
Abstract
Background:
Postless traction has been developed to avoid perineal post-related complications in hip arthroscopy. While it is reported to reduce groin-related issues, its effect on overall nerve injury rates, as well as potential new complications such as lumbosacral discomfort, remains unclear.
Hypothesis:
Postless traction may be linked to improved clinical outcomes but may carry an increased risk of lumbosacral discomfort.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent postless hip arthroscopy were compared with matched patients who underwent conventional post-assisted traction. Patient-reported outcomes, including the Hip Outcome Score–Activities of Daily Living and Sports subscales (HOS-ADL and HOS-SS), the International Hip Outcome Tool–12 (iHOT-12), and the modified Harris Hip Score (mHHS), were collected via follow-up over a mean period of 476 days, ranging from 404 to 560 days. Complications including sensory deficits, perineal injury, and lumbosacral discomfort were also assessed.
Results:
A total of 32 patients who underwent postless hip arthroscopy were compared with 64 patients in the control group undergoing post-assisted traction. There was no significant difference in the overall rate of sensory nerve injury between the 2 groups (31.3% vs 32.8%; P = .88). No perineal soft tissue injuries occurred in the postless group, compared with 1 case (1.6%) in the control group (P > .05). However, the incidence of lumbosacral discomfort was significantly higher in the postless group (28.1% vs 6.3%; P = .008). The postless group showed significantly better scores on the HOS-SS (76.81 ± 21.07 vs 66.78 ± 21.30; P = .009) and iHOT-12 (80.57 ± 14.03 vs 65.65 ± 18.00; P < .001), while no differences were found in HOS-ADL or mHHS.
Conclusion:
Postless hip arthroscopy is associated with superior patient-reported functional outcomes. However, it shows no reduction in the overall rate of sensory nerve injury and is linked to a significantly higher risk of postoperative lumbosacral discomfort.
Keywords
Hip arthroscopy has become widely utilized in the treatment of various intra-articular hip disorders. To gain access to the joint, traction of the operative limb is required. Traditionally, this has been accomplished using a perineal post to provide countertraction. However, numerous studies have demonstrated that this technique is associated with a range of complications, including perineal soft tissue injuries and nerve impairment leading to sensory disturbances.1,4,16,19 Although most of these complications are transient, permanent damage has also been reported. 9 Due to differences in patient populations, surgical techniques, postoperative assessment methods, and definitions of complications across centers, reported complication rates vary considerably, ranging from 1.4% to 74%.3,5,9
These complications are thought to stem from prolonged perineal pressure exerted by the post, 10 which has led to the development of postless traction techniques. While specific techniques vary among centers, most studies describe placing the patient in a Trendelenburg position with 10° to 20° of head-down tilt, utilizing both the friction between the patient and the operating table and the gravitational component along the table to counteract the applied traction force on the lower limb. Compared with post-assisted hip arthroscopy, multiple studies have demonstrated favorable outcomes and reduced complication rates using this method,11,12,22 with Mei-Dan et al 14 reporting no groin-related complications in >1000 consecutive cases. As such, postless traction has gained increasing recognition and adoption.
Traction-related complications may also be associated with intraoperative factors, including the magnitude and duration of traction. 21 In particular, postless techniques typically require lower distraction forces,1,15 which may enhance procedural safety.
Nevertheless, in our clinical practice, we have observed several cases of postoperative sensory deficits in the operative limb following postless hip arthroscopy—findings inconsistent with previous literature. Moreover, many patients reported postoperative discomfort in the lumbosacral region, a factor that may negatively affect clinical outcomes and has received limited attention in prior studies.
Therefore, the purpose of this study was to investigate whether postless hip traction is superior to conventional post-based methods and to assess whether postless traction is associated with an increased risk of lumbosacral discomfort. We hypothesized that postless traction would be linked to improved patient outcomes although it would also carry an increased risk of postoperative lumbosacral discomfort.
Methods
Patients
A retrospective analysis was performed on 32 consecutive patients who underwent perineal postless hip arthroscopy for femoroacetabular impingement syndrome (FAIS) at the sports medicine clinic of our department between October 2023 and March 2024. A control group of 64 patients was selected at a 1:2 ratio from those who underwent hip arthroscopy with the use of a perineal post between March 2017 and July 2022. Matching was performed based on baseline demographic characteristics (age, sex, and body mass index), intraoperative diagnoses and surgical managements. As shown in Table 1, no significant differences were observed between the 2 groups in these aspects. The inclusion criteria were (1) a confirmed diagnosis of FAIS requiring arthroscopic treatment and (2) complete medical and operative records. The exclusion criteria comprised (1) previous hip surgery, (2) avascular necrosis of the femoral head, (3) Ehlers-Danlos syndrome, (4) Legg-Calvé-Perthes disease, and (5) other pathologies including pigmented villonodular synovitis, osteoid osteoma, synovial chondromatosis, and rheumatologic diseases (Figure 1). This study was approved by the ethics committee of our hospital.
Baseline Demographic, Diagnostic, and Surgical Characteristics of Patients a
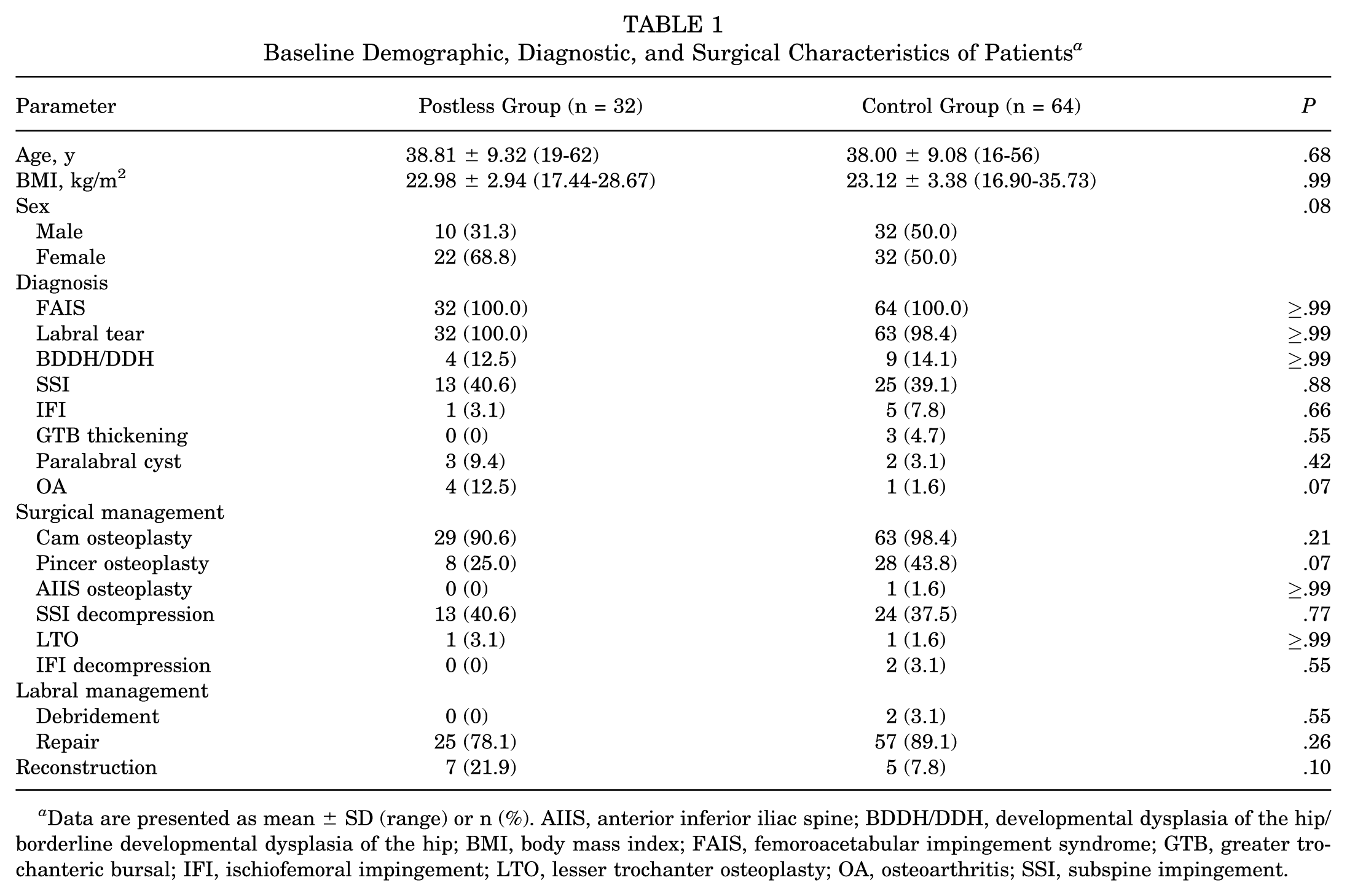
Data are presented as mean ± SD (range) or n (%). AIIS, anterior inferior iliac spine; BDDH/DDH, developmental dysplasia of the hip/ borderline developmental dysplasia of the hip; BMI, body mass index; FAIS, femoroacetabular impingement syndrome; GTB, greater trochanteric bursal; IFI, ischiofemoral impingement; LTO, lesser trochanter osteoplasty; OA, osteoarthritis; SSI, subspine impingement.
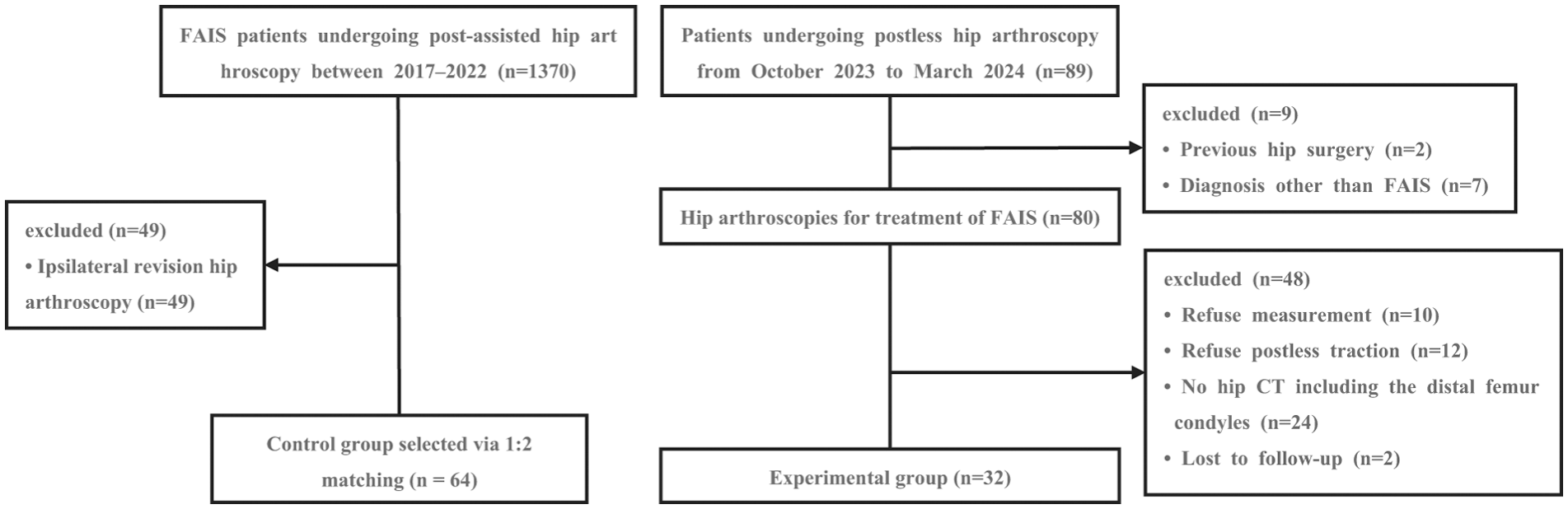
Flowchart illustrating the patient selection process. CT, computed tomography; FAIS, femoroacetabular impingement syndrome.
Surgical Method
As shown in Figure 2, for patients undergoing conventional hip arthroscopy with perineal post traction, they were positioned supine on a hip traction table after the administration of either general or spinal anesthesia. A perineal post with a 20-cm diameter was applied to provide countertraction. The operative limb was secured with a hip positioning apparatus (Smith & Nephew). The patient's feet were placed in traction boots and initial traction was applied. Then, the boots were pulled to distract the hip joint to a working width ranging from 12 to 20 mm. Fluoroscopic guidance was employed to assess both the positioning and the distraction width of the bony hip joint space. The measurement was taken from the most lateral point of the acetabular sourcil, along its line, and perpendicular to the surface of the femoral head. A mobile radiographic unit (OEC One CFD; General Electric) was used for imaging and measurements. Once adequate distraction was confirmed, a 22-gauge puncture guide needle (diameter, 1.2 mm) (Smith & Nephew) was introduced under fluoroscopy to establish the anterolateral portal. Subsequently, a midanterior portal was created, and the articular capsule from the 12-o’clock to 3-o’clock position (external and anterior region) was incised. This approach enabled access to the central compartment, allowing for the management of intra-articular pathologies such as labral tears, pincer-type FAIS, and chondrolabral lesions. Following treatment of the central compartment, the arthroscope was advanced to the peripheral compartment to address cam-type deformities. Resection adequacy was verified via intraoperative fluoroscopy and dynamic hip assessment. Routine capsular closure was performed to complete the procedure.

Surgical illustration. (A and B) Hip arthroscopy with perineal post: the patient was positioned supine on a hip traction table. A perineal post (20 cm in diameter) was applied for countertraction. The operative limb was secured using a hip positioning apparatus, and both feet were placed in traction boots. (C) Postless hip arthroscopy: the patient was positioned supine on the traction table. The contralateral arm was secured to an abduction frame, while the ipsilateral arm was suspended. Countertraction was achieved via a padded strap securing the contralateral inguinal region and an abdominal belt. Both feet were secured in traction boots, with the contralateral leg abducted (45°) and the affected limb extended and internally rotated (15°). The table was tilted to ~10° Trendelenburg.
For patients treated with a novel postless hip arthroscopy technique, they were positioned supine on the operating table, with the contralateral arm fixed to an abduction post and the ipsilateral arm suspended and fixed on an anterior chest brace. The torso was fully in contact with the traction sheet covering the surface of the table, and the buttocks were aligned with the edge of the surgical table. To protect pressure points, both feet and ankles were cushioned with cotton padding and then secured within standard traction boots. The contralateral leg was abducted to 45°, while the operative leg was kept in full extension with approximately 15° of internal rotation. A thickened safety strap, cushioned with cotton padding, was fastened over the contralateral inguinal region, firmly anchoring the patient to the table. Additionally, an abdominal belt was applied to secure the lower trunk against the operating surface, thereby enhancing friction and preventing the patient from shifting or falling. Following complete setup, the table was gradually tilted into a 10° Trendelenburg position, elevating the lower extremities relative to the head. This positioning utilized the friction between the patient's back and the operating table, combined with the gravitational component along the table, to counteract the traction force applied to the lower limb. The following surgical procedure was identical to that used in the perineal post traction technique.
All procedures were performed by a senior attending surgeon (Y.X.) with >25 years of surgical experience, who also served as the department chief.
Rehabilitation Protocol
All patients adhered to a standardized postoperative rehabilitation protocol. During the first 48 hours after surgery, isometric muscle activation and passive range-of-motion exercises were initiated. From postoperative day 3 through week 3, patients were instructed to perform partial weightbearing activities with the goal of progressively restoring joint mobility and normal gait patterns. At week 4, unrestricted full weightbearing ambulation was introduced. Beginning at week 6, patients commenced full weightbearing strengthening exercises combined with dynamic balance training. Thereafter, a gradual return to daily activities and sports participation was recommended according to individual tolerance levels.
Postoperative Follow-up
All patients were followed up postoperatively according to the standard protocol, which included scheduled clinic visits, supplemented by telephone interviews after discharge. The telephone follow-up period ranged from 404 to 560 days, with a mean of 476 days. During follow-up, patients were asked to complete several outcome measures, including the Hip Outcome Score Activities of Daily Living and Sports Specific subscales (HOS-ADL and HOS-SS), the International Hip Outcome Tool–12 (iHOT-12), and the modified Harris Hip Score (mHHS). Additionally, patients were specifically questioned regarding any perineal injuries, lumbosacral discomfort, and whether they experienced any sensory disturbances in the operated lower limb, such as numbness, tingling, or hypoesthesia.
Statistical Analysis
IBM SPSS software (Version 27.0; IBM Corp) was used for statistical analysis. Continuous variables are expressed as mean ± SD. After assessing normality using the Shapiro-Wilk test, either the Mann-Whitney U test or the independent-samples t test was used to compare differences between the postless and control groups. Categorical variables were expressed as percentages, and the chi-square test was used for comparison between groups, with the Fisher exact test for expected frequencies of <5. All statistical tests were 2-tailed with a significance level set at P < .05. G*Power 3.1 (Universität Düsseldorf) was used to calculate the statistical power of the present study.
Results
General Information
The complete patient selection process is depicted in Figure 1, and the patients’ baseline characteristics are summarized in Table 1. Post hoc analyses demonstrated relatively adequate statistical power for most analyses supporting the core conclusions of this study. Additionally, we compared the operative duration between the 2 groups, and the results showed no significant difference (AppendixTable A1). Preoperative functional scores were also comparable between the 2 groups (Appendix Table A2).
Postoperative Outcome Score Differences Between Perineal Post and Postless Hip Arthroscopy
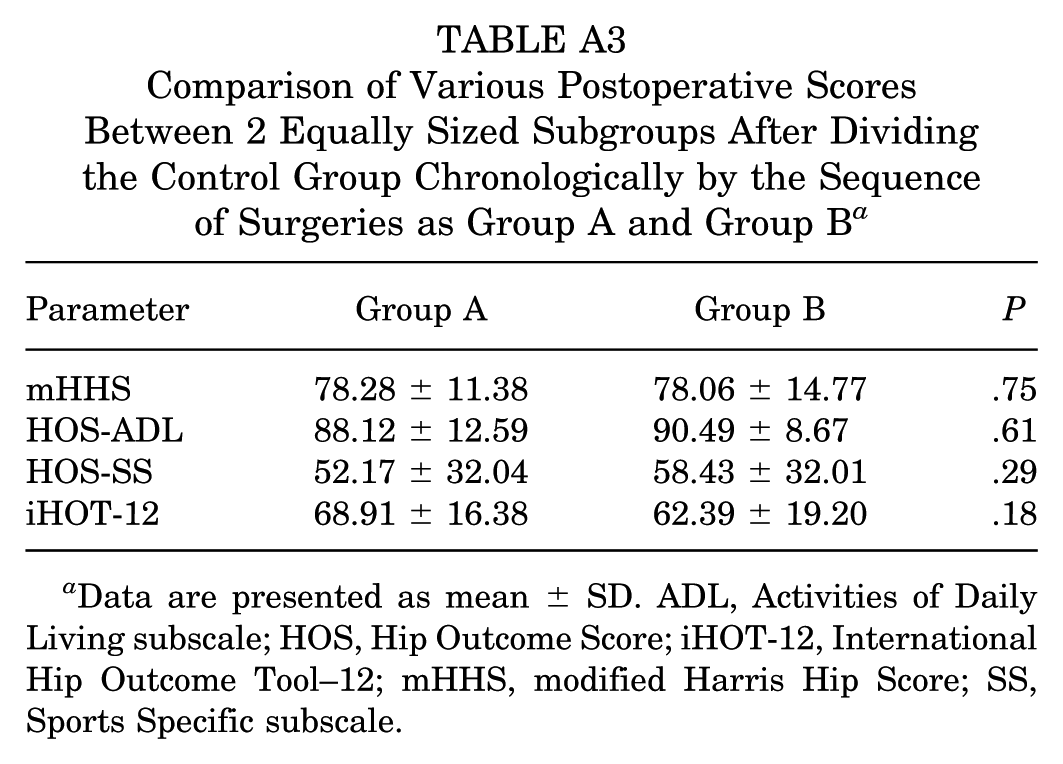
As presented in Table 2, this study compared 4 postoperative outcome measures between the postless and control groups. HOS ADL (88.91 ± 13.34 vs 89.30 ± 10.79) and mHHS (82.59 ± 9.46 vs 78.17 ± 13.08) scores did not differ significantly between the 2 groups (P > .05), whereas the postless group demonstrated significantly higher scores on iHOT-12 (80.57 ± 14.03 vs 65.65 ± 18.00; P < .001) and HOS-SS (76.81 ± 21.07 vs 66.78 ± 21.30; P = .009) compared with the control group. Furthermore, when the control group was divided into 2 equally sized subgroups based on the chronological order of surgery, no statistically significant differences were observed in any of the outcome scores between the 2 subgroups (AppendixTable A3).
Postoperative Patient-Reported Outcome Scores a
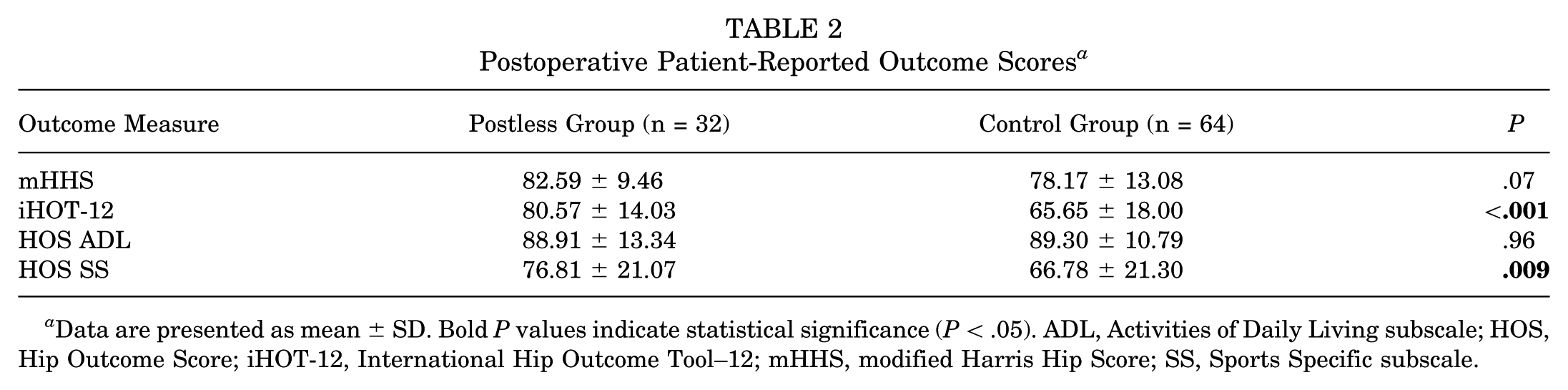
Data are presented as mean ± SD. Bold P values indicate statistical significance (P < .05). ADL, Activities of Daily Living subscale; HOS, Hip Outcome Score; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; SS, Sports Specific subscale.
Postoperative Complication Rate Differences Between Perineal Post and Postless Hip Arthroscopy
As shown in Table 3, all patients in both groups were successfully contacted by telephone follow-up. No significant difference was found in the overall rate of sensory nerve injuries between the 2 groups (31.3% vs 32.8%; P = .88). In both groups, lateral thigh numbness was the most frequently reported symptom. In the control group, 2 patients reported perineal numbness and another 2 reported ankle pain related to the traction boot, whereas no such symptoms were noted in the postless group. Of note, some patients in both groups reported symptoms at multiple sites. In the control group, 1 patient reported both ankle pain and lateral thigh numbness, and 3 patients reported anterolateral leg numbness. In the postless group, 1 patient reported numbness at both the surgical incision site and the sole of the foot.
Postoperative Complications After Hip Arthroscopy a
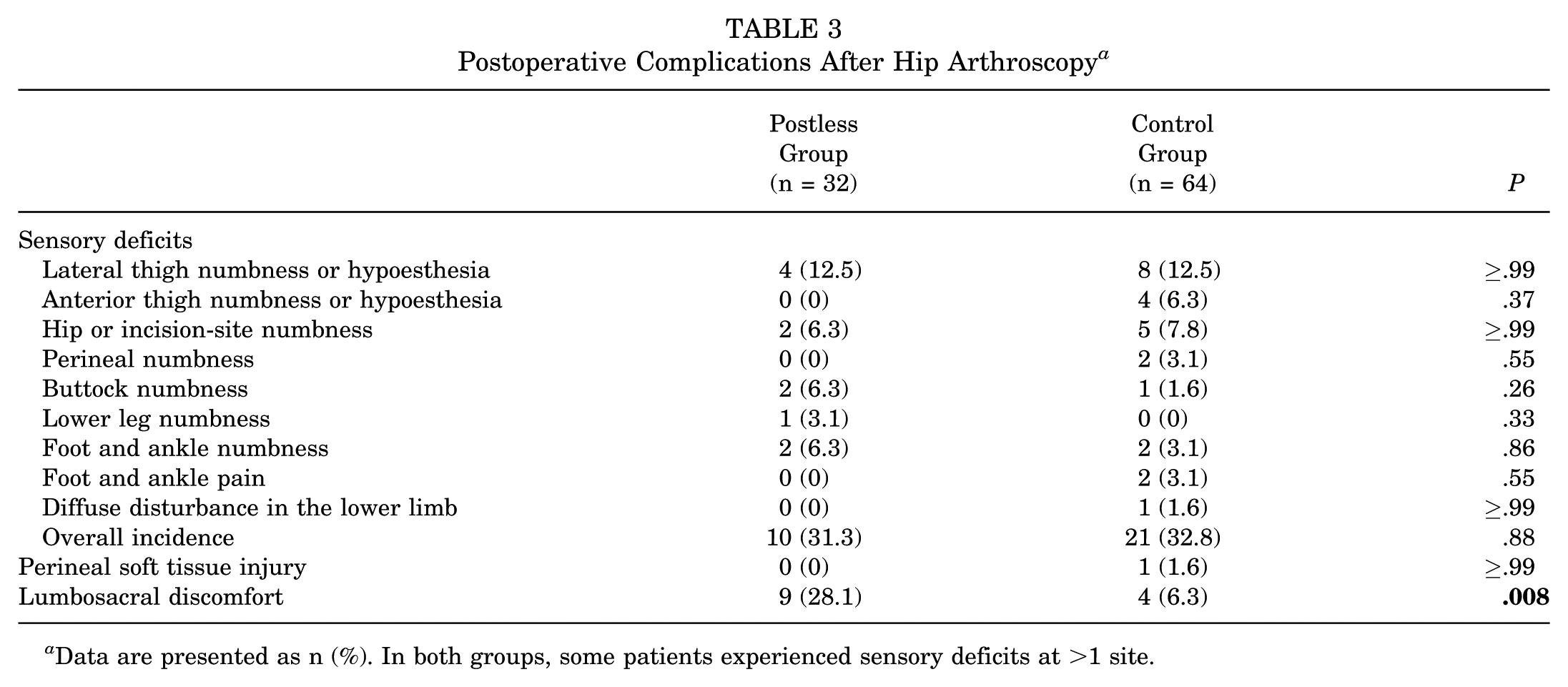
Data are presented as n (%). In both groups, some patients experienced sensory deficits at >1 site.
No perineal soft tissue injury, such as vulvar hematoma, vaginal tear, and skin necrosis of the labium or scrotum, was observed in the postless group, whereas 1 case (1.6%) was identified in the control group; however, the difference between groups was not statistically significant.
In addition, we evaluated the incidence of lumbosacral discomfort after surgery. No skin lesions were observed in either group, but all cases presented with postoperative lumbosacral pain that was provoked or exacerbated by activity, thereby affecting postoperative mobility. The incidence of this complication was significantly higher in the postless group than in the control group (28.1% vs 6.3%; P = .008). The majority of patients experienced relief or recovery within several months to 1 year with rest alone, without specific treatment. Nonetheless, at the time of follow-up, 3 cases in the postless group and 1 in the control group still reported activity-related pain.
Discussion
Our study suggests that postless hip arthroscopy is associated with better overall outcomes for patients. This technique may also be associated with fewer complications related to perineal post pressure, such as nerve damage and soft tissue injury in the perineal region. However, when compared to traction with perineal post, it does not appear to correspond to a reduction in the overall incidence of sensory nerve damage. Additionally, the postless traction may be linked to an increased incidence of lumbosacral discomfort postoperatively.
In this study, there was no significant difference in the overall sensory nerve damage rates between the postless and control groups. Thus, we believe that the technique without the perineal post may not be associated with a distinct advantage in terms of overall nerve damage reduction. This finding appears inconsistent with previous studies, where it was reported that the absence of the perineal post significantly reduced sensory nerve injury due to prolonged perineal post pressure. For example, Mei-Dan et al 14 reported no perineal post-related complications in 1000 cases of arthroscopy performed without the post. Similarly, a systematic review mentioned similar findings in two additional studies. 23 However, this does not negate previous research. The rate we reported was the overall complication rate, rather than specifically focusing on perineal post–related nerve injuries, a point also mentioned in the research by Parkes et al, 17 who reported no significant difference in overall numbness rates between the perineal post and postless groups (30.9% vs 44.6%). Notably, the postless group had a higher proportion of female patients, who were preferentially selected for this surgical approach because of their typically lower traction force requirements. However, as there was no significant difference in the sex ratio between the 2 groups and the degree of intraoperative hip joint traction was consistent, we believe this did not affect the final results. Compared with previous reports on the overall complication rate after hip arthroscopy (ranging from 1.4% to 74%),3,5,10,23 our study's reported rate is within this range but relatively high, which may reflect variations in surgical protocols, patient populations, and inclusion criteria across different centers.
The most common injury associated with prolonged pressure from the perineal post is to the pudendal nerve, leading to numbness in the perineal and inguinal areas, sensory disturbances, or even sexual dysfunction. The control group in our study reported 2 cases of perineal numbness, while the postless group reported none. Although this difference did not reach statistical significance (0% vs 3.1%; P = .55), it may be limited by the low incidence rate and sample size. In the study by Parkes et al, 17 patients with perineal post traction had a significantly higher incidence of inguinal area numbness compared to those without perineal post traction. Thus, the new technique may still correlate with an advantage in reducing complications related to perineal post pressure. However, in our study, the 2 groups had similar surgical methods and postoperative rehabilitation protocols, with the exception of the traction technique, and the overall incidence of complications was nearly identical. This may suggest that the perineal post technique at our center is relatively well-optimized, which may be reflected in a low incidence of post-specific complications.
Postoperative complications such as lateral femoral cutaneous nerve numbness and sciatic nerve paralysis are also commonly observed after hip arthroscopy. These may be related to perineal post pressure, but the proportion of injuries to the pudendal nerve is smaller. Alternatively, they may be associated with traction during surgery. Existing research has shown that traction with the perineal post can be accompanied by a decrease in somatosensory evoked potential amplitudes of the sciatic nerve, as well as reduced blood flow in the popliteal and femoral veins.13,20 However, with postless traction, there is no significant reduction in venous blood flow in the lower limb, and no marked neurological changes are observed, 22 highlighting the advantages of the postless technique. This is likely related to the absence of pressure applied to the perineum and reduced overall traction forces. Furthermore, complications may also be related to the surgical approach. For example, the lateral femoral cutaneous nerve's distribution is very close to the midanterior or anterior portal, 18 while the anterolateral and posterolateral portals may also pose a risk to the sciatic nerve. 2 Given the steep learning curve and complexity of hip arthroscopy, iatrogenic injuries may be significantly associated with overall nerve damage. In our study, both groups reported the highest incidence of numbness in the anterolateral thigh, which is likely due to injury of the lateral femoral cutaneous nerve. Numbness in the distal limbs, such as the calf and ankle, was also reported, possibly indicating sciatic nerve damage.
The control group also reported 2 cases of foot and ankle pain, likely related to prolonged traction and compression from the traction boots. The postless group reported none. This further suggests that perineal post traction may be associated with a greater degree of traction force than postless traction. This has been corroborated by multiple studies, 15 with increased traction forces being a contributing factor to postoperative injuries. However, the traction force required in our center for achieving joint gap opening during hip arthroscopy with post is relatively lower than that reported in other studies. 7 This may relate to the finding that postless traction was not associated with lower postoperative complication rates in our study.
Our study also found that the control group had a higher incidence of soft tissue injuries in the perineal region, with a rate of 1.6%, compared with 0% in the postless group. This finding is consistent with previous studies. However, the difference still did not reach statistical significance; similarly, this may reflect the low incidence rate and the small sample size. The relatively low absolute incidence of these injuries may be related to the wide variation in reported rates across studies, with Funke and Munzinger 6 reporting 1 case of vulvar hematoma among 19 patients, while Griffin and Villar 8 reported 1 vaginal tear in 640 patients 1 year after surgery. Recent reports have similarly described superficial skin tears in 53 patients. 11 For the postless technique, reports are more consistent, with no instances of perineal soft tissue injuries.11,14,23 This is easy to understand, as the absence of direct perineal pressure is associated with benefit for patients in this regard. However, the exact extent of this benefit is likely difficult to quantify and would require studies with larger sample sizes to confirm.
A noteworthy finding in our study was the significantly higher incidence of lumbosacral discomfort in the postless group compared with the control group. Although neither group reported skin-related symptoms, the postless group had more pronounced internal lumbosacral discomfort. This finding has not been widely addressed in previous studies. Since the Trendelenburg position typically involves a small tilt angle and lacks a perineal post to counteract lower limb traction force, the primary resistance, aside from the component of gravity along the traction table, relies on the friction between the patient's back and the operating table. Additionally, abdominal belts are used to prevent the patient from slipping, which increases the pressure between the patient and the table. These factors are associated with greater traction forces on the lumbosacral region. In contrast, this is not the case with the perineal post technique. Although patients may not experience discomfort immediately postsurgery, it tends to emerge during the rehabilitation phase, which may be negatively associated with overall patient outcomes.
We also compared postoperative outcomes using 4 standardized scoring scales. With the exception of the HOS ADL and mHHS, the control group scored significantly lower on the remaining scales, suggesting that the postless traction group experienced better overall postoperative outcomes. This is consistent with the trend reported in previous literature. 12 The HOS ADL and mHHS scales primarily focus on basic daily activities and low-impact exercises, which highlights that both surgical techniques are equally effective in addressing the core pathology without significant differences. The HOS SS scale, on the other hand, includes high-load activities, and the iHOT-12 assesses patient psychological responses to the disease and surgery. Thus, the significantly higher scores in these areas in the postless group may suggest that postless traction is not only associated with addressing the primary pathology but also with better postoperative recovery and enhanced quality of life. At the same time, this may also indicate that although lumbosacral discomfort and sensory nerve injury may, to some extent, be associated with compromised patient outcomes, patients tend to place greater emphasis on hip-related problems, which may exert a larger impact on their daily lives. Nevertheless, since the current scales primarily focus on hip joint function, they may not comprehensively capture other relevant issues. Therefore, more refined assessment tools are needed to better evaluate patients’ overall satisfaction with the surgery.
Limitations
This study has several limitations. First, the small sample size may limit the generalizability of the results and reduce statistical power. Additionally, the single-center recruitment may introduce sampling bias. The reliance on telephone follow-up may introduce recall bias. Last, the retrospective design inherently involves potential selection bias and unmeasured confounding factors. Future research should prioritize multicenter collaboration, precise physical examinations, and prospective study designs.
Conclusion
Postless hip arthroscopy is associated with superior patient-reported functional outcomes. However, it shows no reduction in the overall rate of sensory nerve injury and is linked to a significantly higher risk of postoperative lumbosacral discomfort.
Footnotes
Appendix
Comparison of Various Postoperative Scores Between 2 Equally Sized Subgroups After Dividing the Control Group Chronologically by the Sequence of Surgeries as Group A and Group B a
| Parameter | Group A | Group B | P |
|---|---|---|---|
| mHHS | 78.28 ± 11.38 | 78.06 ± 14.77 | .75 |
| HOS-ADL | 88.12 ± 12.59 | 90.49 ± 8.67 | .61 |
| HOS-SS | 52.17 ± 32.04 | 58.43 ± 32.01 | .29 |
| iHOT-12 | 68.91 ± 16.38 | 62.39 ± 19.20 | .18 |
Data are presented as mean ± SD. ADL, Activities of Daily Living subscale; HOS, Hip Outcome Score; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; SS, Sports Specific subscale.
Final revision submitted March 1, 2026; accepted March 6, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: The work was supported by a grant from the Beijing Municipal Natural Science Foundation (7244429).
Ethical approval for this study was obtained from the ethics committee of the Third Hospital of Peking University (M2019193; (2019)318-02).
Data Accessibility Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.