
Abstract
Background:
Patellar instability in pediatric patients is commonly treated with medial patellofemoral ligament reconstruction (MPFLR). MPFLR alone does not directly address other underlying anatomic risk factors for patellar instability, such as lateralized patella tendon insertion. The Grammont procedure is a technique for medialization of the patella tendon insertion that can correct increased TT-TG distance in skeletally immature patients. This technique has not been studied in acute and recurrent traumatic patellar instability, nor has it been compared as an adjunct procedure to MPFLR.
Hypothesis/Purpose:
The purpose of this study was to compare medial patellofemoral ligament reconstruction (MPFLR) alone versus MPFLR with a Grammont procedure in pediatric patients. It was hypothesized that combining MPFLR with the Grammont procedure, compared with MPFLR alone, would reduce recurrent patellar instability, achieve greater correction of the tibial tubercle–trochlear groove (TT-TG) (MPFLR alone) or patellar tendon insertion–trochlear groove (PTI-TG) (MPFLR + Grammont) distance, and maintain a comparable complication rate.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review was performed including all pediatric patients (<19 years) treated surgically for patellar instability at 1 institution between 2010 and 2023. A total of 45 patients underwent MPFLR and 36 patients underwent MPFLR plus Grammont. Rates of recurrent instability and revision surgery were compared. Pre- and postoperative imaging (radiography and magnetic resonance imaging) was used to evaluate changes in Caton-Deschamps ratio and TT-TG (MPFLR alone) or PTI-TG (MPFLR + Grammont). Additionally, the investigators compared the rate of modified Clavien-Dindo grade II and III complications between surgical groups.
Results:
In the MPFLR + Grammont group vs the MPFLR-only group, patients were younger at the time of surgery (median age 13.4 vs 15.3 years, respectively; P = .013), the percentage of female patients was higher (80.6% vs 55.8%; P = .016), and the mean preoperative TT-TG was larger (18.8 vs 15.7 mm; P = .001). Twenty (25.3%) patients had grade II/III complications, with no significant differences between surgical groups. Twelve patients (14.8%) experienced recurrent instability, with rates of 20.9% in the MPFLR-only group and 8.3% in the MPFLR + Grammont group (P = .120). Revision surgery for recurrent patellar instability was performed in 4 patients in the MPFLR-only group (9.3%) and 1 patient in the MPFLR + Grammont group (2.8%). In the MPFLR + Grammont group, 1 patient had a growth arrest of the tibial tubercle apophysis resulting in recurvatum deformity.
Conclusion:
In pediatric patients with patellar instability and increased TT-TG distance, adding a Grammont procedure to MPFLR resulted in similar overall complication rates compared with isolated MPFLR. The MPFLR + Grammont group was younger and had more severe anatomic risk factors; the investigators observed a possibly lower rate of recurrent instability and fewer revision surgeries.
Keywords
Patellar instability is a complex condition with a wide array of surgical treatment options, each tailored to patient-specific factors. The tibial tubercle–trochlear groove (TT-TG) distance was popularized by Dejour et al 11 in 1994 and has been used to quantify the amount of laterization of the tibial tubercle. The TT-TG distance is the distance between the tibial tubercle and the trochlear groove, using axial imaging. Lateralization of the tibial tubercle is defined by an increase in the TT-TG distance and is a known risk factor for first-time and recurrent patellar dislocations. 9 In skeletally mature patients, tibial tubercle osteotomies (TTOs) and medial patellofemoral ligament reconstruction (MPFLR) have demonstrated high success rates in addressing patellar instability in patients with an elevated TT-TG distance.
TTOs have emerged as an effective surgical intervention to correct an elevated TT-TG distance, with reported success rates of 72.5% to 86% over follow-up periods of 6.2 to 8.2 years.4,30 Additionally, patients undergoing MPFLR in the presence of an elevated TT-TG distance have demonstrated improved functional outcomes and kinematics when combined with TTO. 17 For skeletally immature patients with a lateralized tibial tubercle, traditional TTOs are contraindicated because they would damage the tibial tubercle apophysis. This has led to the development of physeal-sparing techniques, such as the Roux-Goldthwait procedure and the Galeazzi technique.5,8,33 These approaches aim to address the lateralizing force on the patella by rerouting half of the patellar tendon medially (Roux-Goldthwait) or by anchoring medial hamstrings to the inferomedial patella. Grammont et al 18 described a technique in 1985 in which the patellar tendon was detached from the tibial tubercle, preserving only the distal-most tendon-periosteal connection. This approach allowed the tendon to be resecured medially with periosteal fixation and included a lateral release. Krause et al 22 later reported a modified Grammont technique in which no lateral release was performed and the medial side of the tendon was not affixed to the periosteum. Using this modified technique alone, Krause et al observed a 19% (n = 65) redislocation rate with a mean follow-up of 8 years. 22
To our knowledge no study has compared MPFLR alone versus MPFLR with a Grammont procedure in pediatric patients. We hypothesized that combining MPFLR with the Grammont procedure, compared with MPFLR alone, would reduce recurrent patellar instability, achieve medial shift of the tendon insertion, and maintain a comparable complication rate.
Methods
After institutional review board approval was granted, a retrospective review was conducted of pediatric patients (age ≤19 years at the time of surgery) at a single, Level 1 pediatric trauma center, who underwent MPFLR alone or MPFLR + Grammont procedure (Figures 1 -3) for patellar instability between January 2010 and March 2023. Patients with <3 months of postoperative follow-up, congenital or fixed dislocations, simultaneous trochleoplasty/TTO procedure, and revision cases were excluded. Patients were not excluded for incomplete imaging in the postoperative course.
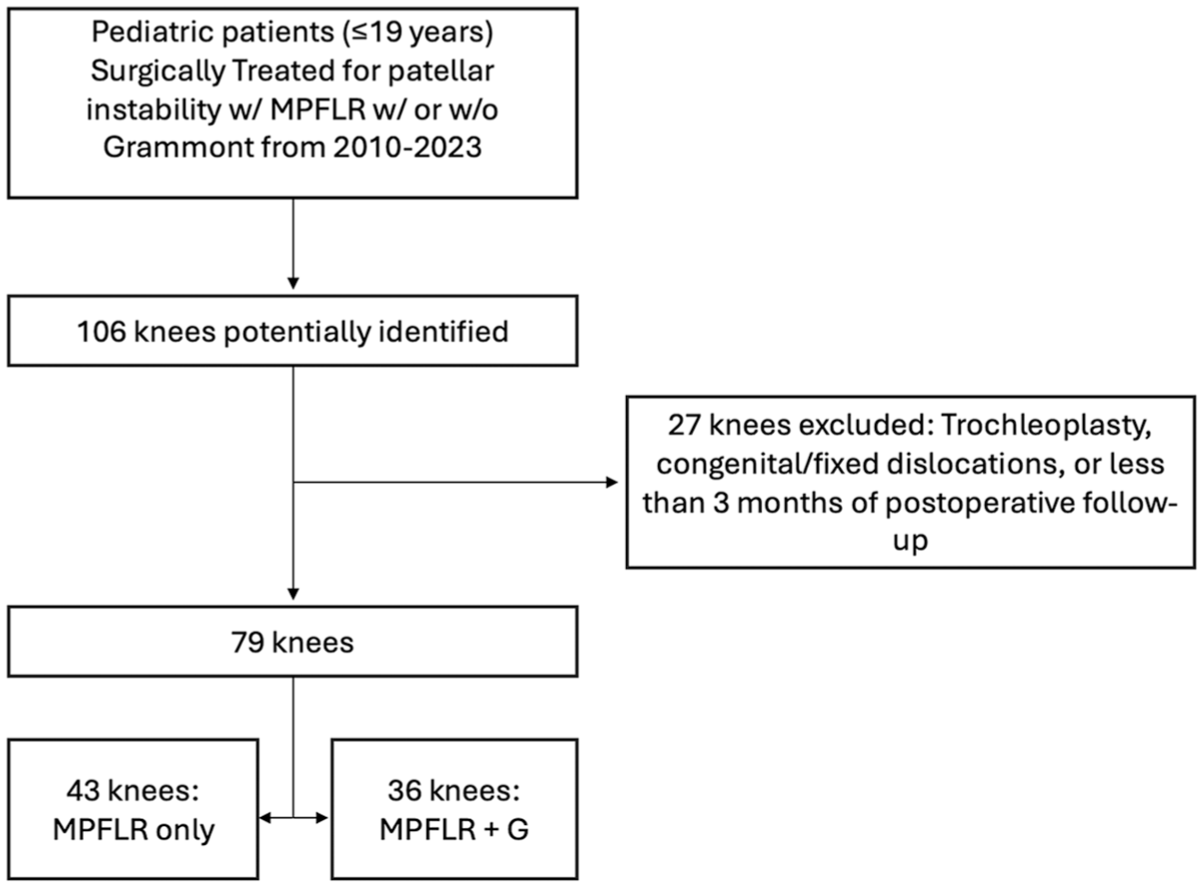
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flow chart. G, Grammont; MPFLR, medial patellofemoral ligament reconstruction.
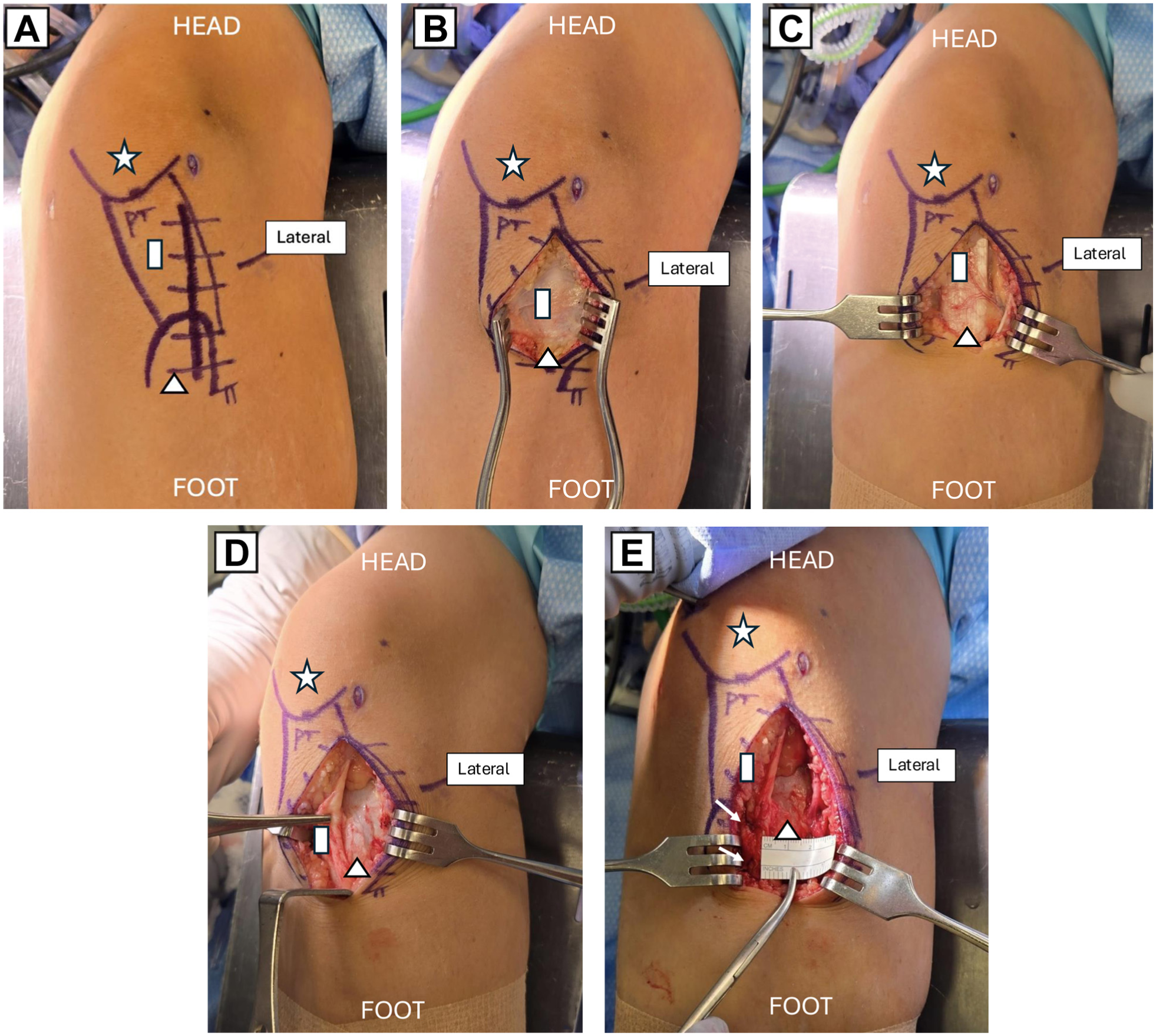
Grammont technique on a left knee. (A) The incision is marked slightly lateral to midline, extending from the distal pole of the patella (white star) along the patellar tendon (PT, white rectangle) to the midportion of the tibial tubercle (TT, white triangle). Note the lateralized attachment of the PT on the TT. (B) The incision is carried down to the peritenon, and flaps are elevated medially and laterally. (C) The peritenon is incised along the lateral border of the patellar tendon (white rectangle) and elevated off the tendon. (D) The tendon (white rectangle) is reflected off the tibial tubercle (white triangle), with care taken not to damage the apophysis. The dissection is carried down distally to the periosteum, and a periosteal flap is elevated. The entire flap is allowed to translate medially. (E) In all cases, the tendon (white rectangle) was repositioned and secured medially using a suture anchor (white arrow, 2 sutures used in this case). The distal extensor mechanism attachment was medialized approximately 1.5 cm, leaving the tibial tubercle exposed (white triangle).
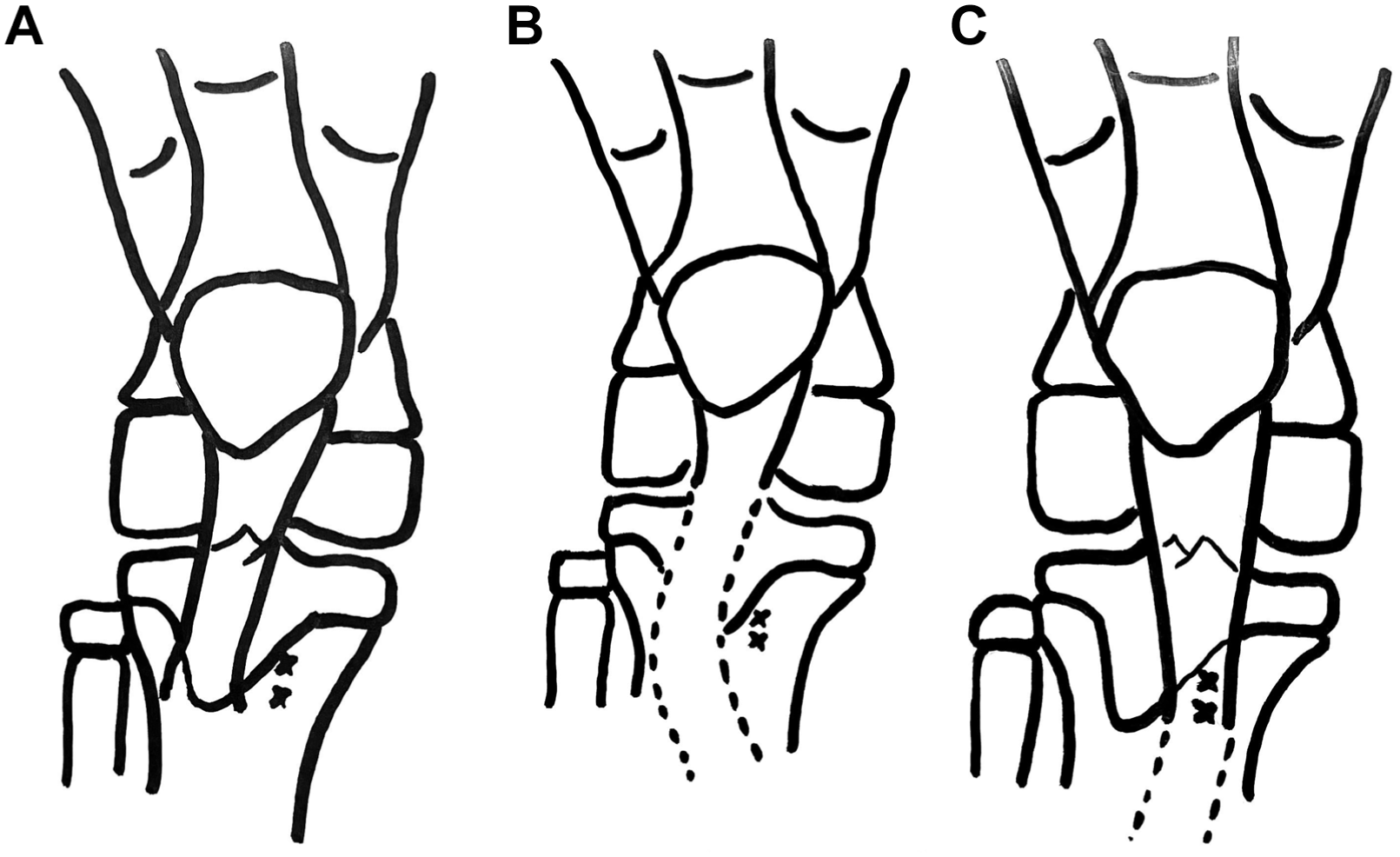
(A) Schematic of a skeletally immature right knee with a lateralized tibial tubercle. The vector of force between the quadriceps tendon and patellar tendon is not colinear, creating a Q-angle. The area marked with a double “x” represents a more medialized position, which could be achieved with a modified-Grammont procedure. (B) The dotted lines represent where the sharp dissection should occur. The patellar tendon is detached off the tibial tubercle apophysis. This dissection continues distally as the tendon blends with the periosteum. Note that the distal-most portion of the periosteum is left attached. A curved apex, lateral sharp dissection as shown allows the patellar tendon–periosteal complex to translate as 1 unit medially over the double “x.” With knee flexion and extension, the tendon is allowed to find a new medialized position before fixation. (C) The new position of the medialized patellar tendon over the double “x” position. The quadriceps tendon vector of force and patellar tendon are now colinear. The dotted line represents the still-attached distal periosteum. Fixation at the double “x” position can be performed with bone anchors or direct suture repair to the periosteum.
Patients were separated into 2 groups: MPFLR only and MPFLR + Grammont. Group assignment was based on the procedure performed as determined by the treating surgeon, reflecting clinical and radiographic decision-making. A total of 79 patients were included in this study, with 43 undergoing MPFLR only and 36 undergoing MPFLR + Grammont procedure. Data collection was done through retrospective chart review of the electronic medical record without any prospective patient contact or standardized follow-up protocol. This included patient demographic characteristics (age at surgery, sex, and body mass index [BMI]), clinical characteristics (operative side, time from initial instability to surgery, history of multiple dislocations), contralateral instability/surgery, alignment/rotational correction, simultaneous osteochondral surgical treatment, and postoperative course. History of multiple dislocations was recorded as a binary variable (yes/no), based on whether the patient reported >1 prior dislocation at the time of the initial visit. Alignment or rotational correction was captured as a binary variable (yes/no), defined as the performance of any adjunctive procedure intended to modify anatomic or rotational alignment, including TTO, distal femoral osteotomy, or rotational osteotomy. Patient follow-up was conducted according to individual surgeon preference and clinical indications, without a standardized protocol for the study; during these routine follow-up appointments, advanced imaging or additional evaluations were obtained only as deemed necessary by the treating surgeon. Postoperative complications were graded by the modified Clavien-Dindo classification after retrospective chart review. 43
The Clavien-Dindo classification is a standardized grading system that grades surgical complications based on the type of treatment required, stratifying complications into 5 main grades (I through V). 43 Sink et al 43 adapted this classification for orthopaedic surgery by preserving the original 5-grade structure while incorporating orthopaedic-specific definitions. This modified version was specifically tested and validated in the context of hip surgery and has since been applied to multiple orthopaedic specialties.
Preoperative and postoperative imaging data were obtained using radiographs and magnetic resonance imaging (MRI). Imaging variables collected include preoperative Caton-Deschamps ratio, preoperative TT-TG distance, postoperative Caton-Deschamps ratio, correction TT-TG distance, and final Caton-Deschamps ratio. Caton-Deschamps ratio was evaluated on lateral knee radiographs in 30° of knee flexion. Preoperative and postoperative coronal plane alignment was assessed using full-length hip-to-ankle radiographs. MRI measurements (preoperative TT-TG distance, patellar tilt, trochlear inclination, Dejour classification, and postoperative patellar tendon insertion–trochlear groove [PTI-TG] distance for MPFLR + Grammont and postoperative TT-TG distance for MPFLR only) were made on axial cuts on T2-weighted MRI sequences. Figure 4 provides details on how TT-TG and PTI-TG measurements were performed. Postoperative TT-TG distance and correction TT-TG distance were collected for 17 patients who had a postoperative MRI scan. Reviewers were not blinded to whether measurements were preoperative or postoperative. Reviewers were blinded to the specific surgical procedure performed (MPFLR alone or MPFLR + Grammont).
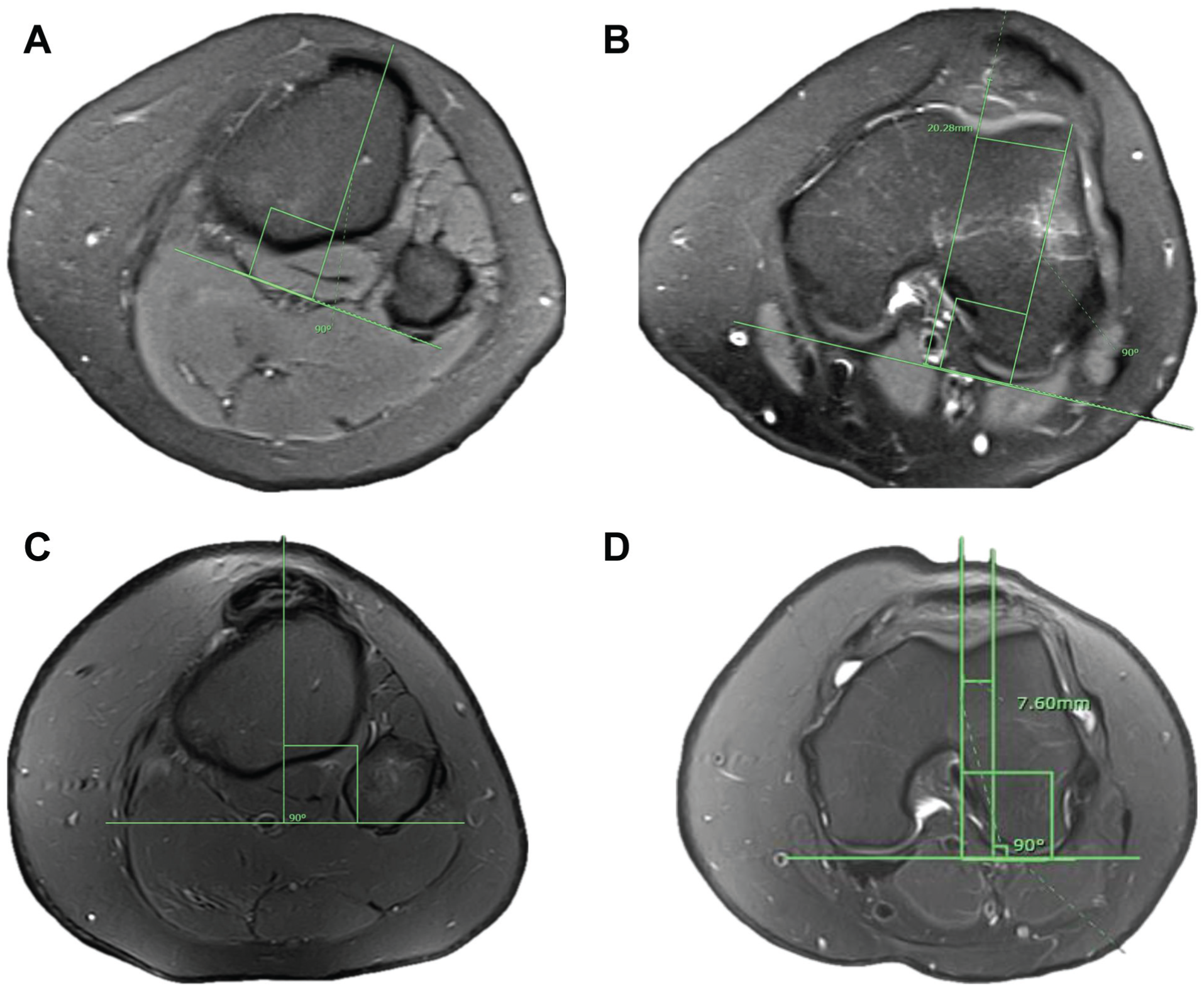
Pre- and postoperative tibial tubercle–trochlear groove (TT-TG) and patellar tendon insertion–trochlear groove (PTI-TG) distance measurements on axial magnetic resonance imaging scan in a patient who underwent medial patellofemoral ligament reconstruction + Grammont. (A) TT-TG distance measurement: A line is drawn through the tibial tubercle at the center of the patellar tendon insertion perpendicular to the axis of the posterior femoral condyles. (B) A line is drawn through the deepest point of the trochlear groove perpendicular to the posterior femoral condyles. The horizontal distance between these parallel lines represents the preoperative TT-TG distance. In this patient, TT-TG distance is 20.28 mm. (C) Postoperative PTI-TG distance measurement: A line is drawn through the tibial tubercle at the center of the medialized patellar tendon insertion perpendicular to the axis of the posterior femoral condyles. (D) A line is drawn through the deepest point of the trochlear groove perpendicular to the posterior femoral condyles. The horizontal distance between these parallel lines represents the PTI-TG distance. In this patient, PTI-TG distance is 7.60 mm.
Statistical Analysis
Continuous variables were assessed using intraclass correlation coefficient (ICC), whereas kappa statistics were used for categorical variables. Categorical variables were assessed by the senior author (E.L.N.) to minimize variability in interpretation.
Unpaired t test and nonparametric Mann-Whitney U tests were used to compare normally and nonnormally distributed continuous data, respectively, between the 2 groups determined by a Shapiro-Wilk test. Chi-square test and/or Fisher exact test (if any of the expected cell sizes were <5) was used to compare binary or categorical data between 2 groups.
Each patient's measurements were evaluated by 4 raters. The 4 raters included 3 attending orthopaedic surgeons (E.L.N., E.S., S.I.A.) and 1 medical student (A.D.). The ICC was calculated to assess interrater reliability between raters. Interobserver reliability was assessed among the 4 raters using a subset of the first 26 patients in the data set to ensure measurement consistency before dividing the remaining cases among the raters. The measurements duplicated for reliability assessment included preoperative radiographic Caton-Deschamps ratio, full-length angle, preoperative TT-TG distance, lateral trochlear inclination angle, and patellar tilt. For continuous variables, ICCs were calculated using a 2-way random-effects model based on single ratings and absolute agreement. The mean ICC values, along with 95% CI, were reported to determine the level of agreement, with ICC values categorized as poor (<0.40), fair (0.40-0.59), good (0.60-0.74), and excellent (0.75-1.0). 7
All statistical tests were 2-sided and performed at the .05 level of significance. Statistical analysis was performed using R statistical software, Version 4.3.2 (R Core Team, 2020).
Results
Patients in the MPFLR + Grammont group were younger at time of surgery (median age 13.4 vs 15.3 years; P = .013) and more patients in that group were female (80.6% vs 55.8%; P = .016). No significant differences in BMI or operative side were found between the groups (Table 1). The time from initial instability event to surgery was comparable across both groups (median 26.4 months; P = .548). The rate of preoperative patella alta was 57.1% in the MPFLR + Grammont group and 48.4% in the MPFLR-only group (P = .478). The mean preoperative TT-TG was higher in the MPFLR + Grammont group (18.8 vs 15.7 mm; P = .001).
Demographic and Clinical Characteristics Between MPFLR-Only and MPFLR + Grammont Groups a
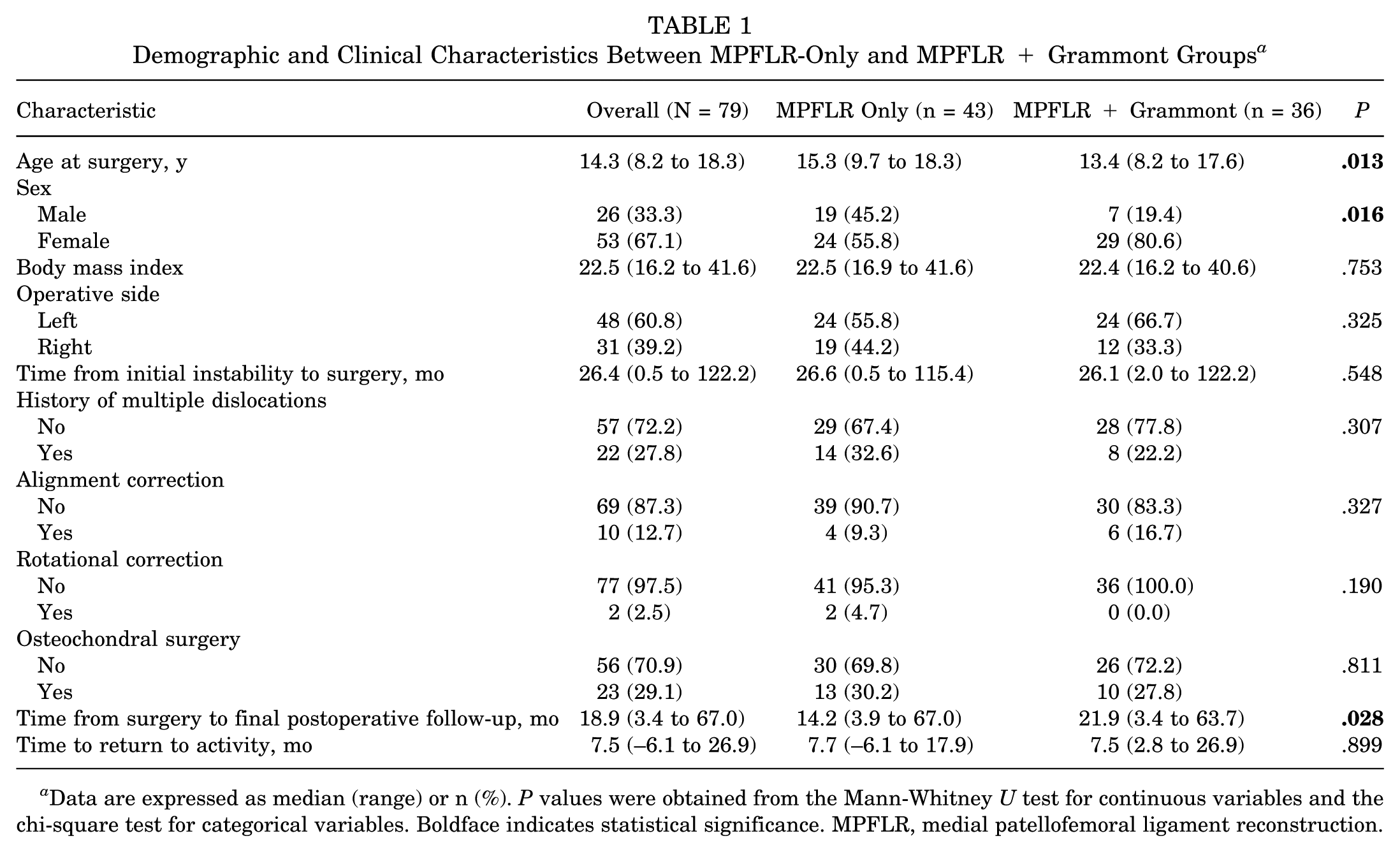
Data are expressed as median (range) or n (%). P values were obtained from the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables. Boldface indicates statistical significance. MPFLR, medial patellofemoral ligament reconstruction.
The median follow-up time for the entire cohort was 18.9 months (range, 3.4-67.0 months), and a significant difference was observed in the MPFLR + Grammont group (21.9 months) compared with the MPFLR-only group (14.2 months). Grade II or III complications occurred in 25.3% of patients (MPFLR, 27.9%; MPFLR + Grammont, 22.2%; P = .563) (Table 2). Recurrent instability was observed in 12 (15.2%) patients, with rates of 20.9% in the MPFLR-only group and 8.3% in the MPFLR + Grammont group (P = .120). Revision surgery for recurrent patellar instability was performed in 4 patients (9.3%) in the MPFLR-only group and 1 patient (2.8) in the MPFLR + Grammont group. Extension and flexion deficits occurred at similar rates in the MPFLR-only and MPFLR + Grammont groups (Table 2). In the MPFLR + Grammont group, 1 patient had a growth arrest of the tibial tubercle apophysis resulting in recurvatum deformity. Acquired valgus deformity occurred in 1 patient in the MPFLR + Grammont group.
Postoperative Complications a
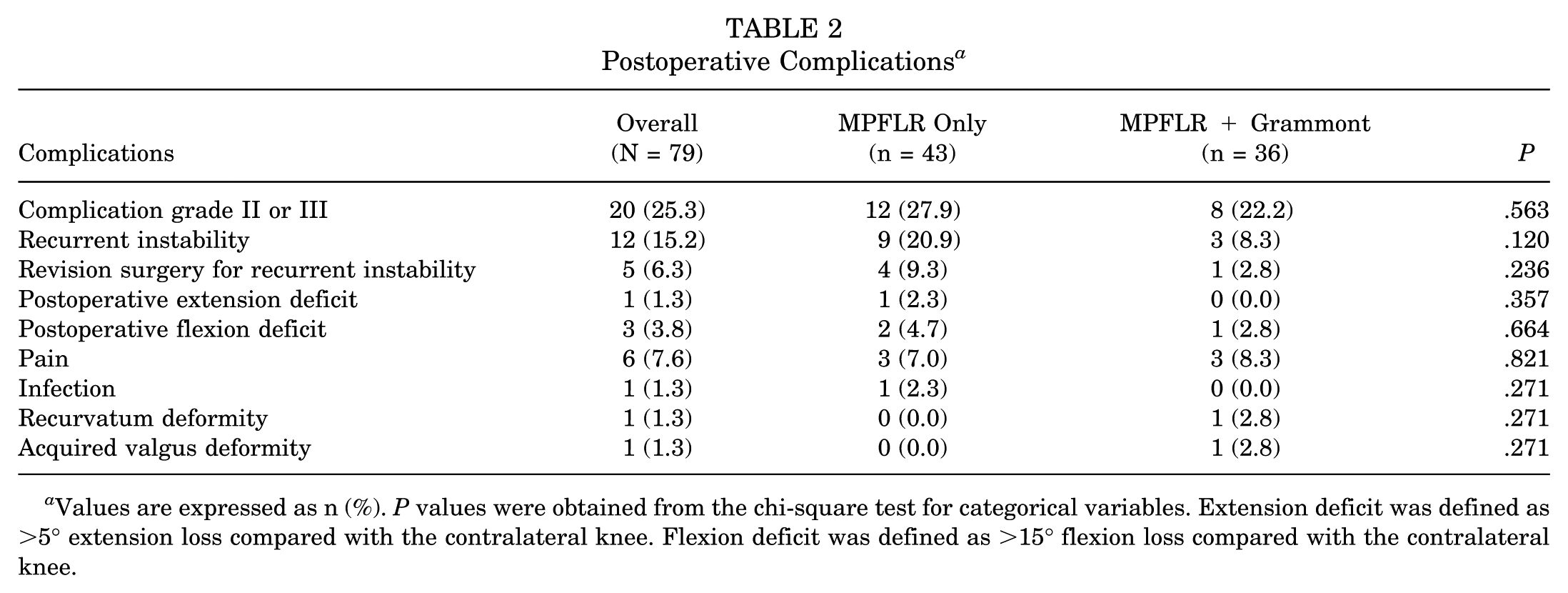
Values are expressed as n (%). P values were obtained from the chi-square test for categorical variables. Extension deficit was defined as >5° extension loss compared with the contralateral knee. Flexion deficit was defined as >15° flexion loss compared with the contralateral knee.
Preoperative TT-TG distance was significantly greater in the MPFLR + Grammont group (18.8 mm) compared with the MPFLR-only group (Table 3). Postoperative PTI-TG distance correction was greater in the MPFLR + Grammont group compared with the MPFLR-only group, but the difference was not statistically significant (Table 3). Final Caton-Deschamps ratio was significantly greater in the MPFLR + Grammont group (Table 3). Among patients stratified by Dejour classification, the rates of grade II/III complications were 38.9% for type A, 13.3% for type B, 14.3% for type C, and 75.0% for type D (P = .01) (Table 4). Interrater reliability of these measurements is shown in Table 5.
Preoperative and Postoperative Imaging Outcomes a
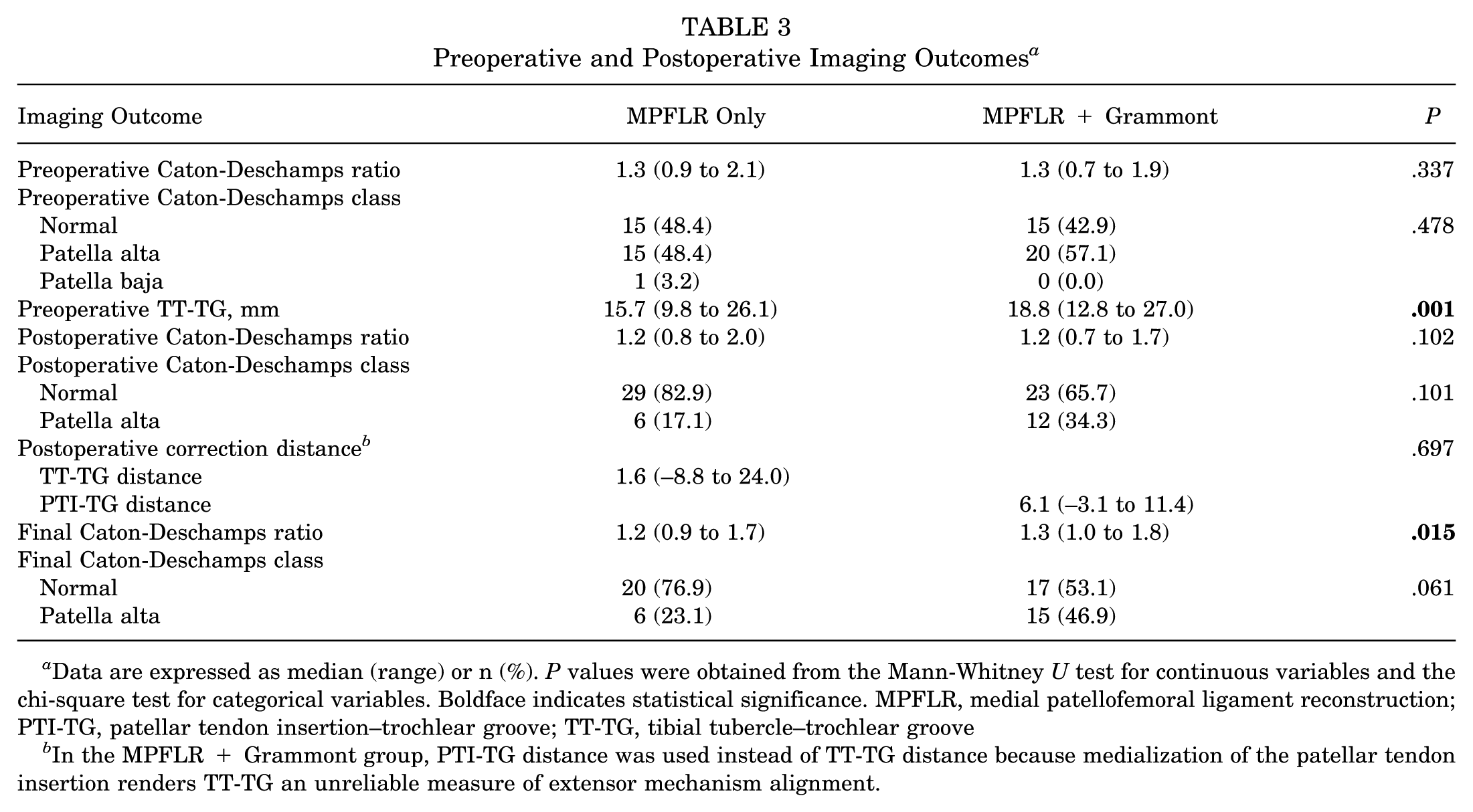
Data are expressed as median (range) or n (%). P values were obtained from the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables. Boldface indicates statistical significance. MPFLR, medial patellofemoral ligament reconstruction; PTI-TG, patellar tendon insertion–trochlear groove; TT-TG, tibial tubercle–trochlear groove
In the MPFLR + Grammont group, PTI-TG distance was used instead of TT-TG distance because medialization of the patellar tendon insertion renders TT-TG an unreliable measure of extensor mechanism alignment.
Complications vs Preoperative Dejour Classification a
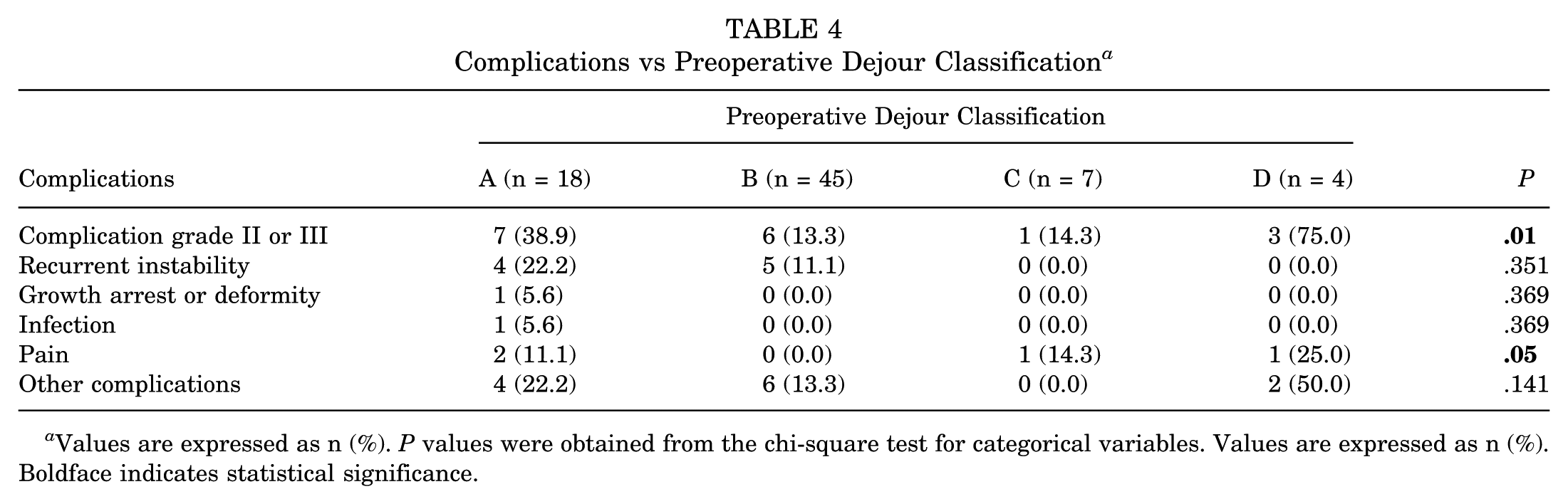
Values are expressed as n (%). P values were obtained from the chi-square test for categorical variables. Values are expressed as n (%). Boldface indicates statistical significance.
Interrater Reliability Between 4 Raters Using Intraclass Correlation Coefficient a
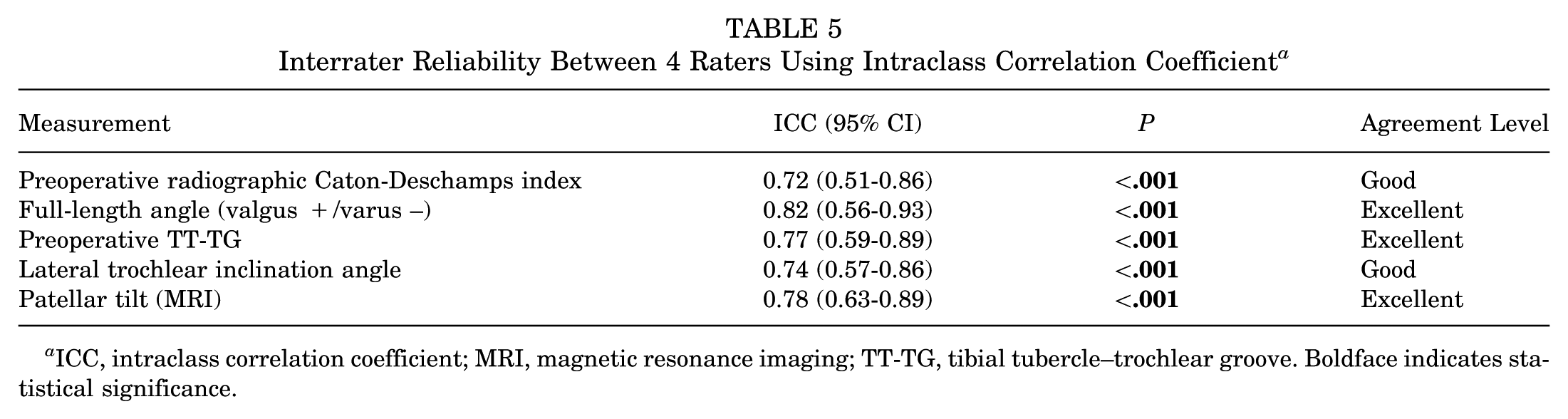
ICC, intraclass correlation coefficient; MRI, magnetic resonance imaging; TT-TG, tibial tubercle–trochlear groove. Boldface indicates statistical significance.
Discussion
The treatment of patellar instability in pediatric patients is challenging due to an increased risk of recurrence with nonoperative treatment combined with the surgical considerations when treating a pediatric population.9,21,22,32,48 We compared the outcomes of MPFLR alone versus MPFLR + Grammont in pediatric patients and found that the latter group had comparably favorable outcomes in terms of recurrent instability rates. Additionally, we found similar rates of overall complications and specifically a low rate of growth disturbance in both groups, albeit in a more complex patient population seen in the MPFLR + Grammont group with younger age and greater TT-TG distance preoperatively.
In pediatric patients undergoing surgical treatment, many techniques and modifications have been described to achieve proximal and distal patellar realignment and stabilization while protecting the distal femoral and proximal tibia physis and tibial tubercle apophysis.29,36,48 As techniques have evolved, physeal-sparing or physeal-protecting MPFLR has become the favored technique for restoring the medial ligamentous checkrein to lateral patellar instability.2,20,23,37,40 However, despite significant advancements in our understanding of MPFL anatomy and ability to perform anatomic reconstructions in the pediatric population, the rate of recurrent instability after isolated MPFLR in pediatric patients is reported between 7.0% to 20.5%. § This is significantly higher than reported rates of failure in adult MPFLR of 0.1% to 4.7%.35,49,51 Specifically, Husen et al 20 noted in their cohort of skeletally immature patients an overall recurrence rate after surgical stabilization of 13.9%. The rate of failure increased to 20.5% in patients who had isolated MPFLR. The authors concluded that failure of surgical treatment could be mitigated by combining MPFLR with TTO.
Lateralization of the attachment of the patellar tendon on the tibial tubercle, typically quantified by TT-TG, has been established as a biomechanical risk factor for patellar instability.6,9,13,34 In the adult population, TTO is often used to address increased TT-TG.13,25 However, in a skeletally immature patient, TTO carries the risk of growth arrest or disturbance of the proximal tibia, which can result in recurvatum, genu valgum, and/or patella baja.27,38,47 The Grammont procedure was originally described for distal patellar tendon medialization in combination with a Langenskiöld procedure (reconstructive soft tissue procedure) in the setting of congenital or fixed patellar dislocation.18,22,28,29 Recently, the Grammont procedure has been used as a physeal-protecting soft tissue realignment technique to address elevated TT-TG in idiopathic pediatric lateral patellar instability, with small series reporting on favorable outcomes and safety profile.22,28,50 Kraus et al 22 performed a modified Grammont without a concomitant medial stabilization (ie, MPFLR or medial plication) and reported an early redislocation rate of 12.3%. Wegmann et al 50 performed MPFLR with a modified Grammont on 7 knees with median TT-TG distance of 17 mm and reported no cases of recurrent dislocation at median 50 months postoperative. However, the efficacy and safety of MPFLR combined with Grammont procedure cannot be determined from these prior studies due to limitations of small sample sizes and lack of comparison groups.
From a technical standpoint, the Grammont procedure has a few key benefits over other distal realignment procedures. Compared with adult TTO, a soft tissue procedure poses less risk to the proximal tibial physis and apophysis. Additionally, the lack of osteotomy negates the risks of nonunion and hardware-related pain.26,39 Postoperative pain and risk of compartment syndrome are similarly decreased. Compared with other soft tissue–only procedures such as the Roux Goldthwait, the Grammont procedure does not require splitting or complete detachment of the patellar tendon attachment.8,16,25,33 Conversely, with the modified Grammont technique, actual medial translation of the patellar tendon insertion may be limited due to lack of medial fixation; with the Grammont technique used in the current study, the tendon was repositioned and secured medially using a suture anchor. It is also uncertain whether there is a risk of insufficiency of the distal patellar tendon attachment over time with this technique. Additionally, dissection of the patellar tendon off the tibial tuberosity still carries a risk of iatrogenic damage to the apophysis and proximal tibia growth arrest.
Our study aims to clarify some of these lingering questions regarding the safety and efficacy of the Grammont procedure by comparing isolated MPFLR versus MPFLR + Grammont. We found that the MPFLR + Grammont group was younger, with greater mean TT-TG distance compared with the isolated MPFLR group. This represents a high-risk group of patellar instability patients due to young age and combined biomechanical risk factors. 24 Overall, our cohort had a rate of postoperative instability (15.2%) comparable to what is reported in the literature. Although not statistically different, the rate was 8.3% in the MPFLR + Grammont group and 20.9% in the MPFLR-only group. Overall complications were similar between the 2 groups; however, the MPFLR + Grammont group had 1 case of recurvatum deformity that occurred due to arrest of the anterior proximal tibia physis. The patient was asymptomatic despite the deformity and was treated with observation. However, this finding highlights the need for close radiographic monitoring in these patients, with routine lateral knee or preferably full-length lateral extremity films. Caution should be exercised when applying this technique in younger patients with significant growth remaining and the highest risk of developing a clinically significant deformity in the setting of physeal injury. There was also 1 case of valgus deformity in the MPFLR + Grammont group. The patient was noted to have bilateral genu valgum deformity stemming from the distal femur, first noted approximately 2 years after MPFLR + Grammont surgery. Growth plates were noted to be open, and the patient underwent guided growth with complete resolution of valgus deformity. This is likely a case of acquired bilateral valgus rather than a case of growth disturbance secondary to surgery. However, given that we cannot completely exclude the latter possibility, the case was included as a complication. Given the response to guided growth, we can at least conclude that no growth arrest resulted from MPFLR surgery but we cannot rule out a growth disturbance or overgrowth occurring at the medial distal femur that led to the valgus deformity on the MPFLR-Grammont knee.
It remains unclear which patients may benefit most from the addition of the Grammont procedure. Unlike more established adult thresholds for surgical indications for TTO, elevated TT-TG distance in pediatric patients differs by age and sex.31,32 Generally, the TT-TG distance has been shown to increase gradually during growth, and therefore younger patients may have a lower threshold for what can be considered “tolerated” TT-TG distance. Further, an increasing body of evidence shows that in adult patients, MPFLR with or without TTO yields similar outcomes and rates of recurrence.12,14,35,44,49 This emphasizes that we are still in the infancy of our understanding of the complex interplay of factors contributing to patellar instability, specifically in the case of pediatric patients. Future directions require prospective randomized studies with large numbers of skeletally immature patients, followed to skeletal maturity, to confirm our findings and further investigate long-term outcomes. This study is the first to directly compare MPFLR with and without distal soft tissue realignment in a pediatric population. Complications, including persistent postoperative pain and any episodes of recurrent instability (including mild subluxation), were systematically documented. Growth disturbances were also evaluated by comparing pre- and postoperative full-length radiographs.
The modified Grammont procedure shares similarities with the historical Hauser procedure in that both aim to correct recurrent patellar instability by altering the vector of the patellar tendon. 19 The Hauser procedure was developed in 1938; a bone block containing the tibial tubercle and patellar tendon insertion is osteotomized and repositioned through a window in the proximal tibia, resulting in a fixed medial and posterior transfer designed to counteract abnormal lateralizing forces on the patella.10,19 Although long-term follow-up studies reported satisfactory outcomes in approximately 70% of patients, with some series extending beyond 30 years, the procedure was ultimately abandoned due to an unacceptably high complication profile.3,5,10 Reported complications included higher overall complication rates compared with alternative techniques, persistent instability in a subset of patients, patella baja, loss of extensor mechanism efficiency related to a reverse Maquet effect, and high rates of patellofemoral arthrosis at long-term follow-up.3,5,10 Additional concerns included genu recurvatum when performed before epiphyseal closure, particularly relevant in pediatric populations.3,5,10 In contrast, the Grammont procedure avoids TTO and bone block fixation, relying instead on soft tissue mobilization of the patellar tendon, thereby preserving tendon length and avoiding rigid posterior or distal transfer. Additionally, this spares the tibial tubercle apophysis from potential injury (although as noted in this study, growth arrest is still possible). These differences may reduce the risk of patella baja, excessive patellofemoral contact pressures, arthritis rates, and long-term extensor mechanism dysfunction. Although the shared principle of modifying patellar tendon alignment warrants careful long-term surveillance, the absence of a fixed bony transfer and the more physiologic, dynamic nature of the Grammont procedure suggest a lower likelihood of reproducing the deleterious patellofemoral mechanics historically associated with the Hauser procedure. This is an area that warrants further study and long-term follow-up.
Limitations
There are several limitations to this study inherent to its retrospective design. The study had a modest sample size, with 43 patients in the MPFLR-only group and 36 in the MPFLR + Grammont group. Selection bias may have been present as patients were not randomized, and there were no standardized criteria for selecting MPFLR alone versus MPFLR + Grammont. The MPFLR-only and MPFLR + Grammont groups were not fully equivalent with respect to age, sex distribution, patella alta, and TT-TG distance, which may have introduced confounding factors. This was a single-center experience, and the findings may not be generalizable. Patients up to 19 years of age were included without assessment of skeletal maturity (eg, Risser stage), which may introduce heterogeneity and affect generalizability of our findings. The follow-up period in this study was relatively short, and follow-up was done retrospectively through chart review. This may have limited the ability to detect late complications or longer term outcomes after surgery. In addition, formal standardized postoperative follow-up evaluations were not performed, and outcomes were therefore based on available clinical and radiographic data. Blinding to pre- versus postoperative status was not feasible, which may have introduced measurement bias during radiographic data collection. Interrater reliability testing was limited to the preoperative variables. As a result, postoperative measurements were not included in the reliability analysis. No postoperative functional testing was conducted, including objective strength or extensor mechanism testing; as a result, potential changes in extensor torque generation after posterior transfer of the patellar tendon could not be directly assessed and should be considered when interpreting the findings. We were unable to reliably calculate potential posterior displacement of the patellar tendon insertion after the Grammont procedure. On a number of patients’ MRI scans, we noted remodeling and medialization of the tibial tubercle apophysis after the Grammont procedure. This finding would benefit from longer term MRI follow-up; further, the potential for patellofemoral compartment degeneration after Grammont was outside the scope of this particular study. A limited number of patients underwent postoperative MRI (17/79) and usually only in the setting of recurrent instability or persistent pain. Therefore, the true amount of patellar tendon medialization achieved with the Grammont technique is unclear.
Conclusion
In this retrospective cohort study, we observed similar rates of success and a comparable complication profile, with low risk of growth disturbance, when MPFLR was combined with a Grammont procedure in pediatric patients with patellar instability and an increased TT-TG distance. Although further investigation is needed to determine the biomechanical and anatomic thresholds and the ideal patient population for its application, this technique has the potential to enhance surgical outcomes and reduce the rates of recurrent postoperative patellar instability in carefully selected pediatric patients.
Footnotes
Final revision submitted January 29, 2026; accepted February 16, 2026.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB approval for this study was obtained from Children's National.