
Abstract
Background:
The Ankle Ligament Reconstruction-Return to Sport After Injury (ALR-RSI) scale can be utilized for assessing patients who have previously sustained lateral ankle ligament injury before returning to sport. Given its original development for use in different languages, it is essential to translate and validate this scale for application to the Chinese population.
Purposes:
To translate and culturally adapt the ALR-RSI scale into a Chinese version and assess its reliability and validity.
Study Design:
Cohort study (Diagnosis); Level of evidence, 2.
Methods:
The procedure of translation and cross-cultural adaptation was performed following the recommended guidelines and the Chinese version of ALR-RSI (ALR-RSI-CHN) was conducted in patients with lateral ankle ligament surgery. Feasibility was assessed by floor/ceiling effects. Reliability was assessed by using Cronbach α as a measure to analyze internal consistency, while the intraclass correlation coefficient was utilized to examine test-retest reliability. Validity was assessed by using Spearman coefficients to analyze the correlations between ALR-RSI-CHN, the Karlsson scale, and the American Orthopaedic Foot and Ankle Society (AOFAS) scale.
Results:
A total of 66 participants were included. The ALR-RSI-CHN scale showed good feasibility with no floor/ceiling effects. The internal consistency of the scale was adequate with a Cronbach α of 0.93, and test-retest reliability was excellent with an interclass correlation coefficient of 0.97 (95% CI, 0.92-0.99). The ALR-RSI-CHN scale demonstrated moderate correlation with the Karlsson scale (r = 0.48 [
Conclusion:
The study demonstrated that the ALR-RSI-CHN scale had satisfactory psychometric properties, rendering it a feasible, reliable, and valid instrument for evaluating patients who have lateral ligament surgery in China.
Keywords
The ankle joint, as a crucial weightbearing joint in the human body, contacts with the ground directly and endures substantial mechanical stress during walking and running, making it highly susceptible to sports-related injuries. Ankle sprain is the most common ankle injury, and studies have shown that the prevalence of ankle sprain in the general population is 11.88%. 12 Ankle sprains are closely related to sports, accounting for 16% to 40% of all sports-related injuries, 28 especially in sports such as basketball and football.10,22 Among all ankle sprains, 85% involve the lateral ankle ligament, 18 often leading to ligament tearing or complete rupture.
The typical symptoms of lateral ankle ligament injury are pain, swelling, and ecchymosis. In most cases, lateral ankle ligament injury can be recovered completely with conservative treatment and rehabilitation training. 29 However, 40% of patients will have recurrent ankle sprains if not managed properly. 11 Further development may lead to chronic ankle instability. 16 For young people, and those who have sport demands, surgery is a better choice, and systematic rehabilitation training after surgery can help them recover to the preinjury sport levels. The modified Broström-Gould procedure, including ligament repair and reconstruction, remains the gold standard for management. 13 It has been reported that about 9% of patients show severe ankle stiffness after surgery, 5% to 12% of patients still have ankle instability, 32 and about 25% of patients are unable to return to sports. 21
Although relatively perfect surgical procedures and complete rehabilitation training can achieve recovery of physiological function, many patients still cannot return to sports. This is because the process of returning to sports involves different stages, requiring patients to be prepared both physically and psychologically. 9 In the process of returning to sports, most patients will have negative emotions, lack of confidence, or fear reinjury. These psychological factors or obstacles could affect the patient's ability to return to sports. 27 If these psychological problems can be controlled, the poor condition of the patient during the process will be improved. Therefore, it is important to assess the psychological factors of the patient before returning to sports.
Several scales, including the Tampa Kinesiophobia Scale and the Knee Self-Efficacy Scale, have been used to assess the role of psychological factors in patients returning to sports after other injuries.14,37 Particularly in patients with anterior cruciate ligament reconstruction, Webster et al 39 designed a 12-item scale (Anterior Cruciate Ligament-Return to Sport After Injury [ACL-RSI]) to assess the psychological readiness of patients returning to sports. This widely used scale can assess the confidence and psychological status of patients in sport performance after anterior cruciate ligament reconstruction. Chen et al 7 translated the ACL-RSI scale into Chinese and demonstrated that it is a valid, reliable, and feasible tool for assessing psychological factors when returning to sport. As an analogy, Sigonney et al 34 replaced the “knee” in the ACL-RSI scale with the “ankle” and designed the Ankle Ligament Reconstruction-Return to Sport After Injury (ALR-RSI) scale to assess the psychological status of patients who returned to sport after lateral ankle ligament reconstruction. It has been proved that the scale is valid and repeatable. Researchers from other countries have made cross-cultural adaptations to the ALR-RSI scale and verified its reliability and validity.1,25,26
Therefore, the aims of this study were to translate and culturally adapt the ALR-RSI scale for patients with lateral ankle ligament surgery in China and subsequently use the Chinese version of the scale to assess its feasibility, reliability, and validity among postsurgical patients with lateral ankle ligament injury. We hypothesized that the ALR-RSI scale would be feasible, reliable, and valid in assessing the psychological status of Chinese patients returning to sports after lateral ankle ligament surgery.
Methods
Study Design
This study was conducted in our hospital in Beijing, China, and was reviewed and approved by the Medical Ethics Committee of Chinese PLA General Hospital (approval number: 2023KY151-KS001).
After signing an informed consent form, all enrolled participants independently completed the Chinese version of the ALR-RSI scale (ALR-RSI-CHN). They then completed an additional and standardized questionnaire with demographic data (age, sex, height, weight, visual analog scale for pain, etc) and 2 valid and reliable functional scales: the Karlsson scale 30 and the American Orthopaedic Foot and Ankle Society (AOFAS) scale. 19 The recording of completion time for the scales and noting any challenges faced while responding were aimed at assessing reliability. A total of 40 randomly selected participants recompleted the ALR-RSI-CHN scale 1 week after the initial completion.
Participants
Between October 7 and October 31, 2023, participants were recruited from Beijing, China, via telephone, posters, and social media. Inclusion criteria were the following: (1) 18 to 50 years old, (2) first unilateral lateral ankle ligament surgery, (3) 3 months to 2 years after surgery, (4) regular physical activity before injury, and (5) Chinese as their native language. Exclusion criteria were the following: (1) ankle fracture, (2) ankle cartilage injury, (3) other ligament injuries of the ankle, or (4) other joint injuries.
According to Hair, 15 the sample-to-variable ratio suggests a minimum observation-to-variable ratio of 5:1. This scale contains 12 items, so at least 60 participants were required.
Translation and Cultural Adaptation
The procedure followed international guidelines for the cross-cultural adaptation of self-administered questionnaires (Figure 1). 4
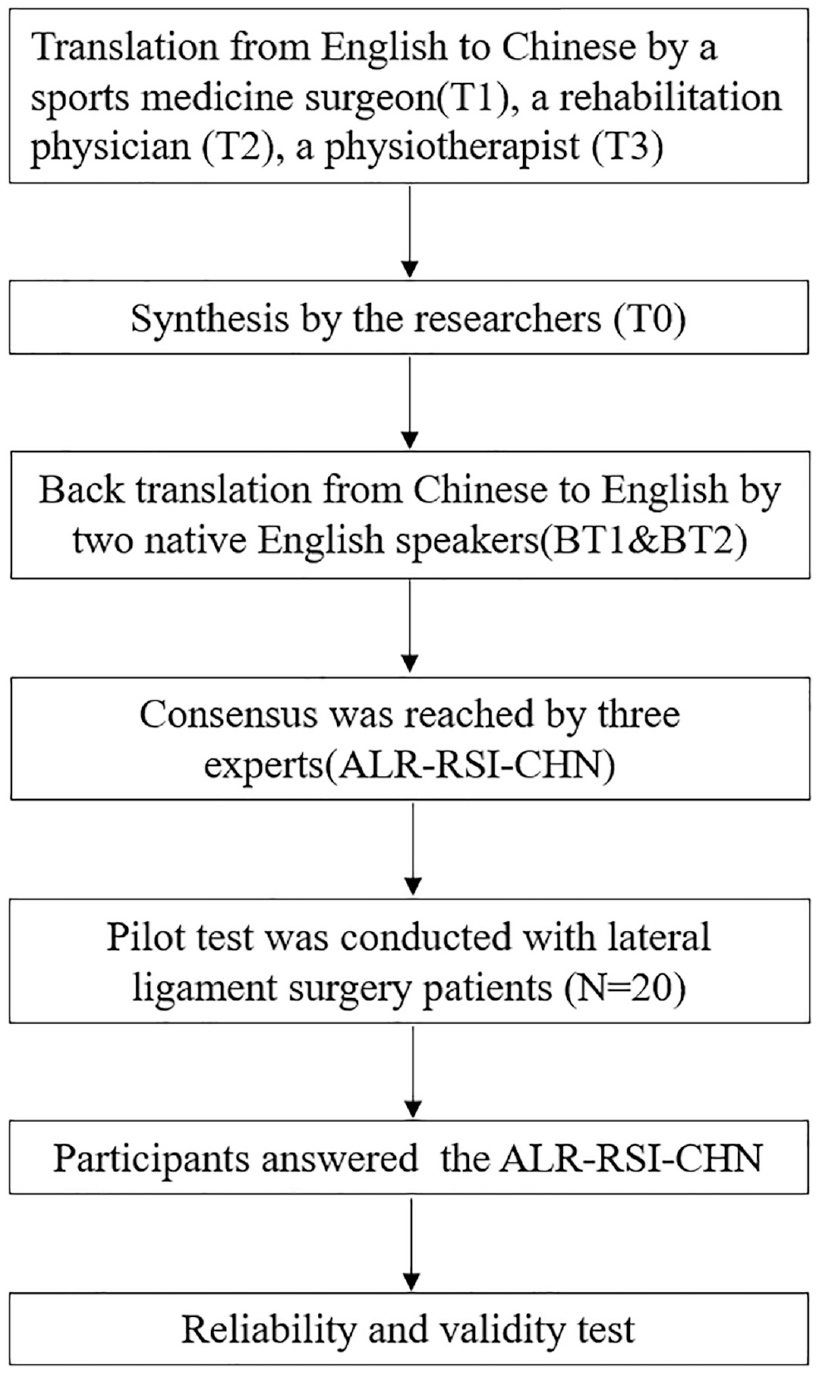
Flowchart of the cross-cultural adaptation, reliability, and validity tests of the Chinese version of ALR-RSI (ALR-RSI-CHN). ALR-RSI, Ankle Ligament Reconstruction-Return to Sport After Injury; T0, Translation 0; T1, Translation 1; T2, Translation 2; T3, Translation 3; BT1, Back Translation 1; BT2, Back Translation 2.
First, the scale was translated from English into Chinese by a sports medicine surgeon, a rehabilitation physician (X.S), and a physiotherapist (Y.X.) who were native Chinese speakers and proficient in English. These 3 Chinese versions of the ALR-RSI scale were named Translation 1, Translation 2, and Translation 3, respectively. Second, the researchers in this study synthesized the translated scales, fully discussed and resolved the differences, and selected a scale named Translation 0 (T0) after reaching a consensus. Then, scale T0 was back translated into English by 2 native English speakers with no knowledge of the original scale and no medical background. These 2 English versions were named Back Translation 1 and Back Translation 2, respectively. Next, an expert committee, consisting of 3 experts in related fields but unrelated to this study, reviewed and evaluated the original scale and all the translated scales, confirming that the translated scales could accurately express the intention of the original scale and that the wording was correct. Thus, the ALR-RSI-CHN scale was produced. Finally, we did a pilot test. A total of 20 patients with lateral ankle ligament surgery were recruited randomly and provided with the ALR-RSI-CHN scale. All participants completed the scale and were asked whether they had difficulties in answering questions, making comments or suggestions so that we could refine the scale as needed. Any problem raised throughout the entire process was also documented and addressed.
Assessments
ALR-RSI Scale
The ALR-RSI scale is adapted from the ACL-RSI scale. The ALR-RSI scale contains 12 items that are considered to obtain psychological readiness before returning to sports after injury, including emotions (5 items), confidence in performance (5 items), and risk evaluation (2 items). 34 Each item is scored from 0 to 10 points with an 11-point Likert scale, and the total score of the scale is calculated by adding the scores of the 12 items and then divided by 1.2 to get the percentage. A score of 0 represents the lowest psychological readiness and a score of 100 represents the highest.
Karlsson Scale
The Karlsson scale comprises 8 items with a total of 100 points, wherein higher scores indicate better functional capacity. This scale enables the evaluation of pain, swelling, instability, stiffness, stair climbing, running, work activities, and support.
AOFAS Scale
The AOFAS scale consists of 3 subscales: pain, function, and alignment. These subscales include a total of 9 items. Pain is assessed using 1 item with a maximum score of 40 points, indicating no pain. Function is assessed using 7 items with a maximum score of 50 points, representing complete functionality. Alignment is assessed using 1 item with a maximum score of 10 points, indicating optimal alignment. The highest possible score on this scale is 100 points, which indicates no indications or limitations in the patient's condition are present.
Data collection and analysis were conducted by an independent person who was not affiliated with the trial and unaware of our study's purpose and design.
Statistical Analysis
Statistical analyses were carried out using Statistical Package for the Social Sciences (SPSS) Version 27.0 (IBM Corp).
Quantitative variables were described using means and standard deviations. For qualitative variables, absolute frequencies (n) and relative frequencies (%) were used. P < .05 was considered significant.
Floor/ceiling effects could be used to describe the content feasibility. According to previous research, 24 if >15% of the participants achieve the lowest or highest attainable scores, it becomes challenging to detect any deterioration or improvement in their performance using the specific instrument. This phenomenon is referred to as floor/ceiling effects and suggests that the content feasibility of the instrument is limited.
Internal consistency indicates the ability of an instrument to involve interrelated items. 2 Cronbach α can be used to assess the internal consistency, and internal consistency is considered to be adequate if the Cronbach α value is <0.7. 38 The item-total correlation (ITC) helps determine the extent to which individual items on the instrument are related to the overall score, and an ITC value >0.3 was considered acceptable, indicating that the items captured the intended construct effectively. The test-retest reliability reflected the ability of the scores of an instrument to be reproducible over time when it is used on the same patient whose condition has not changed.2,5 The intraclass correlation coefficient (ICC) was used to assess the test-retest reliability, and reproducibility was considered “excellent” if the ICC value was >0.9, “good” if between 0.75 and 0.9, “moderate” if between 0.5 and 0.75, and “poor” if <0.5. 20 The interval period between repeated tests was 1 to 2 weeks. 35
The validity of the scale was tested according to the international Consensus-based Standards for the selection of health status Measurement Instruments guidelines. 23 A sample size of 66 produced a 2-sided 95% CI with a width <0.24 when the estimate of Spearman rank correlation was >0.75. The Spearman coefficients were used to assess the correlations between ALR-RSI-CHN and the Karlsson/AOFAS scales. As with results of previous papers, the Spearman coefficient was considered “strong” if the coefficient value was >0.5, “moderate” if between 0.3 and 0.5, and “weak” if between 0.1 and 0.3.
Results
A total of 66 patients participated in the investigation and were included in the study, each of whom had undergone lateral ankle ligament arthroscopic surgery. There were no missing items for any of the participants and all scales were valid. The participants were aged between 21 and 48 years, with a mean age of 28.00 years (SD, 5.90 years). All participants competed at the same level of sport before injury. Of these 66 patients, 29 (43.94%) were injured on the left side and 37 (56.06%) were injured on the right side. Regarding sport recovery, 26 (39.39%) participants stated that they were able to return to their preinjury level of sport, while 40 (60.61%) participants stated that they were not. Other sociodemographic variables and the main scale scores are summarized in Table 1.
Demographic Characteristics of Study Participants a

Data are presented as mean ± SD unless otherwise indicated. ALR-RSI-CHN, Chinese version of the Ankle Ligament Reconstruction-Return to Sport After Injury scale; AOFAS, American Orthopaedic Foot and Ankle Society; BMI, body mass index; VAS, visual analog scale.
Translation and Cross-Cultural Adaptation
The Chinese translation and the English back translation did not cause any significant grammar or wording problems. During the translation stage, the 3 translators translated “are you confident” in items 1, 4, 5, 8, and 11 into “do you have confidence” in Chinese to align with Chinese grammar and expression. In the expert committee synthesis stage, “holding up” in item 8 was suggested to be translated into “have the ability to stabilize” to express the meaning of the original text better. In the pilot test, we kept the answers in the form of checkboxes based on the pilot participants’ comments.
Feasibility
All items of the ACL-RSI-CHN were included, and no missing answers were reported. The mean scale completion time was 2.9 minutes. The floor effect, corresponding to the percentage of patients that answered with a score of 0 for each question, ranged between 1.5% and 4.5%. Meanwhile, the ceiling effect corresponding to the percentage of patients that answered with a score of 10 for each question ranged between 1.5% and 9.1%.
Reliability
Internal Consistency
The internal consistency was assessed by employing Cronbach α, and the ITC coefficient was also computed. The Cronbach α value for the whole scale was 0.93, indicating that the ACL-RSI-CHN had adequate internal consistency. Based on the analysis, the ITC coefficients for the instrument ranged between 0.47 and 0.85, with a mean correlation coefficient of 0.72. Moreover, it confirmed that all items met the criterion of having an ITC coefficient >0.30. During the sensitivity analysis of the items, the Cronbach α coefficient was calculated for each item when it was deleted from the instrument. The results showed that for all items, the Cronbach α coefficients ranged between 0.79 and 0.80, with minimal variation (Table 2).
Internal Consistency of the ACL-RSI-CHN a

ALR-RSI-CHN, Chinese version of the Ankle Ligament Reconstruction-Return to Sport After Injury scale.
Test-Retest Reliability
The reliability of the ALR-RSI-CHN scale was assessed by calculating the ICC denoted as ρ. In this study, the ICC value was 0.97 (95% CI, 0.92-0.99), showing a reproducibility that was considered “excellent.” Meanwhile, the mean ALR-RSI-CHN scale was 60.65 (range, 23.08-75.15) when it was completed for the first time and the value was 59.29 (range, 22.70-69.46) for the second time (Table 3).
ICC of the ACL-RSI-CHN a
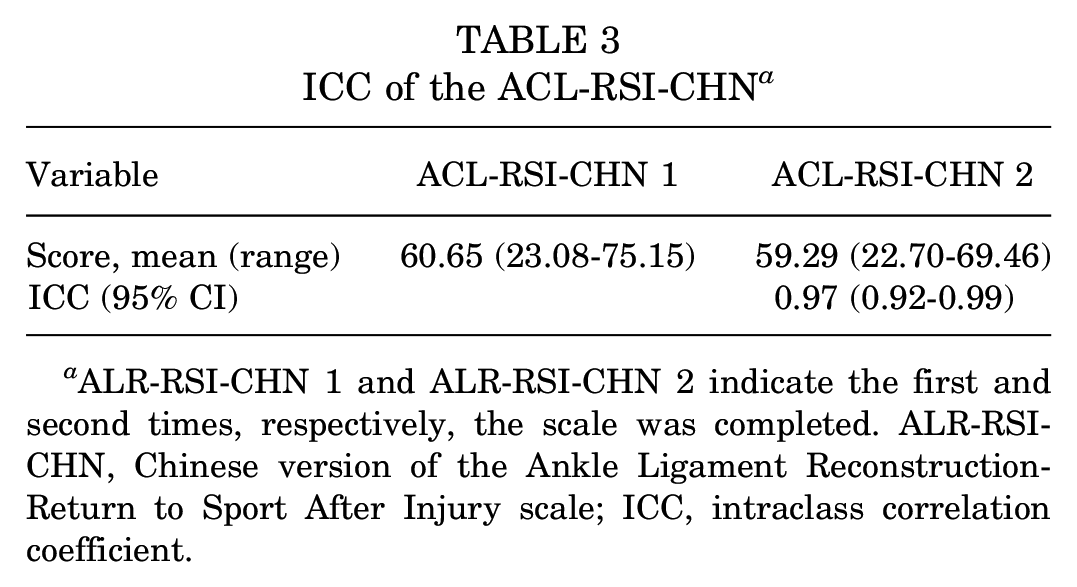
ALR-RSI-CHN 1 and ALR-RSI-CHN 2 indicate the first and second times, respectively, the scale was completed. ALR-RSI-CHN, Chinese version of the Ankle Ligament Reconstruction-Return to Sport After Injury scale; ICC, intraclass correlation coefficient.
Validity
The ALR-RSI-CHN scale demonstrated a good positive correlation with the reference scale that was utilized. The Spearman correlation coefficient between the ALR-RSI-CHN scale and the Karlsson scale was found to be 0.48, showing a moderate correlation. The Spearman correlation coefficient between the ALR-RSI-CHN scale and the AOFAS scale was determined to be 0.55, showing a strong correlation (Table 4).
Correlation Between the ALR-RSI-CHN and the Karlsson/AOFAS a
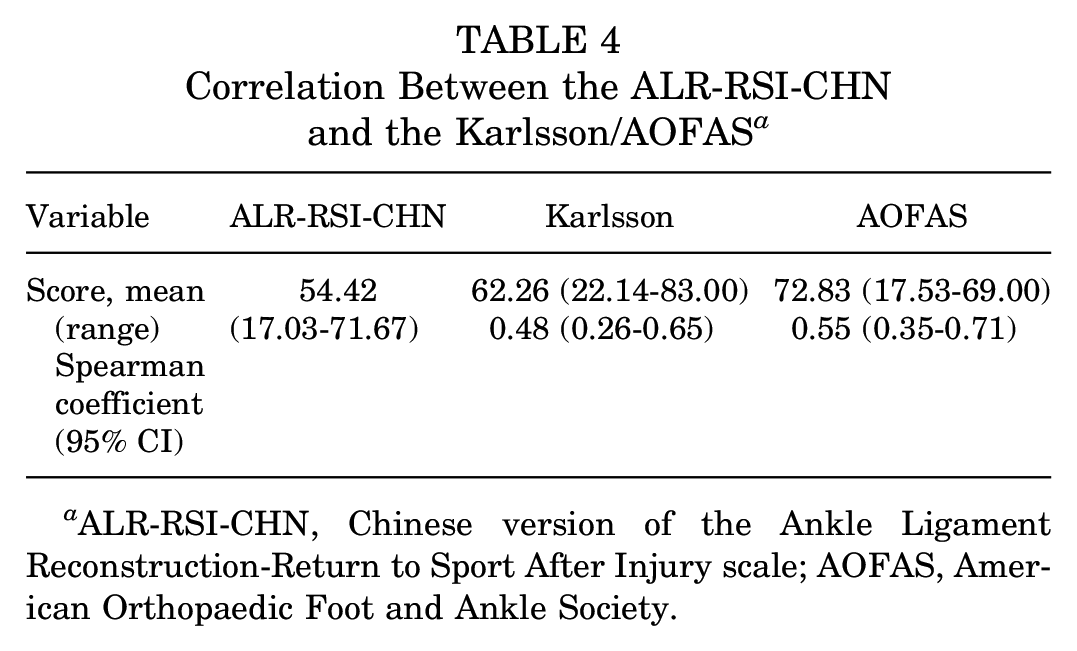
ALR-RSI-CHN, Chinese version of the Ankle Ligament Reconstruction-Return to Sport After Injury scale; AOFAS, American Orthopaedic Foot and Ankle Society.
The ALR-RSI-CHN scores among the return to sports subgroup showed discriminant validity. The mean ALR-RSI-CHN score was found to be significantly greater in patients who resumed sports activity compared with those who did not return to sports. The mean ALR-RSI-CHN score for patients who resumed sports activity was 53.60 (range, 44.50-62.69), while it was 42.25 (range, 35.51-49.00) for patients who did not continue with sports (P < .05) (Table 5).
ALR-RSI-CHN Scores in RTS and No-RTS Groups a
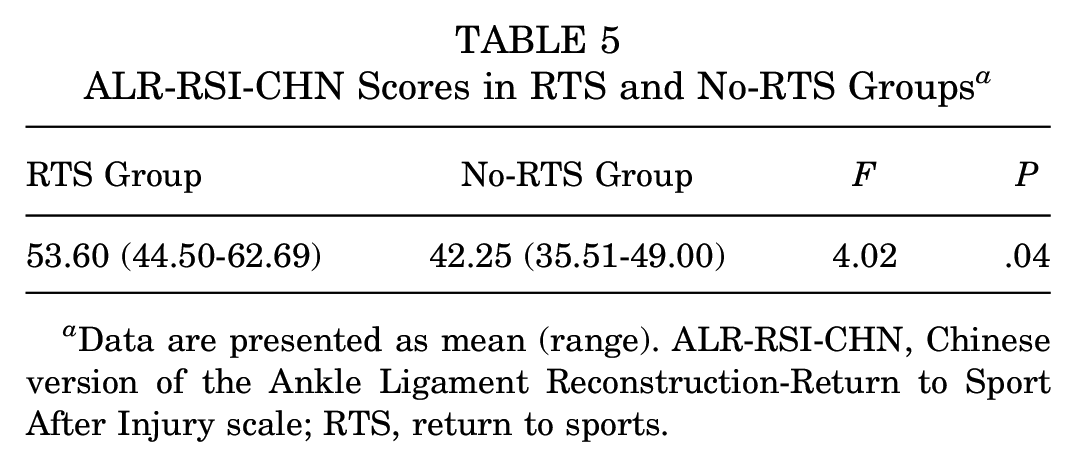
Data are presented as mean (range). ALR-RSI-CHN, Chinese version of the Ankle Ligament Reconstruction-Return to Sport After Injury scale; RTS, return to sports.
Discussion
Based on our results, we found that the ALR-RSI-CHN scale had good feasibility, reliability, and validity in assessing the psychological status of Chinese patients returning to sports after lateral ankle ligament surgery.
Rating scales play a crucial role in assessing the severity of patients’ functional abilities and quality of life and can also offer a standardized tool with which to compare treatment outcomes. The main objective of the present study was to translate and adapt the ALR-RSI scale into a Chinese version and assess its psychometric properties in patients who speak Chinese with lateral ankle ligament surgery. The findings of our study provide support for the reliability and validity of the ALR-RSI-CHN. This instrument can be utilized in clinical and research settings to gather valuable information regarding the impact of lateral ankle ligament surgery on patients’ functional abilities and quality of life.
A systematic review conducted by Hunt et al 17 highlighted the importance of standardized, valid, and reproducible tools for reporting return to sports outcomes. This emphasis on reliable measurement tools was echoed by Clanton et al, 8 who specifically emphasized the significance of subjective data in assessing a person's ability to return to sports after an injury. In this regard, the ALR-RSI scale enables a comprehensive evaluation that aids in making safe and informed decisions regarding return to sports. The ACL-RSI scale serves as a prime example of the importance of incorporating psychological evaluations in the process of determining an athlete's readiness to return to sports after injury. Extensive research has demonstrated a strong and significant correlation between the ACL-RSI scale, a psychological assessment tool, and successful return to sports. 31
The mentioned Cronbach α value of 0.93 for the ACL-RSI-CHN scale is similar to that reported for the French version, which had a Cronbach α value of 0.94, 26 indicating a high level of internal reliability. The present study reported good test-retest reliability for the ACL-RSI-CHN scale, and the ICC values in the present study were slightly greater than those reported in the French study. 26 This suggests that the scale consistently and accurately measures the psychological aspects related to resuming sports activities after such surgery. On the other hand, in the mentioned study conducted in Spain, 25 there was no specific mention of the ICC or test-retest reliability.
As for the validity, the ACL-RSI-CHN scale was compared with the Karlsson and AOFAS scales. The Karlsson scale demonstrated satisfactory sensitivity in assessing the functional ability of patients with ankle sprains. 36 The ALR-RSI-CHN scale had a moderate correlation with Karlsson scale. This may be due to the fact that the Karlsson scale contains some physiological factors, such as pain, swelling, numbness, etc, which are somewhat different from the simple psychological assessment of this scale. The AOFAS scale was chosen because it remains the most used scale for orthopaedic surgeons worldwide to assess patients with ankle or hindfoot injuries. This scale is used to assess ankle function and pain, which are 2 key points for patients who are willing to return to their previous level of sport after ankle ligament injury.6,33 The ALR-RSI-CHN scale had a strong correlation with AOFAS scale, indicating that the ALR-RSI-CHN scale can effectively evaluate the Chinese patients’ psychologic status before they wish to return to sports after lateral ankle ligament surgery. Moreover, this scale also showed significant differences between those who can return to sports and those who cannot, which shows it can effectively distinguish psychological factors in the target population well.
The ALR-RSI scale is designed to evaluate the psychological impact of returning to sports after ankle ligament surgery, and this study confirmed the application value of ACL-RSI in the Chinese population. The decision to allow an athlete to return to sports after an injury involves multiple factors, including physical recovery, functional abilities, and psychological readiness, still with no consensus. 3 Our study provides a credible and reliable psychological assessment tool for relevant personnel, including sports medicine surgeons, rehabilitation physicians, physiotherapists, and researchers, to determine whether patients are psychologically ready to return to sports. The results obtained in our study are also consistent with other results found in previous research.1,25,26 Thus, a more comprehensive assessment can be carried out to help patients return to sports more safely and reduce the incidence of injury and reinjury during sports activity.
There are several limitations in the present study. First, the ALR-RSI scale was not designed specifically but was adapted from the ACL-RSI scale, which has been shown to translate and transpose to other joints and other diseases. Second, the sample size of this study was limited for practical reasons. Therefore, future studies should be designed with a larger sample size and a certain period of follow-up, which will help better analyze the changes in patients who have not returned to the same level of sports.
Conclusion
Our study demonstrated that the ALR-RSI-CHN scale had satisfactory psychometric properties, rendering it a feasible, reliable, and valid instrument for evaluating patients who have lateral ligament surgery in China.
Footnotes
Final revision submitted February 20, 2024; accepted March 18, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from Beijing Nova Program (20230484400). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chinese People’s Liberation Army General Hospital (ref No. 2023KY151-KS001).