
Abstract
Background:
Lower trapezius tendon (LTT) transfer can restore shoulder function, particularly active external rotation (ER) following massive rotator cuff tear (MRCT). However, the optimal graft type and its transfer location on the greater tuberosity remain unclear.
Purpose:
To investigate the optimal graft type and location in LTT transfer for posterosuperior MRCT from a biomechanical perspective.
Study Design:
Controlled laboratory study.
Methods:
Eight fresh-frozen cadaveric shoulders were tested on a shoulder simulator. LTT transfer was performed with an Achilles tendon fixed over the superior-middle facets (LTT-Achilles), a semitendinosus (ST) tendon to the superior facet (LTT-ST-S), or to the middle facet (LTT-ST-M). A 24-N load was applied to each transferred graft. Under each condition (intact rotator cuff, MRCT, LTT-Achilles, ST-S, and ST-M), humeral head translation and functional abduction force (FAF) were evaluated at 0°, 30°, and 60° of glenohumeral elevation. ER torque was assessed across 5 angles (60° internal rotation [60IR], 30° internal rotation [30IR], neutral, 30° ER [30ER], and 60° ER [60ER]) at 0°, 30°, and 60° of glenohumeral elevation.
Results:
None of the LTT conditions significantly depressed humeral head posterosuperior migration as compared with MRCT. Compared with MRCT, FAF improved significantly with LTT-Achilles at 0° elevation (P = .014) and LTT-ST-S at 0° (P < .001) and 30° elevation (P = .003). LTT-ST-M improved ER torque compared with MRCT at 0° elevation (60IR, P = .04; 30IR, P = .02; neutral, P = .007; 30ER, P = .03; 60ER, P = .006) and at 30° elevation (60IR, P = .01; 30IR, P = .02; neutral, P = .006). LTT-ST-M showed higher ER torque than both LTT-Achilles and LTT-ST-S at 0° elevation (30IR [LTT-Achilles, P = .03; LTT-ST-S, P = .04]; neutral [LTT-Achilles, P = .02; LTT-ST-S, P = .007]).
Conclusion:
In LTT transfer for MRCT, LTT-ST-M most effectively restored ER torque, whereas LTT-Achilles and LTT-ST-S improved FAF. None of the conditions of LTT transfer suppressed humeral translation.
Clinical Relevance:
Graft selection and transfer location in LTT transfer can be tailored to patient goals and graft availability, leading to a more patient-specific surgical strategy.
Keywords
For irreparable posterosuperior massive rotator cuff tear (MRCT), muscle transfer procedures such as latissimus dorsi (LD) transfer 27 and lower trapezius tendon (LTT) transfer 9 have been reported to yield favorable outcomes. Among these, the LTT transfer is reported to provide better restoration of external rotation (ER) function, as its line-of-action is more similar to that of the infraspinatus muscle compared with the LD transfer.4,12 Also, biomechanical studies have also demonstrated the LTT's ability to reduce superior migration of the humeral head.4,21 In addition to restoring ER strength, this procedure may act as a dynamic stabilizer that suppresses superior translation of the humeral head caused by MRCT.
The surgical technique involves detaching the LTT from the medial scapular spine and transferring it to the greater tuberosity to restore the function of the torn rotator cuff tendons. However, because the LTT alone cannot reach the greater tuberosity, the transfer is performed using an interposed tendon graft between the LTT and the greater tuberosity. 12 The tendons primarily used for this procedure are the Achilles tendon and the semitendinosus (ST) tendon 1 ; however, to the best of our knowledge, no study has directly compared their outcomes. Furthermore, since the ST tendon is thinner than the Achilles tendon, its transfer location may be more critical. Additionally, while autografts are primarily used for the ST tendon, allografts are required for the Achilles tendon. However, the availability of allografts varies among countries and institutions.26,29 Taken together, understanding the biomechanical characteristics and advantages of each graft type and location is essential for optimizing the application of this procedure according to the regional medical environment and patient cultural concerns with allografts.
The purpose of this study, therefore, was to identify the optimal graft type and transfer location for various LTT transfers in the treatment of irreparable posterosuperior MRCT. To clarify this, a cadaveric model of an MRCT was created, and LTT transfers were performed using an Achilles tendon graft and an ST tendon graft in a repeated-measures fashion. Furthermore, the ST tendon was evaluated with the tendon transferred to 2 different anatomic locations. The biomechanical effects for each procedure were evaluated using a shoulder cadaveric simulator. The hypotheses were (1) that both Achilles and ST tendon grafts would restore ER function lost due to posterosuperior MRCT; (2) the Achilles tendon would provide greater suppression of superior humeral head translation; and (3) that when using the ST tendon, a transfer location closer to the infraspinatus muscle tendon footprint would improve ER function over a transfer location closer to the supraspinatus footprint.
Methods
Specimen Preparation and Experimental Setup
Eight fresh-frozen cadaveric shoulders (mean age, 63 ± 15 years; all male) were used in this study. The specimens were thawed for ≥18 hours before testing. The skin and deltoid muscle were removed, whereas all other soft tissues, including the joint capsule and rotator cuff tendons, were preserved. The humerus was transected at the middiaphysis. Each rotator cuff tendon was identified and tagged with sutures placed in the subscapularis (upper and lower portions), supraspinatus, infraspinatus, and teres minor using No. 5 nonabsorbable braided sutures (Ethibond; Ethicon [Johnson & Johnson). Three high-strength braided lines were sutured through a transosseous hole created at the centroid of the deltoid tuberosity to replicate the anterior, middle, and posterior heads of the deltoid muscle. The setup of the cadaveric shoulder simulator is shown in Figure 1. A humeral rod assembly equipped with a load cell (Nano25; ATI) to quantify rotational torque was inserted distally into the humerus. 14 This was connected to the simulator's abduction arc through a metallic rail assembly containing another load cell (Nano25; ATI) to quantify functional abduction force (FAF). 17 The scapula was clamped to the simulator between 2 metal plates and adjusted to maintain 20° of anterior tilt. 28 The cables attached to the tagged rotator cuff tendons and deltoid tuberosity were connected to computer-controlled pneumatic actuators. Eyebolts and custom 2 degrees of freedom pulley assemblies were used to ensure physiological muscle lines of actions with minimal frictional losses. A constant force of 10 N was applied to each of the rotator cuff muscle tendons,14,20 while the forces applied to the deltoid muscle were adjusted according to the protocol described in each testing condition. 23
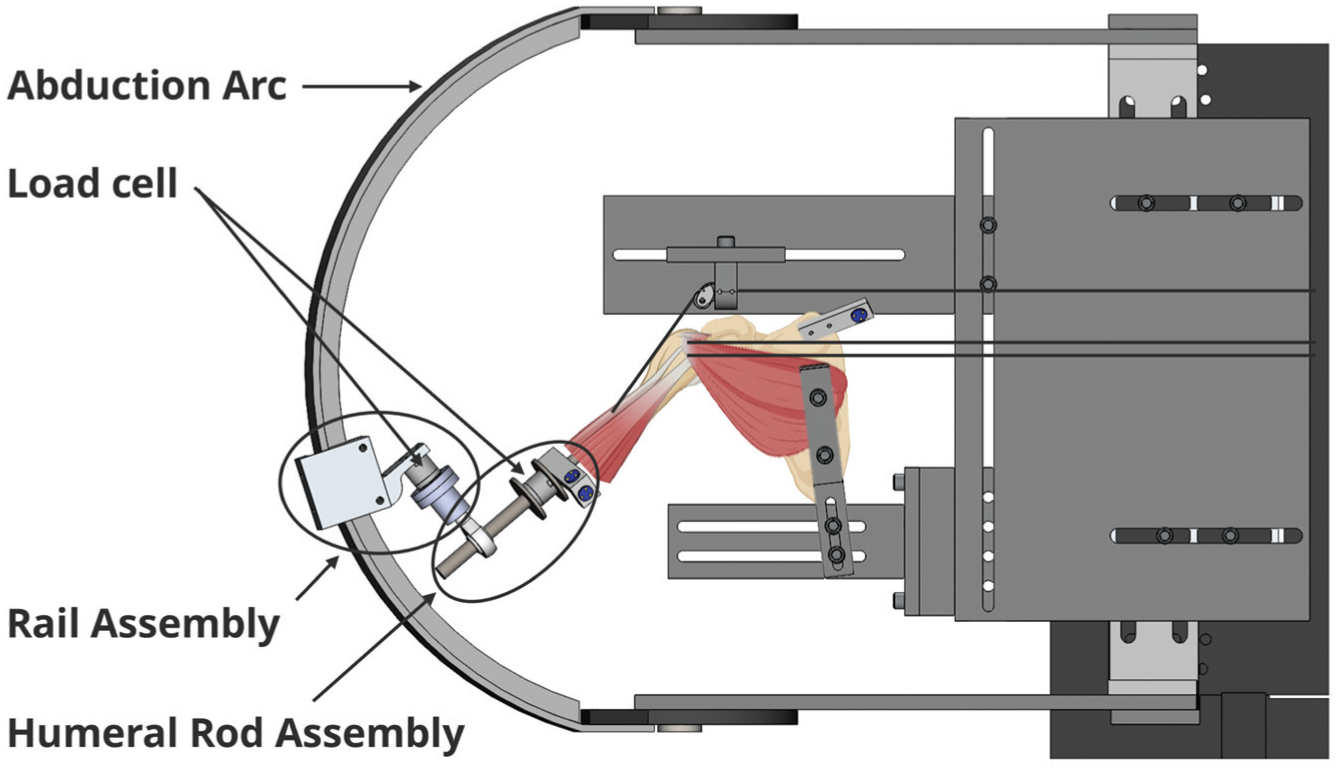
Experimental setup of the cadaveric shoulder simulator. The scapula was secured to the simulator with an optical tracker rigidly fixed to the superior angle of the scapula. A metallic rod equipped with a load cell to quantify rotational torque and an optical tracker was inserted into the humerus from the distal end and mounted on the abduction arc via a rail assembly containing another load cell for functional abduction force measurement.
Testing Conditions
Tests were performed for humeral head translation and FAF under the following 5 conditions: intact, MRCT, LTT transfer with Achilles tendon graft (LTT-Achilles), LTT transfer with ST tendon graft transferred to the superior facet (LTT-ST-S), and LTT transfer with ST tendon graft transferred to the middle facet (LTT-ST-M). For ER function evaluation, tests were performed under 4 conditions, excluding the intact condition. The details of each condition are described below.
Intact
Testing in the intact condition was only performed to measure humeral head translation and FAF. All rotator cuff muscles were intact with 10 N applied to each tendon. As previously stated, 2 loading conditions were performed while evaluating humeral head translation in the intact rotator cuff state. The first applied 30 N of load to the deltoid, distributed equally across 3 lines representing the anterior, middle, and posterior heads, to balance the coronal glenohumeral force couple to center the humeral head in the glenohumeral joint. The second applied an 80-N deltoid load to promote superior humeral head migration, which was important for the cuff-deficient conditions.
Massive Rotator Cuff Tear
To simulate an irreparable posterosuperior MRCT, the supraspinatus, infraspinatus, and the underlying joint capsule were completely resected. As a result, the forces previously applied to the supraspinatus and infraspinatus in the intact condition were no longer loaded. The subscapularis and teres minor were left intact. The long head of the biceps tendon was also tenotomized.
LTT Transfer: Achilles, ST-S, and ST-M
The LTT transfer was then performed in the setting of an MRCT using the Achilles tendon and the ST tendon (Figure 2). The Achilles and ST tendons were harvested from 8 healthy, fresh-frozen cadavers, with each tendon sutured with No. 5 Ethibond using a Krackow technique. The Achilles graft was fixed to the greater tuberosity using transosseous sutures, covering the superior and middle facet. The ST tendon was folded in half and reinforced with whipstitches. The doubled graft was passed through a 6-mm bone tunnel drilled from either the superior or the middle facet toward the bicipital groove and then secured at the groove using a clamp. The line of action of both types of grafts was adjusted to simulate the path of the lower trapezius muscle fibers using the scapular spine as a landmark. 22 Cables were tagged to the medial side of the graft. For the Achilles tendon graft, cables were tagged at the superomedial and inferomedial borders of the graft to promote a more even distribution of tension across the tendon. 5 The grafts were subjected to a force of 24 N following previous research, 17 while the order in which grafts were evaluated was randomized across all cadavers.
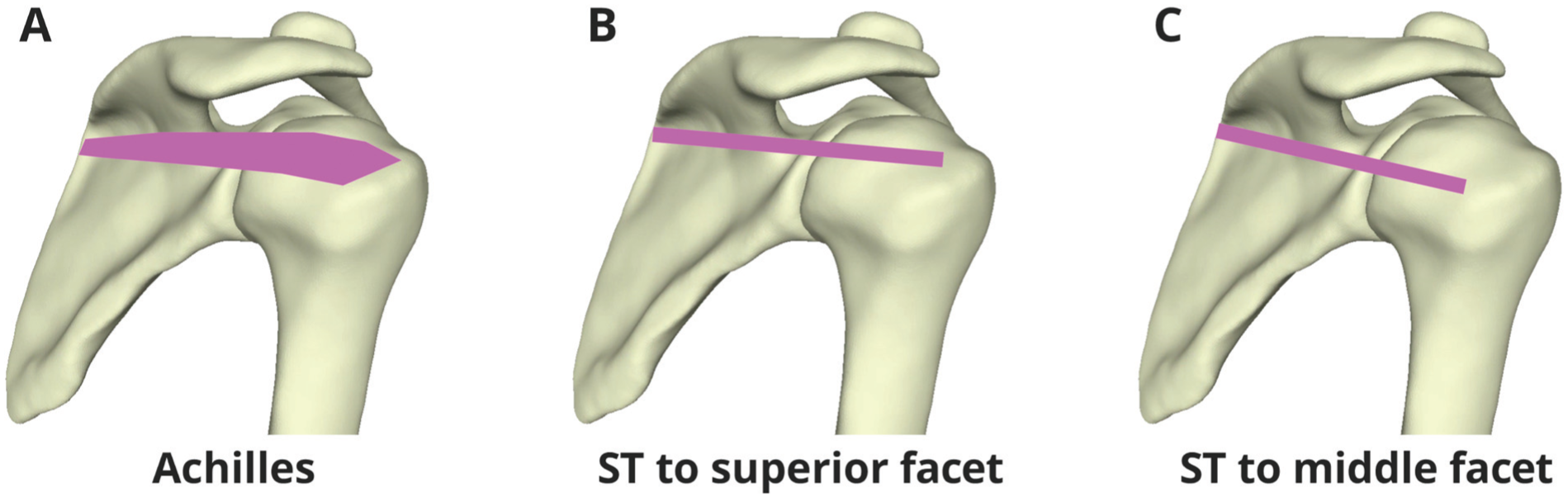
Procedure for LTT transfer. The pink lines indicate the transferred graft in each construct. (A) Transfer of the LTT using the Achilles tendon graft to the superior and middle greater tuberosity facets. (B) Transfer of the ST graft to the superior facet. (C) Transfer of the ST tendon graft to the middle facet. LTT, lower trapezius tendon; ST, semitendinosus.
Testing Protocol and Outcome Variables
The translation of the humeral head was quantified using an optical tracking system (Certus; Northern Digital) with a 3-dimensional tracking accuracy of 0.1 mm and resolution of 0.01 mm. Prior to testing, optical tracking markers were rigidly fixed to the scapula and humerus, 23 ensuring that a clear line of sight was possible between the markers and camera for all testing positions. Following the completion of all tests, a digitization stylus was first used to determine the center of the humeral head using previously established methods. 18 This point was then tracked relative to a glenoid coordinate system, which was constructed by digitizing several points on the glenoid surface.18,23 Additionally, FAF was measured using the load cell in the rail assembly to evaluate abduction function simultaneously. Both humeral head translation and FAF were measured in neutral axial rotation at 0°, 30°, and 60° of glenohumeral abduction in the scapular plane. A pilot test was conducted to determine the deltoid force that best corresponded to a centered humeral head position on the glenoid. The results showed that when a total force of 30 N was applied to the deltoid muscle with the rotator cuff intact, the humeral head was positioned closest to the center of the glenoid. Therefore, the position of the humeral head center under these conditions was defined as the reference point with which humeral head translation in all other testing conditions was compared. A total deltoid force of 80 N was applied to the deltoid muscle for all remaining testing conditions. 23
Furthermore, to evaluate ER function, a 5-N force was applied to each head of the deltoid muscle 8 to maintain the centering of the humeral head. The corresponding loads were then applied to the rotator cuff (upper and lower subscapularis, 10 N each; teres minor, 10 N) and transferred tendons under each condition, and ER torque was measured using the load cell within the humeral rod assembly in 15 combined positions consisting of 5 axial rotation angles (60° of internal rotation [60IR], 30° of internal rotation [30IR], neutral, 30° of ER [30ER], and 60° of ER [60ER]) and 3 glenohumeral elevations in the scapular plane (0°, 30°, and 60°). The neutral axial rotation position was defined as the position in which the bicipital groove was aligned with the anterolateral edge of the acromion. 19
Statistical Analysis
All data are presented as mean ± SE. A 2-way repeated-measures analysis of variance (ANOVA) was performed to examine the effects of condition and glenohumeral elevation, followed by Holm-adjusted post hoc pairwise comparisons for humeral head translation and FAF. For ER torque, within each combination of glenohumeral elevation and rotation, a 1-way repeated-measures ANOVA was performed across conditions, followed by Holm-adjusted post hoc pairwise comparisons. Statistical significance was set at P < .05. All statistical analyses were conducted using R, Version 4.5.1 (R Foundation for Statistical Computing).
Results
LTT Transfer Did Not Suppress the Humeral Head Translation Followed by MRCT
Figure 3A shows the humeral head translation for each condition relative to the intact 30-N condition, while Figure 3B illustrates the direction of translation, which was predominantly posterosuperior at 0° and more posterior at 30° of glenohumeral elevation. Two-way repeated-measures ANOVA revealed significant main effects of condition (P < .001) and elevation (P = .004), as well as a significant interaction between them (P < .001). At 0° and 30° of glenohumeral elevation, all conditions (MRCT, LTT-Achilles, LTT-ST-S, LTT-ST-M) showed significantly greater translation values compared to the intact condition (p < .011). However, none of the grafts showed a significant improvement in translation compared with the MRCT. No significant differences were measured among all groups, including the intact group, at 60° of glenohumeral elevation.
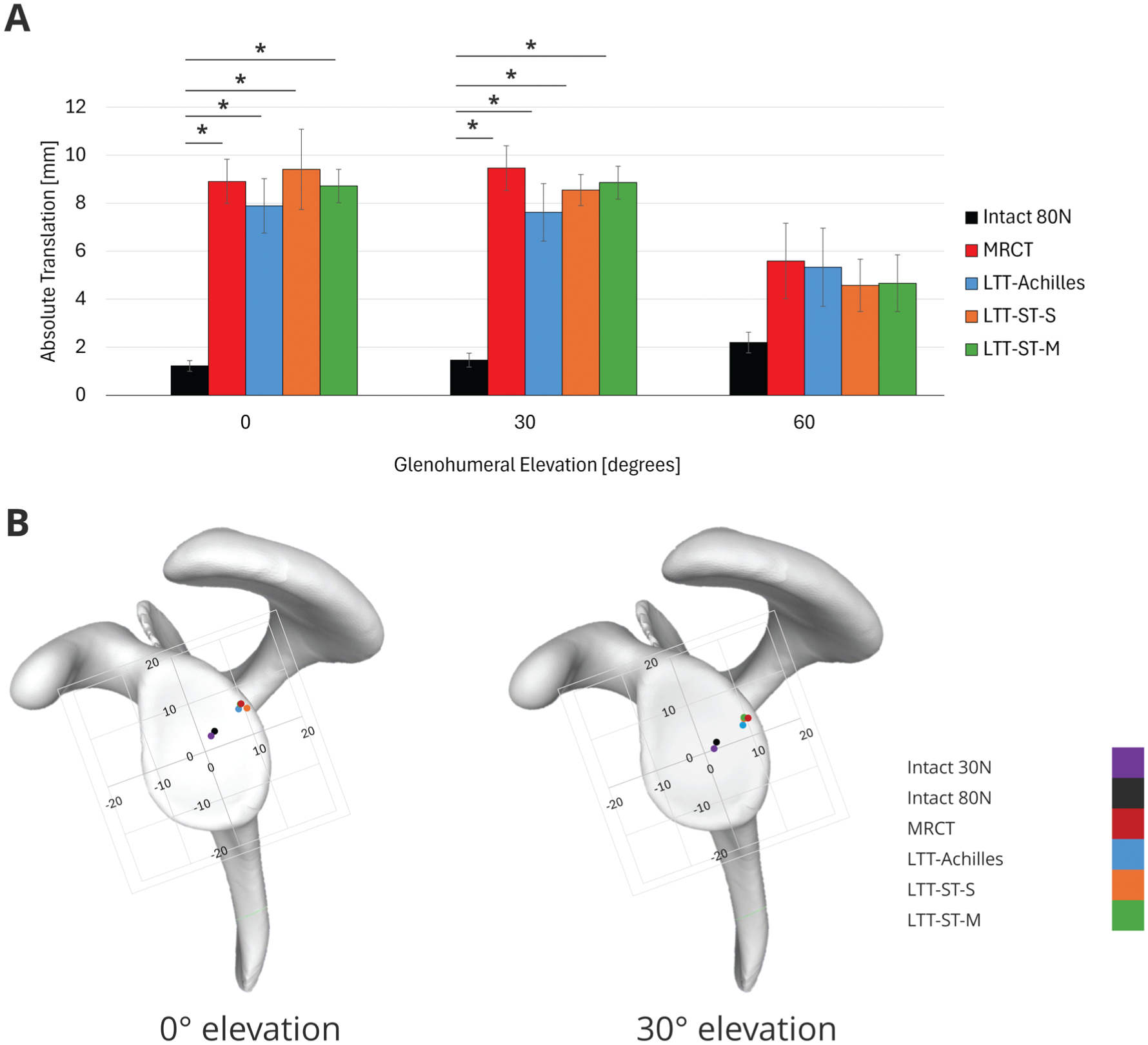
Differences in the humeral head translation by each condition. (A) Translation of the humeral head from the reference point (intact 30 N). Data are shown as mean ± SE. *P <.05. (B) Direction of humeral head translation for each condition. Intact 30 N (purple) was used as the reference point for quantifying translation under each condition in Figure 3A. The values in the figure represent the distance (mm) from the center of the glenoid (0). The left figure shows the results at 0° of glenohumeral elevation, while the right figure shows the results at 30° of glenohumeral elevation. LTT, lower trapezius tendon; M, middle; MRCT, massive rotator cuff tear; S, superior; ST, semitendinosus.
LTT-Achilles and -ST-S Improved FAF Compared With MRCT
Figure 4 demonstrates the FAF under each condition. Two-way repeated-measures ANOVA demonstrated significant main effects of condition (P = .02) and elevation (P = .03), along with a significant interaction between the 2 factors (P = .002). Therefore, post hoc pairwise comparisons with Holm adjustment were conducted to further investigate the effects of condition at each elevation. At 0° of glenohumeral elevation, both LTT-Achilles and LTT-ST-S improved FAF significantly compared with MRCT (LTT-Achilles, P = .01; LTT-ST-S, P < .001). Furthermore, at 30° of glenohumeral elevation, LTT-ST-S showed a significant improvement in FAF compared with MRCT (P = .003) and also exhibited significantly higher FAF than LTT-ST-M (P = .04). At 60° of glenohumeral elevation, no significant differences in FAF were identified between any of the groups (P > .23).
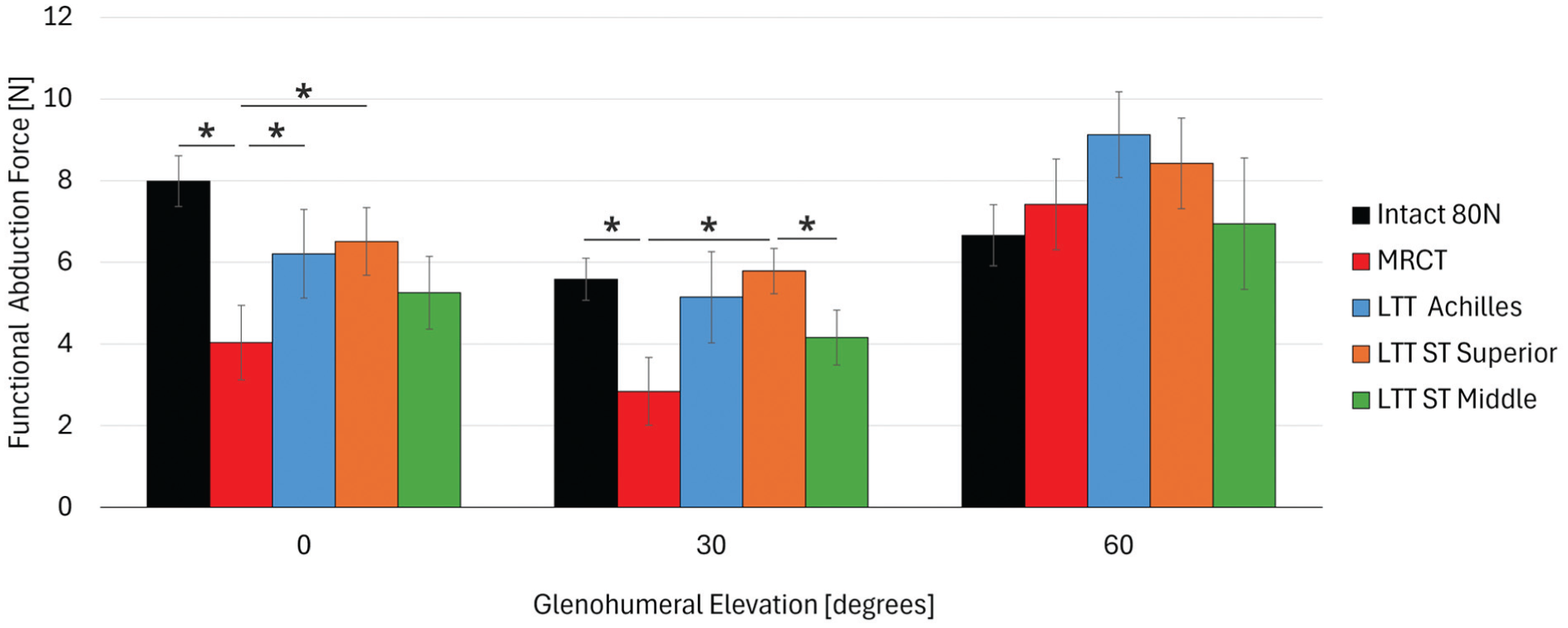
Differences in the effect of each condition on functional abduction force. Data are shown as mean ± SE. *P < .05. LTT, lower trapezius tendon; M, middle; MRCT, massive rotator cuff tear; S, superior; ST, semitendinosus. LTT-ST-M improved external rotation torque effectively.
LTT-ST-M Improved External Rotation Torque Effectively
At 0° of glenohumeral elevation (Figure 5), the LTT-ST-M exhibited significantly greater ER torque than MRCT across all axial rotation angles (P < .04), while both LTT-Achilles and LTT-ST-S demonstrated greater ER torque compared with MRCT only from the neutral to the externally rotated positions (P < .03). At 30IR and neutral positions, LTT-ST-M generated significantly higher ER torque than both the LTT-Achilles and LTT-ST-S (30IR, P < .04; neutral, P < .02). At 30° of glenohumeral elevation, LTT-ST-M again exhibited significantly greater ER torque than MRCT in multiple axial rotation conditions (P < .02), and at 60IR, ER torque was significantly higher than that of LTT-Achilles (P = .04), as shown in Appendix Figure A1. At 60° of glenohumeral elevation, there were few significant differences among the groups, except that LTT-ST-S demonstrated significantly greater ER torque than MRCT at 30ER (P = .03), as shown in Appendix Figure A2.
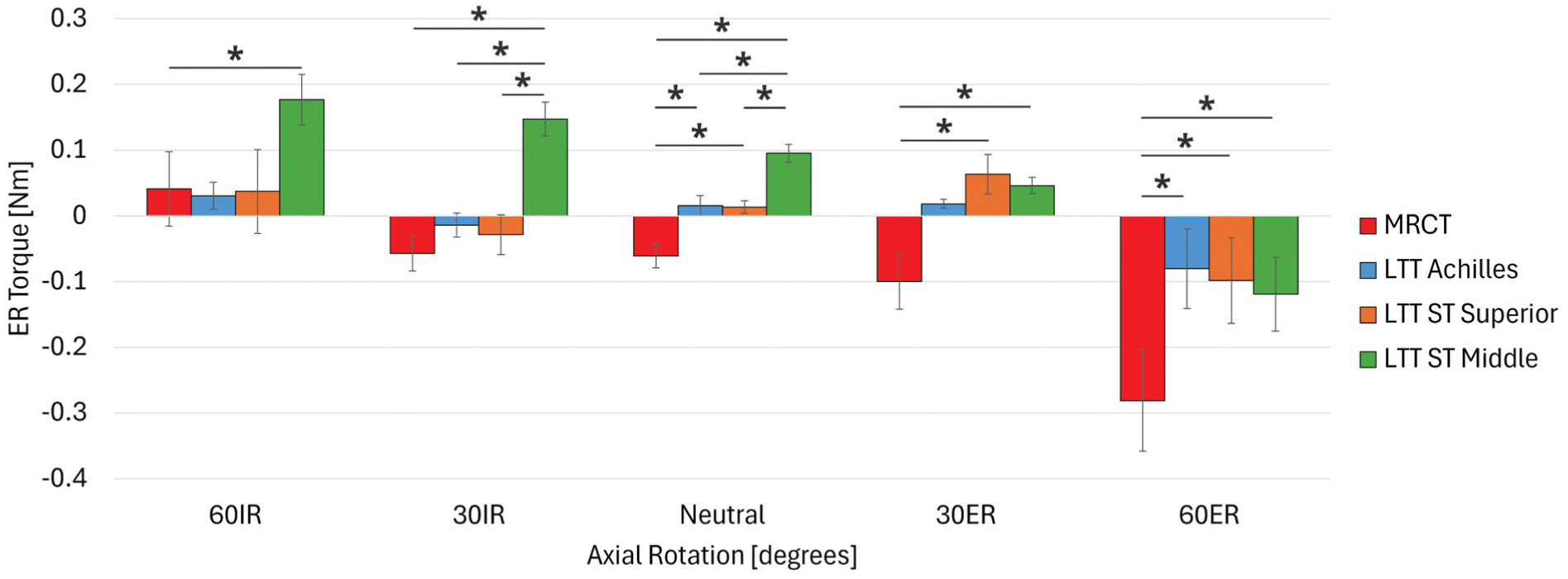
Differences in the effect of each condition on external rotation (ER) torque at 0° of glenohumeral elevation. Data are shown as mean ± SE. *P <.05. IR, internal rotation; LTT, lower trapezius tendon; MRCT, massive rotator cuff tear; ST, semitendinosus.
Discussion
This biomechanical study demonstrated that LTT transfer using both Achilles tendon and ST tendon grafts restored ER function after irreparable posterosuperior MRCT. Among these, the transfer of the ST tendon graft to the middle facet demonstrated superior restoration of ER function. In addition, a significant improvement in abduction function was observed when using the Achilles tendon graft or when transferring the ST tendon graft to the superior facet. However, contrary to our hypothesis, neither the ST nor the Achilles tendon graft significantly suppressed posterosuperior translation of the humeral head as seen in MRCT. These findings provide valuable insights into graft selection and determining the transfer location during LTT transfer in clinical practice.
Regarding the suppression of superior migration of the humeral head, previous clinical studies have reported that the acromiohumeral distance remains unchanged or decreases after LTT transfer.2,16 In contrast, some biomechanical studies have demonstrated that LTT transfer can suppress superior migration of the humeral head.5,22 In the present study, however, no suppression effect on superior translation was observed regardless of the graft type or transfer location. This discrepancy may be related to differences in experimental conditions, particularly variations in muscle loading. Nevertheless, the findings of this study are consistent with previous clinical studies2,16 and therefore appear reasonable.
With respect to FAF, both LTT-Achilles and LTT-ST-S improved FAF compared with posterosuperior MRCT. This finding suggests that transferring either an Achilles or an ST graft to a more superior area during the LTT transfer may be effective in patients who require improvement of abduction strength. In other words, positioning the graft more superiorly on the greater tuberosity may have allowed the load vector of the lower trapezius to act more in the abduction direction rather than in ER, thereby producing the abduction moment more efficiently. Considering these findings together with the results on superior migration, LTT-Achilles and LTT-ST-S may be appropriate options for patients who require improvement of abduction strength without superior migration of the humeral head.
Regarding ER function, LTT-ST-M produced the greatest improvement in ER torque. This may well be attributed to the longer moment arm achieved by transferring the graft to a more posterior location, more efficiently generating torque in the externally rotated direction. A previous computer simulation study has also reported that grafting to the infraspinatus insertion increases the externally rotating moment arm, 24 and the results of the current study support this finding. Additionally, in the ER position, improvements in ER torque were observed for both LTT-Achilles and LTT-ST-S. This is likely because the greater tuberosity was positioned posteriorly in the ER position, favoring the tendon's line of action for ER. In contrast, at 60° of abduction, little improvement in ER torque was observed across all conditions. This may be due to changes in the line of action of the graft with increasing abduction angle, resulting in the force acting more as a compressive force on the joint rather than contributing to ER torque.
LTT transfer was reported by Elhassan et al 11 as a surgical procedure to restore ER function in a patient with brachial plexus injury. Subsequently, it has been widely applied as a surgical option to restore ER function lost due to posterosuperior MRCT. 15 Based on the present results, in patients with isolated loss of ER, 7 characterized by preserved elevation without superior migration of the humeral head, transferring the graft more posteriorly on the greater tuberosity to maximize the ER moment arm may be the most reasonable approach to achieve the primary objective of ER restoration. In this study, transferring the ST tendon graft to the middle facet resulted in the greatest improvement in ER torque, which aligns with the concept of LTT transfer as a procedure primarily intended for restoration of ER. In contrast, when improvement in abduction function is prioritized over ER, transferring the graft to a more superior location on the greater tuberosity to maximize the abduction moment arm would appear to be reasonable. It was also shown herein that abduction force was improved when the ST tendon graft was transferred to the superior facet, as well as when the Achilles tendon graft was fixed to cover a broader footprint, including the superior facet. The improvement in abduction function observed with LTT transfer in this study is also consistent with findings from previous biomechanical research. 5 Furthermore, in a study comparing LTT transfer and LD transfer, LTT transfer demonstrated greater abduction moment arms than LD transfer when transferred to the supraspinatus and infraspinatus insertion sites. 24 In contrast, LD transfer exhibited relatively constant ER moment arms regardless of the transfer location, whereas LTT transfer showed a reduced ER moment arm when transferred to the supraspinatus insertion site. 24 These findings indicated that LTT transfer should not be performed uniformly; rather, the graft location should be tailored to the surgical objective, which allows a more patient-specific and optimized treatment strategy.
Additionally, in graft selection, LTT transfer initially utilized Achilles tendon graft,11,13 which required obtaining an Achilles tendon allograft. However, allograft availability varies by country and institution.26,29 This study demonstrates that using the ST tendon for LTT transfer yields favorable improvements in ER and abduction function depending on the transfer location. Therefore, even when access to allografts is limited, using ST tendon autograft for LTT transfer can achieve good results without relying on Achilles tendon allograft. This implies that LTT transfer is feasible regardless of allograft availability, broadening the surgeon's options and potentially contributing to the wider adoption of LTT transfer.
Limitations
This study has limitations. First, the evaluation was performed in the immediate state after tendon transfer, and thus the time-dependent changes in tendon characteristics and biological healing of the transferred graft were not considered. However, the incidence of tendon rupture after LTT transfer has been reported to be low, 10 and therefore, the biomechanical characteristics determined by the initial graft location are likely to be maintained postoperatively. Second, the experimental setup restricted motion to elevation in the scapular plane, and elevation in other planes or multiplanar movements could not be analyzed. Third, we focused on comparing different graft types and transfer locations in LTT transfer, without assessing its superiority over other surgical techniques. In particular, middle trapezius tendon transfer has a line of action more similar to that of the supraspinatus and primarily aims to suppress upper migration of the humeral head 6 as well as to restore abduction function. 3 Future investigations comparing the lower and middle trapezius tendon transfers at identical insertion sites may help clarify the distinct functional contributions of each muscle portion. Finally, the Achilles tendon graft was transferred to cover the superior and middle facets in the present study. However, another reported technique involves wrapping the graft around the lateral aspect of the greater tuberosity, 25 which could yield different biomechanical outcomes. Considering the line of action and the potential effect on the moment arm, this alternative approach may provide a mechanical advantage in generating ER torque and might behave similarly to the LTT-ST-M configuration observed in this study. Therefore, in clinical practice, optimizing the choice of graft and transfer technique based on individual patient conditions may lead to more favorable functional recovery.
Conclusion
This study biomechanically evaluated the functional differences associated with graft type and transfer location in LTT transfer for irreparable posterosuperior MRCT. The results showed that ER function was most improved when the ST graft was transferred to the middle facet on the greater tuberosity, whereas abduction function improved when the Achilles tendon was transferred to the superior-middle facets or when the ST graft was transferred to the superior facet. However, none of the conditions effectively suppressed the posterosuperior migration of the humeral head seen in massive irreparable cuff tears. These findings suggest that in LTT transfer, graft selection can be tailored according to graft availability, and optimizing graft choice and transfer location based on the patient's required function may provide a more patient-specific approach for restoring shoulder function.
Footnotes
Appendix
Final revision submitted March 4, 2026; accepted March 9, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.A. is a paid consultant for Stryker, and receives royalties from Stryker, Conmed, and Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD).
Ethical approval was not required for this cadaveric study.