
Abstract
Background:
Anterior cruciate ligament reconstruction (ACLR) is frequently followed by significant quadriceps atrophy and strength loss due to postoperative pain and the necessity for low-load rehabilitation. Blood flow restriction (BFR) training is an emerging modality that may facilitate muscle strength and hypertrophy under low-load conditions, but its efficacy for improving functional outcomes after ACLR remains to be conclusively determined.
Purpose:
To systematically evaluate the effects of BFR training on lower limb function, quadriceps strength, and knee pain in patients following ACLR.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A comprehensive literature search was conducted in PubMed, Embase, Cochrane Library, Web of Science, PEDro, EBSCO and CNKI for randomized controlled trials (RCTs) published between January 2015 and August 2025. A total of 606 records were identified through database searching, and 9 RCTs were included after screening. Data on functional scores (Lysholm, International Knee Documentation Committee [IKDC]), quadriceps peak torque (PT), pain (visual analog scale [VAS]), and range of motion (ROM) were extracted and analyzed using RevMan 5.4, and risk of bias was assessed using the Cochrane tool. Meta-analyses were performed using weighted mean differences (WMDs) with fixed- or random-effects models as appropriate, and heterogeneity was assessed using the I2 statistic.
Results:
Nine RCTs involving 372 participants were included. Meta-analysis revealed that BFR training significantly improved Lysholm scores (WMD, 5.75; 95% CI, 0.60-10.90; P = .03) and quadriceps PT (WMD, 8.34; 95% CI, 7.47-9.22; P < .00001), and increased total work output (P = .006). However, no significant differences were observed in IKDC scores, VAS pain scores, or ROM (P > .05). Sensitivity analyses confirmed the robustness of the primary findings.
Conclusion:
Our study demonstrated that BFR training may promote early recovery of quadriceps strength and selected aspects of knee function after ACLR under low-load conditions. BFR appears feasible and generally well tolerated in the included trials; however, safety conclusions are limited by inconsistent adverse-event reporting. Its effects on pain relief, joint mobility, and long-term functional recovery require further investigation.
Keywords
Anterior cruciate ligament (ACL) injury is one of the most common knee traumas among young and physically active individuals engaging in high-intensity sports activities. 49 Although surgical techniques for ACL reconstruction (ACLR) have become increasingly refined, postoperative rehabilitation remains challenging because of pain, swelling, and the need to protect the graft. These factors often necessitate a “low-load” rehabilitation approach, making quadriceps atrophy and arthrogenic muscle inhibition major barriers to recovery.6,36 Any delay in postoperative rehabilitation or restoration of muscle strength may trigger a cascade of “strength loss–compensatory movement patterns–abnormal cartilage loading,” thereby increasing the risk of early-onset knee osteoarthritis and impairing patients’ daily function and return-to-sport (RTS) potential. 44 Although psychological readiness (eg, confidence, fear of reinjury, and kinesiophobia) is also critical for RTS after ACLR, standardized psychological outcomes are infrequently reported in postoperative blood flow restriction (BFR) trials, limiting the ability to synthesize such constructs in secondary analyses.
BFR training, first introduced in the 1960s by Dr. Yoshiaki Sato in Japan, is an emerging rehabilitation modality that allows low-load resistance exercise under partial vascular occlusion.33,42 By applying an inflatable cuff to restrict venous return while maintaining partial arterial inflow, BFR induces a localized hypoxic and metabolically stressful environment that promotes muscle strength gains and hypertrophy. 41 Unlike traditional high-load resistance training, BFR can elicit comparable improvements in muscle mass and strength at only 20% to 30% of 1-repetition maximum (1RM). 16 This makes BFR a promising adjunct or bridge strategy during periods when high-load resistance exercise is not feasible or is clinically deferred (eg, early postoperative phase), rather than a replacement for progressive, multimodal ACL rehabilitation. Previous studies have demonstrated that BFR training can enhance quadriceps strength recovery after ACLR, whereas findings for pain- and symptom-related outcomes have been mixed across trials. 17 Through increased metabolic stress and muscle recruitment, BFR enables early-stage muscle hypertrophy and functional improvement even under low-intensity loading, offering an efficient rehabilitation strategy during the early postoperative phase.34,40 As postoperative healing progresses, BFR may be integrated alongside conventional progressive strengthening and neuromuscular/functional training within a multimodal rehabilitation program.
Recent meta-analyses and clinical trials have provided further insight into the efficacy of BFR after ACLR. A recent systematic review and meta-analysis of randomized controlled trials (RCTs) reported overall benefits of BFR on neuromuscular and selected clinical outcomes after ACLR, while highlighting variability across outcomes and protocols. 14 In addition, a 2025 meta-analysis further explored stage-specific effects (eg, early muscle strength vs midterm knee function), suggesting that postoperative follow-up duration may contribute to heterogeneous findings. 28 Gopinatth et al 14 and Iversen et al 19 reported that BFR training significantly improved quadriceps strength and functional scores compared with conventional rehabilitation, although inconsistent results were observed for International Knee Documentation Committee (IKDC) and pain outcomes. Erickson et al 11 used magnetic resonance imaging and muscle physiology analyses to confirm that BFR enhances muscle fiber cross-sectional area and mitochondrial density, providing microstructural evidence for its anabolic effects. Similarly, Butt and Ahmed 3 and Colombo et al 8 concluded that BFR effectively prevents muscle atrophy during the early postoperative period (2-6 weeks), though evidence for long-term functional benefits remains limited. Despite the growing body of supportive evidence, considerable heterogeneity persists among studies regarding occlusion pressure, cuff width, training frequency, and duration.27-29 Moreover, the optimal timing of BFR intervention—whether during prehabilitation, early, or midphase postoperative recovery—has yet to be established.23,45 Some studies have also questioned its clinical applicability, citing limited real-world efficacy due to poor adherence or inappropriate pressure settings.9,15 Recent prospective trials continue to emerge, including investigations specifically targeting the early postoperative phase, further underscoring the need to continuously update the evidence base. 2 However, beyond numerical updates, there remains a need for a synthesis that explicitly accounts for postoperative time dependence and evidence certainty to avoid overgeneralized clinical claims.
Recent evidence syntheses have summarized rehabilitation strategies for RTS after ACLR, including BFR as one of several adjunctive interventions.25,26 For example, a recent systematic review/meta-analysis and an umbrella review on RTS strategies discussed BFR within a broader, multicomponent rehabilitation framework. 25 However, these reviews were broader in scope and were not restricted to randomized trials focusing specifically on postoperative BFR protocols and commonly pooled outcomes (eg, quadriceps strength, Lysholm/IKDC, pain, and range of motion [ROM]). In addition, psychological readiness outcomes were not consistently reported across postoperative BFR RCTs, which limits evidence synthesis for constructs such as fear of reinjury or kinesiophobia in the current body of trials. Therefore, there remains a need for a focused and updated synthesis restricted to postoperative BFR RCTs after ACLR, with explicit attention to protocol- and time point–related heterogeneity. In contrast to several recent reviews that primarily emphasized statistical significance, the present study additionally integrates time window–based synthesis and certainty-of-evidence interpretation Grading of Recommendations Assessment, Development and Evaluation (GRADE) to distinguish statistically from clinically meaningful effects.
Taken together, BFR training represents a promising adjunct to ACL rehabilitation, particularly in the early postoperative phase when high-load resistance exercise is contraindicated. The purpose of our study was to conduct a systematic review and meta-analysis of RCTs to evaluate the effects of BFR training on lower limb function, quadriceps strength, and knee pain after ACLR. We hypothesized that postoperative BFR training would result in greater improvements in quadriceps strength and patient-reported knee function compared with conventional rehabilitation alone, while having limited or inconsistent effects on pain and ROM.
Methods
Protocol Registration
This systematic review and meta-analysis was not prospectively registered in PROSPERO or other public registries. However, the eligibility criteria, outcomes of interest, and analytical methods were predefined prior to study selection and data extraction. The review was subsequently conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines. 35
Literature Search and Selection Criteria
This meta-analysis aimed to evaluate the effects of BFR training on lower limb function in patients following ACLR. A comprehensive literature search was conducted across multiple databases, including PubMed, Embase, EBSCO, PEDro, China National Knowledge Infrastructure (CNKI), the Cochrane Library, and Web of Science. The search period covered studies published between January 1, 2015, and August 30, 2025. The search strategy used combinations of keywords and Boolean operators, such as “Blood Flow Restriction,”“Anterior Cruciate Ligament Reconstruction,”“Knee Function,”“Strength,” and “Postoperative Rehabilitation” (eg, “Blood Flow Restriction AND ACL Reconstruction AND Strength”). Taking PubMed as an example, its specific search strategy is shown in the Appendix. We included RCTs evaluating BFR training following ACLR. Secondary research (systematic reviews, umbrella reviews, narrative reviews), conference abstracts, and nonrandomized studies were excluded. Scopus was not searched because institutional access was not available during the revision period. To mitigate the potential impact of not including Scopus, we searched multiple complementary databases with substantial overlap in biomedical and rehabilitation journal coverage and additionally performed manual screening of reference lists from included studies and relevant systematic reviews.
The search period was restricted to studies published between January 1, 2015, and August 30, 2025. Although BFR training was originally introduced in the 1960s, its application in postoperative ACLR rehabilitation—particularly within RCTs using contemporary surgical techniques, rehabilitation protocols, and standardized outcome measures—has largely emerged in the past decade. Earlier studies primarily focused on physiological mechanisms or nonsurgical populations and were less relevant to current ACL rehabilitation practice. Therefore, limiting the search to the past decade was considered appropriate to capture clinically applicable and methodologically comparable evidence.
Objective and Outcomes
The objective of this systematic review and meta-analysis was to determine whether postoperative BFR training, compared with conventional rehabilitation without BFR, improves the following prespecified primary outcomes after ACLR: (1) quadriceps strength (eg, peak torque (PT)/strength measures) and (2) patient-reported knee function (Lysholm and/or IKDC). Secondary outcomes included pain (visual analog scale [VAS]), ROM, and adverse events (when reported). Follow-up assessments were categorized as early (≤6 weeks), midterm (>6 to 12 weeks), and later follow-up (>12 weeks).
Inclusion and Exclusion Criteria
Studies needed to be an RCT (parallel-group or crossover if postoperative data were extractable). Based on the PICO (Population, Intervention, Comparator, and Outcome) framework, inclusion criteria comprised the following: human participants who underwent primary ACLR (any graft type), regardless of age or activity level. No restrictions were placed on sex, athletic status, or baseline physical activity, as these characteristics were variably reported across eligible trials. Studies were included provided that participants were free from major neuromuscular disorders, systemic inflammatory disease, or other conditions that would substantially interfere with postoperative rehabilitation. This approach was chosen to reflect the heterogeneous but clinically representative ACLR population encountered in routine practice and to avoid exclusion of otherwise eligible randomized trials because of inconsistent reporting of demographic details. Postoperative BFR training was applied to the operated limb during rehabilitation, in combination with exercise (eg, resistance training, walking, or neuromuscular training). BFR had to be delivered using a pneumatic cuff or similar device with a clearly described pressure prescription (eg, percentage of limb occlusion pressure [%LOP], mmHg, or percentage of systolic blood pressure [%SBP) and ≥1 supervised or protocol-defined training session. Patients underwent conventional postoperative rehabilitation without BFR (usual care), including identical exercise programs without cuff inflation, sham/low-pressure cuff, or standard low-load training. Primary outcomes were predefined as quadriceps strength (eg, isokinetic PT) and patient-reported knee function assessed by validated scales (Lysholm and IKDC), as these outcomes are most clinically relevant to postoperative recovery after ACLR. Secondary outcomes included pain (VAS), knee ROM, Knee injury and Osteoarthritis Outcome Score [KOOS] subscales, total work, and other reported functional or neuromuscular measures. Secondary outcomes were considered exploratory and interpreted with caution, particularly when based on a small number of trials or characterized by substantial heterogeneity. Finally, there needed to be
Exclusion criteria included (1) nonrandomized studies, observational designs, case series/case reports, conference abstracts without full text, editorials, and reviews; (2) studies in which BFR was applied preoperatively only (prehabilitation) without postoperative BFR data; (3) studies lacking extractable quantitative data for any prespecified primary/secondary outcomes; and (4) animal or cadaveric studies.
Study Selection and Data Extraction
Two reviewers (Y.H. and L.G.) independently screened titles and abstracts for eligibility, followed by independent full-text assessment of potentially relevant articles. Any disagreements were resolved by discussion and consensus; if consensus could not be reached, a third reviewer (X.Z.) adjudicated. Data extraction was performed independently by 2 reviewers (Y.H. and L.G.) using a standardized form, including study characteristics (eg, sample size, graft type), BFR protocol parameters (eg, cuff pressure prescription, frequency, duration), comparator details, follow-up time points, and prespecified outcomes. Objective functional performance outcomes (eg, hop tests/limb symmetry index, balance performance such as the Y Balance Test, gait parameters, and RTS readiness measures) were also prespecified for extraction when reported. When data were insufficiently reported (eg, missing mean and standard deviation or inconsistent metrics) or available in only 1 study, we synthesized these outcomes narratively rather than pooling them. Extracted data were cross-checked, and discrepancies were resolved by consensus or third-reviewer adjudication (R.Y.). When required information was missing or unclear, the corresponding authors were contacted for clarification. In addition, backward citation searching was performed by screening the reference lists of included trials and relevant reviews to identify any potentially eligible studies that were not captured through database searches.
Risk-of-Bias Assessment
The methodological quality of each included study was assessed using the Cochrane risk-of-bias tool. The following domains were evaluated: (1) randomization process: adequacy and transparency of random sequence generation; (2) blinding: implementation of blinding among participants, investigators, and outcome assessors; (3) attrition bias: completeness of follow-up and handling of missing data; (4) selective reporting: presence of selective outcome reporting; (5) other sources of bias: funding sources and potential conflicts of interest. Each study was rated as having a low, high, or unclear risk of bias. Two reviewers (Y.H. and R.Y.) independently performed the assessment, and discrepancies were resolved through discussion.
Assessment and Exploration of Heterogeneity
To explicitly address the protocol- and time-related heterogeneity highlighted in prior literature, we predefined postoperative recovery windows (early, ≤6 weeks; midterm, 6-12 weeks; later follow-up, >12 weeks) and conducted time window–based synthesis and subgroup analyses wherever data allowed. Statistical heterogeneity was evaluated using the I2 statistic, with values of <25% indicating low heterogeneity, 25% to 50% moderate heterogeneity, and >50% substantial heterogeneity. A random-effects model was applied when substantial heterogeneity was present. We explored potential sources of heterogeneity using prespecified subgroup analyses where data allowed, including postoperative follow-up window (early, midterm, later follow-up) and key protocol factors (eg, occlusion pressure prescription method, training frequency, and exercise modality). In addition, sensitivity analyses were conducted using a leave-1-out approach to evaluate the influence of individual studies on pooled estimates and heterogeneity. Metaregression was not performed because of the limited number of trials per outcome. We prespecified clinically relevant sources of heterogeneity, including follow-up window, intervention duration, and occlusion pressure prescription, based on prior BFR recommendations and rehabilitation phase considerations. Subgroup analyses were conducted when ≥2 studies were available per subgroup; otherwise, findings were interpreted as exploratory.
Certainty of Evidence (GRADE)
The certainty of evidence for each prespecified outcome was assessed using the GRADE approach, considering the following domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence derived from RCTs was initially rated as high certainty and was downgraded by ≥1 level when concerns were identified. Downgrading decisions were primarily based on methodological limitations, substantial heterogeneity (high I2 values), wide confidence intervals, and small total sample sizes. The overall certainty of evidence for each outcome was categorized as high, moderate, low, or very low.
Statistical Analysis
All statistical analyses were performed using Review Manager (RevMan, Version 5.4; Cochrane). Effect size estimation, for continuous outcomes, the weighted mean difference (WMD), or standardized mean difference (SMD) was calculated to compare the effects of BFR versus conventional rehabilitation on quadriceps strength and knee function. Heterogeneity assessment, between-study heterogeneity, was evaluated using the I2 statistic. Subgroup analyses were conducted based on intervention characteristics such as occlusion pressure and training frequency. When multiple follow-up assessments were reported, outcomes were extracted and synthesized according to the predefined follow-up windows (early, midterm, later follow-up). Prespecified subgroup analyses were planned where data allowed, including follow-up window (early vs midterm), pressure prescription method (individualized %LOP/%SBP vs fixed mmHg or nonindividualized), intervention duration (≤6 vs >6 weeks), and training frequency (2-3 vs 4 sessions/week). Sensitivity analyses were performed by sequentially excluding individual studies to test the robustness of pooled results. Use of alternative effect size metrics (eg, SMDs) was considered; however, because of inconsistent reporting of standard deviations and heterogeneous outcome definitions, such analyses were not feasible for most outcomes. A P value <.05 was considered statistically significant. Effect sizes were interpreted as small (SMD < 0.2), moderate (0.2 ≤ SMD < 0.5), or large (SMD ≥ 0.5). The clinical relevance of findings was discussed based on both effect magnitude and heterogeneity (I2). When multiple assessments were available within a study, we extracted data at the time point closest to each predefined window. Meta-analyses were performed separately within each follow-up window when ≥2 studies reported comparable outcomes; otherwise, findings were summarized narratively. We additionally explored intervention timing (time from surgery to BFR initiation) as a potential source of heterogeneity where data permitted. Publication bias was assessed using funnel plots and Egger regression test when ≥10 studies were available for a given outcome. When <10 studies were included, publication bias was not evaluated, due to insufficient statistical power.
Results
Study Selection and Characteristics
Study selection was conducted by 2 independent reviewers (Y.H. and L.G.) as described in the Methods. A total of 606 records were initially retrieved through systematic register searches. After removing duplicates, screening titles and abstracts, and conducting full-text assessments, 9 RCTs were finally included in this meta-analysis. ‖ The study selection process is presented in Figure 1.
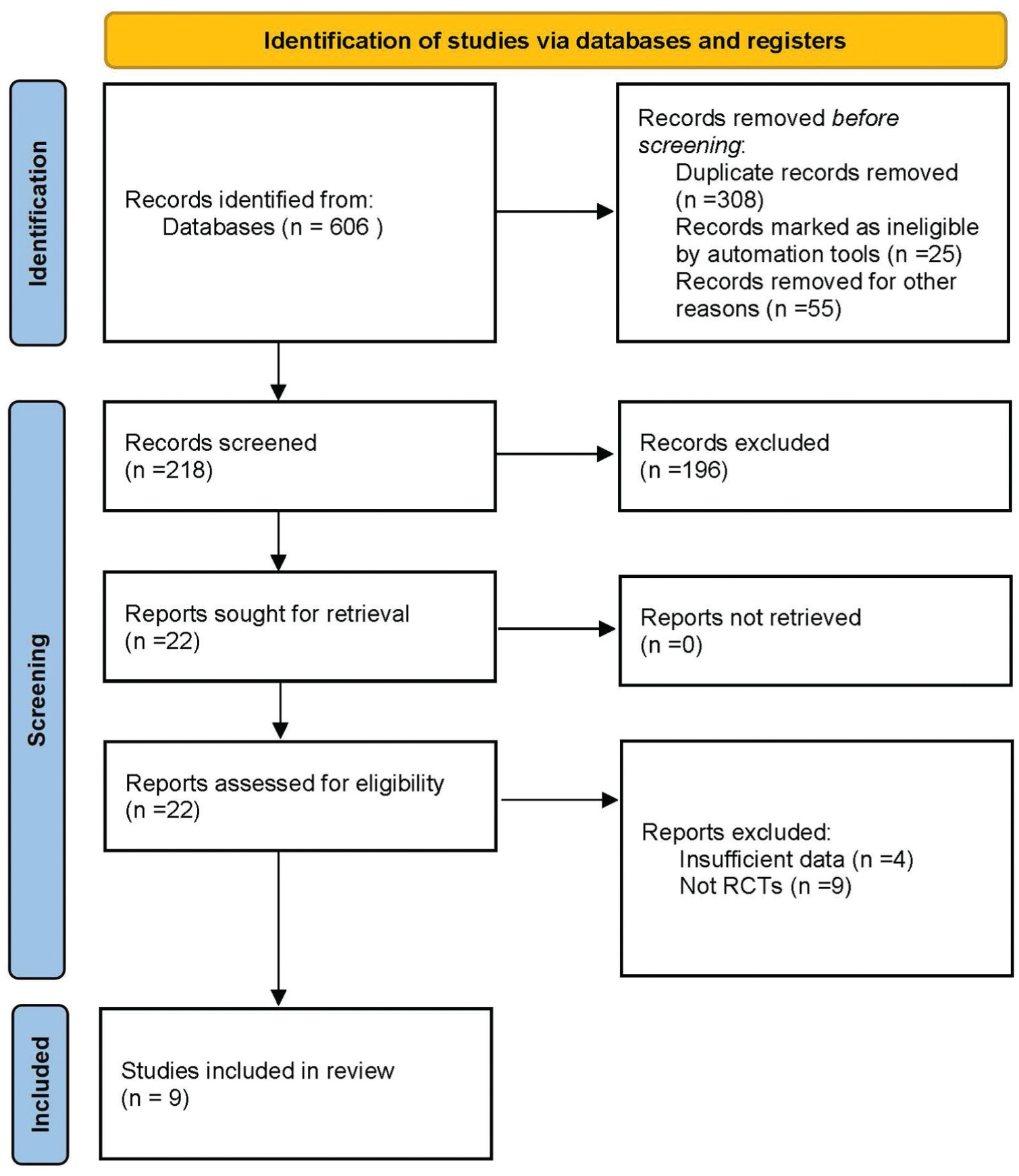
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram. RCT, randomized controlled trial.
The included RCTs were published between 2019 and 2024 and enrolled patients who had undergone ACLR. Sample sizes ranged from 24 to 82 participants, with intervention durations between 2 and 12 weeks and follow-up periods from 6 to 24 weeks. Notably, no included RCT reported follow-up beyond 24 weeks (≈6 months), and long-term outcomes (eg, ≥1 year) were unavailable. In total, 372 patients were analyzed (BFR group, 185; control group, 187). All included studies adopted randomized controlled designs, though variations existed in intervention protocols and assessment time points. Table 1 summarizes the characteristics of the included studies, including author, publication year, intervention protocol, and follow-up duration.
Characteristics of Included Studies in Meta-analysis a
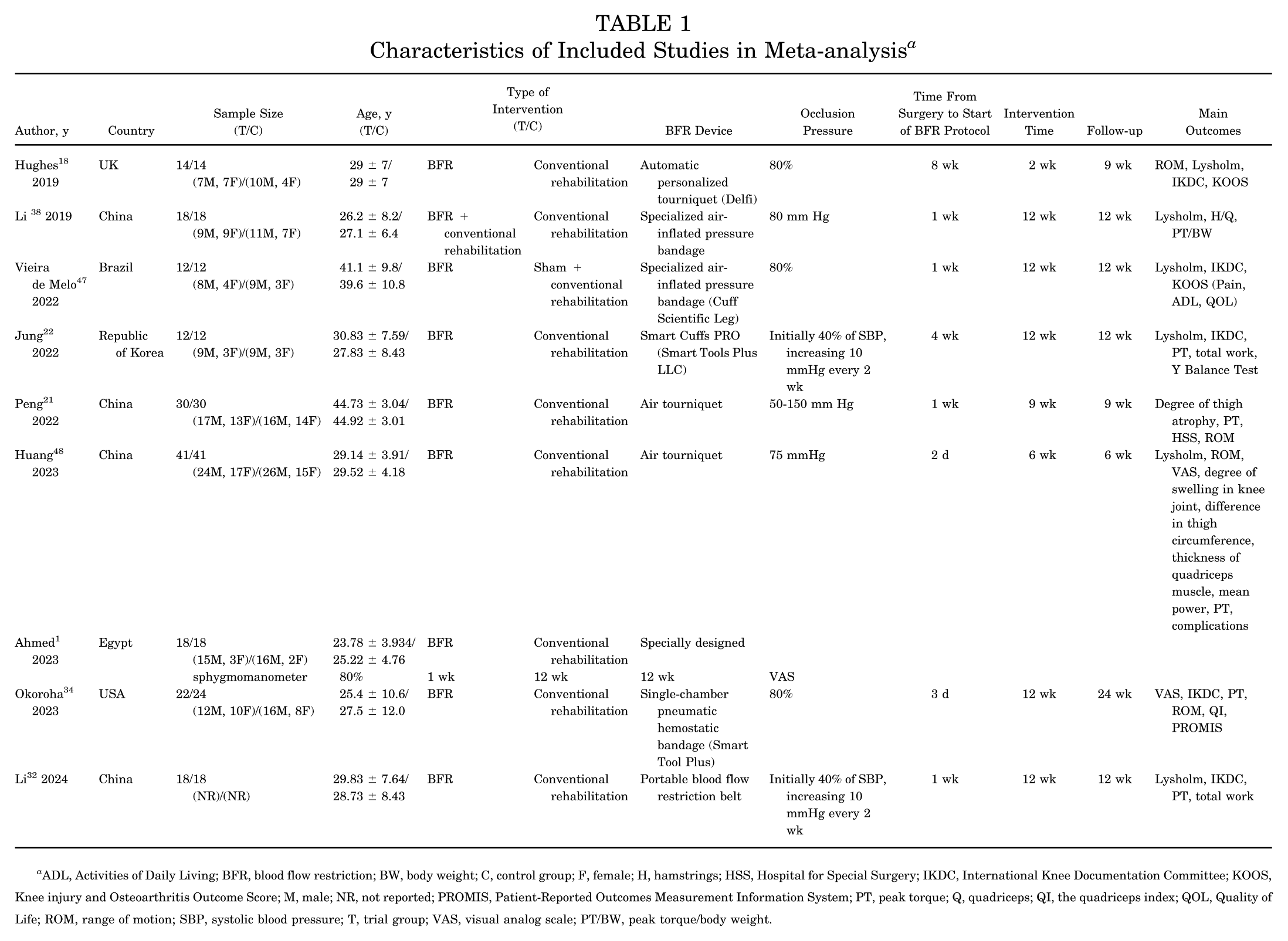
ADL, Activities of Daily Living; BFR, blood flow restriction; BW, body weight; C, control group; F, female; H, hamstrings; HSS, Hospital for Special Surgery; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; M, male; NR, not reported; PROMIS, Patient-Reported Outcomes Measurement Information System; PT, peak torque; Q, quadriceps; QI, the quadriceps index; QOL, Quality of Life; ROM, range of motion; SBP, systolic blood pressure; T, trial group; VAS, visual analog scale; PT/BW, peak torque/body weight.
Risk-of-Bias Assessment
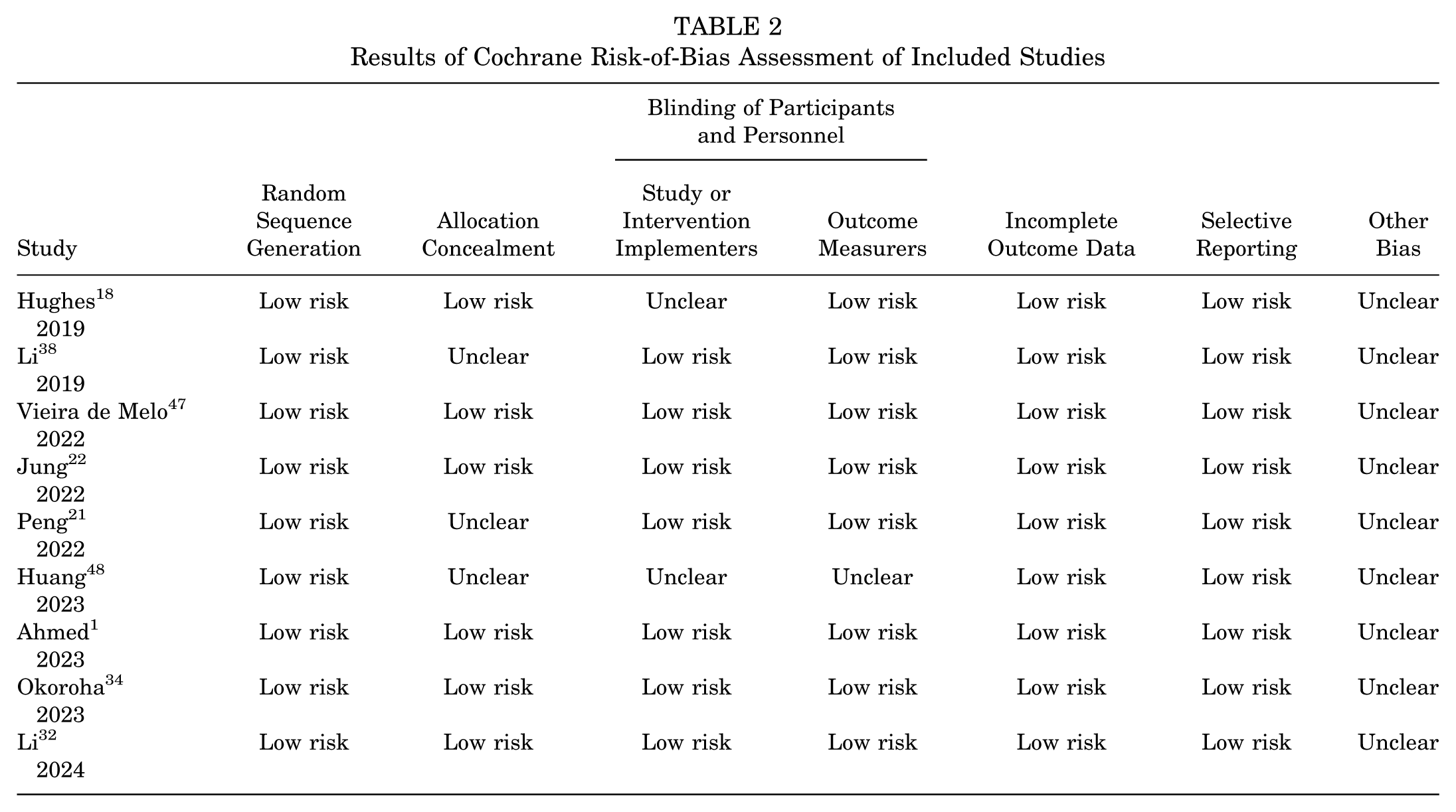
According to the Cochrane Handbook for Systematic Reviews of Interventions, most included trials demonstrated a low risk of bias in the domains of random sequence generation and data completeness. However, several studies had an unclear or high risk related to blinding of participants, personnel, and outcome assessors. Overall, the methodological quality of the included RCTs was considered acceptable, with a low overall risk of bias. Details of the quality assessment are presented in Table 2.
Results of Cochrane Risk-of-Bias Assessment of Included Studies
Meta-analysis Results
Lysholm Score
Six studies18,22,32,38,47,48 (n = 230) reported Lysholm scores. Substantial heterogeneity was observed among studies (I2 = 94%; P < .00001). Using a random-effects model, BFR training demonstrated a significantly greater improvement in Lysholm score compared with conventional rehabilitation (WMD, 5.75; 95% CI, 0.60-10.90; P = .03) (Figure 2).
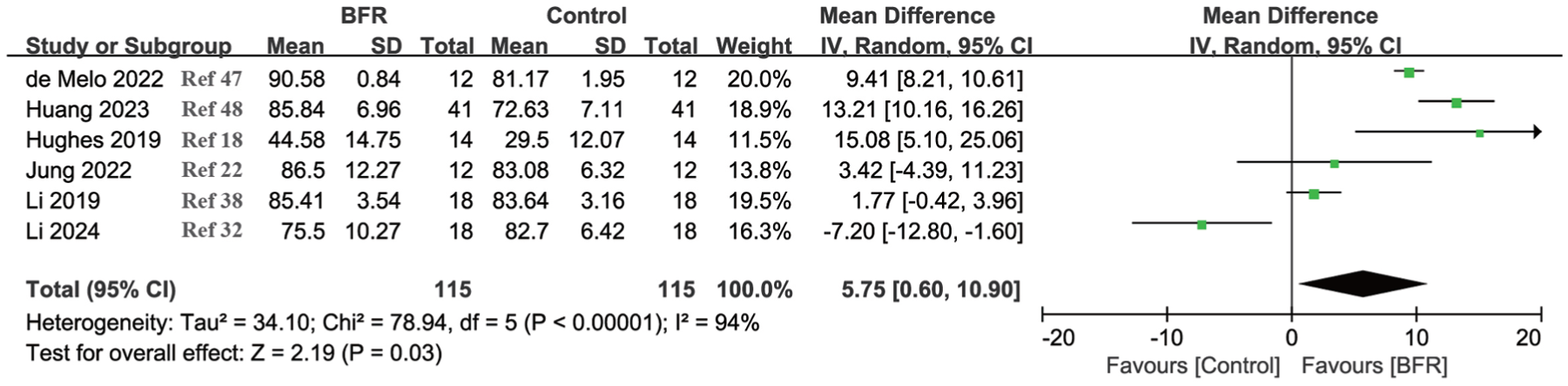
Forest plot for meta-analysis of Lysholm scores in patients with anterior cruciate ligament reconstruction. BFR, blood flow restriction; IV, inverse variance.
Considerable heterogeneity was observed for Lysholm scores (I2 = 94%). Subgroup analyses by postoperative follow-up window (early vs midterm) and BFR pressure prescription method (individualized vs nonindividualized) were attempted; however, the number of studies within each subgroup was small, precluding definitive subgroup inference. Leave-1-out sensitivity analyses showed that the direction of effect remained consistent, whereas heterogeneity remained high, suggesting that variability in rehabilitation phase, BFR protocols, and outcome assessment timing across trials likely contributed to the observed inconsistency. Across trials, BFR prescriptions varied substantially, which likely contributed to the very high I2. Differences in rehabilitation phase and the timing of BFR initiation (immediate vs delayed start) likely contributed to between-study heterogeneity.
A subgroup analysis based on intervention duration revealed that within short-term intervention (≤6 weeks), 2 studies18,48 (n = 110) showed a significant improvement (WMD, 13.37; 95% CI, 10.46 to 16.28; P < .00001), with no heterogeneity (I2 = 0%). Later follow-up (>6 weeks) revealed that 4 studies22,32,38,47 (n = 120) showed no statistically significant difference (WMD, 2.15; 95% CI, –4.42 to 8.71; P = .52), and high heterogeneity persisted (I2 = 95%) (Figure 3).
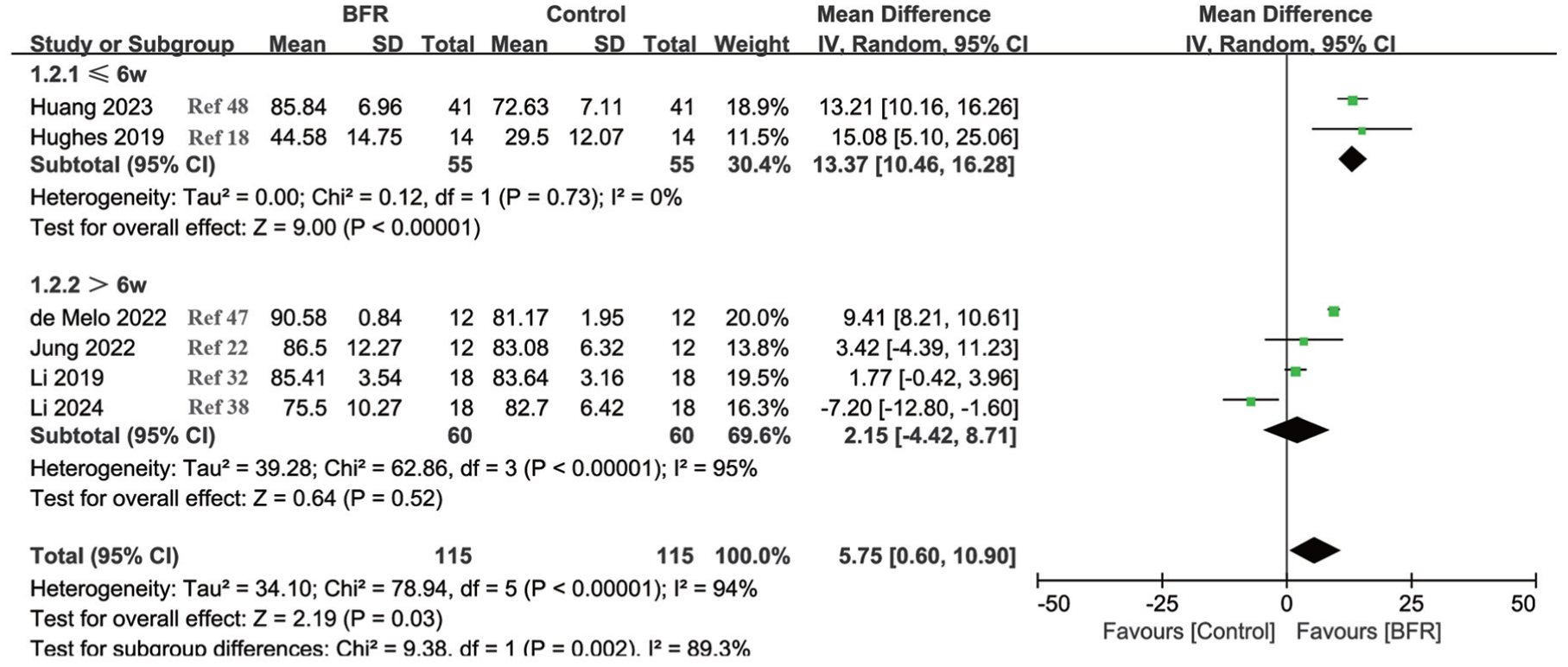
Forest plot for meta-analysis of Lysholm scores in patients with anterior cruciate ligament reconstruction by subgroup. BFR, blood flow restriction; IV, inverse variance.
International Knee Documentation Committee Score
Five studies18,22,32,34,47 (n = 158) assessed the IKDC score. Considerable heterogeneity was detected (I2 = 91%; P < .00001). The random-effects model showed no significant difference between BFR and control groups (WMD, 5.25; 95% CI, –3.01 to 13.51; P = .21) (Figure 4).
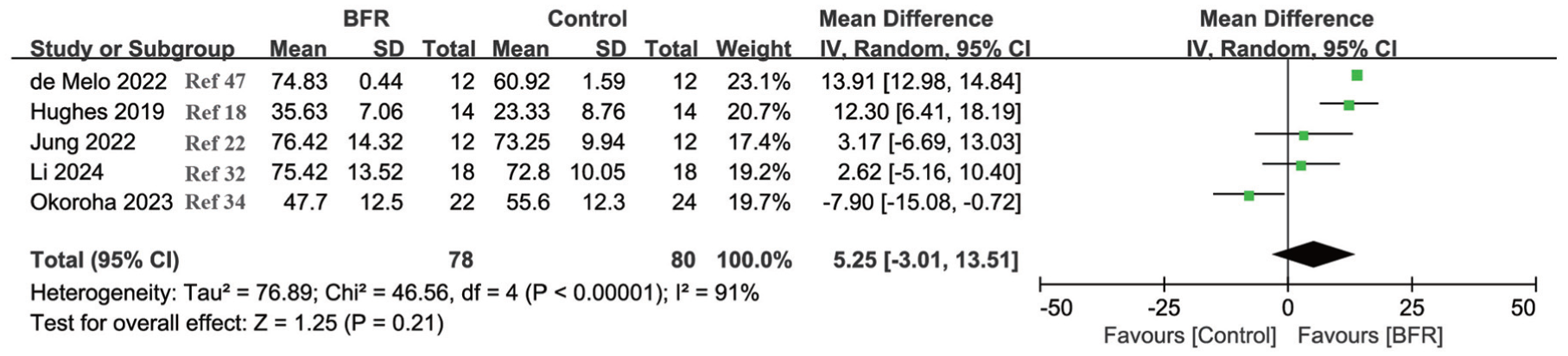
Forest plot for meta-analysis of International Knee Documentation Committee scores in patients with anterior cruciate ligament reconstruction. BFR, blood flow restriction; IV, inverse variance.
Substantial heterogeneity was present for IKDC outcomes (I2 = 91%). Prespecified subgroup analyses according to follow-up window and BFR protocol characteristics were explored, but the limited number of trials per subgroup restricted meaningful interpretation. Leave-1-out sensitivity analyses did not materially alter the pooled effect direction, and heterogeneity remained high, indicating that differences in study populations, intervention timing, and protocol implementation were likely sources of inconsistency.
Range of Motion
Three studies21,34,48 (n = 188) evaluated postoperative knee ROM. High heterogeneity was observed (I2 = 97%; P < .00001). The random-effects analysis indicated no significant difference between groups (WMD, 6.63; 95% CI, –7.66 to 20.92; P = .36) (Figure 5A).
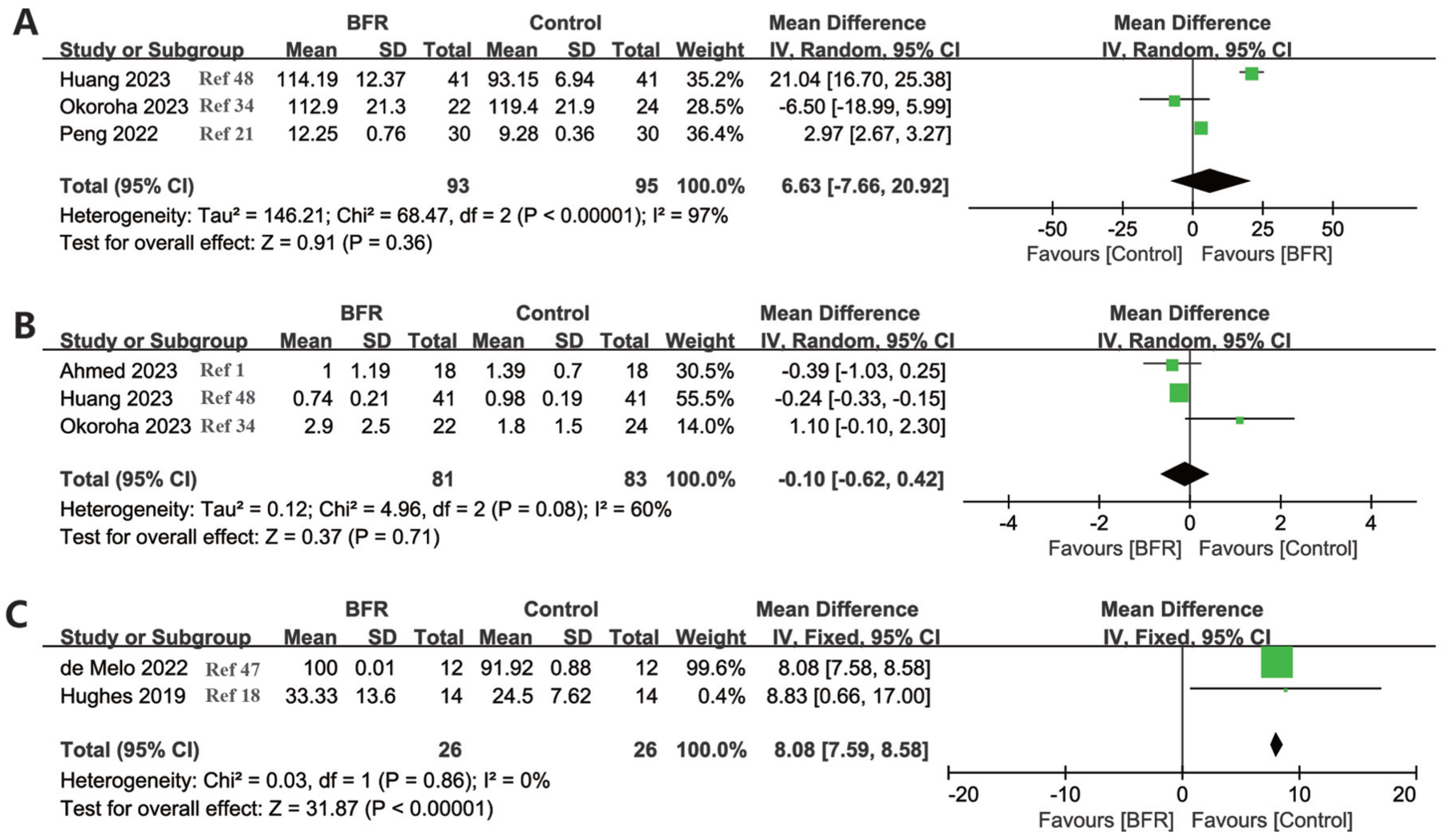
Forest plot for meta-analysis of (A) range of motion, (B) visual analog scale, and (C) Knee injury and Osteoarthritis Outcome Score Symptoms in patients with anterior cruciate ligament reconstruction. BFR, blood flow restriction; IV, inverse variance.
Very high heterogeneity was observed for ROM outcomes (I2 = 97%). Exploratory subgroup analyses by follow-up timing were attempted; however, these analyses were limited by the small number of studies and inconsistent reporting of ROM assessment methods. Leave-1-out sensitivity analyses demonstrated unstable pooled estimates with persistently high heterogeneity, suggesting that differences in rehabilitation phase, measurement protocols, and timing of ROM assessment substantially contributed to between-study variability. The ROM analysis was based on only a small number of trials with limited sample sizes, and the pooled estimate should therefore be interpreted cautiously.
VAS Score
Three studies1,34,48 (n = 164) reported VAS pain scores. Moderate heterogeneity was present (I2 = 60%; P = .08). Random-effects analysis revealed no significant difference in pain reduction between the BFR and control groups (WMD, –0.10; 95% CI, –0.62 to 0.42; P = .71) (Figure 5B). The VAS outcome was derived from few small RCTs, and the findings should be considered exploratory. Given the limited number of trials and small sample sizes, nonsignificant findings for pain and ROM should not be interpreted as evidence of no effect.
KOOS Symptoms
Two studies18,47 (n = 52) used the KOOS Symptoms subscale to evaluate knee outcomes. Heterogeneity was low (I2 = 0%; P = .86). The fixed-effects model showed that BFR training significantly improved KOOS symptoms compared with standard rehabilitation (WMD, 8.08; 95% CI, 7.59-8.58; P < .00001) (Figure 5C). We acknowledge that KOOS includes several clinically important domains. However, only the Symptoms subscale was available with extractable and comparable quantitative data across included trials. Other domains (Pain, Activities of Daily Living, Sports/Recreation, and Quality of Life) were not consistently reported or lacked sufficient data for synthesis and were therefore not included in pooled analyses. KOOS outcomes were reported in very few trials (and only 1 subscale was available for synthesis), limiting the robustness of inference. Using a random-effects model, the pooled estimate remained statistically significant and materially unchanged; results were consistent in fixed-effect sensitivity analysis.
Peak Torque
Six studies21,22,32,34,38,48 (n = 284) reported quadriceps PT outcomes. Between-study heterogeneity was low (I2 = 0%; P = .51). The fixed-effects analysis demonstrated a significant increase in quadriceps PT in the BFR group compared with the control group (WMD, 8.34; 95% CI, 7.47-9.22; P < .00001) (Figure 6A).
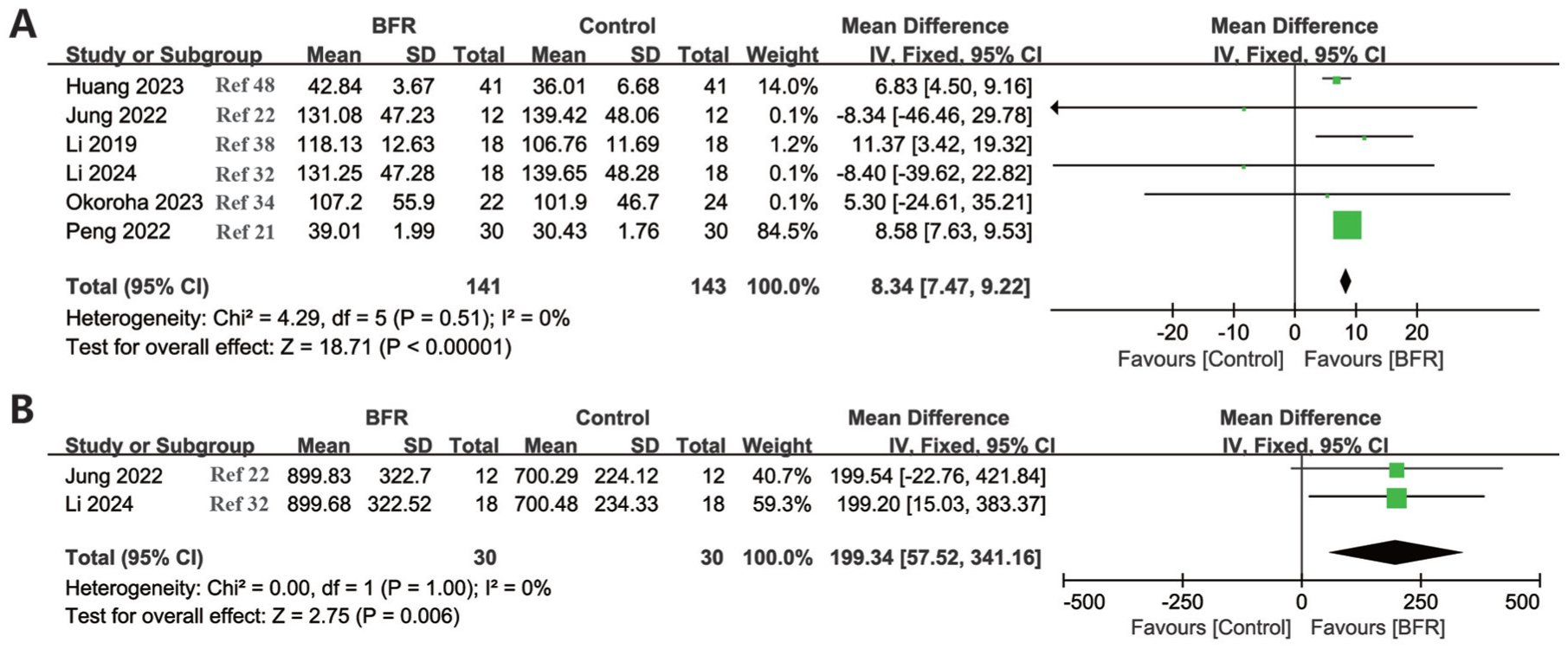
Forest plot for meta-analysis of (A) peak torque and (B) total work in patients with anterior cruciate ligament reconstruction. BFR, blood flow restriction; IV, inverse variance.
Total Work
Two studies22,32 (n = 60) assessed total work output. Heterogeneity was low (I2 = 0%; P≥.99). Fixed-effects analysis revealed that BFR training significantly enhanced total work output relative to conventional rehabilitation (WMD, 199.34; 95% CI, 57.52-341.16; P = .006) (Figure 6B). A random-effects model was applied because of the small number of included trials; the pooled effect and interpretation were consistent in fixed-effect sensitivity analysis. Total work was reported in a limited number of small trials, and the pooled estimate should be viewed as hypothesis generating.
Safety and Adverse Events
Reporting of adverse events was inconsistent across included trials. Three trials explicitly monitored or reported safety outcomes. Hughes et al 18 and Vieira de Melo et al 47 reported no adverse events/adverse effects, including no events such as deep vein thrombosis or other notable complications. Okoroha et al 34 recorded adverse effects and reported 1 participant withdrawal due to cuff intolerance, with no severe adverse events reported. One trial (Huang et al 48 ) reported postoperative complications, including lower-extremity venous thrombosis, chronic pain, and lower limb swelling, with a lower overall complication rate in the BFR group. The remaining trials did not provide extractable adverse-event data, precluding quantitative synthesis of harms.
Clinical Interpretability and Minimal Clinically Important Difference
To contextualize statistical significance with clinical relevance, we compared pooled changes in patient-reported outcome (PRO) measures with published minimal clinically important difference (MCID) thresholds after knee ligament reconstruction/ACLR. Reported MCIDs are approximately 9.9 points for Lysholm, 13.8 points for IKDC, and ~8 points for KOOS (100-point scale). In our analyses, although some pooled estimates reached statistical significance, the magnitude of improvement for Lysholm and IKDC did not consistently exceed these MCID thresholds, and several effects remained imprecise with substantial heterogeneity. Therefore, improvements in these PRO measures should be interpreted cautiously and may represent small to modest perceived benefits rather than clearly clinically important change at the individual patient level.
Certainty of Evidence (GRADE)
Based on the GRADE assessment, the certainty of evidence varied across outcomes (Table 3). Moderate-certainty evidence supported the effect of BFR training on quadriceps strength (PT). The certainty of evidence for patient-reported knee function (Lysholm and IKDC scores) and pain (VAS) was rated as low, primarily because of inconsistency across studies and imprecision related to small sample sizes and wide confidence intervals. Evidence for ROM and adverse events was rated as very low, reflecting very serious imprecision, heterogeneity, and incomplete reporting of safety outcomes.
Summary of Findings and Certainty of Evidence (GRADE) for Blood Flow Restriction Training After ACLR a
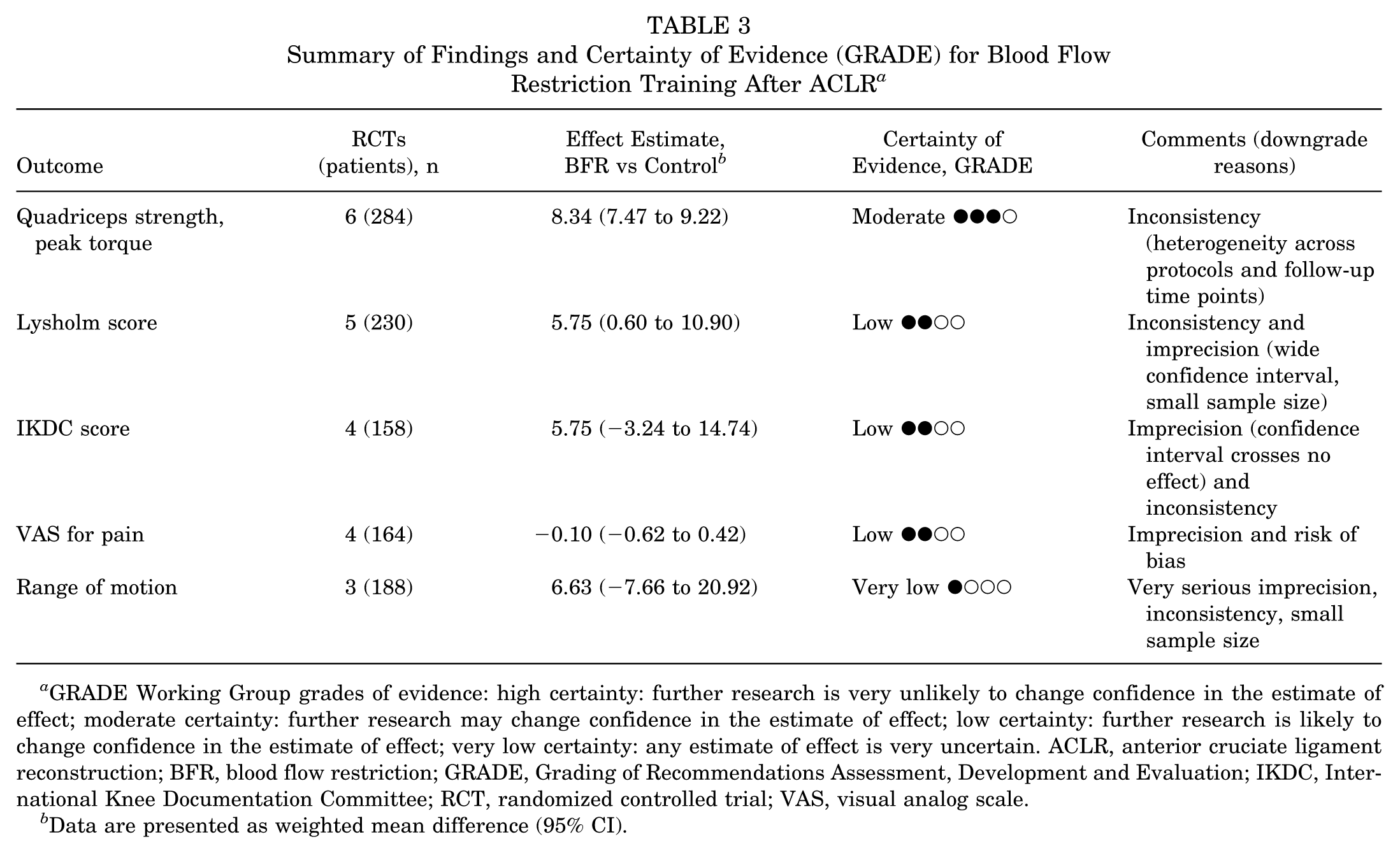
GRADE Working Group grades of evidence: high certainty: further research is very unlikely to change confidence in the estimate of effect; moderate certainty: further research may change confidence in the estimate of effect; low certainty: further research is likely to change confidence in the estimate of effect; very low certainty: any estimate of effect is very uncertain. ACLR, anterior cruciate ligament reconstruction; BFR, blood flow restriction; GRADE, Grading of Recommendations Assessment, Development and Evaluation; IKDC, International Knee Documentation Committee; RCT, randomized controlled trial; VAS, visual analog scale.
Data are presented as weighted mean difference (95% CI).
Sensitivity Analysis
Sensitivity analysis was performed by sequentially excluding each of the 9 included RCTs to examine its influence on the pooled estimates. ¶ No single study substantially altered the pooled estimates, indicating the stability and robustness of the findings.
Discussion
The major findings of this systematic review and meta-analysis synthesized evidence from 9 RCTs to evaluate the effects of BFR training after ACLR. # Pooled analyses showed that BFR improved Lysholm scores (WMD, 5.75; 95% CI, 0.60-10.90; P = .03) and quadriceps PT (WMD, 8.34; 95% CI, 7.47-9.22; P < .00001) and increased total work output (WMD, 199.34; 95% CI, 57.52-341.16; P = .006). In contrast, no significant between-group differences were observed for IKDC, VAS pain, or ROM (all P > .05). These findings suggest that BFR may facilitate early strength recovery, whereas evidence for broader functional improvement and pain reduction remains limited.
The significant improvement in Lysholm scores indicates that BFR training effectively enhances knee function and daily activity performance after ACLR. The Lysholm scale reflects knee stability, gait, and activity limitation; therefore, its improvement suggests that BFR may achieve rehabilitation effects comparable with high-load training while maintaining low mechanical stress on the joint. In contrast, although IKDC scores showed a positive trend, the difference did not reach statistical significance. This discrepancy may be attributed to variations in training protocols, postoperative phases, and assessment timing among included studies. Some trials have reported that BFR-induced functional improvements are primarily evident in the early postoperative period (6-12 weeks), whereas IKDC scores are more sensitive to mid- to long-term recovery outcomes.18,34
In this meta-analysis, BFR training also significantly increased quadriceps PT, highlighting its strong role in restoring muscle strength. Quadriceps atrophy and weakness are common after ACLR due to immobilization and reduced neural activation. While progressive resistance training is a core component of ACLR rehabilitation, higher external loads may be temporarily deferred or limited in the early postoperative phase because of pain, swelling, and graft protection considerations. BFR, by contrast, induces localized ischemia, hypoxia, and metabolic stress under low-load conditions, which stimulates the recruitment of type 2 muscle fibers, promotes hypertrophy, and enhances muscle power. Moreover, BFR has been shown to elevate the secretion of anabolic hormones such as growth hormone and insulin-like growth factor–1, thereby facilitating muscle protein synthesis and mitigating disuse atrophy. 1 In addition to improving PT, BFR training also enhanced total work output, suggesting an improvement in overall muscular endurance capacity. This finding further supports the effectiveness of BFR as an early-stage intervention to counteract postoperative muscle deconditioning. Taken together, these results indicate that BFR training can effectively enhance quadriceps strength and knee function during the early recovery phase following ACLR, providing a foundation for subsequent high-load or sport-specific rehabilitation. However, its contribution to long-term comprehensive functional restoration still warrants further investigation through high-quality, large-sample clinical trials.
The meta-analysis revealed that BFR training did not significantly improve pain (VAS scores) or knee ROM (P > .05). This finding is consistent with previous clinical studies suggesting that BFR has limited effects on postoperative pain relief and joint mobility. 34 Several factors may account for this result: (1) substantial variations in intervention intensity, cuff pressure, and training frequency across studies; (2) the subjective nature of VAS and ROM assessments, which are influenced by individual pain thresholds and compliance; and (3) the relatively short intervention duration in most trials (6-8 weeks), which may be insufficient to reflect long-term joint mobility changes. Nevertheless, some studies have proposed that BFR may indirectly alleviate postoperative pain and swelling by improving local microcirculation, reducing muscle tension, and attenuating inflammatory responses. 18 Therefore, BFR may still play an adjunctive role during the early postoperative rehabilitation phase.
The primary findings of this study are consistent with several recent systematic reviews and RCTs. Charles et al 4 and Colapietro et al 7 reported in their reviews that BFR effectively attenuates early quadriceps atrophy and enhances strength recovery following ACLR, while requiring only 20% to 30% of the maximal training load, thereby substantially reducing joint stress. Similarly, Okoroha et al 34 found that perioperative BFR significantly improved Lysholm scores and quadriceps strength at 6 weeks postoperatively, aligning with the present results. Hughes et al 18 further indicated that BFR training achieves strength and hypertrophy outcomes comparable with traditional high-load resistance training, though its functional benefits may vary depending on rehabilitation stage and concurrent training modalities. Likewise, Erickson et al 11 confirmed through magnetic resonance imaging and muscle physiology analyses that BFR enhances muscle fiber cross-sectional area and oxidative metabolism, but has limited effects on subjective pain perception.
Conversely, some studies have questioned the clinical efficacy of BFR. Herman et al 15 observed in a real-world cohort that BFR did not markedly improve quadriceps strength in patients undergoing ACLR using a quadriceps tendon graft. Curran et al 9 suggested that combining BFR with high-intensity resistance training might reduce adherence and increase fatigue risk. In contrast, Okoroha et al 34 and Roman et al 40 demonstrated that early or perioperative BFR significantly improved muscle strength and functional recovery at 6 to 12 weeks postoperatively, with particularly pronounced effects in younger populations.
The rehabilitative benefits of BFR are primarily attributed to the mechanism of metabolic stress activation. BFR induces localized hypoxia and lactate accumulation, which promote early recruitment of type 2 muscle fibers and trigger endocrine responses that increase the secretion of growth hormone and insulin-like growth factor-1. These hormonal changes activate the Akt/mTOR signaling pathway, thereby enhancing protein synthesis and muscle hypertrophy. 16 Mechanistically, these pathways are most directly expected to improve muscle strength and hypertrophy under low external loads, which aligns with our pooled findings showing the most consistent benefits in quadriceps strength–related outcomes (eg, PT). Furthermore, BFR has been shown to increase muscle fiber recruitment and electromyographic activity, contributing to improved neuromuscular control in the early stages of recovery. 18 However, because objective neuromuscular control and functional performance measures (eg, hop tests, symmetry indices, balance/movement-control outcomes) were inconsistently reported across trials, our meta-analysis cannot determine whether these neuromuscular changes translate into improved limb symmetry or RTS readiness. Kacin et al 23 reported that BFR upregulates intramuscular Akt/mTOR signaling and vascular endothelial growth factor expression, suggesting its role in promoting muscle regeneration and microcirculatory improvement. Recent imaging and biochemical studies have provided additional mechanistic evidence. Erickson et al 11 observed enhanced mitochondrial density and capillary perfusion in the quadriceps following BFR, while Jack et al 20 reported preservation of lower limb bone mineral density and muscle mass. This dual mechanism—metabolic and circulatory—may help explain the potential value of BFR in facilitating early-stage muscle recovery when high external loads are temporarily limited. In contrast, outcomes reflecting broader symptoms and patient-perceived function (eg, IKDC/KOOS domains) as well as pain (VAS) and ROM were not consistently improved in our pooled analyses and were often highly heterogeneous or imprecise; therefore, mechanistic inferences should not be overextended to these endpoints. Moreover, BFR has been found to attenuate inflammatory responses by reducing leukocyte infiltration and downregulating proinflammatory cytokines such as tumor necrosis factor–α. 13 While this anti-inflammatory pathway could plausibly relate to symptom modulation, the current pooled evidence does not confirm reliable improvements in pain or ROM, suggesting that any such effects may be context dependent (eg, timing, pressure prescription, concomitant rehabilitation) and require further confirmation. However, its role in pain relief and ROM improvement remains unclear. Hughes et al 18 noted that BFR may transiently cause local discomfort or pressure-related pain, though it is generally well tolerated and safe. Some studies have suggested that moderate pressure (approximately 60% of LOP) may optimize the balance between training efficacy and discomfort perception. 31 Beyond mechanical loading, rehabilitation-induced adaptations may also be influenced by changes in the local biological and metabolic microenvironment, which has been discussed in the broader context of tissue regeneration and repair. 5 Taken together, the mechanistic literature most strongly supports strength-related benefits of BFR under low-load conditions, whereas evidence remains insufficient to conclude consistent effects on pain, ROM, or higher-level functional recovery. It should be noted that mechanistic explanations are largely extrapolated from physiological and experimental studies and were not directly evaluated in the included clinical trials; therefore, they should be interpreted cautiously.
A potential clinical advantage of BFR is that it may facilitate early quadriceps loading under low external loads. While progressive resistance training can effectively enhance muscle strength, load progression in the early postoperative phase should be individualized and guided by symptoms and graft-healing considerations. BFR can be used as an adjunct/bridge strategy to achieve meaningful neuromuscular stimulus at low external loads (eg, 20%-30% 1RM), particularly when higher loads are temporarily limited early after surgery.10,16 Li et al 28 and Fraca-Fernández et al 12 demonstrated that BFR training promotes earlier restoration of gait function and reduces postoperative muscle atrophy compared with conventional rehabilitation. Furthermore, BFR programs integrated with home-based or telemonitored rehabilitation systems have been proven safe and feasible. 43 However, its clinical application requires careful monitoring of occlusion pressure and individualized physiological responses. Current international guidelines recommend setting the restriction pressure at 60% to 80% of the individual's LOP, performing 3 to 4 sets of 15 to 30 repetitions per session, 2 to 3 sessions per week, for 6 to 12 weeks to ensure both efficacy and safety.7,39
Clinical Interpretability and MCID
To distinguish statistical significance from clinical relevance, pooled improvements in PROs were interpreted in relation to published MCID thresholds following ACLR. Reported MCIDs are approximately 9.9 points for the Lysholm score, 13.8 points for the IKDC score, and around 8 points for KOOS on a 100-point scale. In the present meta-analysis, although some pooled effects reached statistical significance, the magnitude of improvement for Lysholm and IKDC did not consistently exceed these MCID thresholds, and several estimates were further limited by substantial heterogeneity and imprecision. 30 Therefore, observed improvements in these PRO measures likely reflect small to modest perceived benefits rather than clearly clinically meaningful recovery at the individual patient level. For objective strength outcomes such as PT, established MCID thresholds are not consistently available. Accordingly, clinical relevance is more appropriately interpreted using criterion-based benchmarks commonly applied in ACL rehabilitation, such as limb symmetry indices ≥90% and RTS strength criteria, rather than absolute torque differences alone. 24
The variability in outcomes among studies may be partly attributed to heterogeneity in intervention protocols and study designs. First, substantial differences exist in BFR parameters, including cuff width, inflation pressure (typically 60%-80% LOP), training frequency (2-4 sessions per week), and intervention duration (2-12 weeks). Each of these factors can significantly influence the magnitude of training adaptation. Second, inconsistent timing of postoperative assessments represents another important source of variation. Some studies evaluated outcomes at 6 or 8 weeks postsurgery, while others extended follow-up to ≥3 months, making direct comparison between short- and midterm effects difficult. Importantly, the optimal postoperative timing for initiating BFR remains unclear. Across included RCTs, BFR started as early as 2 to 3 days after surgery and as late as 8 weeks. However, few trials were available within each timing category and outcome reporting was inconsistent, precluding robust subgroup inference. Therefore, our findings should not be interpreted as evidence for a specific “best” initiation window, and timing-specific recommendations require dedicated RCTs.
Interpretation of Evidence Certainty
The GRADE assessment provides important context for interpreting the findings of this meta-analysis. Although BFR training demonstrated beneficial effects on quadriceps strength, the moderate certainty of evidence indicates that further well-designed trials may still influence the magnitude of this effect. For knee function, pain, and ROM outcomes, the low to very low certainty of evidence suggests that current findings should be interpreted cautiously. These limitations are largely attributable to substantial heterogeneity in BFR protocols, short follow-up durations, and small sample sizes across trials. In addition, adverse events were not consistently or systematically reported, precluding confident conclusions regarding safety. Future randomized trials with standardized BFR protocols, longer-term follow-up, and comprehensive reporting of both functional and safety outcomes are warranted to strengthen the certainty and clinical applicability of the evidence.
Clinical Implications of Heterogeneity
Very high statistical heterogeneity was observed for several pooled outcomes (eg, Lysholm, IKDC, and ROM), which has important clinical implications and limits direct generalization of the pooled estimates to routine practice. This heterogeneity likely reflects meaningful between-trial differences in both BFR prescription and postoperative timing. First, BFR protocols varied substantially across studies, including pressure calibration methods (individualized %LOP vs fixed pressures), cuff width/type, exercise modality, training frequency and duration, and integration within broader rehabilitation programs, all of which are known to influence the physiological stimulus and training response. 37 Second, outcomes were assessed at heterogeneous postoperative phases and follow-up time points. Given that recovery trajectories for strength, pain, ROM, and function after ACLR are highly time dependent, pooling across dissimilar phases may dilute phase-specific effects and inflate inconsistency. 46 Taken together, the high heterogeneity suggests that BFR effects are likely context dependent—most plausibly as an adjunct to facilitate early quadriceps loading when high external loads are temporarily limited—while evidence for broader functional recovery remains uncertain. Clinicians should therefore interpret pooled estimates cautiously and prioritize individualized, criterion-driven progression rather than assuming uniform benefits across protocols and rehabilitation phases. Although random-effects models were used, such extreme heterogeneity indicates that the pooled estimate represents a mean across markedly different protocols and time points; therefore, clinical generalizability is limited and the results should be interpreted with caution.
Clinical Application and Translational Relevance
In practical ACLR rehabilitation, the primary clinical value of BFR is as an adjunct/bridge strategy to increase quadriceps loading when high external loads are temporarily limited (eg, early postoperative pain, swelling, or graft protection considerations). Based on our findings, BFR may help augment early strength-related outcomes (eg, PT/strength measures), which could support earlier progression from very low-load activation exercises toward progressive strengthening when symptoms permit. However, improvements in PROs were inconsistent and did not consistently exceed published MCID thresholds, and pooled effects for pain and ROM were not robust. Therefore, BFR should not be used as a stand-alone determinant for advancing rehabilitation phase or for RTS decisions. Clinically, progression of loading should remain criterion driven and individualized, using standard parameters such as symptom response (pain and effusion), restoration of ROM, movement quality, and objective strength benchmarks (eg, limb symmetry indices), rather than a reliance on statistically significant group-level changes alone. Importantly, objective functional performance measures (eg, hop tests, gait/balance metrics) and RTS readiness criteria were inconsistently reported across trials, precluding quantitative synthesis. As a result, the current evidence cannot determine whether BFR accelerates readiness for advanced training phases or improves RTS outcomes. Future trials should incorporate standardized functional performance batteries and criterion-based RTS outcomes to clarify translational impact.
Limitations
This study has several limitations. First, the review was not prospectively registered, which may raise concerns about selective reporting despite our predefined methods and independent screening/data extraction. Second, the evidence base was limited, with small RCTs and few studies for several outcomes, leading to imprecision—particularly for secondary endpoints (eg, ROM, VAS, KOOS, total work). Third, substantial clinical and statistical heterogeneity across BFR protocols and outcome assessments (including very high I2 for some outcomes) limits the interpretability and generalizability of pooled estimates. Fourth, follow-up was short (6-24 weeks) with no ≥1-year data, precluding conclusions on long-term function, RTS, and safety. Finally, adverse events and objective performance outcomes were inconsistently reported, and publication bias cannot be excluded. Larger, well-designed RCTs with standardized protocols, longer follow-up, and systematic harms reporting are needed.
Future research should address these limitations by establishing standardized BFR rehabilitation protocols that clearly define the optimal training intensity, occlusion pressure, and intervention duration; conducting large-scale, multicenter, high-quality RCTs to confirm the long-term efficacy and safety of BFR training; integrating biological markers and imaging assessments to further elucidate the mechanisms through which BFR promotes muscle recovery and joint healing; and exploring the synergistic effects of BFR with other rehabilitation modalities, such as neuromuscular training or electrical stimulation, to develop individualized, evidence-based rehabilitation strategies.
Conclusion
Our study demonstrated that BFR training may promote early recovery of quadriceps strength and selected aspects of knee function after ACLR under low-load conditions. BFR appears feasible and generally well tolerated in the included trials; however, safety conclusions are limited by inconsistent adverse-event reporting. Its effects on pain relief, joint mobility, and long-term functional recovery require further investigation.
Footnotes
Appendix
Final revision submitted February 2, 2026; accepted March 8, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not required for this study.
Data Accessibility Statement
The data sets generated and/or analyzed during the current systematic review and meta-analysis are available from the corresponding author upon reasonable request. All data were extracted from previously published studies, which are publicly accessible through databases such as PubMed, Embase, Cochrane Library, Web of Science, PEDro, EBSCO, and CNKI.