
Abstract
Background:
Psychological factors influence return to sport (RTS) and reinjury rates following anterior cruciate ligament (ACL) reconstruction (ACLR). However, many RTS decisions are made without considering psychological factors, or consider psychological and physical factors in isolation, leading to suboptimal RTS and reinjury rates.
Purpose:
To identify distinct profiles of psychological and physical readiness to RTS following ACLR using strength- and performance-based measures of physical readiness and to examine the extent to which these readiness domains align.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Data from the ACL Reconstruction Rehabilitation Outcomes Workgroup (ARROW) registry were used to construct patient profiles of psychological and physical readiness to RTS based on established criteria. Psychological readiness was defined by an ACL Return to Sport after Injury Scale (ACL-RSI) score ≥65 points out of 100. Strength-based and performance-based physical readiness was defined by a limb symmetry index ≥90% in isokinetic quadriceps strength and single-limb hop testing, respectively. Frequencies of all profiles were reported, alignment between psychological and physical domains was assessed, and sensitivity analyses were conducted to investigate differences in age, sex, and time since surgery.
Results:
A total of 822 patients were included in the analysis (age: mean ± SD, 18.8 ± 6.2 years; 51% female). The most common profile represented patients who met psychological (ACL-RSI) and performance-based physical readiness criteria (single-leg hop) but not strength-based physical readiness criteria (quadriceps strength) (32%; 261/822). When considering ACL-RSI, single-leg hop, and quadriceps criteria together, psychological and physical readiness did not align for 69% (571/822) of patients. Patients in the “neither psychologically nor physically ready” profile were older than patients in any other profiles. Male patients obtained psychological and physical readiness scores that aligned more often than female patients.
Conclusion:
There were a variety of distinct profiles of psychological and physical readiness in patients post-ACLR. Psychological, strength-based, and performance-based physical readiness to RTS criteria aligned for less than one-third of participants. Patients who did not meet psychological or physical readiness criteria tended to be older in age, and male patients were more likely to have alignment between their psychological and physical readiness domains.
The importance of psychological factors in anterior cruciate ligament (ACL) reconstruction (ACLR) rehabilitation is increasingly recognized. Measures of psychological readiness are now commonly recommended in addition to traditional objective return to sport (RTS) criteria such as lack of swelling, full range of motion, acceptable strength, and hop performance outcomes.12,16,19,33 While clear associations between psychological factors and secondary injury rates post-ACLR have been identified,2,17,27,37 implementation of psychological measures in post-ACLR assessment remains limited and inconsistent. A systematic review published in 2023 found that 5 of 47 studies (11%) included psychological testing within RTS criteria. 26
Following ACLR, the ACL Return to Sport after Injury (ACL-RSI) scale is the most used measure of psychological readiness. A network meta-analysis of 12 studies using RTS criteria post-ACLR indicated ACL-RSI as the most effective criterion for predicting RTS success (effect size, 1.55; 95% CI, 1.24-1.87), with physical tests only being moderately effective. 15 However, this meta-analysis of previous work assessed each criteria in isolation and the authors advocate for an integrated model combining physical and psychological domains. 15 Common physical outcomes in RTS testing batteries include isokinetic or isometric quadriceps and hamstrings strength, countermovement or drop jump, and single-leg hopping. A meta-analysis of 8 studies reported a full RTS testing battery pass rate of 23% (95% CI, 8%-43%; range, 0%-79%) across 876 patients 5 to 10 months post-ACLR. 34 The low and variable RTS testing pass rates indicate considerable disagreement between the components of RTS criteria. There is no single gold standard measure of physical readiness to RTS following ACLR, likely because there are multiple components or types of physical readiness necessary for successful RTS.
The World Health Organization's International Classification of Functioning, Disability and Health (ICF model) 29 is a framework for measuring health and disability organized into the following categories: body structures and function, activity and function, participation and motivation, environmental factors, and personal factors. This model can be mapped onto ACL RTS testing batteries to improve our understanding of individual patient health, disability, and functioning in an ACL rehabilitation–specific context. For example, tests such as quadriceps strength and single-leg hop performance would fall under the body structures/function and activity/function categories of the ICF model, respectively, representing strength-based and performance-based measures of physical readiness to RTS. It is possible that creating a composite patient profile through the addition of psychological factors (ie, personal factors within the ICF model) to the traditionally assessed physical components of RTS criteria could improve our understanding of individual patient readiness to RTS (ie, participation and motivation component of ICF model).
Therefore, the purpose of this study was to identify distinct profiles of psychological and physical readiness to RTS following ACLR, using both strength- and performance-based measures of physical readiness, and to examine the extent to which these readiness domains align at the individual level. Further, we aimed to investigate whether profiles and alignment of readiness domains differed by age, sex, or time since surgery. We hypothesized that the distribution of patient profiles would differ depending on the physical readiness outcome used and that physical and psychological readiness would not align for a significant proportion of patients.
Methods
This was a multisite study from the ACL Reconstruction Rehabilitation Outcomes Workgroup (ARROW) registry. The ARROW registry combines data from 9 sites across the Midwest, Northeast, and Southeast regions of the United States, representing university, hospital, and research settings, with the primary goal to improve patient care following ACLR. Institutional review board approval was obtained for data collection at each site and for the aggregated registry managed by study team members at the University of Virginia.
Patients
Patients were included if they had been seen for post-ACLR testing at a participating ARROW site 5 to 13 months postoperatively and completed the ACL-RSI, isokinetic quadriceps strength testing, and single-leg hop testing. Four participating sites collected all the required variables and were included in the study. If data were collected from a patient at multiple time points, their most recent (latest postoperative) testing data were included for analysis. Patients of all ages (range, 13-62) and those with concomitant meniscal injuries/treatment were included in the analysis. Patients with a previous history of ACLR were excluded. Descriptive information including demographics, surgical information, time since surgery, and knee symptoms and function as measured by the International Knee Documentation Subjective Knee Form (IKDC) or pediatric IKDC (Pedi-IKDC) scores were collected for all patients. The IKDC was collected for patients ≥18, and the Pedi-IKDC was collected for patients <18 years old. The Pedi-IKDC is a modified version of the IKDC developed for use in children and adolescents aged 10 to 18. 10 The Pedi-IKDC is valid, reliable, and responsive for use with pediatric patients with a variety of knee injuries 10 and highly correlated with the IKDC questionnaire. 24
Psychological Readiness to RTS
The ACL-RSI was used as the psychological readiness measure for this study, representing personal factors within the ICF model. The ACL-RSI is a 12-item questionnaire developed to measure psychological readiness to RTS after ACLR in 3 domains: emotions, confidence, and risk appraisal. 32 The ACL-RSI is scored from 0 points (indicating an extremely negative psychological response and lack of readiness to RTS) to 100 points (indicating no negative psychological responses and readiness to RTS). 32 The ACL-RSI has demonstrated good internal consistency, reliability, structural validity, and construct validity via hypothesis testing for patients with ACL injuries. 8 The ACL-RSI is one of the only patient-reported outcome measures with positive evidence of content validity specifically for patients after ACL injury or reconstruction. 8 Patients were defined as being “psychologically ready” if they scored ≥65 points on the ACL-RSI (out of 100). ACL-RSI score ≥65 has been used as a threshold to represent appropriate psychological response22,23,27,31 and has been linked to 1-year 31 and 2-year 22 RTS outcomes for patients post-ACLR.
Physical Readiness to RTS
Using the ICF model, 2 types of physical readiness outcomes were chosen to create RTS profiles for each participant: (1) strength-based physical readiness as measured by the limb symmetry index (LSI) for isokinetic quadriceps strength at 60 deg/s and (2) performance-based physical readiness as measured by the LSI for single-leg hop for distance.
Isokinetic testing is considered the gold standard for strength testing after ACLR, 36 and 60 deg/s has been indicated as the optimal speed to assess quadriceps strength and identify side-to-side differences in limb strength postoperatively.7,12,14 Instrumented strength testing was conducted at each ARROW site by a licensed physical therapist, athletic trainer, or trained graduate researcher using a HUMAC Norm (Computer Sports Medicine), or Biodex System 3 or 4 Pro (Biodex Medical Systems). Good interdevice agreement has been shown between HUMAC and Biodex dynamometers. 4 Participants completed quadriceps strength testing seated at 90° of hip flexion with the dynamometer arm secured proximal to the ankle joint. Both limbs were tested, starting with the nonoperative limb. After warm-up trials, the testing consisted of 5 maximal effort trials completed at 60 deg/s through a range of motion from 90° to 0° of knee flexion.28,30 Maximal peak torque in N·m for knee extension were recorded.
Single-leg hop testing is a standard sport task used in most RTS testing batteries following ACLR.12,33 Hop testing was conducted at each ARROW site by a licensed physical therapist, athletic trainer, or trained graduate researcher. Patients were asked to hop on 1 leg as far as they could with a controlled landing (ie, without loss of stability on the hopping leg), and this was repeated for both limbs. The distance hopped in meters was recorded and a mean of 3 trials was taken.
For both the strength and the hop-testing physical readiness outcomes, patients were defined as being “physically ready” if their LSI was ≥90%. This cutoff is widely accepted for both quadriceps strength and single-leg hop tests as important RTS criteria following ACLR.12,14,34 LSIs were calculated as [peak quadriceps torque or mean hop distance ACLR limb]/[peak quadriceps torque or mean hop distance nonoperative limb] × 100.
Profile Construction
Readiness profiles were then created to categorize patients by their physical and psychological readiness to RTS based on the aforementioned criteria. Three sets of profiles were constructed: (1) psychological and strength-based physical readiness (using ACL-RSI and quadriceps strength), (2) psychological and performance-based physical readiness (using ACL-RSI and single-leg hop testing), (3) psychological and combined (strength- and performance-based) physical readiness (using ACL-RSI, quadriceps strength, and single-leg hop testing) as outlined in Table 1.
Patient Readiness Profiles a
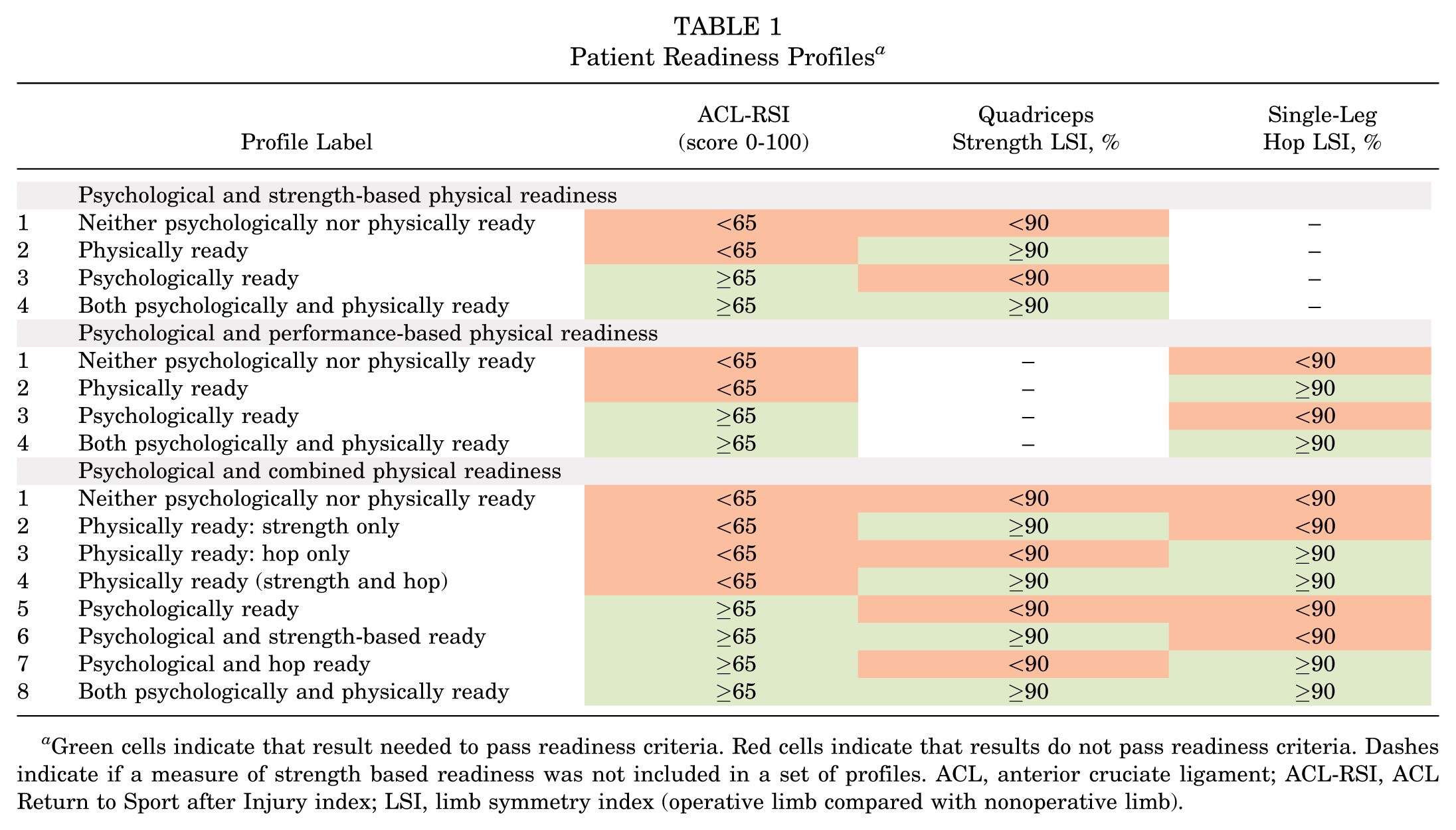
Green cells indicate that result needed to pass readiness criteria. Red cells indicate that results do not pass readiness criteria. Dashes indicate if a measure of strength based readiness was not included in a set of profiles. ACL, anterior cruciate ligament; ACL-RSI, ACL Return to Sport after Injury index; LSI, limb symmetry index (operative limb compared with nonoperative limb).
Statistical Analysis
Descriptive statistics (means, standard deviations, and frequencies) were calculated for demographics and psychological/physical readiness variables. The frequency of each profile was calculated using the categories displayed in Table 1. The distribution of psychological and physical readiness was examined for each set of profiles (ie, strength based, performance based, or combined physical readiness). The alignment between psychological and physical readiness was determined by the proportion of patients who were “neither psychologically nor physically ready” and “both psychologically and physically ready” within each set of profiles. To avoid misleading estimations of psychological/physical domain alignment based on borderline scores (eg, a patient's psychological and strength-based physical readiness being categorized as not aligned when scoring 64 on the ACL-RSI and 91% on quadriceps strength), a sensitivity analysis was performed excluding patients with scores within 5 points or 5% of the threshold value in either direction (ie, 60-70 points on ACL-RSI and 85%-95% LSI for hop or strength tests). The relationship between each of the 3 readiness criteria were also investigated with pairwise Pearson correlation coefficients, whereby the relationships between variables were interpreted as none (r < 0.1), weak (r = 0.10-0.39), moderate (r = 0.40-0.69), strong (r = 0.70-0.99), or perfect (r = 1.00). 1
Finally, a sensitivity analysis was conducted to investigate differences in age, sex, and time since surgery between the patients categorized to each profile and between the groups of patients whose psychological and physical readiness did/did not align. Age- and time since surgery–based differences across readiness profiles were investigated using a 1-way analysis of variance (ANOVA), while sex-based differences were assessed using a chi-square test of independence (χ2). To understand significant differences between profiles and groups, Bonferroni post hoc tests were used for the ANOVA analyses, and standardized residuals were calculated for the χ2 analyses. For the χ2 test, groups with standardized residuals >1.96 were identified as having significantly different counts than expected and contributing to the overall significance. Statistical significance was set at P < .05. All statistical analyses were conducted using StataNow/BE Version 19.5
Results
A total of 822 participants (18.8 ± 6.2 years old; 51.1% female; 7.6 ± 1.8 months from surgery) were included in the analysis (Table 2). Using the established cutoffs for the ACL-RSI score, isokinetic quadriceps strength, and single-leg hop distance, 70% (577/822), 29% (242/822), and 67% (551/822) of participants passed each of these readiness criteria, respectively (Table 2).
Patient Demographics and Outcome Measures (N = 822) a
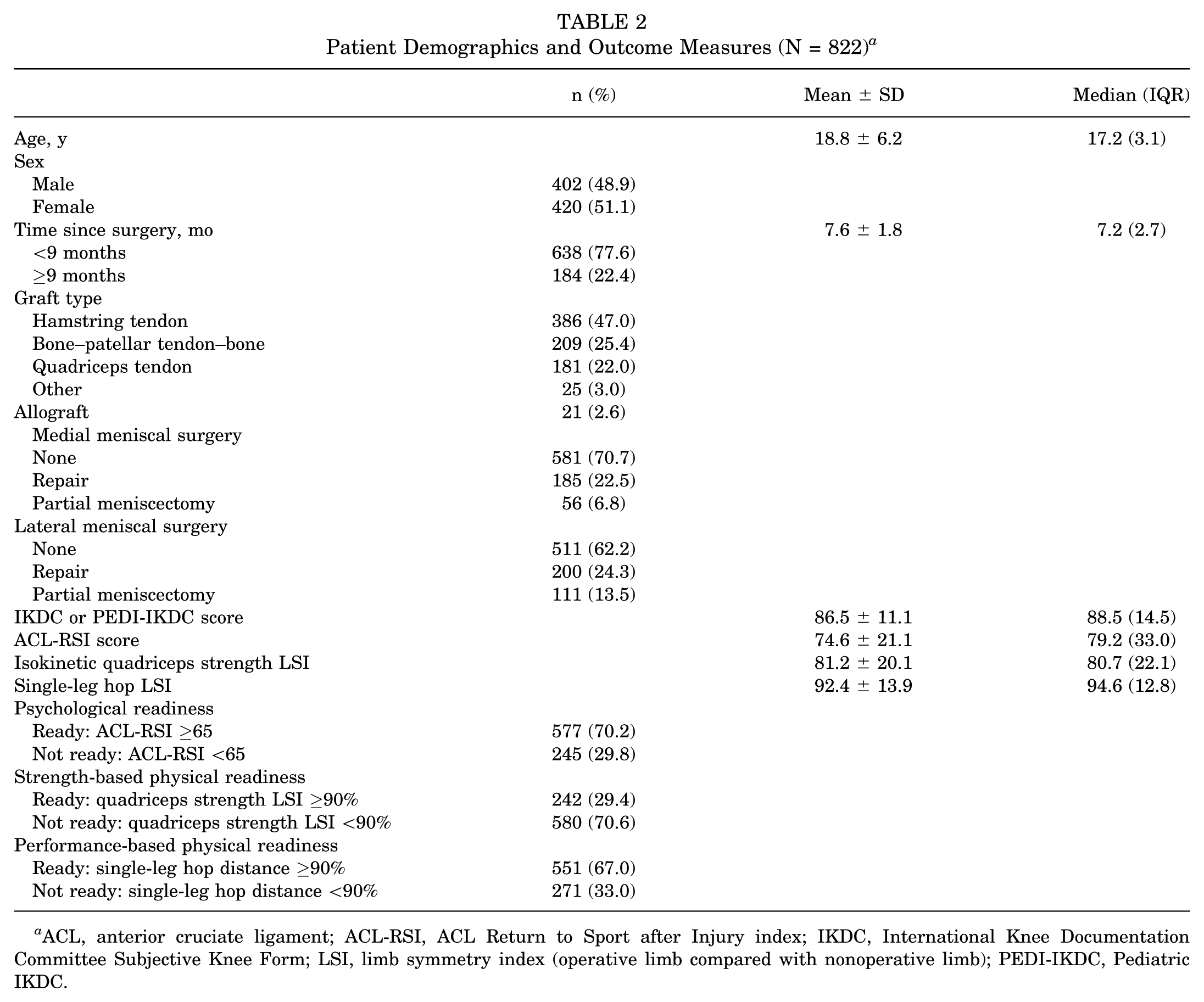
ACL, anterior cruciate ligament; ACL-RSI, ACL Return to Sport after Injury index; IKDC, International Knee Documentation Committee Subjective Knee Form; LSI, limb symmetry index (operative limb compared with nonoperative limb); PEDI-IKDC, Pediatric IKDC.
Figure 1 depicts the proportion of patients categorized into each readiness profile. In the psychological and strength-based physical readiness profile (Figure 1A), the most common readiness profile included patients who were psychologically but not physically ready (385/822; 47%). In the psychological and performance-based physical readiness profiles (Figure 1B), the most common readiness profile included patients who were both psychologically and physically ready (416/822; 51%). In the combined profiles (Figure 1C), psychologically and hop ready had the highest prevalence (261/822; 32%). Approximately 12% (96/822) of patients did not meet any of the 3 readiness criteria (neither psychologically nor physically ready) (Figure 1C).

Distribution of patient profiles representing readiness to return to sport following anterior cruciate ligament reconstruction (N = 822). (A) Psychological and strength-based physical readiness profiles; (B) psychological and performance-based physical readiness profiles; (C) psychological and combined physical readiness profiles.
The proportion of patients for which psychological and physical readiness criteria aligned was largest in the psychological and performance-based physical readiness profiles (526/822; 64%), followed by the psychological and strength-based physical readiness profiles (387/822; 47%) and psychological and combined physical readiness profiles (251/822; 30.5%) (Figure 2). The proportion of domain alignment was similar for psychological and performance-based physical readiness (351/504; 70%), psychological and strength-based physical readiness (272/579; 47%), and psychological and combined physical readiness (147/409; 36%) when borderline ready/not ready scores were removed. Further, pairwise Pearson correlation coefficients suggested a significant but weak relationship between ACL-RSI scores and single-leg hop LSI values (r = 0.28; P < .01), and quadriceps strength LSI (r = 0.19; P < .01), suggesting that while these outcomes are related, the magnitude of agreement between psychological and physical outcomes is not strong. The association between the 2 physical readiness outcomes, hop and strength LSI values, was stronger but still weak (r = 0.36; P < .01).

Alignment between psychological and physical readiness to return-to-sport criteria in patients following anterior cruciate ligament reconstruction, stratified by profile set/type of physical readiness measure used (N = 822).
There were consistent age-based differences across readiness profiles (Tables 3 and 4). For all 3 sets of profiles, patients categorized as neither psychologically nor physically ready (labeled as profile 1) were the oldest and patients categorized as both psychologically and physically ready (labeled as profile 4 or 8) were the youngest. The patients in the least ready profile were significantly older than patients in almost all the other profiles (P < .05) (Tables 3 and 4).
Differences in Age, Sex, and Time Since Surgery Between Patient Readiness Profiles Using Either Strength-Based or Performance-Based Physical Readiness Measures a
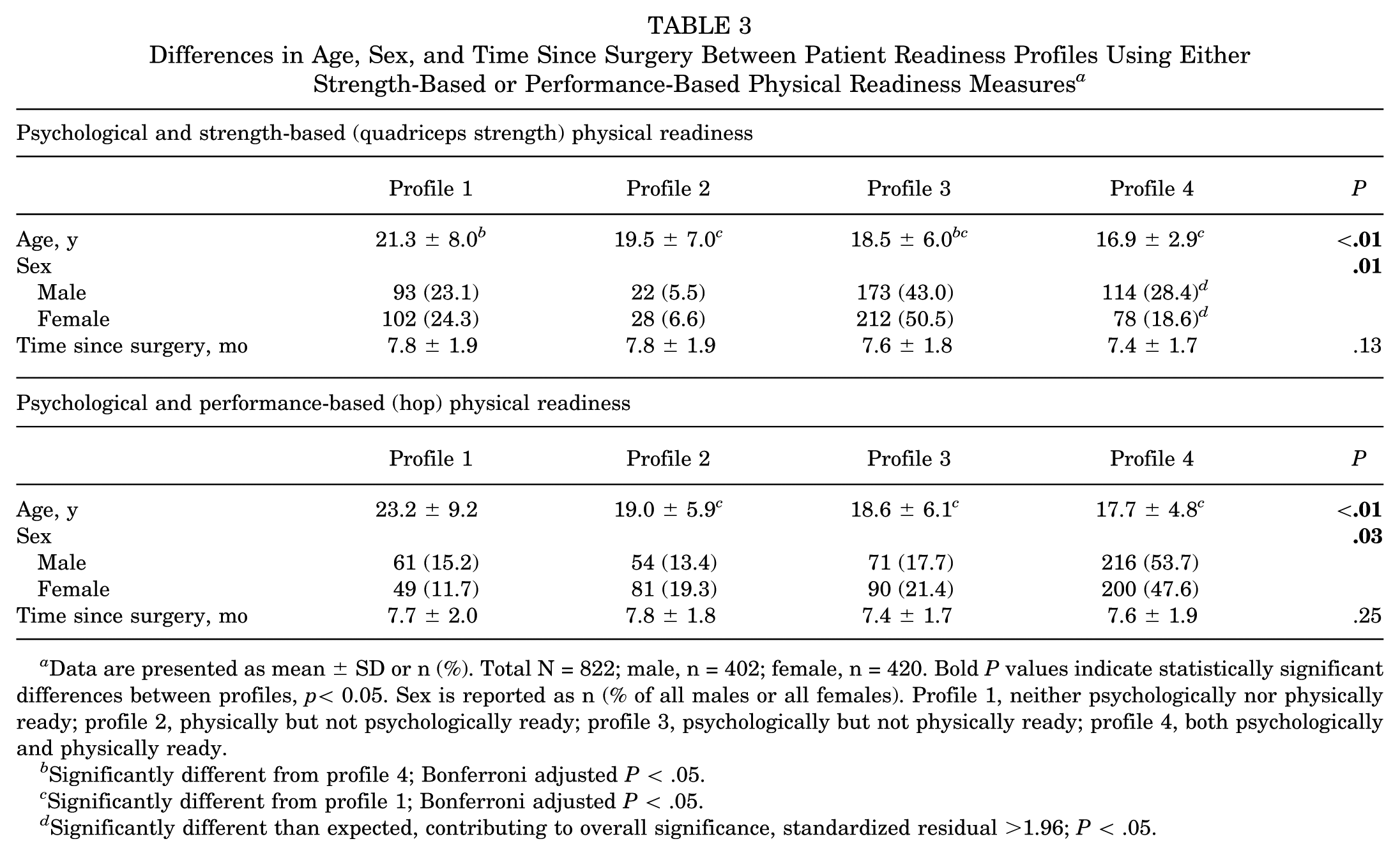
Data are presented as mean ± SD or n (%). Total N = 822; male, n = 402; female, n = 420. Bold P values indicate statistically significant differences between profiles, p< 0.05. Sex is reported as n (% of all males or all females). Profile 1, neither psychologically nor physically ready; profile 2, physically but not psychologically ready; profile 3, psychologically but not physically ready; profile 4, both psychologically and physically ready.
Significantly different from profile 4; Bonferroni adjusted P < .05.
Significantly different from profile 1; Bonferroni adjusted P < .05.
Significantly different than expected, contributing to overall significance, standardized residual >1.96; P < .05.
Differences in Age, Sex, and Time Since Surgery Between Patient Readiness Profiles Using Both Strength-Based and Performance-Based Physical Readiness Measures a
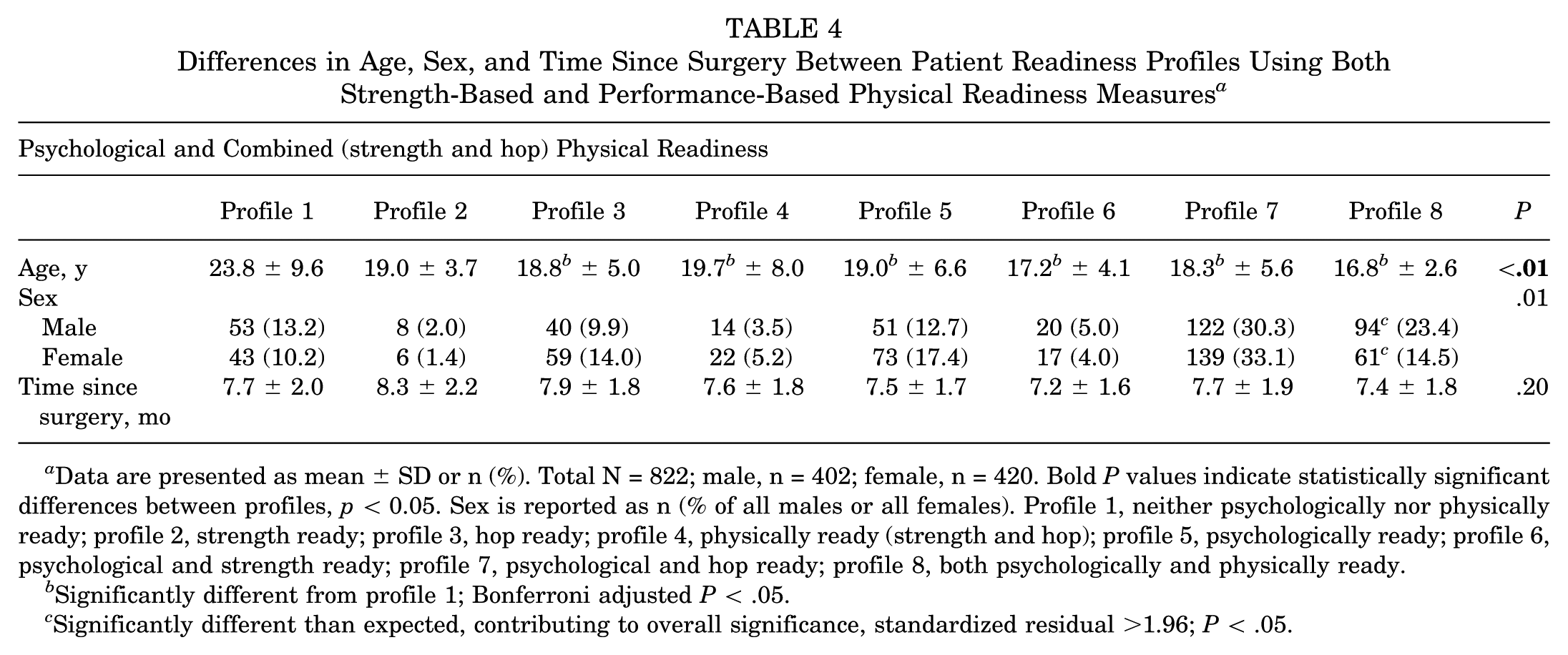
Data are presented as mean ± SD or n (%). Total N = 822; male, n = 402; female, n = 420. Bold P values indicate statistically significant differences between profiles, p < 0.05. Sex is reported as n (% of all males or all females). Profile 1, neither psychologically nor physically ready; profile 2, strength ready; profile 3, hop ready; profile 4, physically ready (strength and hop); profile 5, psychologically ready; profile 6, psychological and strength ready; profile 7, psychological and hop ready; profile 8, both psychologically and physically ready.
Significantly different from profile 1; Bonferroni adjusted P < .05.
Significantly different than expected, contributing to overall significance, standardized residual >1.96; P < .05.
When comparing alignment in psychological and physical readiness criteria, male patients tended to be overrepresented in the aligned group (Table 5). When combining the ACL-RSI, strength, and hop criteria, there were significantly more male patients and fewer female patients in the aligned group than expected (standardized residual, >1.96) (Table 5). There were no significant differences in time since surgery across any set of readiness profiles or between aligned/not aligned readiness groups (Tables 3-5).
Differences in Age, Sex, and Time Since Surgery Between Patients Whose Psychological and Physical Readiness Did and Did Not Align a
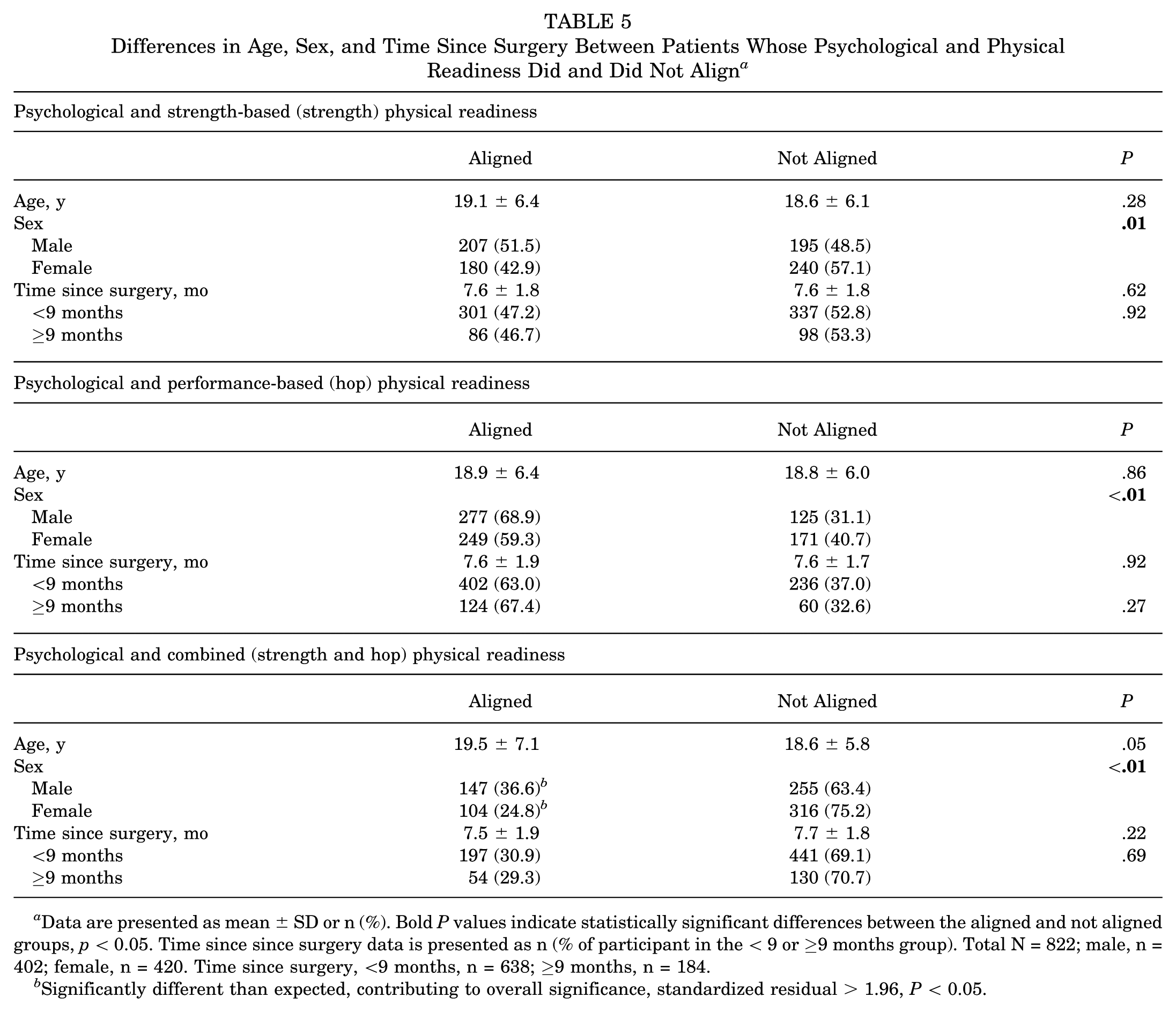
Data are presented as mean ± SD or n (%). Bold P values indicate statistically significant differences between the aligned and not aligned groups, p < 0.05. Time since since surgery data is presented as n (% of participant in the < 9 or ≥9 months group). Total N = 822; male, n = 402; female, n = 420. Time since surgery, <9 months, n = 638; ≥9 months, n = 184.
Significantly different than expected, contributing to overall significance, standardized residual > 1.96, P < 0.05.
Discussion
The primary finding of this study was that patients exhibit varying profiles of physical and psychological readiness to RTS post-ACLR, with patients commonly passing either psychological or physical readiness criteria, but not both. This study also indicated important age- and sex-based differences in readiness profiles. We observed that being later in rehabilitation was not significantly associated with more favorable patient readiness profiles. These findings contrast with the commonly held belief that with proper treatment and care, psychological and physical readiness will improve continually across the ACL recovery timeline.
The distribution of the patient readiness profiles revealed inconsistency in outcomes post-ACLR as well as important discrepancies in the pass rates of objective RTS criteria. Only 29% of patients met or surpassed the quadriceps strength criterion while 67% passed the single-leg hop LSI threshold to RTS. This pattern is similar to that observed in other studies investigating RTS criteria post-ACLR in which suboptimal rates of passing quadriceps strength testing has been observed.14,35 A study by Thompson and colleagues 25 reported disagreements in pass rates between isokinetic quadriceps strength testing at 90 deg/s and single-leg hop testing in 36.5% of the sample. The disagreement rate between isokinetic strength testing at 60 deg/s and single-leg hop testing in the current study was 50% (411/822 patients), with 88% (360/411) of those disagreements being a passed hop test and failed quadriceps strength test. Only 6% (51/822) of the entire sample in the current study passed the quadriceps strength RTS criteria but failed to meet the single-leg hop test criterion. These results suggest that isokinetic quadriceps strength may be a more difficult physical readiness assessment to pass following ACLR than single-leg hop performance and that these tests measure distinct constructs of physical readiness.
In addition to the disagreement between physical outcome measures, an important amount of misalignment between psychological and physical readiness was observed. Depending on the profiles used, 36% to 69% of patients showed misalignment between these criteria. If ACL-RSI, isokinetic quadriceps strength, and single-leg hop distance are used as RTS criteria, almost 70% of patients will have disagreement between the interpretation of psychological readiness and ≥1 measure of physical readiness. This discrepancy appears to be driven by the low pass rate of the quadriceps strength testing. Of the 571 patients with misaligned psychological and physical readiness outcomes in the psychological and combined physical readiness profiles, 82.7% (472/571), 30.6% (175/571), and 26.1% (149/571) did not pass quadriceps strength, single-leg hop, and ACL-RSI readiness criteria, respectively.
As such, this study emphasizes the need for well-rounded RTS testing, and the use of composite decision-making tools that combine different types of physical and psychological measures to create a full picture of the patient's status and identify important discrepancies. The ARROW group has created a clinician dashboard that could be one such tool. The ARROW ACL Dashboard (https://acldashboard.com/) allows clinicians to enter patient demographics, strength, hop performance, self-reported function (IKDC/Pedi-IKDC), and psychological readiness to RTS (ACL-RSI) and to visualize an individual patient's outcomes compared with all other patients in the data set, or to patients of similar age, sex, graft source, and time from surgery. 13 Using this dashboard, clinicians could identify what profile defined in the current study their patients fit into, whether their psychological outcomes make sense within the context of their physical outcomes (ie, an adaptive or maladaptive response), and use this information to guide treatment and RTS decisions.
It is crucial to understand adaptive (ie, favorable) versus maladaptive (ie, unfavorable) psychological responses during the RTS phase post-ACLR 3 and to interpret psychological outcomes concurrently with physical outcomes, to understand whether the observed responses are appropriate for the specific patient being assessed. For example, consider a patient who is 5 months post-ACLR with a 60% LSI for quadriceps strength and single-leg hop testing. A low ACL-RSI score (<65) would indicate an appropriate psychological response to injury for this patient given his or her physical functioning and current stage of rehabilitation, suggesting the athlete has adapted a realistic perception of one's current readiness to participate in sport. In contrast, a high ACL-RSI score (≥65) would be inappropriate at this stage of recovery and may indicate a maladaptive response that could result in risk taking and overconfidence. For comparison, if a patient 18 months post-ACLR has excellent physical performance and has been functionally cleared to RTS, a low ACL-RSI score would indicate an inappropriate response and potentially maladaptive fear or anxiety, whereas a high score would be appropriate/adaptive in this context. In both maladaptive cases, there may be an associated increase in secondary injury risk RTS due to the misalignment between psychological and physical outcomes.
Across all analyses, patients categorized to profiles indicating they were neither psychologically nor physically ready to RTS were older than those with other readiness profiles. Previous work has shown that adult patients may experience more barriers throughout rehabilitation following ACLR including life transitions, modified activities and priorities away from competitive sport, decreased access to care or sport opportunities, and financial and time burdens.5,6,21 Each of these factors could contribute to lower physical and psychological readiness to RTS. Lower psychological readiness, measured by the ACL-RSI score, has been reported for adult patients compared with adolescents across multiple samples.11,18,21,38 A recent study by Roman and colleagues 21 further investigated age differences across the individual items of the ACL-RSI and its 3 subscales: confidence, emotions, and risk appraisal. The results of that study indicated that teenagers (mean ± SD age, 16.1 ± 1.1 years) had significantly higher ACL-RSI total scores and significantly higher confidence subscale scores compared with adults (mean ± SD age, 22.8 ± 3.1 years); however, there were no age-based differences in the emotion or risk appraisal scales. Roman and colleagues cautioned clinicians to be aware of higher ACL-RSI scores in teens, as confidence levels that are disproportionately high compared with physical performance measures could result in poor outcomes. Further, the study by Roman and colleagues provides insight that total ACL-RSI scores might be inflated by high levels of confidence and potentially mask less favorable emotional responses or risk appraisals. 21
There was a larger proportion of male participants whose psychological and physical readiness aligned (either not ready in either category or ready in both categories) compared with their female counterparts. Other studies that have observed lower psychological and physical readiness to RTS following ACLR in female compared with male patients 9 including worse quadriceps atrophy, 20 worse knee extension and flexion strength, 9 and lower ACL-RSI scores.11,18,38 Therefore, we would expect the sex difference to be driven by a larger proportion of male participants who were both psychologically and physically ready. While this was observed in our sample, there was also a larger proportion of male patients who were neither psychologically nor physically ready and larger proportions of female patients with mixed readiness. As such, further research is needed to understand how we might better align psychological and physical RTS criteria for female athletes.
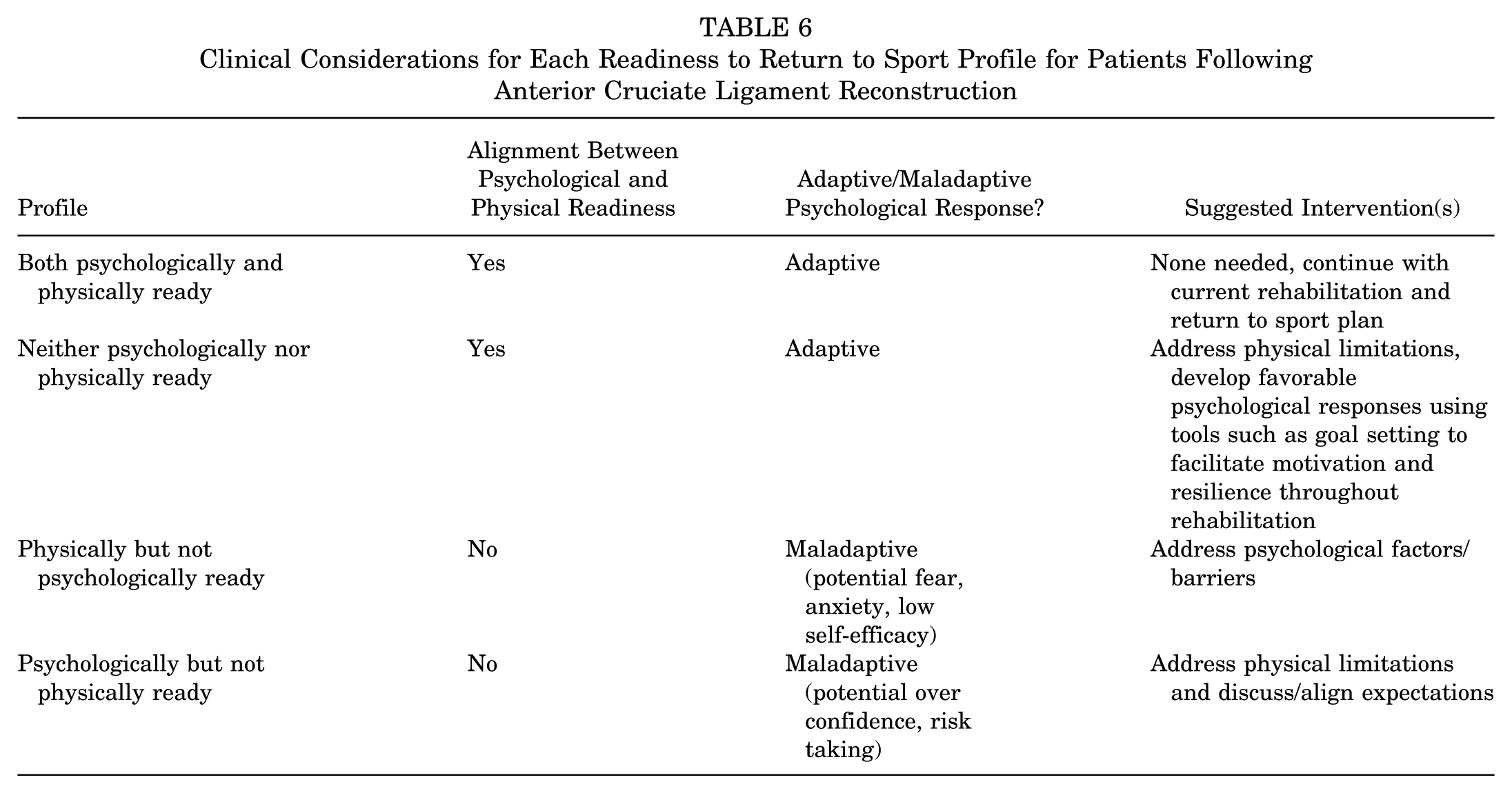
Implications for Clinical Practice and Orthopaedic Research
The proposed approach to readiness profiles is a practical method of integrating physical and psychological outcomes into clinical and RTS decision-making after ACLR. The integration of both physical and psychological factors into a clinician's assessments of patient status allows for a holistic approach to care. While directionality of how physical and psychological factors affect each other is not fully clear, interpreting psychological responses in conjunction with objective physical function can be helpful for guiding treatment decisions. Table 6 outlines how clinicians and patients can utilize the profiles described in the paper for outcome interpretation and treatment indication. These profiles can be easily constructed by rehabilitation specialists based on patient outcomes. Importantly, these profiles should be used in future orthopaedic research to understand their association with RTS and injury recurrence. Given the already established association between the psychological and physical outcome measures chosen to construct the profiles and RTS and reinjury rates, it will be critical to understand the nuance of how different permutations of these outcomes influence these important endpoints. For example, based on previous literature we can assume that patients with profiles other than both psychologically and physically ready may be at an increased risk of no RTS or of subsequent injury.
Clinical Considerations for Each Readiness to Return to Sport Profile for Patients Following Anterior Cruciate Ligament Reconstruction
Limitations
This study is limited in its retrospective design and inconsistency in outcome collection across registry sites. While the isokinetic and hop-testing protocols were similar across sites, there may have been testing differences that were not controlled for (warmup, number of test trials, setting, observers, etc). Additionally, there is no standardized rehabilitation protocol for patients included in this multisite registry, as patients are referred for testing at participating ARROW sites from multiple locations (ie, private or university- or hospital-based physical therapy, athletic trainers, sports teams, etc). However, the multisite contribution of data increases our representation of patients from a variety of locations and centers and makes the findings more widely applicable. To improve feasibility and interpretation, the domains of psychological, strength-based and performance-based physical readiness were operationalized with 1 outcome measure. It is possible that other outcome measures or a combination of measures may better represent RTS readiness. Additionally, we had data for patients tested up to a maximum of 13 months postoperative and the majority of patients (78%) were <9 months postoperative. A later time point for RTS testing and secondary injury data collection might provide further information related to physical and psychological readiness and the association with reinjury. This cohort will be followed to understand their outcomes and profile categorization at later rehabilitation time points and to investigate how their RTS readiness profiles relate to RTS and secondary ACL injury rates. While the current cross-sectional study data indicated no difference in the distribution of profiles for patients 5 to 9 months postoperative compared with those 9 to 13 months postoperative, having data from earlier rehabilitation time points will be beneficial in understanding the trajectories of profiles and whether individual patients’ profiles stay consistent or change over time. This study used the ICF model as a basis for contextualizing the different constructs of readiness to RTS being measured within the profiles that were created. Environmental factors are an important component of the ICF model not explicitly measured in this study. However, we observed important age- and sex-based differences that were likely related to patients’ home, school/work, and sport/physical activity environments.
Conclusion
There are a variety of distinct profiles of physical and psychological readiness in patients post-ACLR. Psychological, strength-based, and performance-based physical readiness to RTS criteria align for less than one third of participants. Patients who did not meet psychological or physical readiness criteria tended to be older in age, and male patients were more likely to have alignment between their psychological and physical readiness.
Footnotes
Final revision submitted February 21, 2026; accepted February 27, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.M. is supported by research funding from the Canadian Institutes of Health Research. S.B. is supported by research funding from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Ethical approval was obtained from the University of Virgina Institutional Review Board for Health Sciences Research (IRB Nos. HSR230225 and HSR230335).