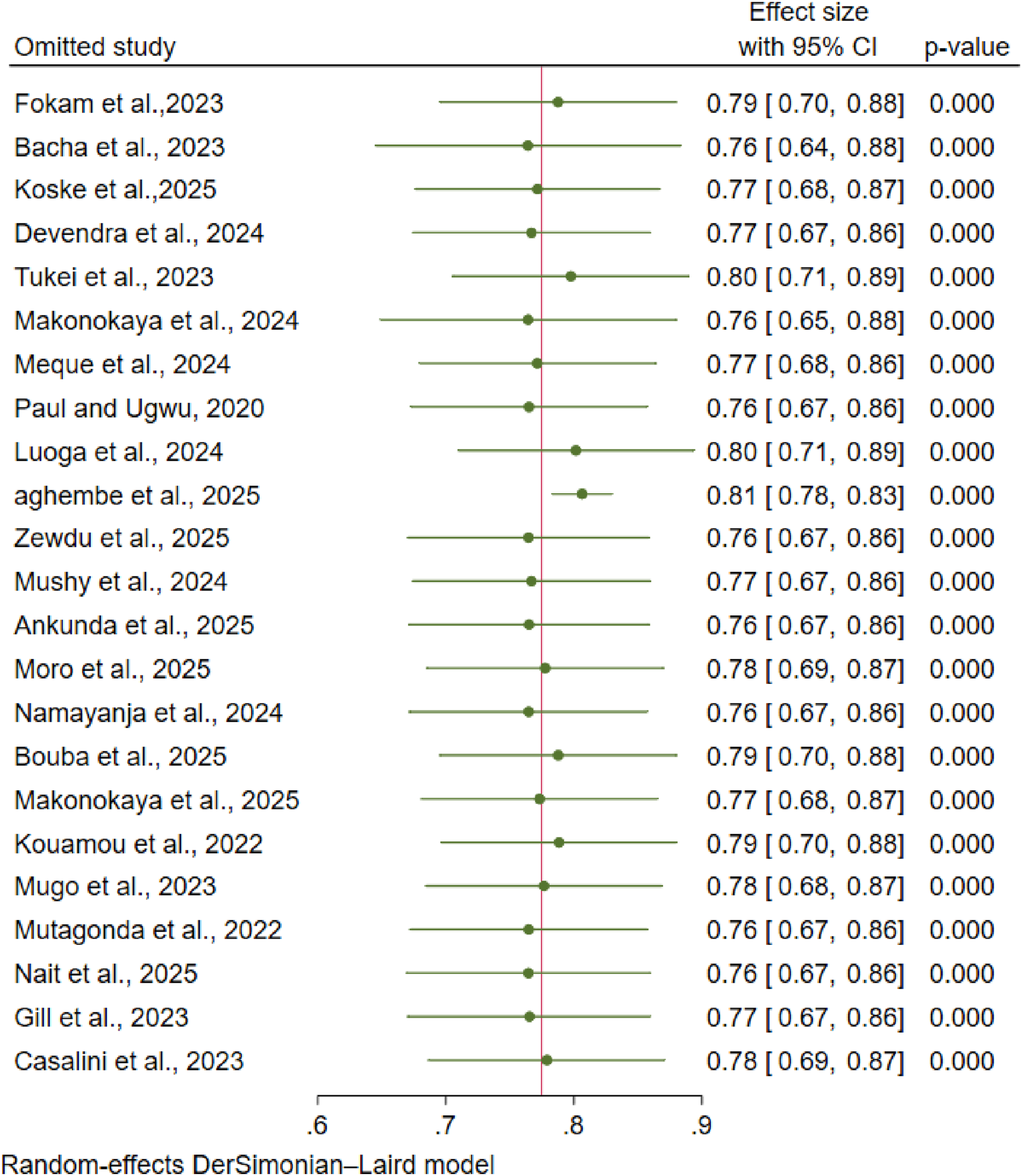
Sensitivity Analysis
A leave-one-out sensitivity analysis was carried out to determine the trustworthiness of the pooled effect sizes as well as the impact of individual studies. This method systematically removes each study successively and regenerates the pooled estimate. The investigation revealed that no single study had a disproportionate effect on the meta-analysis. The adjusted effect sizes were consistent, with point estimates ranging from 69-73%, 81-84%, and 76-81% for viral suppression (VS) following DTG-based ART initiation, VS irrespective of baseline viral load, and DTG uptake rates. The results remained statistically significant (p < 0.001), and the 95% CI continuously excluded the null value. These data suggest that the observed high positive relationships are robust and not attributed to a single study (Figures 7-9). Sensitivity analysis showing the effect of removing each study individually on the pooled prevalence of viral load suppression after initiation of dolutegravir-Based Antiretroviral Therapy among children and adolescents HIV Patients in Africa Sensitivity analysis showing the effect of removing each study individually on the pooled prevalence of viral load suppression after initiation of dolutegravir-Based Antiretroviral Therapy, irrespective of baseline viral load among children and adolescents HIV Patients in Africa Sensitivity analysis showing the effect of removing each study individually on the pooled uptake of dolutegravir-Based Antiretroviral Therapy among children and adolescents HIV Patients in Africa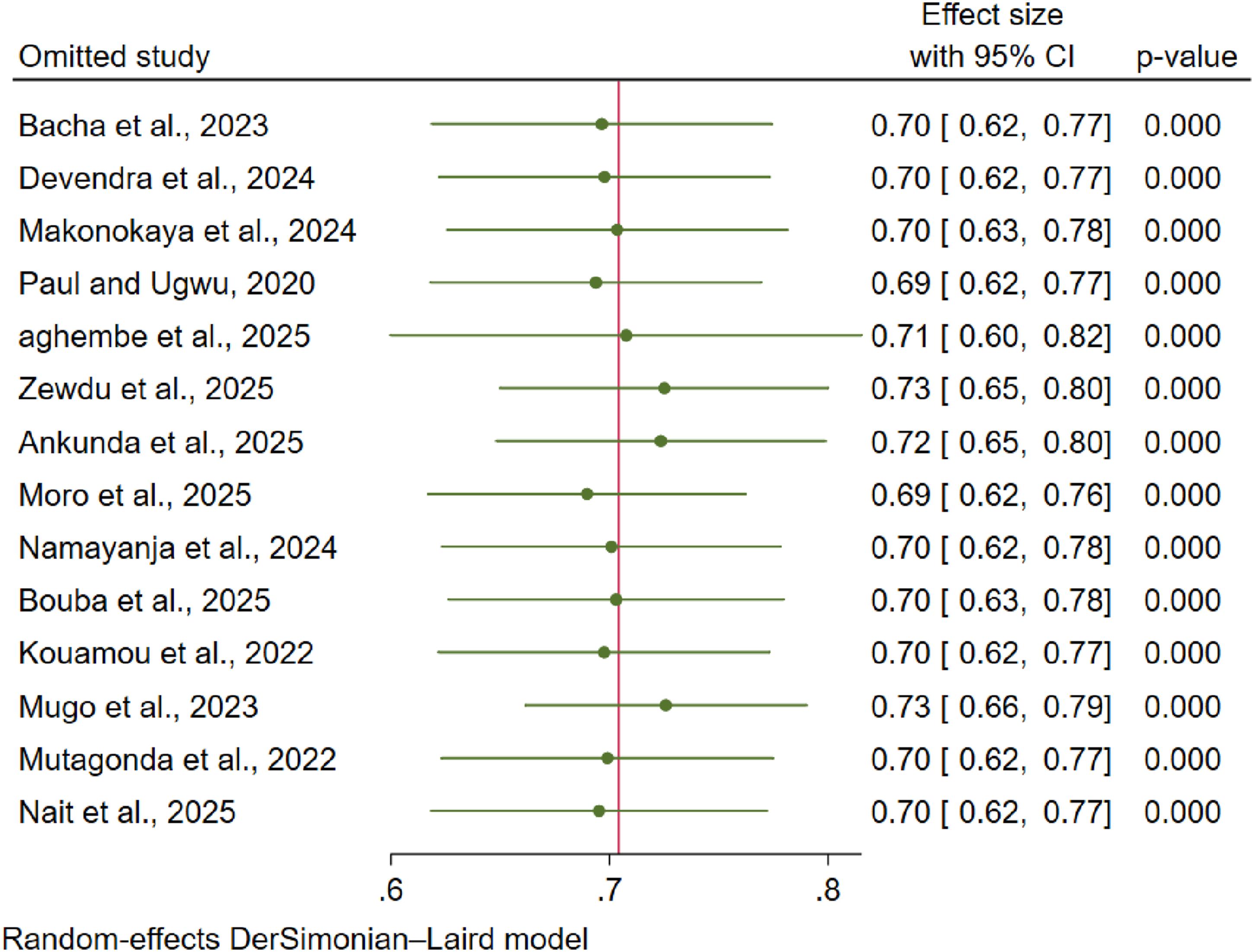
Meta Regression
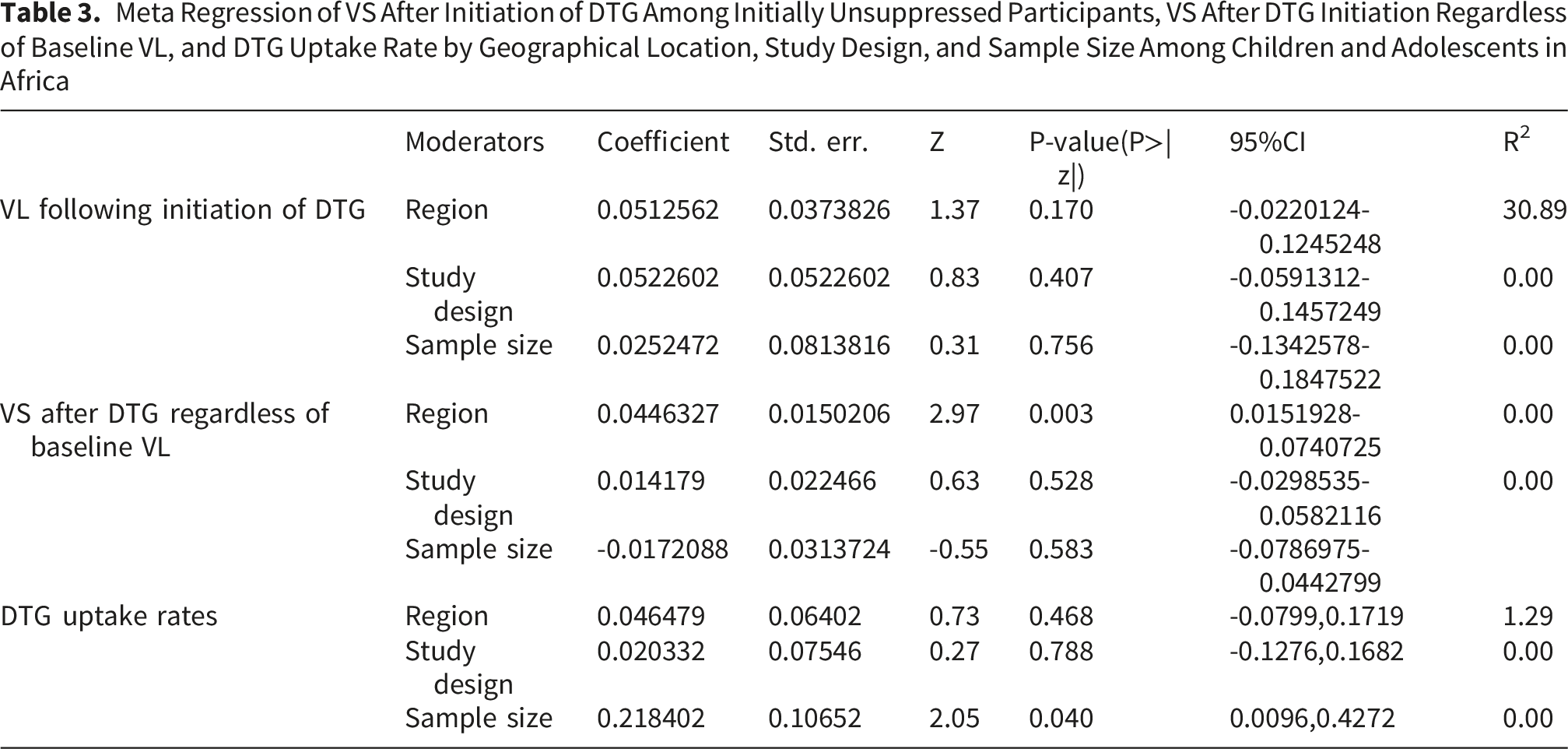
To explore sources of heterogeneity across the three meta-analysis outcomes, a series of random-effects meta-analyses were performed using geographical region, study design, and sample size as moderators. For viral suppression following DTG-based initiation, none of the moderators significantly affected the pooled effect (region=0.170; study design: p=0.407; sample size=0.756), explaining only a small portion of the variance (R2=0-30.89%), with a substantial residual heterogeneity remaining (I2=97.12%).In contrast, for VS after DTG initiation, irrespective of baseline viral load, geographical region was a significant predictor(β=0.0446,p=0.03), while study design(β=0.0144, p=0.528) and sample size (β=-0.172,p=0.583) were not. Despite this, the between-study variance remained unexplained (R2=0%), and residual heterogeneity was high (I2=99.5%), suggesting that additional unmeasured study-level or methodological factors likely contribute to the observed variability.
Meta Regression of VS After Initiation of DTG Among Initially Unsuppressed Participants, VS After DTG Initiation Regardless of Baseline VL, and DTG Uptake Rate by Geographical Location, Study Design, and Sample Size Among Children and Adolescents in Africa
Discussion
This systematic review and meta-analysis comprised 24 primary articles that included 119,292 HIV-positive children and adolescents who commenced dolutegravir (DTG)-based antiretroviral therapy (ART), regardless of their baseline viral load. Overall, 104,968 (88.0%) study participants experienced viral suppression over the follow-up period. Out of the 24 included studies, 14 reported patients with baseline viral loads >1,000 copies/mL (n=19,328), of whom 12,586 (61.1%) achieved viral suppression following DTG-based ART commencement.
There was significant heterogeneity among the studies (I2 = 98.08%, p = 0.01), and a DerSimonian-Laird random-effects model was employed. Using this method, the pooled prevalence of viral suppression after six months was 70% (95% CI: 62%-77%) among participants with baseline viral loads greater than 1,000 copies/mL and 82% (95% CI: 79%-85%) among all participants, regardless of initial viral load. The certainty of evidence for these outcomes was rated as low due to substantial heterogeneity and observational study designs.
These findings suggest short-term virological control; however, substantial heterogeneity limits the precision and generalizability of the pooled estimate. They fall short of the UNAIDS 95-95-95 objective of 95% viral suppression among people taking ART. The high heterogeneity limits the precision and generalizability of the pooled estimates.
The pooled results are generally consistent with evidence from multicountry African cohorts, such as a six-country research in Eastern and Southern Africa that found an overall viral suppression of about 93% among those treated with DTG in children and adolescents. 22 The slightly lower prevalence observed in our meta-analysis may be due to the inclusion of diverse studies with varying baseline viral load, ART experience, adherence support, and programmatic monitoring. However, these compressions should be interpreted cautiously, given the extreme heterogeneity observed in this analysis.
These findings are in line with a global systematic review across Europe, Africa, Asia, and the United States on the efficacy and safety of dolutegravir (DTG) in children and adolescents, which revealed viral suppression rates of more than 70% with DTG-based therapy at 12 months.
55
In comparison, higher suppression rates of 88-91% have been documented in studies from Europe and Thailand
56
The discrepancy could be explained by variations in virological suppression definitions, healthcare system capacity, and population factors. Europe and Thailand viral suppression is commonly reported using a stricter threshold of (<50 copies/mL), alongside well-established healthcare infrastructure, such as routine viral load monitoring, adherence support, and integrated pediatric HIV services. Furthermore, a significant proportion of participants had prior ART experience and were already virologically suppressed at DTG initiation, facilitating rapid suppression, as opposed to many African cohorts that include a higher proportion of ART-naive children or individuals with high baseline viral loads.
When compared with the ODYSSEY randomized controlled trial, which demonstrated that dolutegravir-based ART in children and adolescents resulted in rapid and durable viral suppression with lower rates of virological failure, 57 the pooled viral suppression estimates in this meta-analysis were slightly lower. This trial provide high-quality evidence under controlled conditions, including routine viral load suppression monitoring and structured adherence support, which are known to optimize treatment outcomes.
The observed discrepancy may therefore be attributed to differences in study design, as real-world settings included in this meta-analysis are less controlled and may involve variability in adherence, baseline clinical status, and healthcare system capacity. Despite these variations, both the current meta-analysis and the ODYSSEY trial support the effectiveness of dolutegravir-based ART in achieving high levels of viral suppression in children and adolescent populations. However, the certainty of evidence from this meta-analysis is limited and was rated as low due to substantial heterogeneity and the observational design of the included studies
In contrast, the pooled estimate of viral suppression in this review exceeds that reported in the global analysis. Multiregional evidence indicates that children and adolescents continue to lag behind adults in achieving viral suppression worldwide, even after adjusting for missing viral load data in long-term cohorts. A global analysis across 31 countries found that, after accounting for loss to follow-up and missing measurements, only 59-64% of children and adolescents achieved viral suppression less than 1000 copies/mL with three years of ART initiation. 12
This improvement is likely attributable to the rapid scale-up of dolutegravir-based antiretroviral therapy, which has substantially enhanced viral suppression among children and adolescents. DTG is a potent integrase strand transfer inhibitor with a high genetic barrier to resistance and a favorable safety and tolerability profile, features that support adherence and reduce the risk of treatment failure compared with older regimens based on non-nucleoside reverse transcriptase inhibitors or protease inhibitors. Emerging evidence indicates that DTG-based regimens achieve more rapid and durable viral suppression, including among individuals with high baseline viral loads or prior treatment exposure, thereby contributing to the higher short-term suppression rates reported in recent African programmatic data. Collectively, the potency, durability, and tolerability of DTG underpin its status as a preferred option in pediatric ART programs and its effectiveness in improving real-world treatment outcomes.22,55,58 However, observed pooled estimates vary considerably across settings.
In this meta-analysis, 77% (95% CI: 68-86%) of children and adolescents received dolutegravir-based ART, either as treatment-naїve therapy or following a switch from older regimens. This finding reflects substantial uptake of DTG in pediatric HIV care in the region, while also indicating persistent gaps in full implementation. The pooled estimate is broadly consistent with programmatic data from southern Mozambique, where 95.7% of children receiving ART were transitioned to DTG-based regimens during the national rollout, underscoring the prioritization of DTG over non-nucleoside reverse transcriptase inhibitor or protease inhibitor-based therapies. 23 The lower prevalence observed in the present analysis likely reflects the inclusion of multiple countries with heterogeneity in guideline adoptions, drug availability, and health system capacity. However, these estimates should be interpreted with caution due to substantial variability in implementation across included settings.
Globally, observational cohort studies beyond Africa, including the Icona cohort in Italy, have similarly reported high uptake of DTG among both ART-naïve and treatment-experienced individuals, with regimen switches frequently occurring in those with suboptimal response to previous regimens. 59 Additionally, the pooled prevalence of dolutegravir use in our meta-analysis (77%) is consistent with the global trend, although slightly lower than that reported in the ODYSSEY trial, a large randomized clinical study conducted across Africa, Europe, and Asia. In ODYSSEY, nearly all eligible children and adolescents were either initiated on or switched to dolutegravir-based ART, reflecting its favorable safety profile, high genetic barrier to resistance, and superior virological outcomes. 57 The lower prevalence observed in our meta-analysis likely reflects the difference between routine programmatic settings and the controlled trial environment, where regimen selection was protocol-driven and supported by frequent monitoring and structured follow-up, resulting in higher and more consistent dolutegravir uptake.
Similarly, when compared to large observational cohorts from Europe and Thailand, 56 the pooled prevalence in our meta-analysis is slightly lower, but it reflects the global trend of transitioning children and adolescents to dolutegravir-based ART. In those cohorts, DTG was extensively utilized as either naïve therapy or as a step up from previous regimens, according to newly released guidelines and great clinical confidence in its effectiveness. Many individuals had prior ART experience; DTG use generally exceeded 80-90% during follow-up. These differences could be due to health system infrastructure, guideline implementation, and drug availability, which are likely to have contributed to the rapid and more consistent adoption reported in Europe and Thailand, as opposed to the diverse routine programming settings covered in our research.
The observed variation in dolutegravir uptake rates between our pooled estimates and those reported from high-resource settings likely reflects differences in health system infrastructure, drug availability, clinical prescription practice, and the timing of guideline implementation. In countries such as Mozambique, rapid national rollouts and targeted uptake initiatives can accelerate DTG adoption, whereas the multicountry programmatic data included in our meta-analysis capture more heterogeneous implementation and access challenges.
These findings underscore the importance of contextual factors in shaping DTG uptake among children and adolescents living with HIV. They also underscore substantial variability in implementation across settings, which contributes to the high heterogeneity observed in pooled estimates. Overall, the certainty of evidence for uptake of dolutegravir-based ART was rated as very low due to extreme heterogeneity and variability in programmatic implementation across included studies.
Implication of the Study
This study demonstrates the significant potential of dolutegravir-based antiretroviral therapy to improve pediatric HIV care outcomes in Africa, while it also highlights persistent gaps in care that require targeted interventions.
For clinical practice and program implementations: the findings support the continued use of dolutegravir (DTG)-based ART as the preferred first-line regimen for HIV-infected children and adolescents in Africa. However, the observed gaps in viral suppression and uptake rates, particularly among those unsuppressed at baseline, indicate the need for increased clinical monitoring, structured adherence counseling, and prompt viral load testing to guarantee early detection and management of treatment failure.
For policymakers and guideline development, policymakers must address the large regional differences in DTG uptake highlighted by our findings, transitioning from universal guidelines to individualized implementation strategies. A specific focus is required to help children who were unsuppressed at baseline and had lower viral suppression (70%), through focused adherence programs and tighter monitoring within national recommendations.
Public health and epidemic control: although the pooled viral suppression rate of 82% (95% confidence interval: 79-85%) demonstrates DTG’s efficiency, it falls short of the UNAIDS target of 95%. This disparity, together with significant variation in outcomes among studies (I2 ≥ 98%), indicates systemic problems in healthcare delivery, patient retention, and viral load monitoring effectiveness. To accelerate epidemic control and reduce HIV transmission, public health strategies must prioritize structural strengthening of these health system components, particularly in regions with lower suppression rates, to ensure equitable and long-term treatment success for all children and adolescents. Overall, the certainty of evidence across outcomes ranged from low to very low due to substantial heterogeneity and the observational nature of the included studies. Therefore, future research
Limitation of the Study
This systematic review and meta-analysis are subject to several limitations that should be acknowledged when interpreting its findings. First, the included studies exhibited substantial heterogeneity, as reflected by high I2 values (ranging from 98.08 to 99.99%). While subgroup and meta regression analyses were performed, much of this variability remained unexplained, likely attributable to unmeasured contextual, methodological, and programmatic factors such as differences in adherence support structures, viral load monitoring protocols, healthcare infrastructure, and implementation timelines across diverse African settings.
Second, variability in the definition of viral load suppression across studies with thresholds ranging from <50copies/mL to<1000copies/mL may have influenced the pooled estimate and limited comparability. Notably, certain studies were excluded due to differing viral load cut-off points, which may have narrowed the scope of evidence considered.
Third, the analysis relied on aggregated study-level data rather than individual patient data, which constrained our ability to adjust for important clinical and socio-demographic covariates, including age subgroups, prior ART experience, adherence behaviors, and socioeconomic factors. Collectively, these limitations suggest caution in generalizing the pooled estimates and highlight the need for more harmonized research designs and reporting standards in future pediatric HIV studies.
Conclusion
This systematic review and meta-analysis provide a comprehensive synthesis of evidence on the impact of dolutegravir-based antiretroviral therapy on viral load suppression and uptake of dolutegravir-based ART regimen among children and adolescents living with HIV in Africa. The findings demonstrate that DTG-based ART is highly effective in pediatric HIV care, with a pooled viral load suppression of 70% among those unsuppressed at baseline and 82% overall after initiation of ART treatment, alongside a DTG uptake rate of 77%, reflecting considerable but incomplete adoption. Despite these promising outcomes, viral suppression and treatment coverage remain below UNAIDS 95-95-95 targets, indicating persistent gaps in treatment optimization. This observed heterogeneity across the studies suggests the influence of contextual and health system factors, reinforcing the need for strengthened, context-specific strategies to maximize DTG implementation and achieve equitable outcomes for children and adolescents living with HIV.
Supplemental Material
Supplemental Material - Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis
Supplemental Material for Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis by Desalegn Mitiku Kidie, Abraham Dessie Gessesse, Jenberu Mekurianew Kelkay, Tsegaamlak Kumelachew Derse, Addisu Simachew Asgai in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
Supplemental Material - Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis
Supplemental Material for Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis by Desalegn Mitiku Kidie, Abraham Dessie Gessesse, Jenberu Mekurianew Kelkay, Tsegaamlak Kumelachew Derse, Addisu Simachew Asgai in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
Supplemental Material - Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis
Supplemental Material for Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis by Desalegn Mitiku Kidie, Abraham Dessie Gessesse, Jenberu Mekurianew Kelkay, Tsegaamlak Kumelachew Derse, Addisu Simachew Asgai in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
Supplemental Material - Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis
Supplemental Material for Impact of Dolutegravir-Based Antiretroviral Therapy on Viral Load Suppression and Uptake of DTG-Based Regimen Among Pediatric HIV Patients in Africa: A Systematic Review and Meta-Analysis by Desalegn Mitiku Kidie, Abraham Dessie Gessesse, Jenberu Mekurianew Kelkay, Tsegaamlak Kumelachew Derse, Addisu Simachew Asgai in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgement
We would like to acknowledge all the primary authors of the studies included in this systematic review and meta-analysis for their valuable contribution to the evidence base used in this work.
Ethical Considerations
This study is a systematic review and meta-analysis based exclusively on previously published studies and publicly available data. Therefore, ethical approval and informed consent were not required.
Authors’ contribution
Funding
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of conflicting Interests
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.