Abstract
Objectives:
Sleep disturbance is a significant symptom associated with both rotator cuff tears and arthroscopic rotator cuff repair. Melatonin has been shown to be safe and effective in managing multiple sleep disorders, including secondary sleep disorders, with relatively minor adverse effects, and lack of addictive potential. The purpose of this study was to investigate the effects of oral melatonin on postoperative sleep quality after arthroscopic rotator cuff repair (aRCR).
Methods:
This was a prospective, randomized, clinical trial evaluating patients undergoing arthroscopic rotator cuff repair. Consecutive patients undergoing arthroscopic rotator cuff repair for rotator cuff tear were included. Exclusion criteria included history of alcohol abuse, current antidepressant or sedative use, revision rotator cuff repair, severe glenohumeral arthritis, and concurrent adhesive capsulitis. Patients were randomly assigned in a 1:1 ratio to one of two groups: 5 mg dose of melatonin 1 hour before bedtime, or standard sleep hygiene (6+ hours per night, avoid caffeine and naps in the evening). Patients in the melatonin group took their assigned melatonin dose for 6 weeks beginning the day of surgery. Patient reported outcome assessments included the Pittsburgh Sleep Quality Index (PSQI), the American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES), Single Assessment Numerical Evaluation (SANE), and pain medication logs. Outcome measures were collected preoperatively, as well as at 2 weeks, 6 weeks, 3 months, 4 months, and 6 months post-operatively. Numeric variables were analyzed using paired and unpaired t-tests, with significance set at p<0.05.
Results:
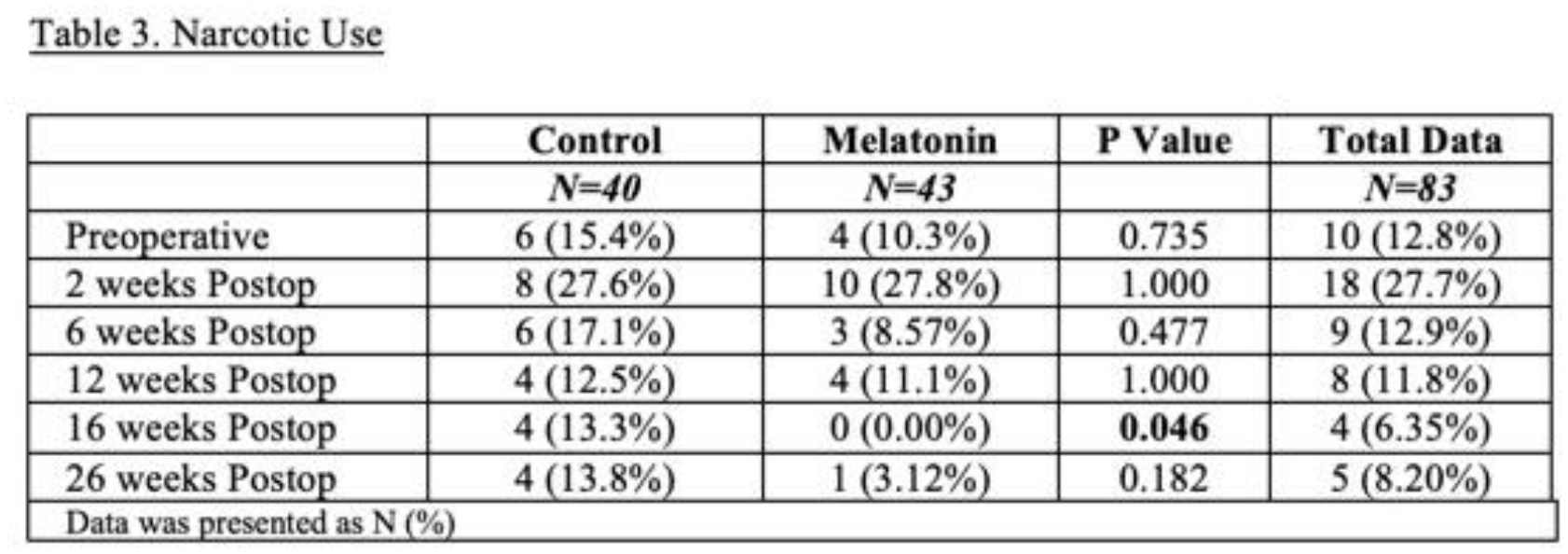
Eighty-three patients were included for final analysis (40 control, 43 melatonin). Patient demographics such as age, sex, race, BMI, and laterality did not differ significantly between groups (p≥0.05). Preoperative ASES, SANE, and PSQI scores did not differ between groups (p≥0.055). PSQI scores were significantly lower (better quality sleep) in the melatonin group at the 6-week postoperative period (p=0.036). There was a positive correlation between how patients rated the intensity of their pain and the PSQI at the 6-week assessment (0.566). The PSQI question regarding sleep quality was found to be significantly greater in the melatonin group at the 3-month, 4 month, and 6 month postoperative time point (p=0.015, p=0.041, and p=0.05, respectively). SANE scores in the melatonin group were significantly lower (p=0.011), then higher (p=0.017) at the 6- week and 6-month time point, respectively. ASES scores were significantly greater in the melatonin group at 4 and 6 months (p=0.022 and p=0.020). Patients who were randomized into the melatonin group were found to use significantly less narcotic medication at the 4 month postoperative time point (p=0.046). There was no difference in complication rates between groups.
Conclusions:
Melatonin use after aRCR led to improved sleep quality in the early postoperative period and improved functional outcomes and decreased narcotic use in the later postoperative period. Based on this investigation, we recommend the use of melatonin postoperatively after aRCR to reduce sleep disturbance in the early postoperative period and potentially help with longer term functional outcome.