
Abstract
Background:
Recent studies suggest that increased tibiofemoral (TF) rotation elevates the risk of anterior cruciate ligament (ACL) reconstruction failure, with a proposed threshold of 4.5° of internal rotation (IR). However, the role of TF rotation in primary ACL injury remains unclear.
Purpose/Hypothesis:
The purpose was to evaluate whether axial TF malalignment, as reflected by the TF axial rotation angle and tibial tubercle–trochlear groove (TTTG) distance, is associated with primary ACL injury in professional soccer players. It was hypothesized that increased internal TF rotation is associated with ACL injury.
Study Design:
Cross-sectional study.
Methods:
A retrospective review was performed on a consecutive series of professional soccer players who underwent ACL reconstruction between January 2012 and August 2024. Inclusion criteria were primary ACL injury and availability of preinjury magnetic resonance imaging (MRI). Cases were matched 2:1 by age with controls, who were players who underwent meniscal surgery during the same period and had no history of ACL injury. The groups were compared in terms of age, TTTG distance, medial and lateral posterior tibial slope, resting knee flexion, and axial TF rotation during MRI acquisition. All MRI scans were independently reviewed by 2 musculoskeletal radiologists.
Results:
Twenty-four professional soccer players (mean ± SD age, 25.3 ± 4.2 years) with MRI and arthroscopy-confirmed primary ACL injuries were included. The control group consisted of 48 players (mean age, 23.6 ± 3.3 years) who had intact ACLs confirmed via MRI and arthroscopy and underwent meniscal surgery. No statistically significant differences were observed between groups for age, medial and lateral posterior tibial slope, knee flexion during MRI, or axial TF rotation (IR, 6.7°± 5.8° vs 4.3°± 5.9°; all, P > .05). The prevalence of resting axial TF rotation ≥4.5° of IR was also not significantly different between groups (70.8% vs 66.7%; P = .721). The TTTG distance was significantly smaller in players with ACL injuries (8.9 ± 3.4 mm vs 10.9 ± 4.2 mm; P = .050) but did not reach statistical significance when adjusted for knee flexion (odds ratio, 1.15; 95% CI, 1.00-1.32; P = .059). There was no difference in resting axial TF rotation and TTTG between pre- and postinjury MRI scans in players with ACL injury.
Conclusion:
In this cohort of professional soccer players, TF axial rotation was not significantly associated with primary ACL injury. Although not statistically significant, the association between a smaller TTTG distance and ACL injury may reflect an underlying anatomic predisposition related to IR malalignment. Notably, neither resting axial TF rotation nor TTTG distance differed before and after injury, indicating that these features are likely inherent.
Anterior cruciate ligament (ACL) injuries are among the most common knee injuries in physically active individuals, with an incidence ranging from 60 to 78 per 100,000 people.30,32,35 Athletes involved in sports such as American football, soccer, and basketball are particularly at risk.5,13 In elite athletes, an ACL tear has serious implications, as surgical reconstruction is frequently followed by a decline in performance and, in many cases, premature termination of the athletic career.3,4
Numerous risk factors have been identified that contribute to ACL injuries, including neuromuscular and neurocognitive deficits, genetic predisposition, biological sex, environmental factors, and structural anatomy.38,39 Of the anatomic factors, a steep posterior tibial slope (PTS), a narrowed intercondylar notch, and malalignment in the coronal plane have been consistently associated with increased stress on the ACL and a higher risk of rupture.27,38,44
More recently, however, research has focused on axial alignment, particularly tibiofemoral (TF) rotation, as a potential biomechanical contributor to ACL injury and graft failure after reconstruction.23,24,46 Increased internal rotation (IR) of the tibia in relation to the femur has been shown to lengthen the ACL, 17 which may place greater strain on the ligament and predispose it to injury or overload.26,31 While previous studies have shown that ACL rupture is frequently accompanied by anterior and rotational subluxation of the tibia relative to the femur,28,42,45,49 more recent reports suggest that patients with postinjury increased axial TF IR are more likely to demonstrate injuries to the anterolateral structures and exhibit a higher-grade pivot shift during clinical examination. 23 The same authors reported that patients undergoing ACL reconstruction with a preoperative TF rotation angle >4.5° of IR had an almost 7-times higher risk of graft failure. 24
Supporting these findings, a biomechanical study showed that combined injuries of the ACL and anterolateral structures result in increased IR. This abnormal rotation persists after isolated ACL reconstruction but can be restored to native levels when the anterolateral structures are also reconstructed, 8 which has been validated by studies demonstrating the critical role of anterolateral structures in maintaining normal knee kinematics.12,19,20,22,29,48 Similar observations have been reported for a reduced tibial tubercle–trochlear groove (TTTG) distance having an association with ACL injury.7,25,33,36 These findings raise an important question: is increased TF IR malalignment an independent risk factor for primary ACL injury, or does it simply represent a surrogate marker of unresolved anterolateral subluxation after concomitant anterolateral injury, which, if left untreated, contributes to the increased risk of ACL graft failure reported in recent literature?
Therefore, the purpose of this study was to evaluate whether TF axial malalignment, specifically the preinjury TF rotation angle, and TTTG distance are associated with primary ACL injury in professional soccer players. It was hypothesized that increased TF IR is associated with ACL injury in professional soccer players.
Methods
This study was conducted in accordance with UK Health Research Authority standards, with institutional approval obtained prior to its initiation. 15
Patient Selection
A retrospective cohort analysis was performed involving all professional soccer players who underwent primary ACL reconstruction with hamstring or patellar tendon autografts between January 2012 and August 2024 by the senior author (A.W.). Eligible players were aged ≥17 years, as this is the minimum age to sign a professional contract, and had pre– and post–ACL injury magnetic resonance imaging (MRI) available for review. Players were excluded if they had previous ACL injury. This selection process yielded a cohort composed entirely of professional soccer players with primary ACL injury who had available MRI of the knee before and after the ACL injury. This cohort was matched 2:1 by age with controls, who were professional soccer players who underwent meniscal surgery during the same period with available MRI of the index knee and had no history of ACL injury until the end of the study period. Players with isolated lateral meniscal injuries were selected as the control group because these athletes frequently undergo preoperative MRI and have arthroscopically confirmed intact ACLs. In addition, lateral meniscal injuries were chosen to minimize potential confounding related to medial meniscal ramp lesions, which have been suggested to influence TF rotational stability.11,40 This approach allowed comparison with a large, relatively homogeneous cohort of professional soccer players, thereby reducing variability within the control group. Demographic details such as age and sex and meniscal interventions were retrieved from operative and clinical records.
All MRI scans were independently assessed by 2 fellowship-trained musculoskeletal radiologists. The assessments included medial and lateral PTS, TTTG distance, and axial TF rotation. Knee flexion angle at the time of imaging was also measured given its known influence on TTTG and TF axial rotation values.1,21
Medial and Lateral PTS
PTS was evaluated by the method described by Hudek et al. 18 On a midsagittal MRI slice that included the posterior cruciate ligament and intercondylar eminence, 2 concentric circles were drawn within the tibial metaphysis to define the tibial axis. Medial and lateral PTS was measured as the acute angle between a line perpendicular to this axis and a tangential line along the tibial plateau (Figure 1).
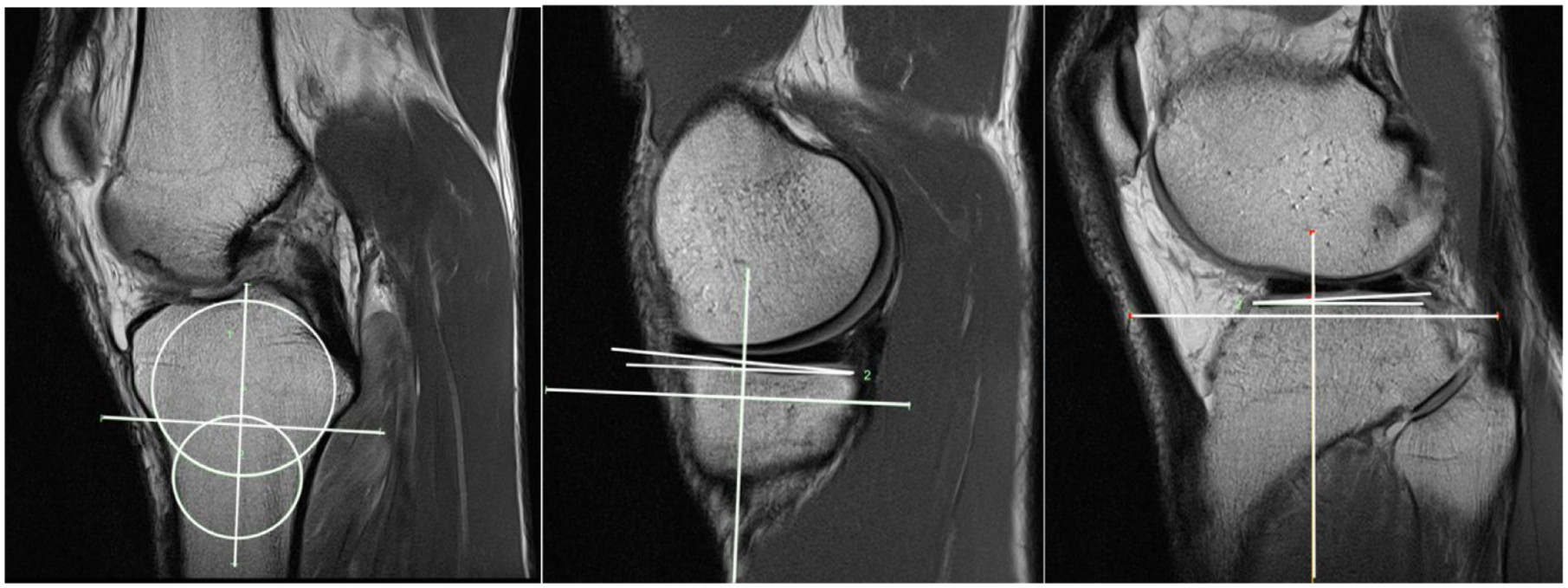
Measurement of medial and lateral posterior tibial slope on sagittal knee magnetic resonance imaging. The tibial longitudinal axis is defined by 2 diaphyseal cortical circles, and the posterior tibial slope is calculated as the angle between this axis and a line tangential to the tibial plateau, subtracted from 90°.
Knee Flexion Angle
Flexion angles were determined by sagittal MRI slices. The best profiles of the anterior femoral and tibial cortices were selected, and lines were drawn along these cortices. The angle formed between these lines represented the knee flexion angle, as described in prior literature (Figure 2).21,41

Measurement of knee flexion angle on sagittal magnetic resonance imaging, defined as the angle between the anterior femoral (1) and tibial (2) cortices, subtracted from 180°.
Tibial Tubercle–Trochlear Groove
The TTTG distance was measured on axial images. It was defined as the perpendicular distance from the anterior aspect of the tibial tuberosity to the deepest point of the trochlear groove, relative to a posterior condylar reference line (Figure 3).14,37
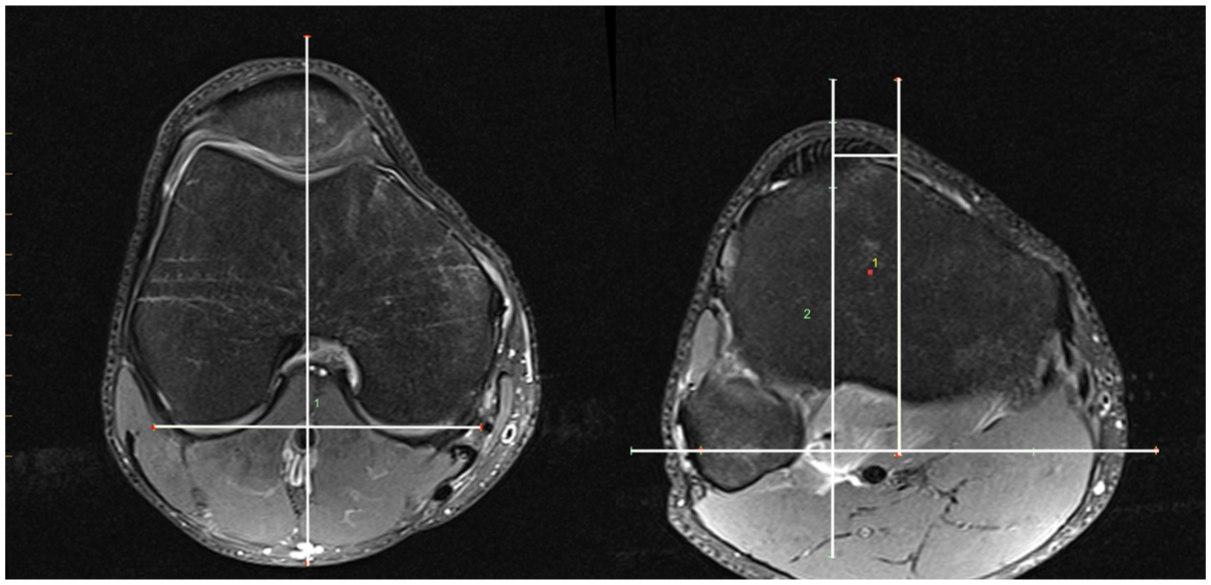
Measurement of the tibial tubercle–trochlear groove distance on axial magnetic resonance imaging, defined as the perpendicular distance between parallel lines through the trochlear groove (1) and the tibial tubercle (2).
TF Rotation
TF rotation was calculated on axial MRI sequences by measuring the angle between lines tangential to the posterior femoral condyles and the posterior tibial plateau just distal to the articular surface. 43 Positive values indicated IR of the proximal tibia relative to the distal femur (Figure 4). 9
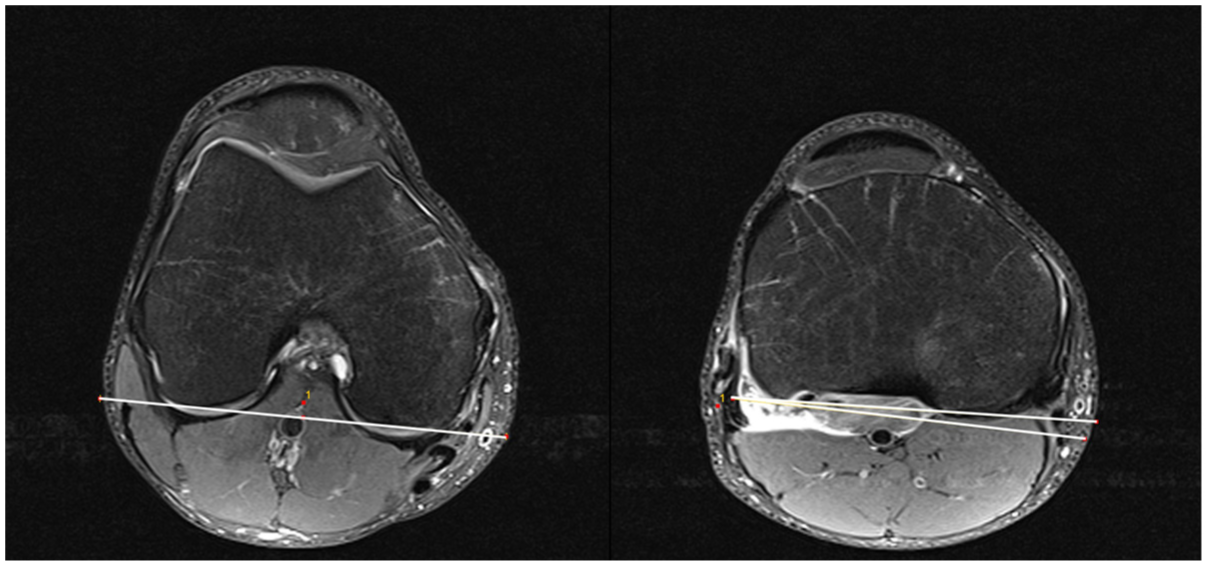
Measurement of the tibiofemoral rotation angle on axial magnetic resonance imaging, defined as the angle between the posterior femoral condylar axis and the posterior tibial condylar axis.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics. Normality of distribution was tested with the Shapiro-Wilk test. Hence, continuous variables were compared by the Mann-Whitney U test or independent t test. A chi-square or Fisher exact test was utilized to compare categorical data between groups. A paired t test was utilized to assess the change in TF rotation and TTTG from pre– to post–ACL injury. Intraclass correlation coefficients with 95% confidence intervals were calculated for PTS, knee flexion, TTTG, and TF rotation. Lastly, multivariate logistic regression analysis was performed to calculate the odds ratio for the risk of ACL injury based on TF axial alignment.
An a priori power analysis indicated that a sample size of 72 (allocation 2:1) was needed to achieve 80% power to detect a significant difference in TF rotation (2.8°) between groups, based on recently published data showing a significant influence of TF rotation on the risk of ACL graft failure. 24
All statistical analyses were performed in SPSS for Mac (IBM). Significance was set at P≤ .05.
Results
A total of 274 professional soccer players underwent ACLR during the study period. Of these, 24 players (mean ± SD age, 25.3 ± 4.2 years) had pre– and post–ACL injury MRI scans available and were included in the analysis. These were matched to 48 players (mean age, 23.6 ± 3.3 years) who underwent isolated lateral meniscal surgery with an MRI- and arthroscopy-confirmed intact ACL during the study period. None of these players had a history of ACL injury until the end of the study period.
Intraclass correlation coefficients for interobserver reliability for all measurements were excellent and ranged from 0.968 to 0.993 (Table 1). Players with ACL injury showed no statistically significant difference in PTS, knee flexion angle, and TF rotation measurements as compared with players without a history of ACL injury (P > .05). Meanwhile, TTTG was significantly smaller in players with ACL injury (P = .050) (Table 2). The incidence of TF IR ≥4.5° was also not significantly different between groups (70.8% vs 66.7%; P = .721). When adjusting for knee flexion, a smaller preinjury TTTG distance did not reach statistical significance as an independent risk factor for ACL injury (odds ratio, 1.15; 95% CI, 1.00-1.32; P = .059). There was no difference in TF rotation (6.7°± 5.8° vs 6.5°± 5.5°; P = .798) and TTTG (8.9°± 3.4° vs 8.8°± 3.5°; P = .798) between pre- and postinjury MRI scans in players with ACL injury.
Intraclass Correlation Coefficients of Interobserver Reliability a

ACL, anterior cruciate ligament; ICC, intraclass correlation coefficient; TTTG, tibial tubercle–trochlear groove.
Comparison Between Players With and Without ACL Injury a
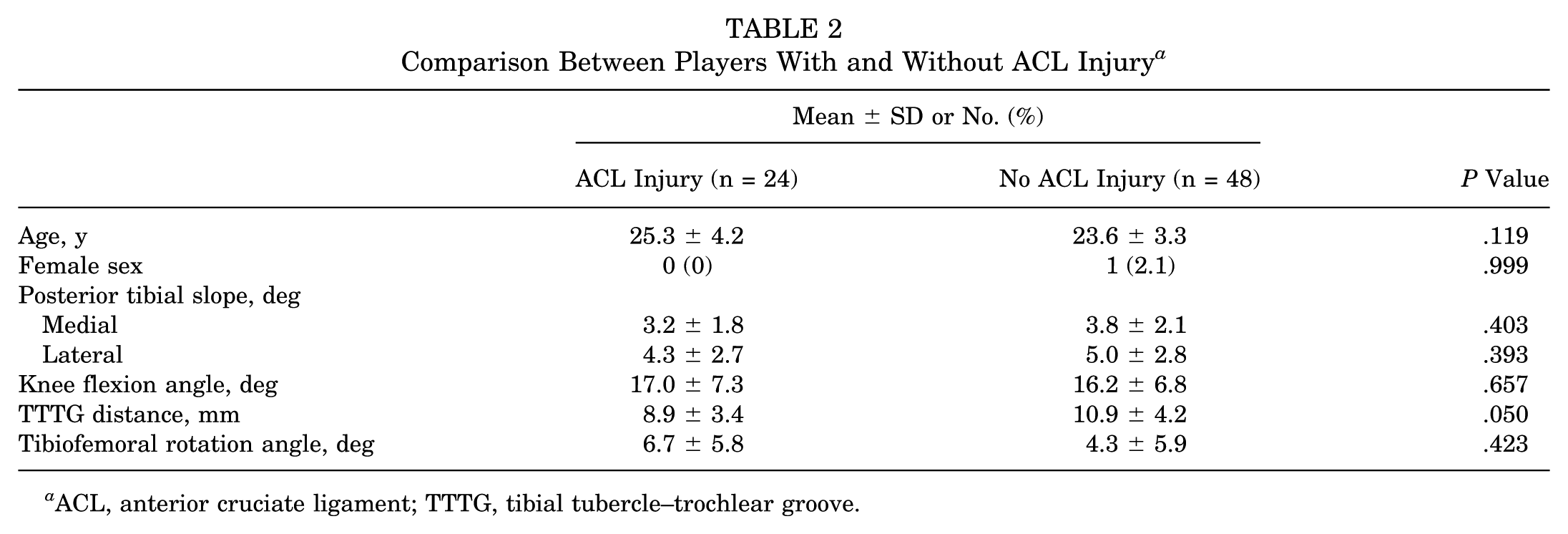
ACL, anterior cruciate ligament; TTTG, tibial tubercle–trochlear groove.
Discussion
The key finding of the current study is that increased TF axial IR was not significantly associated with primary ACL injury in professional soccer players. While prior investigations have implicated elevated TF rotation in graft failure after ACL reconstruction, our data do not support its role as a risk factor for primary ACL rupture. Interestingly, athletes with ACL injuries demonstrated a significantly reduced TTTG distance, which did not reach statistical significance when adjusted for knee flexion, suggesting a potential anatomic predisposition that may still reflect IR malalignment. Furthermore, neither TF rotation nor TTTG distance changed significantly after ACL injury when compared with preinjury measurements, indicating that these parameters are likely inherent rather than injury induced.
Previous literature has suggested that increased TF IR rotation may play a role in ACL injury mechanisms.34,45,49 Leite et al 24 reported that patients with TF IR >4.5° had a markedly higher risk of ACL graft failure, with a 7-fold increase observed in a matched analysis of revision versus intact reconstructions. A subsequent study from the same group linked increased TF IR to anterolateral structure injury and higher pivot-shift grades, raising uncertainty whether increased rotation represents a preinjury predisposition or a consequence of ACL rupture. 23 This raises the question of whether increased TF IR predisposes individuals to ACL injury, particularly involving the anterolateral structures, or whether TF rotation increases as a consequence of ACL rupture, given that the ACL restricts internal tibial rotation, which may be amplified by concomitant injury to the anterolateral structures. 2 The current study did not identify a statistically significant difference in TF axial rotation on ACL-intact MRI scans between players who subsequently sustained an ACL injury and those who did not, despite a between-group difference of 2.4°, which is comparable to the 2.8° difference reported by Leite et al. This discrepancy may be attributable to inherent selection bias in professional soccer, where individuals with anatomic characteristics that predispose to injury are less likely to reach or remain at the highest levels of competition. Indeed, an ACL rupture in an established senior first team soccer player is relatively rare. 10 Moreover, the present study included a smaller sample size (N = 72) as compared with the 302 patients analyzed in the Leite et al study, which may have limited our ability to detect subtle associations despite sufficient statistical power. Furthermore, no differences were observed in TTTG distance or TF rotation between pre- and postinjury MRI, suggesting that ACL rupture does not substantially alter these parameters at rest. This finding supports the interpretation that TTTG distance and resting TF rotational alignment are largely inherent to the individual and that postinjury MRI measurements in this cohort likely reflect baseline alignment rather than injury-induced changes.
However, the current study found an association between a smaller TTTG distance and ACL injury, which may reflect increased tibial IR relative to the femur rather than pure medial translation of the tibia, given the constraints imposed by articular geometry and the medial meniscus. 47 This interpretation is supported by prior work demonstrating that TTTG is primarily influenced by TF rotational alignment and the position of the tibial tubercle. 16 This finding is interesting as it, at first glance, contradicts previous studies that have associated larger TTTG distances with ACL injuries, with and without concomitant anterolateral injury.7,25,33,36 Polat et al 33 compared the TTTG distance in patients with intact ACLs and torn ACLs with and without concomitant anterolateral injury, reporting increasing TTTG distances from intact to isolated and combined ACL injuries. This finding seems counterintuitive as ACL and anterolateral injuries result in anterolateral instability, which would increase tibial IR and thus decrease TTTG. 2 However, the authors hypothesized that combined injury may result in greater overall rotational instability knee, which could paradoxically lead to an increased TTTG distance during MRI assessment. The current study differs from that of Polat et al in that TTTG distance was measured exclusively in ACL-intact knees, of which 24 later sustained an ACL injury. This design enabled assessment of TTTG in knees with preserved rotational stabilizers, including the ACL and anterolateral structures. While prior studies have suggested that increased TTTG may serve as a surrogate marker for rotational instability in ACL-deficient knees,7,25,33,36 the present findings indicate that a smaller TTTG distance is potentially associated with future ACL injury. Notably, none of the referenced studies accounted for knee flexion during MRI acquisition, a key limitation, as extension induces tibial external rotation via the screw-home mechanism and has been shown to significantly affect TTTG measurements.1,6 The smaller TTTG in players with subsequent ACL injury may therefore reflect an underlying IR malalignment that increases strain on the ACL and predisposes to injury.17,26,31
Importantly, this study not only evaluated the role of TF rotation and TTTG distance in the risk of primary ACL injury among professional soccer players but also examined whether ACL injury itself alters these parameters. The results showed no significant difference in TF rotation or TTTG distance between pre- and postinjury imaging within the ACL injury cohort, suggesting that ACL rupture does not influence these measurements. This contrasts with previous studies that reported increased axial malalignment following ACL injury.7,23,25,33,36 The present study is novel in assessing the same knee on MRI in an ACL-intact and ACL-deficient state, thus allowing for direct comparison within 1 individual while controlling for knee flexion. Nevertheless, on first glance the current findings seem to contradict prior biomechanical studies showing increased tibial IR following ACL rupture. This is explained by the simple fact that in the present study the angle measured is the axial rotation “at rest” in the MRI scanner, whereas the biomechanical studies detect increased terminal IR under load with IR torque.8,26,34 Also, instability symptoms resulting from ACL deficiency occur near the end range of IR, whereas the resting position of the knee during MRI acquisition is relatively “midrange.” Last, the observed discrepancy may be influenced by the timing of imaging after ACL injury. Professional soccer players typically undergo MRI within hours to a few days postinjury, whereas imaging in the general population often occurs several days to weeks, or even months, later. This delay may allow for progressive stretching or attenuation of peripheral rotational stabilizers, potentially resulting in greater axial malalignment. However, prior research has not demonstrated significant differences in TF rotation between acute and chronic ACL-deficient knees. 45
Limitations
This study has several limitations. Its retrospective design introduces the potential for selection bias, particularly as only 9% of players who underwent ACL reconstruction had preinjury MRI available. The generalizability of findings is limited by the exclusive focus on professional soccer players, a highly specific cohort with distinct biomechanical, anatomic, and performance demands. This population is subject to a form of natural selection, whereby individuals with unfavorable anatomic variations, or intrinsic risk factors, may not reach or sustain elite levels, reducing applicability to broader patient populations. While this homogeneity enhances internal validity, it limits external validity. Nonetheless, the unique nature of this cohort offers a rare opportunity to analyze knee MRI scans with intact ACLs that went on to sustain injury. Additionally, TF rotation and TTTG distance measurements are sensitive to variability introduced by differences in knee flexion during image acquisition. Yet, this confounding factor was accounted for in the analysis, strengthening the methodological robustness. Although the sample size is relatively large for imaging-based ACL research in elite athletes and was determined through a priori power analysis, it may still be underpowered to detect subtle but clinically meaningful differences, as mentioned previously. In addition, the control group consisted of players with lateral meniscal injuries, and it is possible that certain anatomic or biomechanical characteristics may predispose to this injury pattern, potentially introducing residual confounding. Information regarding the specific mechanisms of ACL injury was not available, precluding analysis of whether particular alignment or rotational parameters are associated with distinct injury mechanisms. Furthermore, the clinical indications for obtaining preinjury MRI scans were not consistently documented, which may have contributed to selection bias. Finally, while measurements were performed by experienced musculoskeletal radiologists, intraobserver reliability was not assessed and therefore represents an additional limitation.
Conclusion
In this cohort of professional soccer players, TF axial rotation was not significantly associated with primary ACL injury. Although not statistically significant, the association between a smaller TTTG distance and ACL injury may reflect an underlying anatomic predisposition related to IR malalignment. Notably, neither resting axial TF rotation nor TTTG distance differed before and after injury, indicating that these features are likely inherent.
Footnotes
Final revision submitted December 12, 2025; accepted December 19, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from NHS Health Research Authority.