
Abstract
Background:
Over 130,000 anterior cruciate ligament (ACL) reconstructions (ACLRs) are performed annually in the United States. Previous studies have shown that circumferential preconditioning reduces the diameter of fresh-frozen allografts, but no studies have described the effect in ACL autografts used during ACLR.
Purpose:
To characterize the changes in the hamstring autograft diameter as a result of preparatory circumferential preconditioning.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 135 patients with ACLR, with a median age of 15 years (interquartile range, 14-16 years; 50.4% boys), were identified in 2 pediatric hospitals. Three orthopaedic surgeons recorded hamstring autograft diameters at 2 time points during graft preparation. Hamstring tendons were prepared using a standardized procedure, tensioned to 15 to 20 lbs, and measured using cylindrical sizing guides. The graft was left with passive compression in the smallest initial rigid sizing guide for 10 minutes on both the tibial and femoral sides and then measured again immediately before implantation. Tunnels were drilled based on the second measurement of graft size. Comparisons were made between the graft diameter before and after circumferential preconditioning. A random-effects regression model and a linear regression model were performed to capture any unexplained variance on the linear predictor scale and determine correlations between demographics and graft characteristics.
Results:
The median initial diameter for both femoral and tibial sides was 9.5 mm. After longitudinal tension and circumferential preconditioning, the median autograft diameter of both sides decreased by 1 mm (P < .001) to 8.5 mm. In the random-effects model, decreased patient height was a significant predictor of greater reduction in graft diameter. Increased height was a significant predictor for greater initial graft diameter (average beta coefficient = 3.08; P < .01). No intraoperative complications were noted with implantation of the preconditioned grafts in smaller diameter tunnels.
Conclusion:
The median diameter of hamstring ACL autografts decreases by 1 mm after circumferential preconditioning within standard cylindrical sizing guides. This allowed for drilling of tunnels that were an average of 1 mm smaller without any noted intraoperative complications with graft insertion.
For young, active patients with anterior cruciate ligament (ACL) tears, ACL reconstruction (ACLR) remains the mainstay of treatment. 13,16 From an anatomic and biomechanical standpoint, reconstructing the ACL with an appropriately sized graft is important for re-creating native anatomy and providing a ligament of sufficient strength to resist physiological loads. Indeed, many authors have suggested that grafts that are too small may predispose patients to early failure. 4,13,14 While there are various methods of fixing grafts, 7,19 seating a graft in a bone tunnel is a near universal method for intra-articular ligamentous reconstruction. Placement of larger grafts requires larger bone tunnels and thus the removal of additional bone stock around the knee. There are multiple situations, such as a revision ACLR or ACLR in a very young or small patient, where large grafts may be advantageous to decrease the risk of reinjury, but large tunnels may pose a problem surgically because of the lack of available bone for tunnel creation and fixation.
While preimplantation tensioning is a well-accepted principle of graft preparation for reducing tissue creep within the graft and thus decreasing postoperative graft lengthening, 21 little research has been directed at determining how grafts are sized and prepared circumferentially. 3,5,9 Cruz et al 5 suggested that preconditioning a soft tissue graft with circumferential preconditioning may allow for implantation of a larger soft tissue graft in a smaller tunnel. The authors showed that applying a standard sizing block to a soft tissue graft decreased the ultimate size that they would have picked for graft implantation by almost 2 sizes (as measured in 0.5-mm increments). They claim that the circumferential preconditioning mimicked the passive compression that the grafts would experience in a bone tunnel and that circumferential preconditioning, like pretensioning, may help improve the match between the graft and tunnel. Circumferential preconditioning would also allow for the implantation of larger grafts into smaller tunnels, providing an advantage in certain surgical scenarios.
However, the study by Cruz et al 5 was performed with allograft tissue. Since allografts are subject to processing and freeze-thaw cycles, they may behave very differently than autograft tissue under circumferential preconditioning. In addition, the authors did not demonstrate that these circumferentially preconditioned grafts could indeed be implanted in the smaller-sized bone tunnels without swelling again during the implantation process. Thus, the purpose of this study was to investigate the change in size of hamstring autografts with circumferential preconditioning applied together with longitudinal tension during the preparatory phase of ACLR. We also sought to assess intraoperative complications associated with implanting circumferentially preconditioned grafts into smaller bone tunnels. We hypothesized that, like allograft tissue, hamstring autografts with both longitudinal tension and circumferential preconditioning would decrease in diameter and affect the performance of the surgical procedure.
Methods
Data Collection
A retrospective study was conducted at 2 pediatric hospitals after obtaining institutional review board approval at both institutions. A billing query was performed at each institution to identify patients aged 10 to 18 years who had undergone ACLR with an autologous hamstring tendon graft (Figure 1) by 1 of the 3 senior surgeons (J.T.R.L., T.J.G., K.M.D.) between May 2016 and May 2018. Patient demographic data were collected in addition to intraoperative details, such as graft diameters before and after any preconditioning, number of strands used, the occurrence of intraoperative complications, or the need to redrill tunnels because of inability to seat a graft in a tunnel.
Experimental protocol: schematic description.
Graft Preparation With an Additional Circumferential Preconditioning
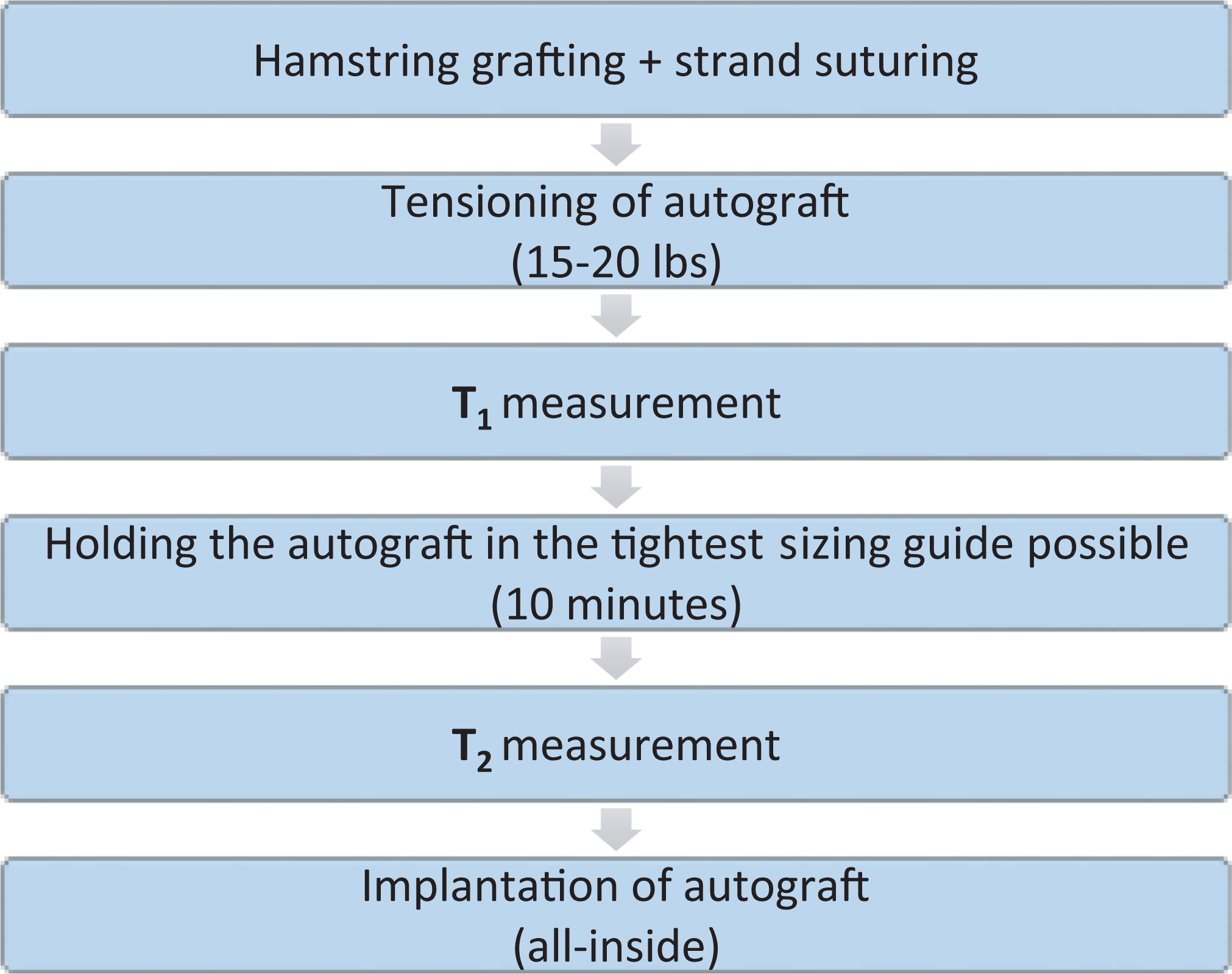
The 3 senior authors shared the same technique based on a clinical habit related to previous research and training. All ACLRs were performed with semitendinosus and gracilis tendon autografts using an all-inside technique. 10,11 Grafts were prepared, folded, and stitched using standard suturing techniques for performing an all-inside reconstruction. 6,8,18 The number of strands was recorded in each case, as it was tailored based on the characteristics of the tendon graft and the surgeon’s decision. The goal for graft preparation was to create a folded graft 70 to 75 mm in length, with a diameter of 8 to 10 mm. If the semitendinosus tendon was sufficient to generate an appropriately sized graft, the gracilis tendon was not utilized at all, giving a 4-stranded graft. Six- and 7-stranded grafts were mainly utilized in cases in which the gracilis tendon was not of adequate length. All autografts were tensioned to 15 to 20 lbs (∼89 N). The graft diameter was then measured and recorded using standard 7-cm cylindrical sizing guides in 0.5-mm increments (time point 1; T1). The size recorded was the smallest size socket that the graft could fit into at this stage of graft preparation. Next, the autograft was inserted with both ends of the graft into the tightest and smallest size cylindrical sizing guide for an additional 10 minutes (Figure 2). After this short period, the autografts were measured again (time point 2; T2), and the smallest diameter sizing guide that would accommodate the graft without excessive pressure was recorded. Grafts were then seated and secured with suspensory fixation into sockets drilled using the circumferentially preconditioned graft size (T2). A socket length of 20 to 25 mm was created on the femoral side while a 30- to 35-mm socket was created on the tibial side.
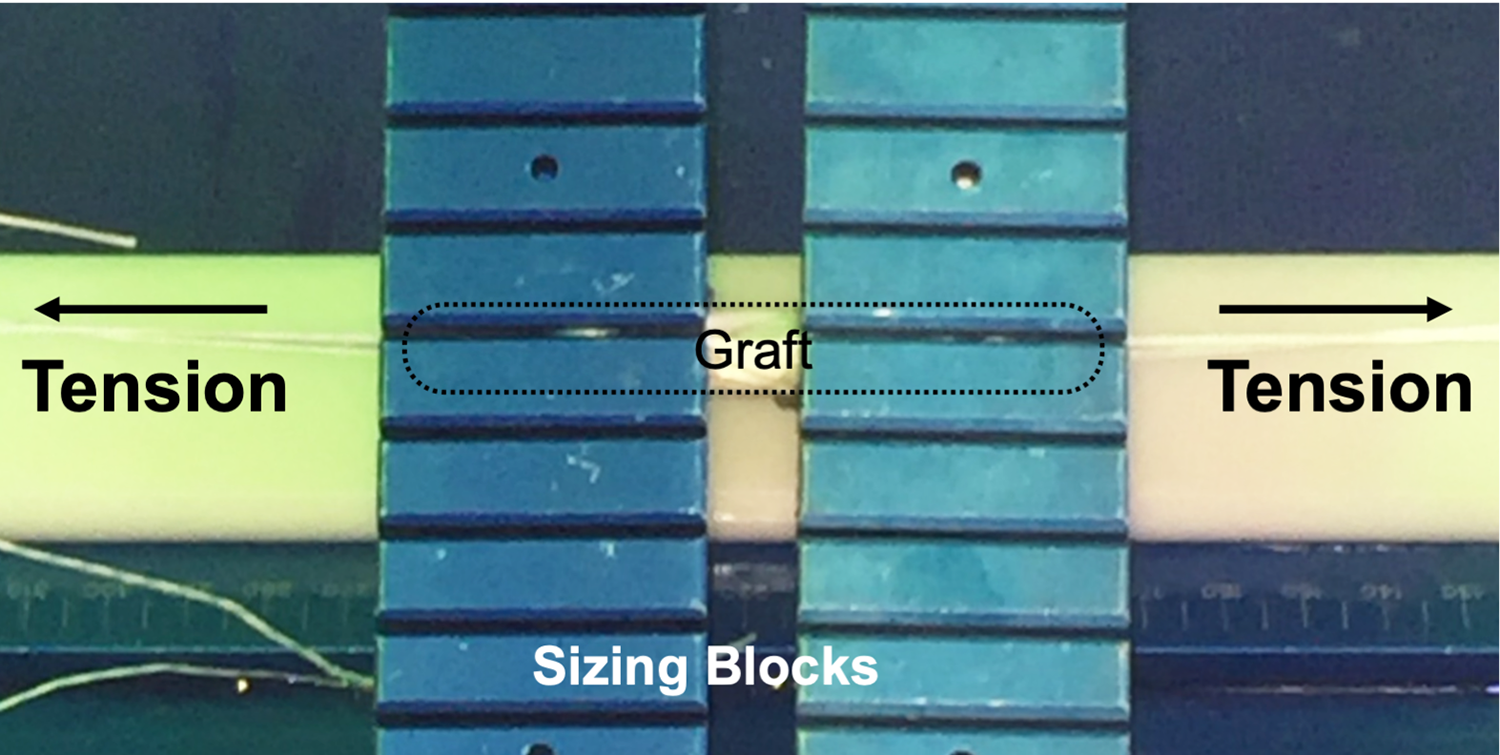
Clinical photograph of cylindrical preconditioning of a hamstring graft. The prepared hamstring graft was placed under tension at each end and then the smallest/tightest cylindrical sizing guide was placed on each end of the graft. The graft was left under a damp cloth for about 10 minutes and then resized before implantation.
Statistical Analysis
Demographic factors for the cohort were assessed using the Fisher exact test or the chi-square test. For continuous variables with non-normal distributions, the Mann-Whitney U or Kruskal-Wallis test was used. Comparisons were made between graft diameter at each time point. Because graft diameters were measured at 2 time points and on both sides of the graft (tibial side and femoral side), a random-effects regression model was performed to capture any unexplained variance on the linear predictor scale and determine correlations between demographics and graft characteristics. Statistics were calculated via SPSS Version 23.0 (IBM).
Results
The median age in the cohort was 15 years (interquartile range [IQR], 14-16 years), and 68 of the 135 (50.4%) patients were boys and 67 (49.6%) were girls. The median height was 167 cm (IQR, 162-173 cm), the median weight was 67.4 kg (IQR, 57.7-75.8 kg), and the median body mass index was 23.45 kg/m2 (IQR, 21.32-26.40 kg/m2).
The median initial (T1) diameter of both the femoral and tibial sides of the autografts during longitudinal tension was 9.5 mm (IQR, 9-10 mm). After adding circumferential preconditioning by placing the graft in the smallest sizing guide that it would fit in initially, the median final diameter (T2) of both graft sides was 8.5 mm (IQR, 8-9 mm). This 1-mm reduction in median graft diameter was noted (Figure 3) on both the tibial and femoral sides of the graft (P < .001 for both). Also, 39.5% decreased by 0.5 mm, 52.5% decreased by 1 mm, and 4% decreased by 1.5 mm or more. In the whole cohort, only 4% of cases showed no decrease in diameter between time points. There was no identified common feature that explained this small group of nonresponsive cases. Just over two-thirds (69%) of all autografts had the same tibial and femoral diameters after circumferential preconditioning (at T2) before implantation.

Box-and-whisker plot of graft diameters before and after circumferential preconditioning. The median graft diameter was significantly decreased after 10 minutes of longitudinal tension and circumferential preconditioning for both the tibial and femoral sides (P < .001 for both).
A regression analysis was performed to identify whether any associated demographic or physiological patient characteristics may have contributed to the change in size of these grafts with circumferential preconditioning. In the random-effects model, patient height was the only factor significantly associated with change in graft diameter (P < .01), with shorter patient height predicting a greater decrease in graft diameter. In addition, patient height was also the only significant predictor of initial graft diameter, with taller patients having larger graft diameters (average beta coefficient 3.08; P < .01). The most common graft configuration was an 8-strand construct (87.4%). While a lower strand number (ie, 4-strand grafts) was associated with taller patients (P < .01), strand number was not associated with change in graft size after the circumferential preconditioning.
To assess for the ability to insert circumferentially preconditioned grafts into smaller tunnels, we assessed for intraoperative complications related to graft insertion. No intraoperative complications were noted with implantation of these grafts in smaller diameter tunnels.
Discussion
Over 130,000 ACLRs are performed annually in the United States, and rates of ACL injury and subsequent reconstruction seem to be increasing in both adult and pediatric populations. 1–2,20 Much attention has been focused on the type of tissue used for the reconstruction (ie, autograft vs allograft and patellar tendon vs hamstring) as well as on the anatomic localization and fixation used for those grafts. However, the literature describing graft-preparation techniques is sparse. While it is a well-accepted principle that grafts should be preconditioned under tension to prevent graft elongation after implantation, little work has been performed to assess the cross-sectional area of a graft once implanted into a bone tunnel. The primary goal of this study was to investigate the diameter change of a hamstring autograft using a novel method of graft preparation that includes longitudinal tension with circumferential preconditioning for ACLR. The main finding in this study is that circumferential preconditioning of hamstring autografts in the tightest sizing guide that the soft tissue graft will fit into initially decreases the median graft diameters by 1 mm, allowing for easy implantation into bone tunnels drilled on average 1 mm smaller.
Establishing an optimized fit between the graft and bone tunnel is a central concern in ACLR, as proper sizing of grafts in a bone socket may lead to better graft integration and reduced tunnel widening. Cruz et al 5 recently evaluated the impact of circumferential compression in addition to tension on fresh-frozen hamstring allografts. Those authors demonstrated a mean decrease of 0.9 mm in the assessed diameter of the graft with circumferential compression. Our results confirm that the autograft hamstring tissue can be preconditioned to about the same degree as the allograft tissue.
Ease of graft implantation into the bone tunnel is also a primary concern to many surgeons, as the inability to fully seat a graft into a tunnel can lead to significant surgical delays or issues with graft tensioning. For fixation techniques that utilize interference fit of an additional device alongside the graft in the tunnel, graft-tunnel mismatch may not be as critical. However, for suspensory fixation techniques, a tight, line-to-line fit is important. While Cruz et al 5 did not implant their circumferential preconditioned grafts, they did note that the compressed nature of the graft persisted even when tension and compression were removed for some time. Since the reduction in graft diameter remained even after compression was released, they argued that the size of a nonconditioned graft would likely decrease and persist in a bone tunnel once implanted. Therefore, circumferential preconditioning may help improve bone-tunnel match. However, because they never implanted their grafts, it is not clear whether the passively compressed grafts would expand back to their preconditioned size and prevent implantation in tunnels drilled corresponding to the smaller compressed diameter. The results presented here support the notion that grafts show a persistent reduction in diameter after circumferential preconditioning and can be easily implanted in smaller bone tunnels.
The clinical implications of circumferential preconditioning extend beyond the potential of reducing graft-tunnel mismatch. For ACLRs performed with soft tissue grafts, it is now clear that the size of the graft affects the risk of retear, with grafts <7.5 to 8 mm showing increased risks of early failure. 4,13 However, placement of larger grafts comes with the price of increased bone loss as a result of drilling larger diameter tunnels. In certain clinical situations, such as revision cases or pediatric cases, large bone tunnels may not be viable because of anatomical considerations. 12 As such, strategies to place larger soft tissue grafts with less bone loss may be important. Meyer et al 15 have shown that applying circumferential compression on a graft can reduce the graft diameter by extrusion of water without decreasing the structural properties of the graft. These data suggest that circumferential preconditioning allows for implantation of a graft with greater structural content in smaller bony tunnels. Additionally, a smaller tunnel with a tighter graft-tunnel match might result in less risk to an open physis.
During the circumferential preconditioning of the graft, no excessive force was applied to the graft other than the force applied by a standard sizing block during routine graft preparation. Since a prior in vitro study noted that graft preparation and sizing have good intraobserver reliability, it is unlikely that there was a significant difference in the sizing block used at this phase of the study among the providers. 5 Also, the force applied by this initial sizing block only provides a comparable passive compression with what would be applied to the graft in its bony tunnel after implantation. Thus, it is reasonable to conclude that the forces applied during the preconditioning phase of this study constituted loads that would not damage the graft beyond what it would experience once implanted.
When determining significant predictors of change in graft diameter, we were not surprised that height was significantly associated. In our cohort, all cases with low strand number (n = 4) were associated with taller (>175 cm) patients (P < .01). The study by Nuelle et al 17 on hamstring autograft characteristics based on different anthropometric measurements showed a moderately strong correlation between an increase in the patient’s height with tendon diameter (R2 = 0.60). This explains why taller patients, with larger harvested grafts, may need fewer folds to achieve an appropriate graft diameter before implantation. While graft compression has been shown to remove water from the grafts, 15 it likely also decreases dead space within the grafts. Multistrand grafts may have more dead space, explaining why shorter patients with thinner autografts would have an increased strand number and exhibit a more substantial decrease in graft size after circumferential preconditioning. These conclusions are consistent with our findings that increased initial graft diameter is associated with taller patients as well as with lesser reduction in graft diameter after preconditioning. These findings may help guide a surgeon’s process of graft preparation and bony tunnel size estimation in patients of various heights.
This study is not without its limitations. The study is retrospective, and the data were obtained from surgical notes. Although the findings may be theoretically reproduced in other soft tissue autographs (quadriceps tendon, etc), this study is related only to hamstring autographs. While standardized prospective data-collection procedures or even a randomized protocol may have been better, the relevant data points for this study were reliably and routinely recorded in the medical record. Another limitation in this study is that we cannot necessarily comment on the long-term clinical utility or safety of the procedure. In this study, we feel that we have demonstrated that this new method of preconditioning does not lead to any intraoperative issues with implantation. However, the next step will be to investigate clinical outcomes of such preconditioned autografts to determine whether tunnel widening, postoperative functional results, or retear rates are affected. With 3 surgeons performing the procedures, there may have been slight variations because of personal bias, experience in harvesting, and preparing the autografts, or practice in determining graft diameter. However, these differences are likely negligible because the protocol for sizing grafts is very uniform and has been shown to be extremely uniform among surgeons. 5 In addition, the fact that a similar size reduction was seen between 3 different surgeons at 2 different institutions, possibly using slightly different sizing guides or graft preparation techniques, supports the generalizability of the effect seen in this study. The methods employed here represent a “real-world” clinical application for graft preparation and do not appear to affect the ease of graft implantation. Finally, in this study, the number of 8-strand grafts was substantially larger than 4-, 6-, or 7-strand grafts. While this may lower the accuracy of our correlational analyses, as it relates to graft diameter change based on strand number, it does not diminish the clinical significance of our main finding that almost all grafts show a reduction in diameter as a result of circumferential preconditioning.
Conclusion
The median diameter of hamstring ACL autografts decreases by 1 mm compared with baseline after circumferential preconditioning using a standard cylindrical sizing guide to a tensioned graft. Clinically, this may allow drilling of tunnels that are an average of 1 mm smaller without compromising ease of graft insertion. Using circumferential preconditioning during graft preparation in pediatric, double-bundle, or revision ACLR may reduce unnecessary bone removal and achieve a better fit between the graft and the bone tunnels. The technique utilized is considered safe, as no intraoperative complications were noted relative to graft implantation.
Footnotes
Final revision submitted January 29, 2021; accepted February 25, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.M.D. has received grant support from Arthrex. T.J.G. has received research support from Vericel, Arthrex, and AlloSource and educational support from Liberty Surgical and is a paid associated editor for The American Journal of Sports Medicine. J.T.R.L. has received educational support from Arthrex and Liberty Surgical and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Children’s Hospital of Philadelphia (protocol No. 15-012614).