
Abstract
Background:
Rotator cuff tears are common injuries that significantly impair shoulder function and quality of life, particularly for large to massive tears, where maximal repair often results in high retear rates. Bridging reconstruction using acellular dermal allografts such as GraftJacket and AlloPatch offers a promising alternative by providing a scaffold that supports tendon healing and enhances structural stability. Although these grafts have similar biomechanical strengths, they differ in processing and biological properties, and comparative clinical outcomes remain understudied.
Purpose:
To compare radiologic and clinical outcomes of patients who underwent arthroscopic rotator cuff reconstruction using GraftJacket or AlloPatch allografts.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent arthroscopic bridging reconstruction for large to massive rotator cuff tears (>3 cm) using GraftJacket or AlloPatch were included. The primary outcome was healing assessed by magnetic resonance imaging. The secondary outcome was the Western Ontario Rotator Cuff (WORC) index. Tertiary outcomes were imaging-based structural metrics, including acromiohumeral interval (AHI), muscle atrophy (Warner grade), fatty infiltration (Goutallier-Fuchs classification), and structural integrity (Sugaya classification). Demographics, intraoperative data, and all outcome measures were compared between graft groups.
Results:
There were no significant demographic differences between GraftJacket (n = 49) and AlloPatch (n = 37) groups. The AlloPatch group had higher baseline supraspinatus muscle atrophy (P = .006) and fatty infiltration (P = .03) grades, along with more concurrent subscapularis repairs (P < .001). Postoperative imaging occurred at 2.22 ± 1.14 years for GraftJacket and 1.35 ± 0.70 years for AlloPatch (P < .001). Graft healing was not significantly different between groups (AlloPatch: 76%, GraftJacket: 69%; P = .52). Postoperative patient-reported outcomes were measured at 2.91 ± 0.87 years for GraftJacket and 2.64 ± 0.66 years for AlloPatch (P < .27). Both groups improved WORC scores from preoperative to postoperative assessment (P < .001), with no between-group difference (P = .97). The AlloPatch group had an increased postoperative AHI (P = .045), and the GraftJacket group did not, although the GraftJacket group had higher structural integrity (Sugaya) grades postoperatively (P = .02). No other between-group differences in imaging-based structural metrics were found.
Conclusion:
GraftJacket and AlloPatch dermal allografts yield comparable healing, patient-reported outcomes, and structural imaging metrics following arthroscopic bridging reconstruction for large to massive rotator cuff tears, demonstrating similar efficacy.
Keywords
Rotator cuff tears are a prevalent pathology that affects 20.7% to 60% of the general population, causing upper extremity disability and shoulder pain, and affecting daily activities and quality of life.17,18,26,36,39,42 Maximal repair, the gold standard operative intervention for large to massive rotator cuff tears, aims to reattach as much torn tendon to the humerus as possible, but has drawbacks, including tendon stretching and impaired healing.7,17 Despite short-term pain relief and improved functionality, retear rates from maximal repair surgery range from 50% to 90% and increase with age.1,5,7,11,13,30
Bridging reconstruction is an alternative procedure that can provide additional strength and stability for large to massive rotator cuff tears and has been shown to be effective for irreparable tears. 24 This technique uses a suture with or without a graft as a “bridge” to secure the tendon to its humeral attachment site. The goal of bridging reconstruction is to improve rotator cuff function by maintaining the anteroposterior (AP) coupling force through containment of the humeral head within the glenoid.15,40 Using an acellular dermal allograft—a nonimmunogenic graft derived from human skin—for bridging reconstruction is beneficial, as it acts as a scaffold, facilitating healing from the cuff remnant to the graft and subsequently from the graft to the bone.19,20 Additionally, the use of acellular dermal allografts for bridging reconstruction is believed to increase the load to failure and provide greater suture pull-out strength compared with the remnant cuff.1,6
Both GraftJacket and AlloPatch are freeze-dried acellular human dermal matrices used in bridging reconstruction for rotator cuff tears, but they differ in several aspects. GraftJacket is prepared by eliminating all cellular components while preserving vascular channels, collagen, elastin, and proteoglycan. 10 This preparation ensures proper integration into the tissue, with histological samples showing proper orientation and extensive blood vessels without signs of inflammation. 36 In contrast, AlloPatch is noted for its high levels of angiogenesis, likely due to its lower collagen matrix density allowing more porosity and space for blood vessels, which is beneficial for blood supply during healing. 26 Additionally, AlloPatch is a minimally processed graft that is prepared aseptically rather than terminally sterilized, potentially retaining more of its natural elements, whereas GraftJacket is a regenerative tissue matrix that is sterilized terminally. 26 Both grafts have similar strength profiles and tensile moduli, which are superior to non-dermal allograft types such as tendon grafts. 4 Of note, GraftJacket is typically thinner than 3 mm while AlloPatch is 3 to 5 mm thick, given that it is taken from a deeper reticular layer of the dermis than GraftJacket. The availability of allografts varies widely, even between hospitals within the same region, complicating the standardization of treatments for large to massive rotator cuff tears. GraftJacket and AlloPatch have been shown to have superior biomechanical properties compared with other widely available allograft types. 4 The current literature describes successful outcomes when GraftJacket is used for bridging reconstruction and rotator cuff augmentation, but lacks data investigating or comparing the use of AlloPatch or other graft types.22,31,32 Understanding long-term healing outcomes across allografts is crucial for hospitals selecting materials and for surgeons making informed treatment decisions. Thus, the purpose of this study was to retrospectively compare postoperative outcomes of patients who underwent arthroscopic rotator cuff repair and bridging reconstruction using GraftJacket or AlloPatch allografts. The primary outcome was healing, determined via magnetic resonance imaging (MRI), and the secondary outcome was patient-reported outcomes measured using the Western Ontario Rotator Cuff (WORC) index. Tertiary outcomes were imaging-based structural metrics, including acromiohumeral interval (AHI), and changes in muscle atrophy, fatty infiltration, and structural integrity grades. We hypothesized that both groups would show comparable healing rates and that there would be no significant differences in patient-reported outcomes or imaging-based structural metrics between groups.
Methods
Study Design
This study received ethical approval from the Nova Scotia Health Research Ethics Board (file No. 1029260). This study was a single-center, single-surgeon, retrospective case analysis of patients who underwent bridging reconstruction between 2012 and 2021.
Participant Selection
Inclusion in this study required that patients had been treated surgically with arthroscopic bridging reconstruction using acellular human dermal allograft matrix. Patients must have undergone bridging reconstruction using either GraftJacket (LifeCell) or AlloPatch (MTF Biologics) dermal allografts. Patients from the GraftJacket group received surgery between 2012 and 2018, while patients from the AlloPatch group received surgery between 2018 and 2021. Our institution switched from GraftJacket to AlloPatch in 2018 because AlloPatch is a thicker and less expensive graft; the remainder of the surgical approach and technique did not otherwise change over time. Participants were excluded from the study if they did not obtain a routine preoperative and/or minimum 6-month postoperative MRI 28 or if they were deceased at follow-up. Patients were not eligible to receive surgery if they had a local or systemic infection, neurological or vascular condition, and/or another concomitant condition that would influence their surgical safety.
Surgical Technique
All surgeries were conducted at the Queen Elizabeth II Health Sciences Center in Halifax, Nova Scotia, by a fellowship-trained orthopaedic surgeon (I.W.). Indications for surgery included an MRI-confirmed diagnosis of a large to massive rotator cuff tear (>3 cm) and/or involving ≥2 tendons with some tendon remaining for reattachment to the greater tuberosity.
The surgical technique used in this retrospective study has been previously described. 40 All patients were placed in the lateral decubitus position and underwent a 15-point arthroscopic diagnostic evaluation. A partial rotator cuff repair using single-row technique was completed followed by allograft reconstruction using 1 of the 2 dermal allografts (Allopatch or GraftJacket). The graft was prepared on the back table, where 11 sutures were sequentially tied to the graft, with 3 sutures placed anteriorly, posteriorly, and medially, and 2 sutures laterally. The sutures were passed from the dermal allograft through the remnant medial cuff using a Spectrum suture passer (ConMed Corp). The graft was then shuttled into the shoulder, tied to the remnant cuff and greater tuberosity anchors, and tensioned using a double-row configuration.
Rehabilitation Protocol
All patients underwent the same rehabilitation protocol performed in person, guided by a physical therapist. The protocol consisted of 8 weeks of immobilization in a sling. 29 Passive forward flexion and external rotation were permitted for the following 4 weeks, progressing to active assisted and active shoulder motion for another 4 weeks. Strengthening began at 16 weeks postoperatively.
Demographic and Intraoperative Data Collection
Patient demographic information including age at surgery, body mass index (BMI), sex, operative side, and whether the surgery was a primary or revision case, as well as baseline imaging-based metrics including Hamada grade for rotator cuff arthropathy 16 were collected to characterize the groups. Intraoperative data including the AP and mediolateral (ML) sizes of the rotator cuff tear, the size of the graft, and whether there was concurrent subscapularis repair were also collected.
Rotator Cuff Healing
The primary outcome was rotator cuff healing. Healing was measured by a fellowship-trained orthopaedic surgeon (R.O.), blinded to graft type using MRI images obtained at minimum 6-months postoperatively. 28 The 1.5-T MRI images, using T1 and T2 weighting, were routinely requested for all patients to determine graft and rotator cuff healing. Postoperative MRI readings of graft status were interpreted and divided into 3 categories (healed, partial tear, and complete tear).3,24,40 A healed graft appeared as a continuous hypointense linear band extending from the native tendon to the greater tuberosity, with a flat or linear subacromial course and a down-sloping convexity at the humeral insertion. Partial tears showed partial continuity from the tendon to the greater tuberosity, with areas of discontinuity, incomplete fibers, or curvilinear morphology. A complete tear was defined by a full-thickness gap in both the AP and the craniocaudal dimensions or a serpentine/curvilinear retracted configuration of the graft. 3
Patient-Reported Outcomes
The secondary outcome measure was the WORC index. The WORC is a rotator cuff–specific health-related quality of life questionnaire. 25 It contains 21 items across 5 domains, including physical symptoms, sports and recreation, work, social function, and emotions. Each item is scored from 0 (no symptoms) to 100 (worst possible symptoms). Final scores are calculated as a percentage score, and total scores range from 0% (highest functional status) to 100% (lowest functional status). WORC scores were collected preoperatively and again at a standardized follow-up between 2 and 4 years postoperatively.
The minimal clinically important difference (MCID) in WORC scores was calculated for each group using a distribution-based method: MCID = 0.5 × SD of the change in WORC score (postoperative–preoperative). The proportion of each group achieving the respective MCID was determined by comparing each participant's change score with the MCID value. This approach is supported by empirical research demonstrating that a change of this magnitude reflects a moderate effect size (Cohen d = 0.5) and is typically perceived by patients as both meaningful and beneficial.23,33,35,41 The 0.5-SD threshold has been widely validated as an indicator of clinically important improvement across various health-related quality of life instruments, including in orthopaedic populations.33,35,41
Imaging-Based Structural Metrics
Plain radiographs in the AP view were evaluated to determine pre- and postoperative radiographic outcomes measured using the AHI. Shoulder radiographs were taken with the arm in neutral and were unweighted. The AHI was measured as the shortest distance between the inferior aspect of the acromion to the humeral head. Pre- and postoperative MRIs were measured to determine muscle atrophy and fatty infiltration in the supraspinatus and infraspinatus. Muscle atrophy was categorized using the Warner classification system, defined as grade 1 (no atrophy), grade 2 (mild atrophy), grade 3 (moderate atrophy), or grade 4 (severe atrophy).14,38 Fatty infiltration was reported according to the Goutallier-Fuchs (GF) classification, categorized as grade 0 (normal muscle), grade 1 (some fatty streaks), grade 2 (<50% fatty muscle atrophy), grade 3 (50% fatty muscle atrophy), or grade 4 (>50% fatty muscle atrophy).14,38 Finally, postoperative MRIs were further evaluated using the Sugaya method for structural integrity and graded based on graft thickness, presence of high intensity areas or discontinuity, and graft homogeneity. 37 Sugaya categories are classified as type 1 (sufficient thickness compared with normal rotator cuff with homogeneous low intensity signal; normal), type 2 (sufficient thickness with partial high intensity; mild degeneration), type 3 (<50% thickness without discontinuity; no full retear), type 4 (minor discontinuity; small partial retear), or type 5 (major discontinuity; full thickness retear). 37 The same assessor (R.O.) evaluated all imaging-based structural metrics for all patients.
Statistical Analysis
Statistical analysis was performed using RStudio (Version 2024.12.0+467; Posit PBC), with the significance level set at an alpha value of .05. Descriptive statistics were used to characterize the study population at baseline, using mean and standard deviation for continuous variables, frequency and percentage for categorical variables, and median and interquartile range for ordinal variables. Between-group comparisons were conducted for all baseline variables. A Shapiro-Wilk test was used to assess normality, and the Levene test was used to assess homogeneity of variance. Continuous demographic variables (age, BMI, postoperative MRI follow-up time) and intraoperative measures (AP tear size, ML tear size, graft size) were compared using independent t tests or Mann-Whitney U tests, depending on the results of normality and variance testing. Categorical variables (sex, operative side, revision surgery, concurrent subscapularis repair) were analyzed using the chi-square or Fisher exact test based on expected frequencies. Ordinal baseline radiographic variables (Hamada grade for rotator cuff arthropathy, Warner grade for muscle atrophy, and GF classification for fatty infiltration) were analyzed using the Mann-Whitney U test.
For the primary outcome, rotator cuff healing between-group differences were assessed using the Mann-Whitney U test. Secondary outcomes included WORC scores, which were analyzed using a 2-way repeated measures analysis of variance (ANOVA) to test the main effects of group and time along with their interaction. Pre- and postoperative WORC scores, change (pre- to postoperative) scores, and clinical follow-up durations were compared between groups using independent t tests or Mann-Whitney U tests, as appropriate. The proportion of patients achieving the MCID in WORC scores was compared between groups using a chi-square or Fisher exact test. For tertiary imaging outcomes, AHI was analyzed using a 2-way repeated measures ANOVA to assess the main effects of group and time, and their interaction, with post hoc testing completed as necessary. Progression (ie, an increase of ≥1 grade) in Warner and GF grades for muscle atrophy and fatty infiltration, respectively, were compared between groups using the chi-square or Fisher exact test. Finally, postoperative Sugaya grades for structural integrity were compared between groups using the Mann-Whitney U test.
Results
Demographic and Intraoperative Data
A total of 139 consecutive patients were initially identified for study, and 86 were included (GraftJacket, n = 49; AlloPatch, n = 37) (Figure 1). The 2 graft groups did not differ significantly across demographic variables (Table 1). The AlloPatch group had statistically significantly higher supraspinatus Warner (P = .006) and GF (P = .03) grades than the GraftJacket group, indicating more muscle atrophy and fatty infiltration at baseline. There were no other statistically significantly different preoperative structural imaging characteristics between groups (Table 1). Intraoperatively, there were no statistically significant differences in the mean AP tear size, ML tear size, or graft size (Table 1). However, a significantly higher proportion of patients in the AlloPatch group underwent a concurrent subscapularis repair compared with the GraftJacket group (P < .001).
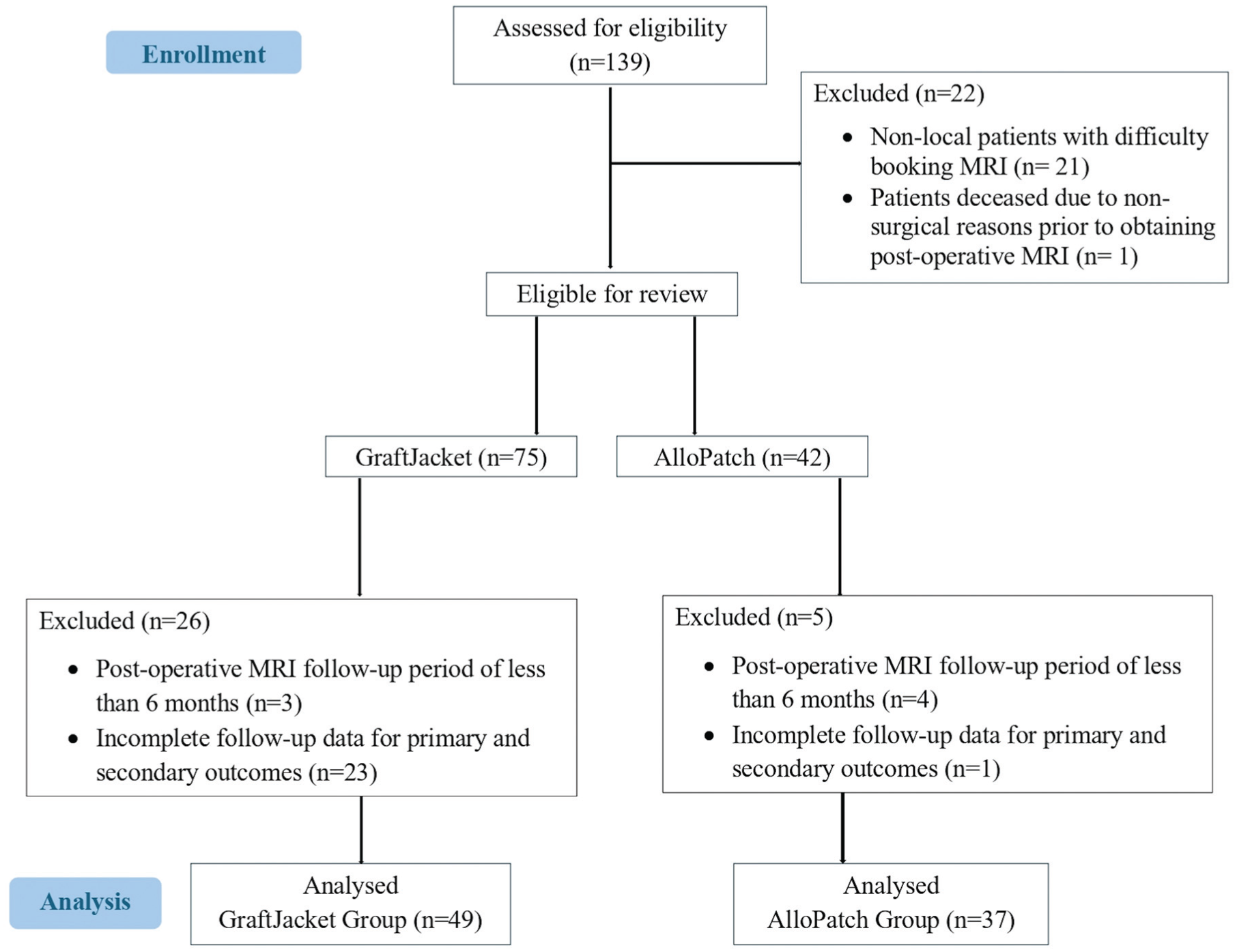
Flowchart depicting the process of patient selection. MRI, magnetic resonance imaging.
Baseline Patient Characteristics and Intraoperative Data a
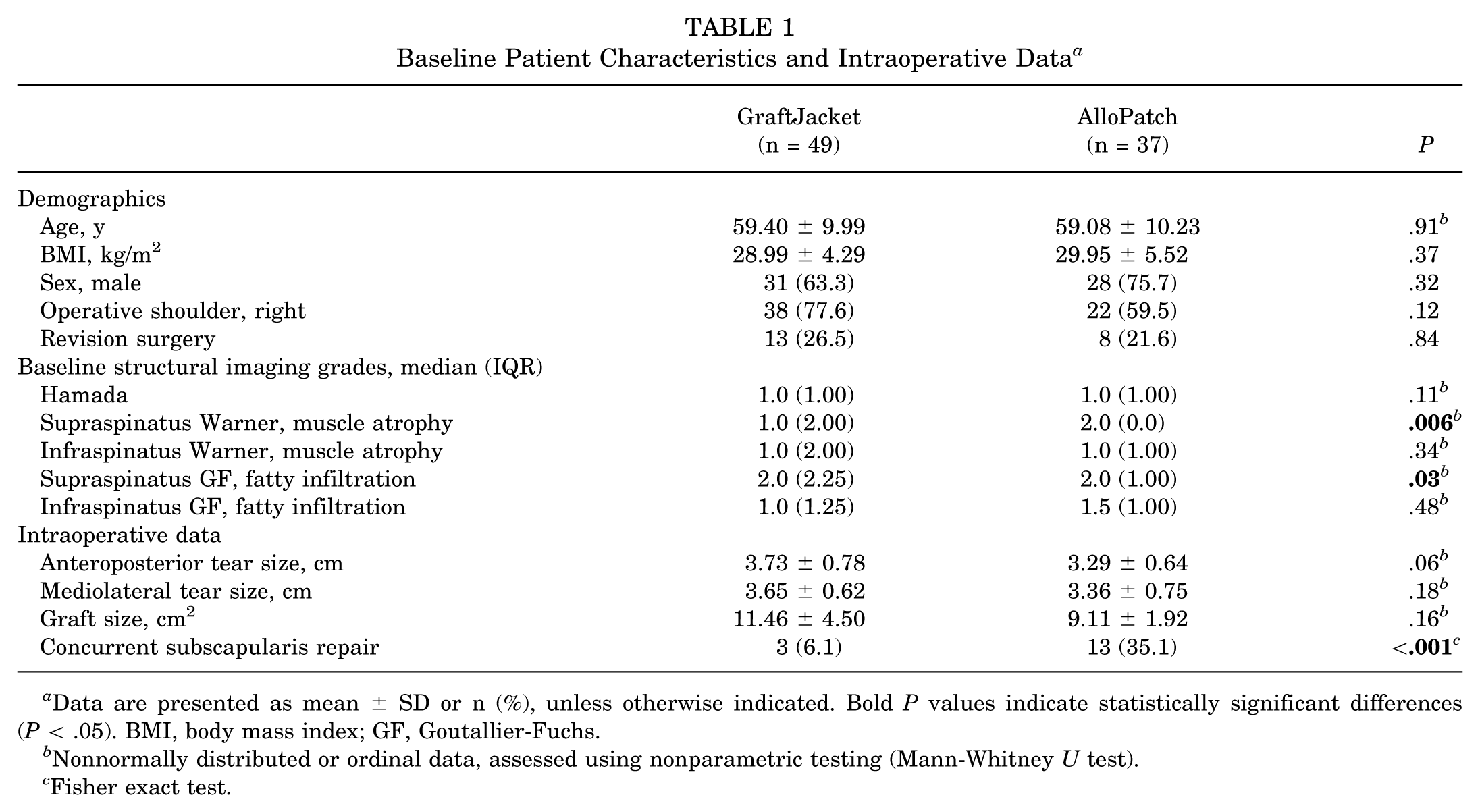
Data are presented as mean ± SD or n (%), unless otherwise indicated. Bold P values indicate statistically significant differences (P < .05). BMI, body mass index; GF, Goutallier-Fuchs.
Nonnormally distributed or ordinal data, assessed using nonparametric testing (Mann-Whitney U test).
Fisher exact test.
Rotator Cuff Healing
The time between surgery and postoperative MRI differed significantly between groups (P < .001). Mean ± SD postoperative imaging occurred at 2.22 ± 1.14 years (range, 0.50-5.58 years) in the GraftJacket group and 1.35 ± 0.70 years (range, 0.59-3.09 years) in the AlloPatch group. Postoperatively in the GraftJacket group (n = 49), 69.4% of patients (n = 34) showed complete healing, 16.3% (n = 8) showed partial tears, and 14.3% (n = 7) demonstrated complete graft tears. In the AlloPatch group (n = 37), 75.7% of patients (n = 28) demonstrated complete healing, 13.5% (n = 5) had partial tears, and 10.8% (n = 4) had complete tears. There were no statistically significant differences in healing between groups (P = .52).
Patient-Reported Outcomes
The length of clinical follow-up did not differ significantly between groups (P = .27) (Table 2). Clinical follow-up time points ranged from 2 to 4 years for both groups. There was no statistically significant main effect of group (P = .97), or interaction between group and time (P = .29), on WORC scores. However, there was a statistically significant main effect of time on WORC scores (P < .001), indicating that WORC scores significantly improved from pre- to postoperatively across both groups. There were no statistically significant between-group differences in preoperative, postoperative, or WORC change scores (Table 2). The cohort-specific MCID thresholds for WORC scores were calculated as −13.03% for GraftJacket and −13.64% for AlloPatch. There was no significant between-group difference in the proportion of patients who achieved the MCID in WORC scores (Table 2).
Western Ontario Rotator Cuff (WORC) Scores a
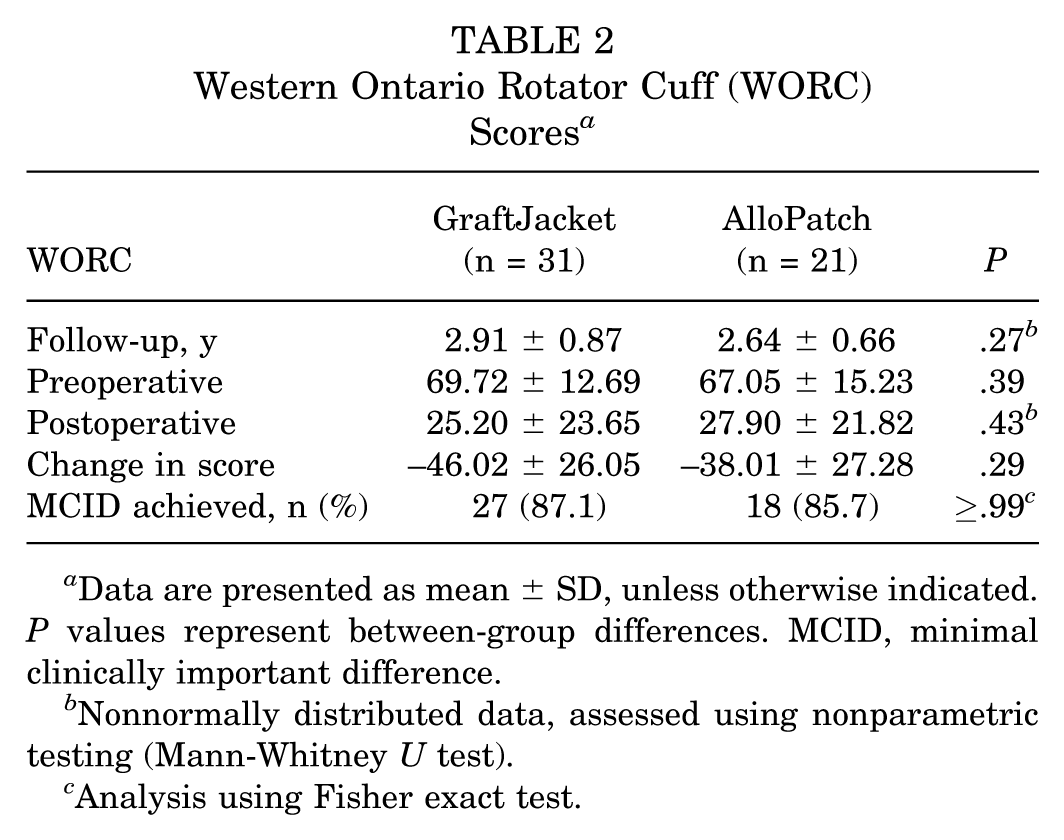
Data are presented as mean ± SD, unless otherwise indicated. P values represent between-group differences. MCID, minimal clinically important difference.
Nonnormally distributed data, assessed using nonparametric testing (Mann-Whitney U test).
Analysis using Fisher exact test.
Imaging-Based Structural Metrics
There was a statistically significant main effect of time (P = .046), and interaction between group and time (P = .01), but no significant main effect of group (P = .32) on AHI (Table 3). Post hoc testing revealed a significant increase in AHI from pre- to postoperative in the AlloPatch group (P = .045), but not in the GraftJacket group (P = .55).
Acromiohumeral Intervals (AHIs) Gathered via Radiographic Image a
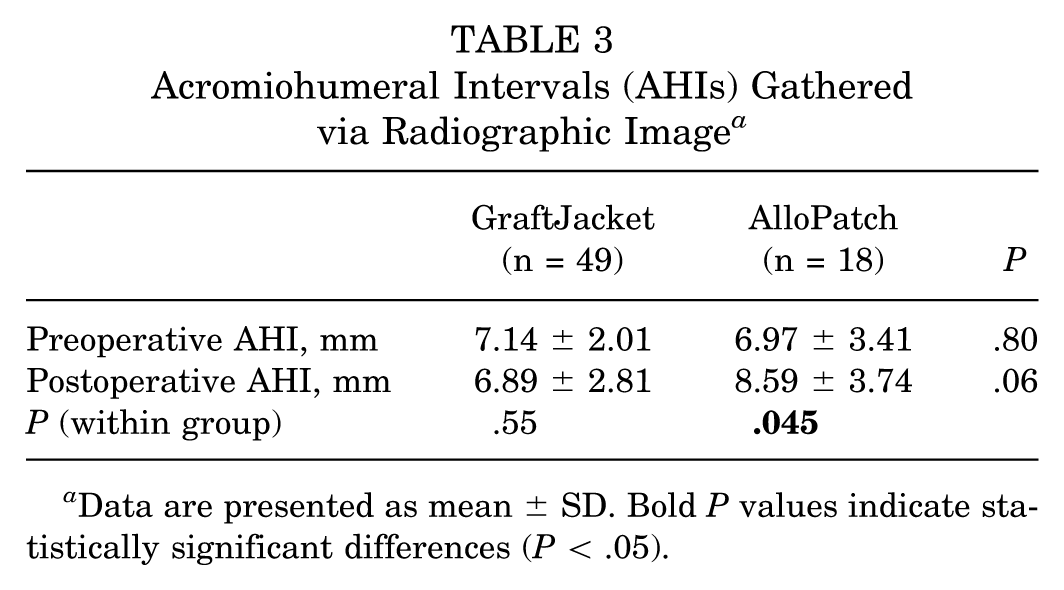
Data are presented as mean ± SD. Bold P values indicate statistically significant differences (P < .05).
Postoperative Warner grades, with median (IQR), in supraspinatus were 2.0 (1.00) for GraftJacket and 2.0 (0.00) for AlloPatch and in infraspinatus were 1.0 (2.00) for GraftJacket and 2.0 (1.00) for AlloPatch. Postoperative GF grades with median (IQR) in supraspinatus were 1.0 (2.25) for GraftJacket and 3.0 (1.00) for AlloPatch and in infraspinatus were 2.0 (2.00) for GraftJacket and 2.0 (1.25) for AlloPatch. There were no statistically significant between-group differences in progression of Warner (muscle atrophy) or GF (fatty infiltration) grades in the supraspinatus or infraspinatus muscles (Table 4).
Progression of Atrophy (Warner Classification) and Fatty Infiltration (GF Classification) Grades for Supraspinatus and Infraspinatus Muscles a
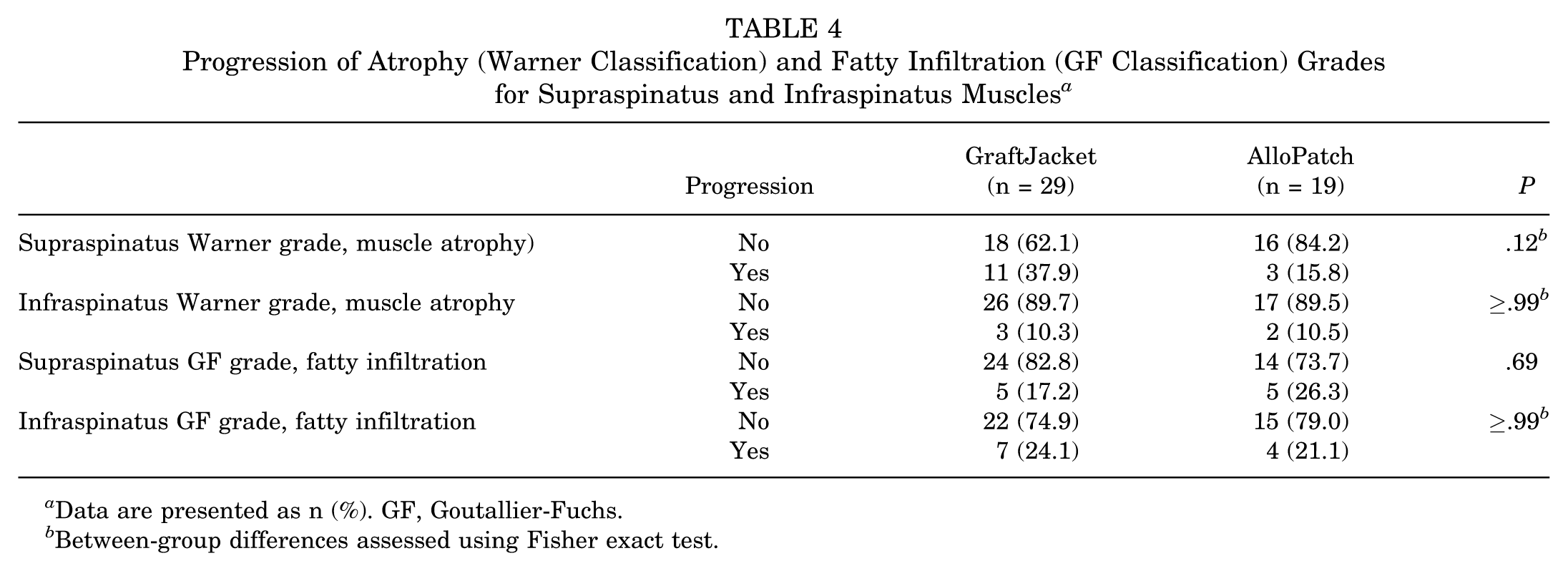
Data are presented as n (%). GF, Goutallier-Fuchs.
Between-group differences assessed using Fisher exact test.
Finally, there was a statistically significant between-group difference in postoperative structural integrity of the rotator cuff, measured using the Sugaya scale (P = .02). Median (IQR) postoperative Sugaya grades were 3 (2.0) for GraftJacket and 2 (1.0) for AlloPatch.
Discussion
This study found no difference in healing rates between GraftJacket and AlloPatch groups, and patient-reported outcomes measured using the WORC index improved from pre- to postoperatively, with no significant between-group differences. Although the AlloPatch group demonstrated greater baseline muscle atrophy, fatty infiltration, and more intraoperative subscapularis repairs than the GraftJacket group, the AlloPatch cohort achieved better postoperative structural integrity and a significant increase in AHI from pre- to postoperatively. These findings suggest that AlloPatch may provide superior structural outcomes even in the setting of less favorable baseline characteristics, though differences in baseline pathology should be considered when interpreting these imaging-based results. Overall, the results from this study suggest that both dermal allografts largely provide comparable effectiveness in the bridging reconstruction of large to massive rotator cuff tears.
Healing rates following bridging reconstruction with human acellular dermal allografts did not differ between graft types. Similar healing rates align with intraoperative findings of comparable tear and graft sizes between groups. These results align with findings from Barber and Aziz-Jacobo, 4 who reported similar suture retention strength for GraftJacket and AlloPatch. 8 The strength of both grafts was superior to other available allografts. 4 Additionally, both cohorts showed few differences in baseline demographic, imaging, and intraoperative metrics. These factors are important because previous research has shown that age, AP tear size, and fatty infiltration of the infraspinatus muscle, among other factors, were significant prognostic determinants influencing rotator cuff healing after surgical reconstruction.12,27 Finally, other previous studies documented healing and concurrent improvements in patient-reported and functional outcomes for patients treated with GraftJacket2,31 and AlloPatch,2,31 which collectively align with the results of this study.
Patients in both groups demonstrated significant improvement in patient-reported outcomes (WORC scores) following bridging reconstruction with dermal allografts, with no between-group differences. Additionally, there were no between-group differences in the proportion of patients achieving the allograft-specific MCID values, suggesting that both graft types provide clinically relevant functional improvement. The magnitude of pre- to postoperative changes in WORC scores across both groups (36%-47%) are comparable with previous research that reported improvements of approximately 40% following GraftJacket reconstruction. 40
This study demonstrated that AHI significantly increased in the AlloPatch group from pre- to postoperatively, while the GraftJacket group experienced a nonsignificant decrease in AHI. The current AlloPatch results generally agree with findings by Ono et al, 34 who showed that increased AHI is associated with better healing outcomes and improved WORC scores. The current GraftJacket findings also align with previous research that showed a decrease in AHI following bridging reconstruction with GraftJacket. 40 In our opinion, our findings of different AHI outcomes per group could potentially be explained by the thickness of the grafts. Since AlloPatch is thicker (between 3 and 5 mm) than GraftJacket (<3 mm), the increased graft thickness may account for the observed improvement in AHI by providing increased stability. In addition, the AlloPatch group was noted to have a significantly higher rate of concurrent subscapularis repair than the GraftJacket group, which may have contributed to the strength of the repairs within this group through restoration of the anterior force-couple, increased anterior stability, and provision of reduced stresses on the rotator cuff tear. Previous retrospective studies have shown that concurrent subscapularis repairs with arthroscopic rotator cuff repairs led to successful functional and/or structural outcomes.9,21
Furthermore, current findings suggest that despite the AlloPatch group having worse baseline supraspinatus muscle atrophy and fatty infiltration compared with the GraftJacket group, there were no statistically significant differences in progression of muscle atrophy or fatty infiltration grades between grafts, and the AlloPatch group demonstrated better structural integrity postoperatively. Prior evidence has demonstrated that lower Sugaya grades (better structural integrity) are associated with higher postoperative abduction strength scores. 43 In this context, the superior structural integrity observed in the AlloPatch group, despite less favorable baseline muscle quality, suggests that graft selection may play a role in optimizing functional and/or biomechanical outcomes.
Limitations
This study has limitations that should be acknowledged. First, this study was limited by the single-surgeon, single-center, retrospective design. Only 1 rater was used to measure healing outcomes, which may reduce the reproducibility of these measurements. Additionally, this study may be influenced by several potential sources of bias. For instance, approximately 38% of the potential candidates identified for this study had incomplete data for primary analysis and were consequently excluded, and approximately 27% of included participants did not complete WORC scores at a minimum of 2 years postoperatively, which may lead to a missing data bias. There may also be a temporal bias because the 2 graft cohorts underwent surgery sequentially. These temporal changes may have led to potential confounding factors, including longer postoperative imaging and clinical follow-up time frames in the GraftJacket group, and a higher proportion of concurrent subscapularis repair in the AlloPatch group. Additionally, the 2 groups had different muscle atrophy and fatty infiltration at baseline, and we were unable to differentiate between large and massive rotator cuff tears; both limitations were consequences of the retrospective study design and including all available patients. There was also lack of information regarding biceps pathology and treatment available for these patients. In terms of outcomes, “healing” was essentially defined as a “failure to show a tear.” However, the graft remaining mechanically intact may differ from actual graft healing and incorporation into the tendon or bone. Also, while patient-reported outcomes were considered, there were no objective physical exam findings for further analysis of functional outcomes. Finally, this study examined 2 types of dermal allograft and did not include a non–dermal allograft comparison or nonaugmented repair control group. In our opinion, future studies would benefit from exploring differences between different types of grafts in a randomized controlled trial design to eliminate potential sources of bias and determine the most optimal graft type for rotator cuff bridging reconstruction.
Conclusion
Two different dermal allografts, GraftJacket and AlloPatch, yield comparable healing, patient-reported outcomes, and structural imaging metrics following arthroscopic bridging reconstruction. These findings indicate that both dermal allografts offer similar efficacy for treatment of large to massive rotator cuff tears using bridging reconstruction.
Footnotes
Acknowledgements
The authors acknowledge the support of the Laila B. Chase Research in Medicine (RIM) Summer Studentship.
Presented at the Orthopaedic Summit in Boston, September 2023, and at the Canadian Orthopaedic Association annual meeting in Halifax, June 2024.
Final revision submitted February 9, 2026; accepted February 16, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: I.W. reports personal fees from DePuy Mitek Inc, Smith & Nephew, CONMED Corp, Bioventus LLC, Arthrex, and VALD outside the submitted work; is an editorial board member for the American Journal of Sports Medicine, Arthroscopy, and The HIVE Musculoskeletal Journal; is an associate editor for the Orthopaedic Journal of Sports Medicine; and is a board or committee member for AANA, ISAKOS, and AAC. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study was approved by the institutional review board of Nova Scotia Health (No. 1029260).