
Abstract
Background:
Acromioclavicular joint (ACJ) injuries are common; however, there is disagreement about the optimal treatment of Rockwood type ≥III ACJ dislocations.
Purpose:
To systematically review and meta-analyze the outcomes of all randomized controlled trials that compared the operative and nonoperative treatment of Rockwood type III to V ACJ dislocations.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
A systematic search of 4 databases was performed through September 15, 2024. Inclusion criteria included (1) adult patients, (2) acute Rockwood type III to V ACJ dislocations, (3) direct comparisons of operative to nonoperative management, (4) randomized controlled trial methodology, and (5) reporting of clinical outcomes. The primary outcome was the Constant score, and secondary outcomes consisted of other patient-reported outcome measure (PROM) scores, cosmesis, radiographic findings, range of motion, return to work/sport, complications, and unplanned surgery.
Results:
There were 5 comparative studies included in this review with a total of 367 patients: 193 patients underwent operative treatment (102 type III, 11 type IV, 40 type V, and 40 type III-V), and 174 underwent nonoperative treatment (84 type III, 13 type IV, 34 type V, and 43 type III-V). The mean age was 39.1 years for operative patients and 37.4 years for nonoperative patients. The follow-up ranged from 12 to 229.2 months. The mean Constant score at ≥2 years was 92.4 for operative patients and 90.1 for nonoperative patients, with meta-analysis demonstrating no significant differences at ≥2 years (95% CI, –0.03 to 0.43; P = .2). However, at shorter follow-up durations, individual studies found statistically significant differences favoring nonoperative management. One study found improved return to work rates with nonoperative management at 3 months, with no differences found at other time points. Meta-analysis found no significant differences in major complications between operative and nonoperative management (P = .84), although there were statistically significantly more minor complications with operative management (P < .0001). There were few reported outcomes for isolated type III, IV, or V injuries, but where reported, these outcomes followed the overall trend, with early PROM scores favoring nonoperative treatment and comparable outcomes between treatment groups at longer follow-up.
Conclusion:
There were comparable PROM scores at ≥1 year when comparing operative to nonoperative treatment in patients who sustained a Rockwood type III to V ACJ dislocation. However, early PROM scores favored nonoperative management. There were comparable satisfaction rates and comparable return to work/sport rates between groups. Therefore, the nonoperative management of type III to V ACJ dislocations resulted in comparable clinical outcomes compared to operative treatment.
Acromioclavicular joint (ACJ) injuries are commonly encountered in orthopaedic practice, representing approximately 9% to 12% of all shoulder injuries.10,18 These injuries typically occur after direct trauma to the lateral aspect of the shoulder and are classified using the Rockwood classification system, which categorizes injuries into 6 types based on the extent of ligamentous damage and clavicular displacement.8,18
Management strategies are based largely on injury severity and displacement. Rockwood types I and II, involving a partial ligamentous injury without significant displacement, are generally managed nonoperatively with early mobilization and structured rehabilitation. 10 However, there is more disagreement regarding the best treatment option for more displaced injuries, particularly types III through V.10,18 Previous studies have shown good outcomes for both the operative and nonoperative management of these injuries, and they are commonly grouped together in the literature, given the clinical challenges in differentiating between types III to V.3,4 Type VI injuries, although rare, are universally considered for surgical treatment because of inferior displacement of the clavicle beneath the coracoid process. 22
Several systematic reviews and meta-analyses have attempted to resolve this controversy. Giai Via et al 8 found no significant differences in functional outcomes such as the Constant score between operative and nonoperative treatment for type III injuries, although surgical patients exhibited superior radiographic alignment. Similarly, Bianco Prevot et al 1 reported no clinically meaningful differences in most patient-reported outcomes but noted higher complication rates after a surgical intervention. Okereke and Abdelfatah 18 reviewed a variety of surgical techniques, concluding that coracoclavicular reconstruction methods yield better outcomes and fewer complications than hardware-based fixation, although no gold-standard technique has yet emerged. Additionally, no studies have systematically reviewed the outcomes when combining type III to V injuries, even given the poor interrater reliability in classification.3,4
Given the persistent controversy surrounding type III to V ACJ injuries, and the recent publications of high-quality studies,2,25 there is a need for an updated synthesis of outcomes. The purpose of this review was to compare the outcomes of the operative and nonoperative management of Rockwood type III to V ACJ dislocations to further support evidence-based clinical decision-making.
Methods
This systematic review focused on comparing the outcomes of the operative and nonoperative management of patients with Rockwood type III to V ACJ dislocations. 20 This review was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 15 The study was registered in PROSPERO (CRD42024600112).
Search Strategy
A systematic search of 4 databases (MEDLINE, Embase, CINAHL, and Cochrane), combined with a manual search, was performed through September 15, 2024 by 2 reviewers (M.C. and A.C.) for literature related to ACJ dislocations. Gray literature and conference abstracts were searched manually. The complete search strategies can be found in Appendix 1. The inclusion criteria for this review were (1) patients who sustained a Rockwood type III to V ACJ dislocation, (2) patients who underwent either nonoperative or operative management of their injury, (3) comparative studies that directly compared operative to nonoperative management, (4) randomized controlled trials (RCTs), (5) reporting of clinical outcomes, (6) acute ACJ injuries, (7) adult patients (aged ≥18 years), and (8) published in English. Exclusion criteria included (1) chronic injuries and (2) follow-up <1 year. Rockwood types III to V were pooled, given the significant challenges that practitioners have differentiating the subtle differences between the types and what has been done previously in the literature.3,4
Study Screening
The title and abstract of all studies from the initial search after duplicate removal were assessed by 2 authors (M.C. and A.C.) independently. All disagreements between reviewers and studies with insufficient data were progressed to the full-text review stage. After a duplicate review of full text, a third author (D.L.L.) resolved any disagreements. A separate manual search of the literature was conducted. Any study that did not report the primary clinical outcomes after an ACJ dislocation (ie, secondary analyses of health status, etc) was excluded. The level of agreement between reviewers was calculated using the kappa coefficient. 11 The risk of bias was calculated using the Risk of Bias 2 tool. 24
Data Abstraction
The data were abstracted by 2 reviewers (M.C. and A.C.) and inputted into predetermined tables using Google Sheets (Alphabet). The data were all reviewed in duplicate by a third author (D.L.L.). The data abstracted included number of patients, patient characteristics (sex, age, body mass index, etc), study characteristics (journal, authors, publication year, study design, level of evidence, etc), follow-up duration, patient-reported outcomes, objective outcomes (range of motion, radiographic findings, etc), reoperation rates, and adverse events/complications. The level of evidence was determined based on published levels or, if not reported, the American Academy of Orthopaedic Surgeons guidelines. 28 For studies with missing patient data, as well as missing mean Constant scores, an attempt to contact the authors was made.
Primary Outcome
The primary outcome of this study was the Constant score because in the included studies, it was the most common patient-reported outcome measure (PROM). 6 Additionally, within the ACJ literature, the Constant score is the most utilized outcome measure. 19 Previous studies have demonstrated that the Constant score is acceptable for use in acromioclavicular injuries and general shoulder abnormalities, with low interrater and intrarater variability.5,19,29 The Constant score assesses shoulder function after an injury using a combination of objective and subjective measurements. 30 The Constant score is reported on a scale from 0 to 100, with 0 being the worst possible score and 100 indicating the best possible outcome (high level of function).6,30 A previous study demonstrated that the minimal clinically important difference for the Constant score when assessing outcomes after ACJ surgery was 16.6. 23
Secondary Outcomes
The secondary outcomes consisted of PROM scores, cosmesis, radiographic findings, range of motion, return to work/sport, complications, and unplanned surgery. Secondary PROMs included the Acromioclavicular Joint Instability (ACJI) score, American Shoulder and Elbow Surgeons (ASES) score, Disabilities of the Arm, Shoulder and Hand (DASH), Larsen score, Oxford Shoulder Score (OSS), patient satisfaction, Short Form–12 (SF-12) mental component summary (MCS) and physical component summary (PCS), Subjective Shoulder Value (SSV), Simple Shoulder Test (SST), Taft score, Tegner score, University of California, Los Angeles (UCLA) score, and visual analog scale (VAS) for pain. Major complications were any complications that were reported as major by the authors or associated with significant clinical morbidity/necessitating a reoperation. Major complications consisted of persistent discomfort (requiring surgery), cosmetic concerns (requiring surgery), hardware loosening, acromial erosion, redislocations, clavicle fractures, stiff/frozen shoulder, deep infections, implant irritation (requiring surgery), or soft tissue compromise. Minor complications included any complications reported as minor by the authors or leading to mild/no morbidity and comprised superficial infections, minor hardware issues, peri-incisional numbness, and heterotopic ossification without functional impact. Unplanned surgery was defined as any operative procedure that was unexpected (ie, excluding planned hook plate removal) and included patients initially allocated to the nonoperative group who underwent surgery for pain and/or cosmesis. ACJ degenerative changes/osteoarthritis were reported as published.
Statistical Analysis
Meta-analyses were conducted separately for continuous and dichotomous outcomes. For continuous outcomes, mean differences were pooled when studies used the Constant score. When outcomes were assessed using conceptually similar but distinct instruments, specifically the DASH and the quick version of the DASH (QuickDASH), standardized mean differences were calculated to allow for appropriate synthesis. For dichotomous outcomes, including major and minor complication rates, risk ratios (RRs) with 95% confidence intervals (CIs) were calculated. Meta-analyses were conducted using a fixed-effects model when heterogeneity was low or absent (I2 = 0%), and a random-effects model (DerSimonian and Laird method) was applied when heterogeneity exceeded conventional thresholds (I2≥ 50%). Statistical heterogeneity was assessed using the chi-square test (with P < .10 considered indicative of significant heterogeneity), the I2 statistic, and the tau-squared value (τ2) (when appropriate). Thresholds for interpreting I2 followed Cochrane guidance: 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. Funnel plots were not generated because of the small number of included studies (<10), which limits the interpretability of such plots. Meta-analyses and forest plots were generated in R (Version 4.5.2). Statistical significance was set at a 2-sided P value <.05. In studies with patient crossover, patient-reported outcomes were determined based on as-treated analysis (as reported in the studies); however, complications were determined based on intention-to-treat analysis.
Weighted means were calculated for patient and outcome variables. Pooled standard deviations were calculated when standard deviations were available. Alternatively, standard errors or ranges were used to impute standard deviations when available. 27 To compare outcomes between operative and nonoperative groups across studies for the Constant score, the Welch 2-sample t test using group-level summary statistics (means, standard deviations, and sample sizes) was utilized. Analyses were conducted in R (Version 4.5.2).
Otherwise, outcomes were presented in a narrative summary fashion. Because of small numbers of patients or outcomes, poor interrater reliability, 4 and pooling of patients in studies of type III to V ACJ dislocations, no subgroup analysis was performed based on injury type.
Results
There were 2691 studies identified from the initial search, with 1774 studies remaining after duplicate removal. After a review of the title and abstract, 25 studies remained that progressed to a full-text review. Ultimately, 5 studies2,3,9,16,25 remained after the application of inclusion and exclusion criteria and were included in this study (Figure 1). One study 14 presented an analysis of general health status and was excluded as a previously included study reported primary clinical outcomes. Overall, 4 studies were level 1 evidence, and 1 study was level 2 evidence (Appendix 2). Additionally, 2 studies had a low risk of bias, and 3 studies had a moderate risk of bias (Appendix 3).
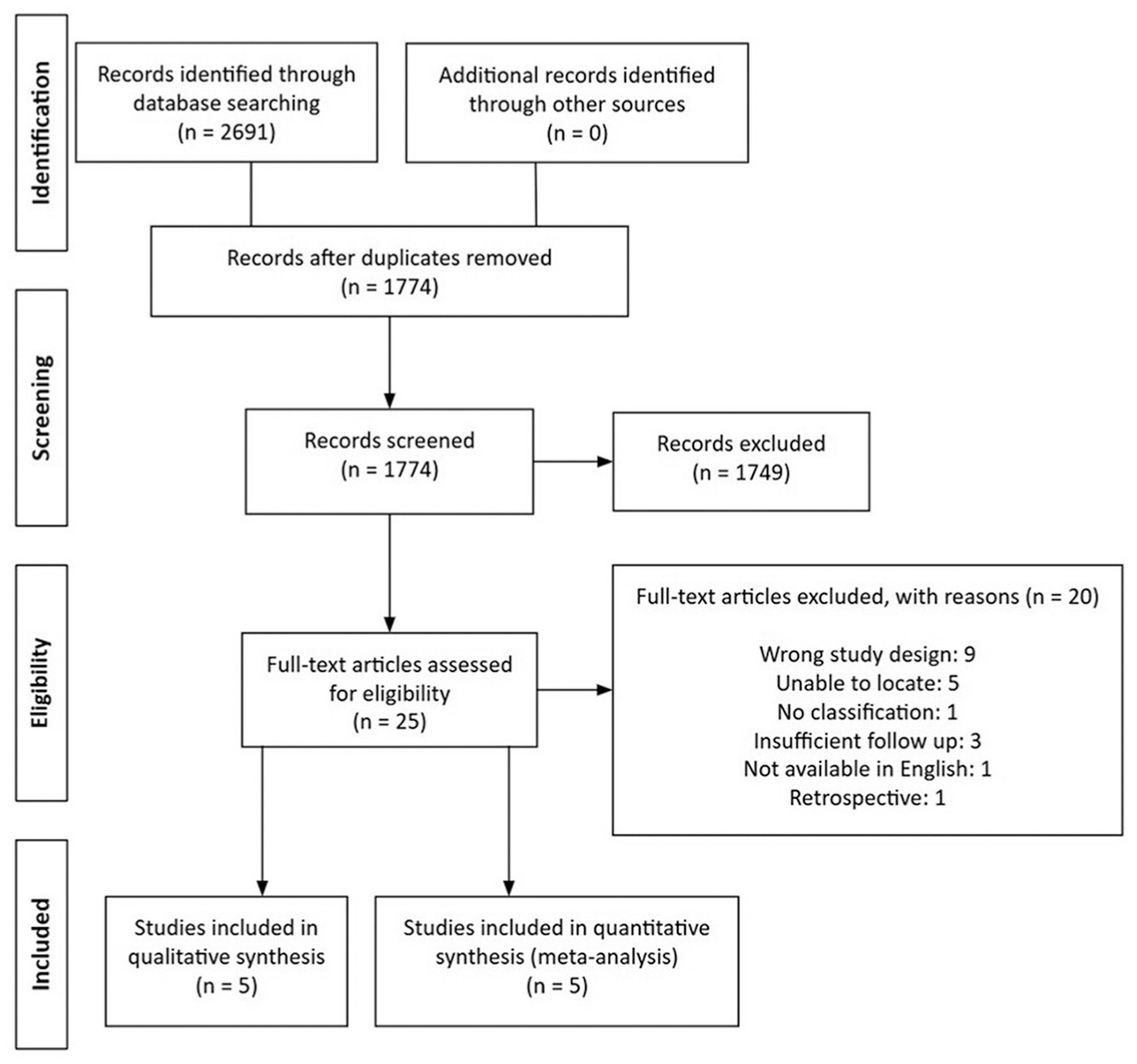
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram.
Patient Characteristics
A total of 367 patients were included in this study, with 193 patients undergoing operative management and 174 patients undergoing nonoperative management (Table 1). Overall, 2 studies2,9 included patients with type III and V injuries, 1 study 3 included patients with type III to V injuries, 1 study 16 included patients with type III to IV injuries, and 1 study 25 included patients with only type III injuries. In the operative group, 102 patients were reported as having type III, 11 type IV, 40 type V, and 40 as ranging from type III to V, whereas in the nonoperative group, 84 were reported as having type III, 13 type IV, 34 type V, and 43 as ranging from type III to V. The mean age was 39.1 and 37.4 years for operative and nonoperative patients, respectively. Most patients were male, with 10.9% and 6.3% female patients in the operative and nonoperative groups, respectively. There were no significant differences in patient characteristics between groups. The follow-up duration ranged from 12 to 224.4 months for operative patients and from 12 to 229.2 months for nonoperative patients. The majority of studies2,3,25 had a minimum follow-up duration of 24 months.
Patient Characteristics
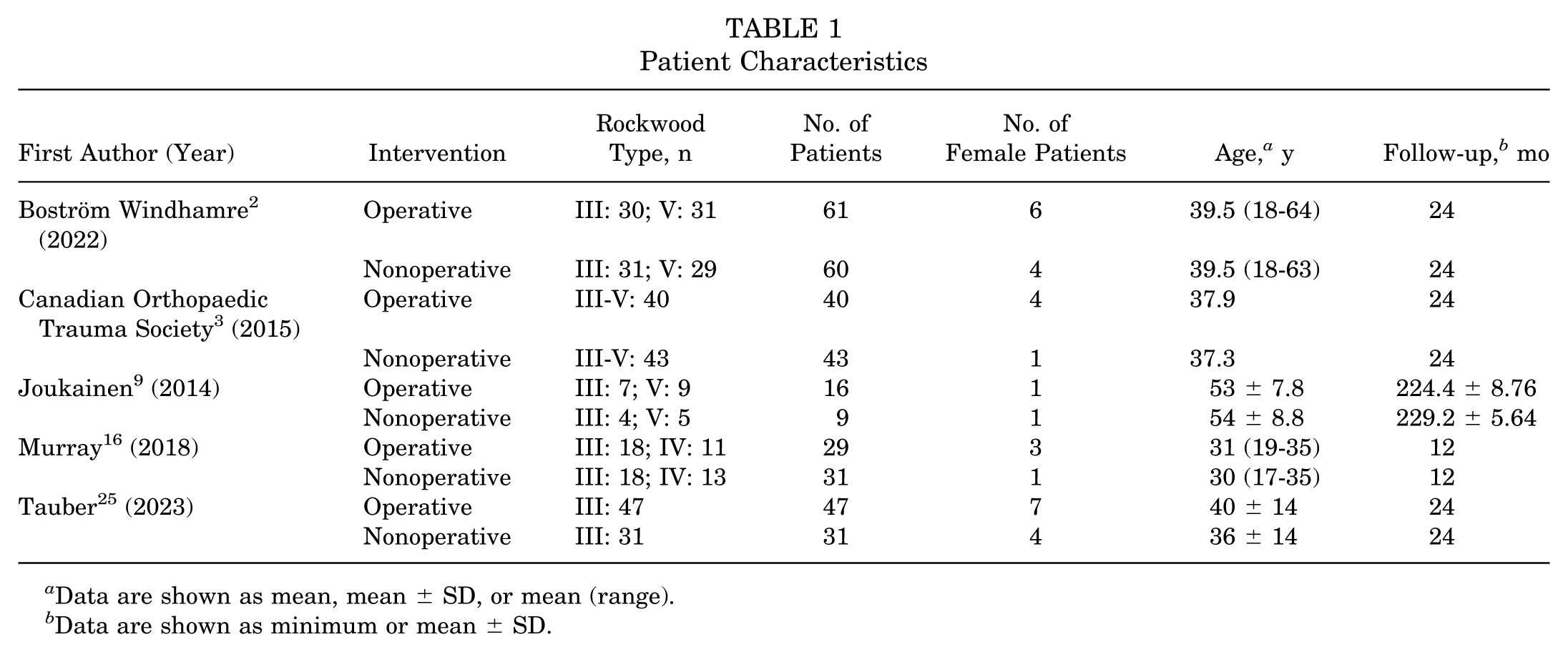
Data are shown as mean, mean ± SD, or mean (range).
Data are shown as minimum or mean ± SD.
Operative treatment varied between studies: 2 studies2,3 used a hook plate, 1 study 9 used Kirschner wires across the ACJ, 1 study 16 used a suspension device to secure the clavicle to the coracoid, and 1 study 25 used a combination of hook plates and suspension devices (Appendix 2). Nonoperative management consisted of the use of a sling in 4 studies2,3,16,25 and a Kenny Howard splint in 1 study, 9 and immobilization in a sling lasted from 10 days to 4 weeks (Appendix 4).
Constant Score
The Constant score was reported at ≥2 years in 4 studies.2,3,9,25 The weighted mean Constant score for operative treatment was 92.4 ± 0.5 compared to 90.1 ± 0.8 for nonoperative treatment. Meta-analysis demonstrated no significant differences at ≥2 years’ follow-up (95% CI, –0.03 to 0.43; P = .2) (Figure 2).

Forest plot of Constant score at ≥2 years.
Nonoperative treatment was associated with a significantly higher Constant score at 6 weeks compared to operative treatment in one study. 3 Similarly, nonoperative treatment was associated with a significantly higher Constant score at 3 months in 2 studies2,3 compared to operative treatment (Table 2). At 3 months, the weighted mean Constant score was 63.9 ± 1.8 for operative management and 83.4 ± 1.3 for nonoperative management (P < .0001) and was greater than the previously reported minimal clinically important difference in the literature of 16.6. 23
Constant Scores a
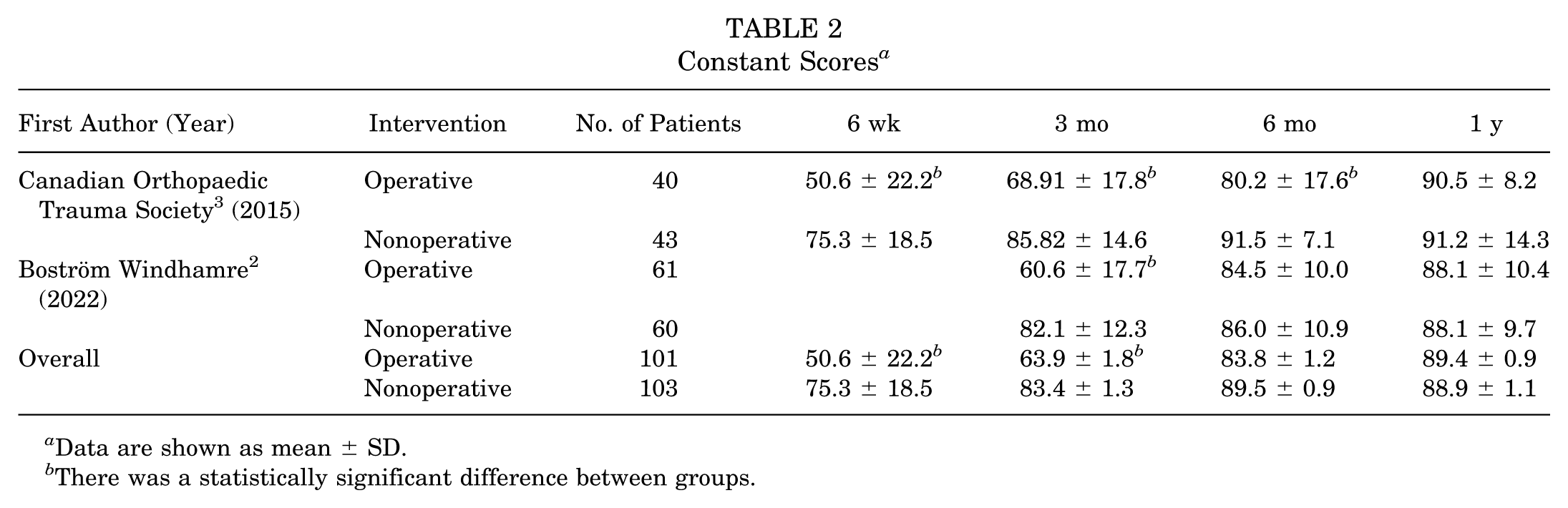
Data are shown as mean ± SD.
There was a statistically significant difference between groups.
At 6 months, 1 study 3 found a statistically significant difference in the Constant score, favoring nonoperative management, and 1 study 2 did not find a difference. The weighted mean Constant score at 6 months was 83.8 ± 1.2 for operative management and 89.5 ± 0.9 for nonoperative management (P = .0011). At 1 year, 2 studies2,3 reported no differences in the Constant score between groups, with a weighted mean of 89.4 ± 0.9 and 88.9 ± 1.1 for operative and nonoperative management, respectively (P = .75).
One study 2 reported Constant scores for type III and V injuries, and another study 25 reported only type III injuries. For isolated type III injuries, at 3-month follow-up for operative compared to nonoperative treatment, there was a significant difference favoring nonoperative treatment in one study 2 (57.1 vs 80.2, respectively) and no difference in another study. 25 There were no differences in the Constant score between operative and nonoperative treatment at 6 or 12 months in either study. For isolated type V injuries, one study 2 compared operative and nonoperative treatment and found a statistically significant difference favoring nonoperative treatment at 3 months (64.0 vs 84.1, respectively) but no differences at 6 or 12 months. Similarly, there were no differences between the operative treatment of type III and V injuries and the nonoperative treatment of type III and V injuries in one study 2 at 3, 6, or 12 months.
DASH/QuickDASH Score
There were 2 studies3,16 that reported the DASH score at 1 year, and 1 study 2 reported the QuickDASH score, with all studies reporting no differences between treatment groups (Appendix 5). Meta-analysis for the DASH/QuickDASH score at 1 year did not favor either treatment group, with a mean difference of 0.00 (95% CI, –0.24 to 0.24; P > .99) (Figure 3).

Forest plot of Disabilities of the Arm, Shoulder and Hand (DASH) or quick version of the DASH (QuickDASH) score at 1 year.
The weighted mean DASH/QuickDASH score at 1 year was 6.6 ± 0.6 and 5.9 ± 0.8 for operative and nonoperative management, respectively. At ≥2 years, the weighted mean DASH/QuickDASH score was 5.0 ± 0.7 and 7.2 ± 1.2 for operative and nonoperative management, respectively. One study 3 found a statistically significant difference (P < .01), favoring nonoperative management, in the DASH score at 6 weeks. Another study 2 found an improvement in the QuickDASH score, favoring nonoperative patients compared to operative patients, at 3 months’ follow-up for both type III and V injuries but no differences at other time points and no differences between operatively treated type III and V injuries or nonoperatively treated type III and V injuries.
Other PROM Scores
A total of 4 studies2,9,16,25 reported on additional PROMs. There were no statistically significant differences reported in ACJI, ASES, Larsen, OSS, patient satisfaction, SF-12 MCS/PCS, SSV, SST, Taft, Tegner, UCLA, or VAS pain scores at final follow-up in any of the studies (Appendix 6).
For isolated type III injuries, one study 25 found no difference in ACJI, ASES, Taft, or VAS pain scores between operative and nonoperative treatment. One other study 9 found no differences in UCLA, Larsen, or SST scores between operative and nonoperative treatment. Another study 2 found an improvement in the SSV score for nonoperative patients at 3 months’ follow-up but no differences at other time points and no differences in the percentage of patients who rated their shoulder as excellent at long-term follow-up.
For isolated type V injuries, one study 9 found no differences in UCLA, Larsen, or SST scores between operative and nonoperative patients. Another study 2 found an improvement in the SSV score for nonoperative patients at 3 months’ follow-up but no differences at other time points and no differences in the percentage of patients who rated their shoulder as excellent at long-term follow-up.
When comparing type III to type V injuries, one study 9 found no differences in UCLA, Larsen, or SST scores between operatively and nonoperatively treated patients. Another study 2 reported no differences in the SSV score or percentage of patients who rated their shoulder as excellent at long-term follow-up.
Cosmesis
There were 4 studies2,3,16,25 that reported on cosmesis. In one study, 2 the authors found no differences in cosmesis of the shoulder between groups, with 67% and 60% of patients satisfied with the appearance of their shoulder after operative and nonoperative treatment, respectively. Additionally, they asked patients to rate their satisfaction with the cosmetic appearance of their shoulder from 0 to 10 (10 indicating the best cosmesis) and found a mean score of 7.8 and 8.0 for operative and nonoperative management, respectively. Similarly, another study 3 found no differences (P = .234) between groups at 2-year follow-up, with 96% of patients not dissatisfied with their shoulder's appearance after operative management and 78% of patients not dissatisfied with their appearance after nonoperative management. One other study 16 noted that 1 patient initially allocated to the nonoperative group crossed over specifically because of concerns around cosmesis. Additionally, one study 25 reported that there were 8 early failures with crossover from the nonoperative group to the operative group because of issues with either pain or cosmesis.
For isolated type III injuries, one study 25 found no difference in subjective cosmetic outcomes. In another study, 2 the authors found that 55% of patients in the nonoperative group were satisfied with their shoulder's appearance compared to 68%, which was not significant. Similarly, the mean score for cosmetic appearance was 7.8 for nonoperative treatment compared to 8.1 for operative treatment, which was not significant. Similarly, this study 2 found no differences for isolated type V injuries treated operatively or nonoperatively.
Radiographic Findings
There were 4 studies2,9,16,25 that reported follow-up radiographic findings. Because of concerns regarding measurement methodology, distances were not pooled. All studies found radiographic outcomes (distance from acromion to clavicle, ACJ width, distance from coronoid to clavicle) that were statistically significantly greater for those with nonoperative management. For isolated type III injuries, 25 this was especially demonstrated, with operative patients having significantly decreased diastasis at all follow-up time points. In another study, 9 at long-term follow-up, there was no significant difference in ACJ width for type III injuries treated operatively or nonoperatively (4.8 vs 8.1, respectively); however, there was a statistically significant decrease in ACJ width for type V injuries treated operatively compared to nonoperatively (mean, 2.4 vs 8.5 mm, respectively; P = .007).
Range of Motion
One study 25 assessed range of motion in patients with isolated type III injuries at 6 weeks and found statistically significant differences in flexion, abduction, internal rotation, and external rotation, favoring those with nonoperative management. Additionally, another study 9 reported outcomes for type III and V injuries, not finding any statistically significant differences in active flexion or active abduction at long-term follow-up between operative and nonoperative treatment or between type III and type V injuries, regardless of the intervention.
Return to Work/Sport
One study 3 reported on return to work and found a statistically significant difference in improved return to work rates with nonoperative management compared to operative management (76% vs 43%, respectively; P = .004) at 3 months; however, at 6 weeks, 6 months, 1 year, and 2 years, there were no differences. Another study 16 reported on return to sport, finding comparable rates within 1 year: 73% and 85% for operative and nonoperative patients, respectively. Similarly, there were comparable rates of return to preinjury sporting levels between groups: 73% and 78% for operative and nonoperative treatment, respectively. However, it was noted at 6 weeks that there was a greater proportion of nonoperative patients (33%) who returned to sport compared to operative patients (15%). 16
Complications
All studies reported major complications (Appendix 7). Meta-analysis demonstrated a slightly increased risk of major complications with operative treatment; however, the difference was not statistically significant (RR, 1.13 [95% CI, 0.34-3.80]; P = .84) (Figure 4). The most common complication for operative management was hardware issues (n = 10), and the most common major complication for nonoperative management was persistent pain or issues with cosmesis requiring surgery (n = 15).

Forest plot of major complications.
Minor complications were reported in 3 studies.3,9,25 Meta-analysis showed a significantly increased risk of minor complications associated with operative treatment, favoring nonoperative management (RR, 5.43 [95% CI, 2.39-12.31]; P < .0001) (Appendix 8). The most common minor complication in both groups was heterotopic ossification without functional impairment (28 patients in operative group and 5 patients in nonoperative group).
ACJ degenerative changes/osteoarthritis were reported in 4 studies3,9,16,25 (Appendix 9). The rate of ACJ degenerative changes/osteoarthritis ranged from 0.0% to 68.8% for operative patients and from 2.3% to 100.0% for nonoperative patients. Of note, one study 9 had a significantly longer follow-up period (>18 vs ≤2 years, respectively) and had a significantly higher rate of ACJ changes (68.8% for operative patients and 100.0% for nonoperative patients) compared to the next highest studies,16,25 with 17% for operative patients and 6.9% for nonoperative patients at 2-year follow-up.
Unplanned Surgery
A total of 14 patients (7.3%) had unplanned surgery after being allocated to the operative group (n = 191) (Appendix 10). This was comparable to the rate of unplanned surgery for those allocated to the nonoperative group (8.9% [16/180]).
Discussion
The primary findings of this review were that at ≥1-year follow-up, there were no differences in the Constant score between the operative and nonoperative management of type III to V ACJ dislocations; satisfaction rates were comparable between groups; and most parameters, aside from radiographic displacement, were also similar. Therefore, the nonoperative management of type III to V ACJ dislocations resulted in comparable outcomes to those of operative management. Additionally, nonoperative management favored earlier patient-reported outcomes and earlier return to work.
Given the findings of this review, it is a reasonable approach to initially treat patients with type III to V injuries, without absolute indications for surgery, nonoperatively. There were 4 studies2,3,16,25 that treated patients with a simple sling for 10 days to 4 weeks, followed by shoulder rehabilitation. With this approach, one would only perform surgery on those with persistent pain after a trial of nonoperative management or those who have concerns with cosmesis, trading a bump for a scar. This review found comparable rates of satisfaction with the appearance of the shoulder between the nonoperative and operative groups, with one study 2 demonstrating 60% of patients satisfied with their shoulder's appearance compared to 67%, respectively, and another study 3 demonstrating 78% not dissatisfied with their shoulder's appearance compared to 96%, respectively. Additionally, one study 3 found improved Constant scores from 6 weeks to 6 months along with improved DASH scores from 6 weeks to 3 months with nonoperative treatment. However, both of these scores were not different between treatment groups at 1-year follow-up.2,3,16 Furthermore, there were comparable rates of return to sport and work at 1-year follow-up, with earlier return to sport favoring nonoperative management compared to operative management (33% vs 15%, respectively). 16 The unplanned surgery rates were also comparable, with the majority of patients crossing over to undergo an index procedure when treated nonoperatively compared to those for a surgical complication (most commonly hardware issues) when treated operatively. As such, treating those with a type III to V ACJ dislocation initially nonoperatively is a reasonable approach for most patients.
Although clinical outcomes were comparable between operatively and nonoperatively treated patients, there are some concerns with nonoperative treatment that need to be discussed with the patient. As expected, patients treated nonoperatively had greater displacement between the clavicle and the acromion or the coracoid at follow-up.3,9,16,25 The ACJ does not self-reduce with time and leads to a persistent bump that does not typically improve. However, this study has demonstrated that clinical outcomes are not reliant on a reduced ACJ, with early patient-reported outcomes favoring nonoperative management and long-term outcomes comparable between operative and nonoperative treatment (even with persistently displaced ACJs). Outcomes are comparable, even though this persistent displacement may lead to more ACJ degenerative changes/osteoarthritis. At shorter term follow-up (1-2 years), rates of degeneration were comparable across groups3,16,25; however, at long-term follow-up (>18 years), degeneration was observed in 100.0% of nonoperatively treated patients compared to 68.8% of those treated operatively. 9 Notably, only 9 of the 21 nonoperatively treated patients (42.9%) had long-term follow-up compared to 84.2% of operatively treated patients. 9 As such, there may be an increase in degenerative changes with persistent ACJ displacement, but the evidence is very limited. Lastly, patients who cross over from initially being treated nonoperatively to operatively may have worse outcomes. Murray et al 16 compared nonoperatively treated patients to a subgroup of patients that crossed over to operative management (suspension device) and found statistically inferior DASH and OSS scores for those who crossed over. Therefore, a thorough discussion should take place with the patient, and surgery should be considered earlier for those with significant cosmetic concerns.
When considering operative treatment, there are many options for surgical management including hook plates, suspension devices, suturing, ACJ pins, coracoclavicular screw insertion (Bosworth method), and coracoclavicular ligament reconstruction.7,9,26 In this study, 3 primary techniques were included: ACJ pins, hook plates, and coracoclavicular suspension devices. When considering stabilizing across the ACJ, both Kirschner wires and hook plates are available options, with hook plates becoming more popular because of complications seen with ACJ pins, particularly with pin migration.7,13 The use of hook plates remains a reasonable option with reportedly good clinical outcomes.3,21 However, there are drawbacks, including the need for second surgery to remove the plate, the risk of migration, loss of reduction, and clavicle fractures.12,17 Coracoclavicular suspension devices are also frequently used and lead to good clinical outcomes and only require one operative procedure. Nevertheless, they are associated with complications such as suture breakage, clavicle fractures, hardware irritation, and loss of reduction.7,25 Interestingly, one study 25 used both suspension devices and hook plates; for some patients, the authors used 1 suspension device, and in others, they used 2 devices. They had to stop using only one suspension device during the study because of concerns with early loss of reduction within 6 weeks of surgery. 25 Other common options that were not compared in this review include coracoclavicular ligament reconstruction and acromioclavicular ligament reconstruction, and future RCTs comparing these options to nonoperative management may be warranted. 7
A major strength of this review is the inclusion of only RCTs and ones with a low to moderate risk of bias. All included studies directly compared the operative and nonoperative management of ACJ dislocations. There was some variability in the exact included types between studies, with some studies only assessing type III injuries, 25 others assessing all type III to V injuries, 3 and further studies assessing only type III and IV injuries 16 or type III and V injuries.2,9 This highlights how challenging clinically it can be to exactly differentiate between types III to V, and because of poor intraobserver reliability, 4 it is clinically relevant to include all 3 types together when assessing outcomes, as has been done previously in influential studies. 3 By pooling types III to V, this increases the number of RCTs included in this study; however, by limiting it to RCTs, there are smaller total sample sizes. Yet, there is convincing evidence that the nonoperative management of type III to V ACJ dislocations leads to comparable outcomes compared to hook plates, ACJ pins, or coracoclavicular suspension devices.
Limitations
There are multiple limitations to this review. Although we assessed the management of types III to V, not all studies reported the outcomes of all 3 types. Because of very small numbers of reported outcomes for isolated type III, IV, and V injuries, there was no statistical analysis of these outcomes, which instead were reported in a narrative fashion where possible, with limited return to work/sport and complication rates for isolated injuries. However, combining all 3 types is an established approach, as previous studies have shown poor interrater reliability in differentiating between the Rockwood types, 4 and prior studies have combined the outcomes of all 3 types. 3 In addition, multiple operative treatment methods were included (ie, hook plates, ACJ pins, and coracoclavicular suspension devices), which could lead to differing patient outcomes and complication rates. However, one included study 25 that used both hook plates and coracoclavicular suspension devices compared the clinical outcomes based on surgical technique and found no difference. There were also no studies that focused primarily on coracoclavicular ligament reconstruction, and further comparative studies between this treatment option and nonoperative treatment should be considered. Furthermore, when calculating major complication rates, crossing over from nonoperative to operative treatment was considered a major complication, as it led to unplanned surgery (following intention-to-treat analysis). This may overestimate the risk of major complications for patients initially treated nonoperatively who continued to undergo nonoperative management. Nevertheless, often, patients crossed over because of persistent pain or cosmetic issues, which can be considered a major complication. There were also differences in what was considered a major or minor complication between authors, and judgment had to be used when classifying.
Conclusion
There were comparable PROM scores at ≥1 year when comparing operative to nonoperative treatment in patients who sustained a Rockwood type III to V ACJ dislocation. However, early PROM scores favored nonoperative management. There were comparable satisfaction rates and comparable return to work/sport rates between groups. Therefore, the nonoperative management of type III to V ACJ dislocations resulted in comparable clinical outcomes compared to operative treatment.
Footnotes
Final revision submitted January 9, 2026; accepted February 19, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for the present study.