
Abstract
Background:
Anterior shoulder instability with glenoid bone loss (GBL) poses a clinical challenge, especially for athletes aiming to return to sports (RTS). While arthroscopic Bankart repair (ABR) has demonstrated varying strengths, arthroscopic anatomic glenoid reconstruction (AAGR) has emerged as a promising alternative to address GBL.
Purpose/Hypothesis:
The purpose of this study was to compare the rate and time of RTS between AAGR and ABR in patients with anterior shoulder instability. A subobjective was to compare recurrent instability rates between the groups. It was hypothesized that AAGR would result in higher RTS rates and lower redislocation rates compared to ABR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with anterior shoulder instability and GBL treated with either AAGR or ABR between 2016 and 2021 were retrospectively analyzed. The inclusion criteria required preoperative participation in recreational or competitive sports. Patient characteristics, sports participation levels, RTS outcomes (based on patient survey), reasons for not returning to sports, and postoperative recurrence and complications were collected. Statistical analyses involved chi-square tests for categorical variables and t tests or Mann-Whitney U tests for continuous variables, with significance set at P < .05.
Results:
A total of 84 patients were included in the analysis (AAGR, n = 44; ABR, n = 40). The AAGR group had 21% GBL while the ABR group had 10% GBL (P < .001). Despite this difference, RTS rates were significantly higher in the AAGR group (75%) compared with the ABR group (50%) (P = .038). The redislocation rate was significantly lower in the AAGR group (2.3%) compared with the ABR group (17.5%) (P = .025).
Conclusion:
In patients with anterior shoulder instability, our study showed that anterior AAGR demonstrates superior patient-reported RTS rates and lower redislocation rates than ABR, with comparable recovery timelines despite the AAGR group having higher GBL. These findings suggest that bone block procedures may achieve higher RTS rates than ABR alone. This study provides valuable guidance for clinicians advising athletes on surgical options by establishing appropriate RTS expectations and demonstrating that AAGR provides suitable RTS in the presence of GBL.
Keywords
Anterior instability of the glenohumeral joint is a common issue, particularly among young male athletes participating in overhead sports. 29 For these individuals, shoulder instability can substantially impede a return to preinjury performance, underscoring the necessity for effective and timely surgical intervention. Arthroscopic Bankart repair (ABR), introduced in the 1990s, offered a less invasive alternative to traditional open procedures and quickly became a favored technique for addressing glenohumeral instability. 28 However, recurrence rates after ABR remain problematic, ranging from 15% to 43%, especially in patients with notable glenoid bone loss (GBL) and/or humeral head bone loss (ie, Hill-Sachs lesions).2,33 Specifically, ABR has been shown to be inferior to the Latarjet procedure at long-term follow-up. 42 These shortcomings have motivated investigations into alternative procedures for shoulder stabilization. These procedures include soft tissue approaches, such as Bankart repair with Remplissage, to address Hill-Sachs lesions, and bony procedures, such as the Latarjet procedure and arthroscopic anatomic glenoid reconstruction (AAGR) with distal tibia allograft (DTA).35,41
The AAGR procedure with DTA has been shown to provide a safety profile comparable to ABR for complications, such as subluxation, infection, and neurovascular injury, while demonstrating improved success in preventing recurrence. 38 It is especially beneficial for younger athletes and individuals with multiple prior instability episodes. 38 Moreover, AAGR minimizes donor-site morbidity, has a more favorable learning curve for surgeons than the Latarjet procedure,9,25 and has a reported recurrence rate3,40 under 2%. Complication rates for AAGR are relatively low, with previous reports of 14% of patients experiencing >50% resorption and 100% of patients experiencing graft union. 37
A recent systematic review of athletes undergoing surgical treatment for anterior instability found that 18% did not return to sport (RTS). 39 Notably, these decisions were predominantly attributed to non-shoulder-related factors, such as fear of reinjury. 39 Across surgical procedures, RTS rates vary widely. Patients who underwent ABR had RTS rates of 44% to 93%, whereas Latarjet procedures had higher RTS rates of 65% to 96%, depending on the specific sport.2,27,34 Nevertheless, 56% to 71% of athletes were reported to return to their preinjury level of performance.8,27
To date, RTS rates after AAGR with DTA have not been determined, and how these rates and recovery timelines differ between AAGR and ABR remains unknown. This study aimed to compare RTS and recurrence rates between AAGR and ABR procedures to best inform clinicians and sports participants on expected RTS rates and timelines. We hypothesized that AAGR would provide higher RTS rates and lower recurrence compared with ABR.
Methods
Study Design and Patient Selection
This cohort study is a retrospective analysis of prospectively collected data from patients’ charts. Data from patients who underwent either AAGR with DTA or ABR for anterior shoulder instability between 2016 and 2021 were included in this study. All surgeries were performed by a single surgeon (I.W.), with extensive experience in both procedures. Patients were included if they participated in a sport before surgery at a self-reported recreational or competitive level. All patients were identified as having a minimum of 1 instance of anterior shoulder dislocation. Patients were excluded from the study if they had multidirectional instability, instability resulting from a glenoid fracture, were a revision case, or did not self-report participation in a sport before their injury. All surgeries and clinical follow-ups were conducted at the Queen Elizabeth Health Sciences Center in Halifax, Nova Scotia, with research ethics approval (REB No. 1027255). The study’s primary outcome was the RTS rate, defined as the number of patients who returned to sports divided by the total number of patients in each group. The secondary outcome was time to RTS, defined as the number of months until the patient returned to full sports participation. Tertiary outcomes included postoperative recurrence and/or complications.
Surgical Indications
Indications for both procedures can include one or more of the following: GBL, multiple dislocations, contact and overhead sports athletes who are at higher risk of redislocation, and/or shoulder laxity.31,41 Generally, the surgeon performed AAGR when >13.5% GBL was determined intraoperatively. 36
Surgical Procedure Overview
Both surgical procedures in this study were completed as previously reported.17,41 All patients were placed under general anesthesia, positioned in the lateral decubitus position, and a diagnostic arthroscopy was performed from the posterior viewing portal. For the ABR, the presence of an anteroinferior labral injury (Bankart lesion) was verified and subsequently addressed by releasing the labral tissue, preparing the glenoid to enhance healing potential, and securing the labrum to the glenoid with three or more Q-FIX (Smith & Nephew) knotless suture anchors (Smith & Nephew) to recreate the labrum bumper and decrease the capsular volume. 17 For AAGR, after the diagnostic arthroscopy, the procedure was performed as previously described. 41 Briefly, a DTA, which had been previously stored in a low-temperature freezer, was prepared on the back table and fixed to the anterior rim of the glenoid using 2 cannulated screws through the Halifax portal. 26 Next, a labral repair was completed over the graft and fixated onto the native glenoid rim, using an inferior to superior capsular shift, and rendering the allograft extra-articular. In both AAGR and ABR, concomitant Remplissage was performed in patients with Hill-Sachs lesions who had surgical procedures from mid-2020 onwards. This procedure involves filling the humeral head defect with the posterior capsule and infraspinatus tendon and using 2 Q-FIX sutures inserted superiorly and inferiorly within the defect. 24 Anchors are placed after graft insertion but before the Bankart repair, while the sutures are not tied until the very end of the procedure. 24 Postoperatively, all patients were encouraged to engage in physical therapy and instructed to follow rehabilitation guidelines set by the American Society of Shoulder and Elbow Surgeons. 14
Data Collection
For all included participants, patient characteristics, including age at surgery, sex, body mass index (BMI), and time of postoperative follow-up (months), were collected. Preoperative information collected from patients’ charts included the sport each individual participates in and the competition level at which they play (recreational or competitive). While “recreational” generally refers to sports played for leisure or fitness, and “competitive” to elite or varsity competition, the ultimate categorization was determined by the patient.
The glenoid width defect was determined intraoperatively through measurement of the anterior-posterior (AP) glenoid width. Using this value and the superior-inferior glenoid dimension measured on the preoperative CT (computed tomography) scan, 32 the percentage of GBL was calculated mathematically based on ratios. 30 Intraoperatively, the width and depth of the Hill-Sachs lesion were also measured using a calibrated probe from the posterior portal and compared between groups, as well as whether or not a remplissage procedure was performed.
At a minimum of 24 months postoperatively, data were collected by emailing patients a survey regarding their RTS status, including whether they returned to sport (yes/no) and the date they returned to sports in full (identified as time to RTS). The time to RTS was determined as the interval from surgery to the date patients reported resuming regular participation in their chosen sport, as recorded in postoperative clinical follow-ups and standardized patient questionnaires. If a patient reported not returning to sports, the reason was specified. These reasons were categorized into (a) aged out of league; (b) work/school/life became my priority; (c) pain/problems with joints; (d) lack of confidence/fear of reinjury; and (e) redislocation. As a secondary analysis, complications, such as redislocation, subluxation, infection, hardware complications, nerve injury, graft or glenoid fractures, or stiffness/adhesive capsulitis, were recorded. Postoperative CT scans, when available, were used to determine graft or hardware complications. All patients who had a CT pre- and postoperatively underwent 2-mm axial CT scans in supine, sagittal, and coronal positions, with 3-dimensional reconstructions.
Statistical Analysis
All statistical analyses were performed in RStudio (Version 2023.03.0+386; RStudio, Inc), and significance was set to α = .05. To statistically compare between surgical groups (ABR and AAGR) for each categorical variable, including the rate of RTS, level of sport, concomitant remplissage, and sex, cross tabulation with a chi-square statistic was completed. To analyze the differences between the AAGR group and ABR group for continuous variables, including time to RTS (in months), age at surgery (years), time of follow up (months), GBL (%), Hill-Sachs width and depth (mm), and BMI (kg/m2), the Shapiro-Wilk test of normality and the Levene test (for homogeneity of variance) were first completed. When the data met the assumptions of normality and homogeneity, independent-samples t tests were used. When normality and homogeneity were violated, the Mann-Whitney U test was used. Lastly, for patients who did not return to their sport postoperatively, a descriptive analysis of the reasons why patients did not return was included. The distribution of sports participated in was identified and described.
Results
Patient Characteristics
A total of 230 patients were identified as having undergone AAGR with DTA or ABR between 2016 and 2021, and their charts were reviewed. After application of the inclusion and exclusion criteria, 84 patients were included in the final analysis: 40 in the ABR group and 44 in the AAGR with DTA group (Figure 1).
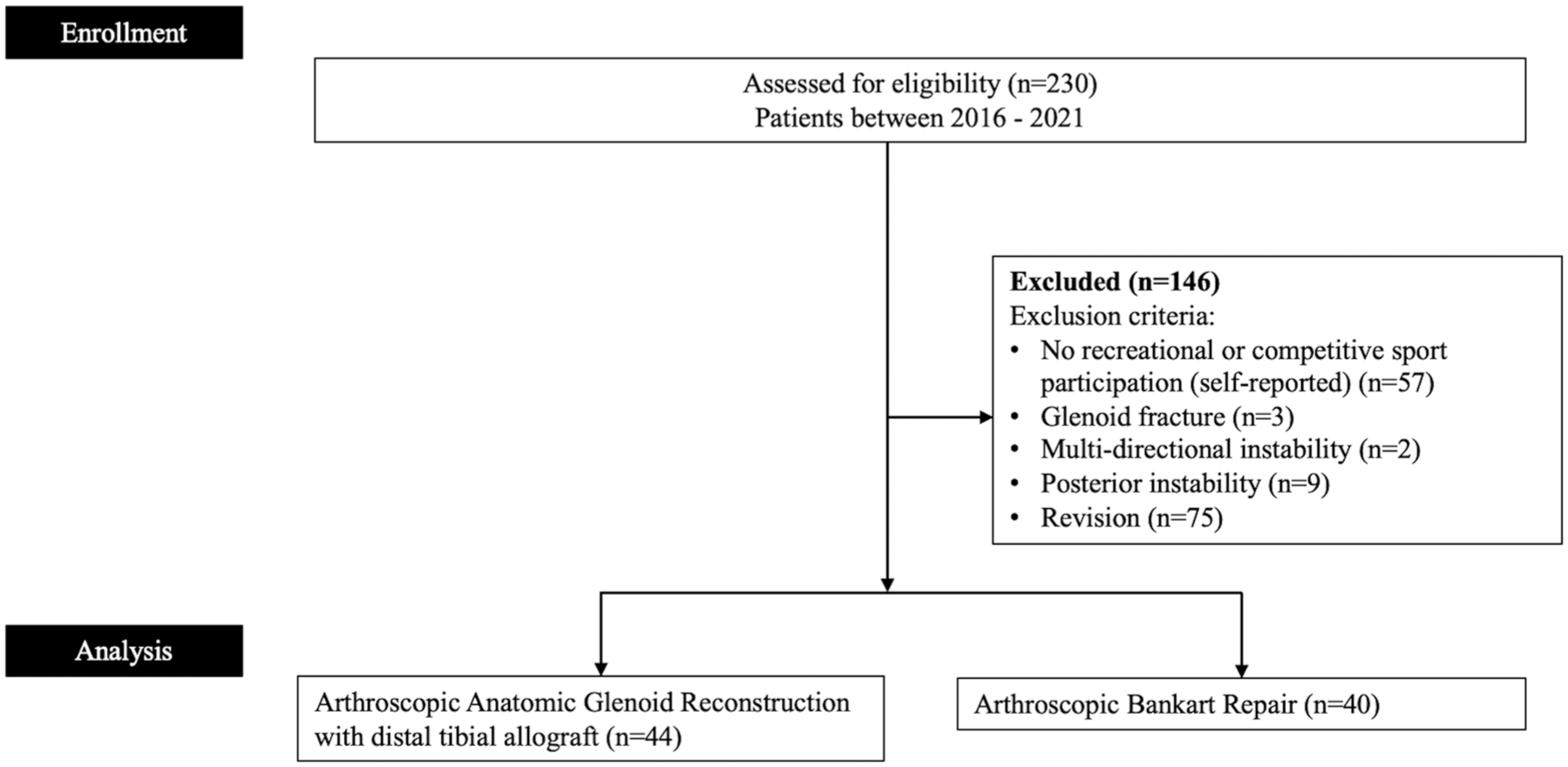
CONSORT flow diagram illustrating the number of patients included in the analysis. CONSORT, Consolidated Standards of Reporting Trials.
No statistically significant differences were observed in age, sex distribution, BMI, or concomitant Remplissage performed between the groups (Table 1). However, the mean percentage of preoperative anterior GBL was higher in the AAGR group than in the ABR group (P < .001) (Table 1). Additionally, patients in the AAGR group had deeper Hill-Sachs lesions than in the ABR group (P = .008) (Table 1).
Summary of Patient Characteristics and Baseline Characteristics Between Groups a
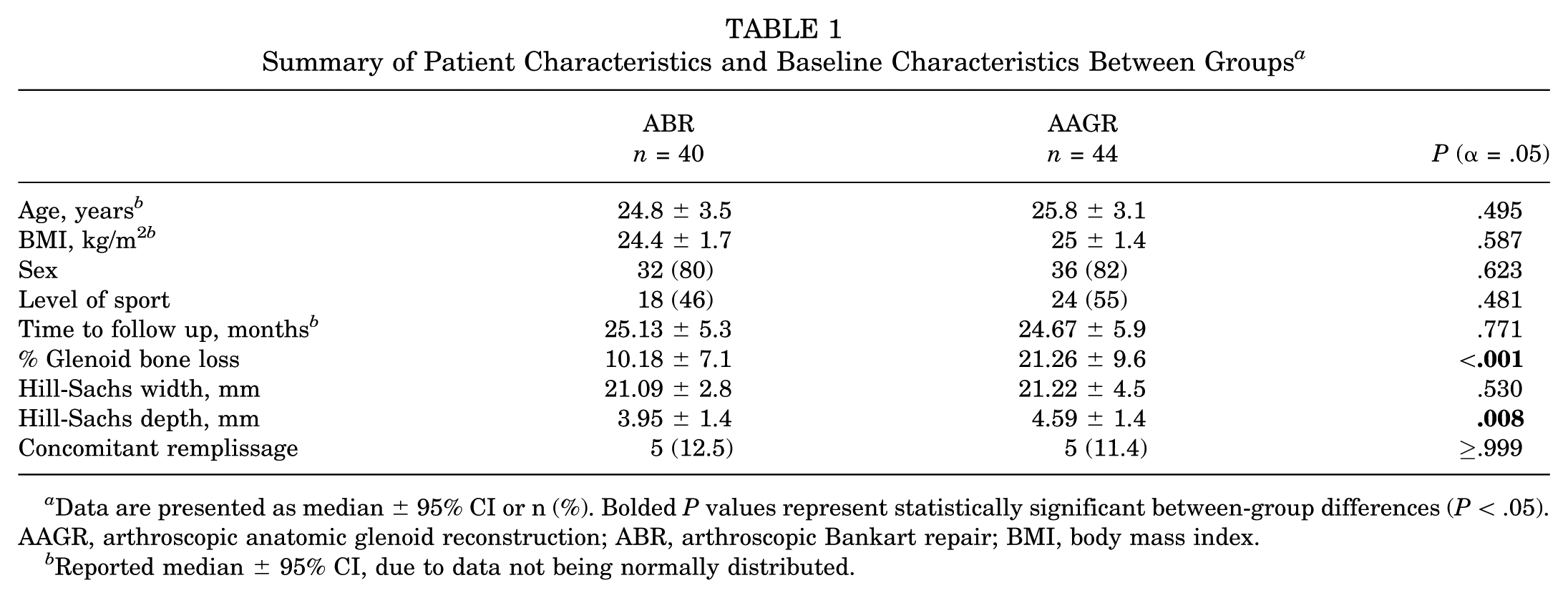
Data are presented as median ± 95% CI or n (%). Bolded P values represent statistically significant between-group differences (P < .05). AAGR, arthroscopic anatomic glenoid reconstruction; ABR, arthroscopic Bankart repair; BMI, body mass index.
Reported median ± 95% CI, due to data not being normally distributed.
The total number of patients who self-reported competitive-level sports participation before surgery was 22 in the ABR group and 20 in the AAGR group, and the number who self-reported recreational-level participation was 18 in the ABR group and 24 in the AAGR group (Figure 2). There were no statistically significant differences in the distribution of recreational versus competitive athletes between groups (Table 1). Between the 2 groups, patients reported approximately 25 different sports, with hockey most frequently reported in both the ABR (n = 9/40; 22.5%) and AAGR groups (n = 11/44; 25%).
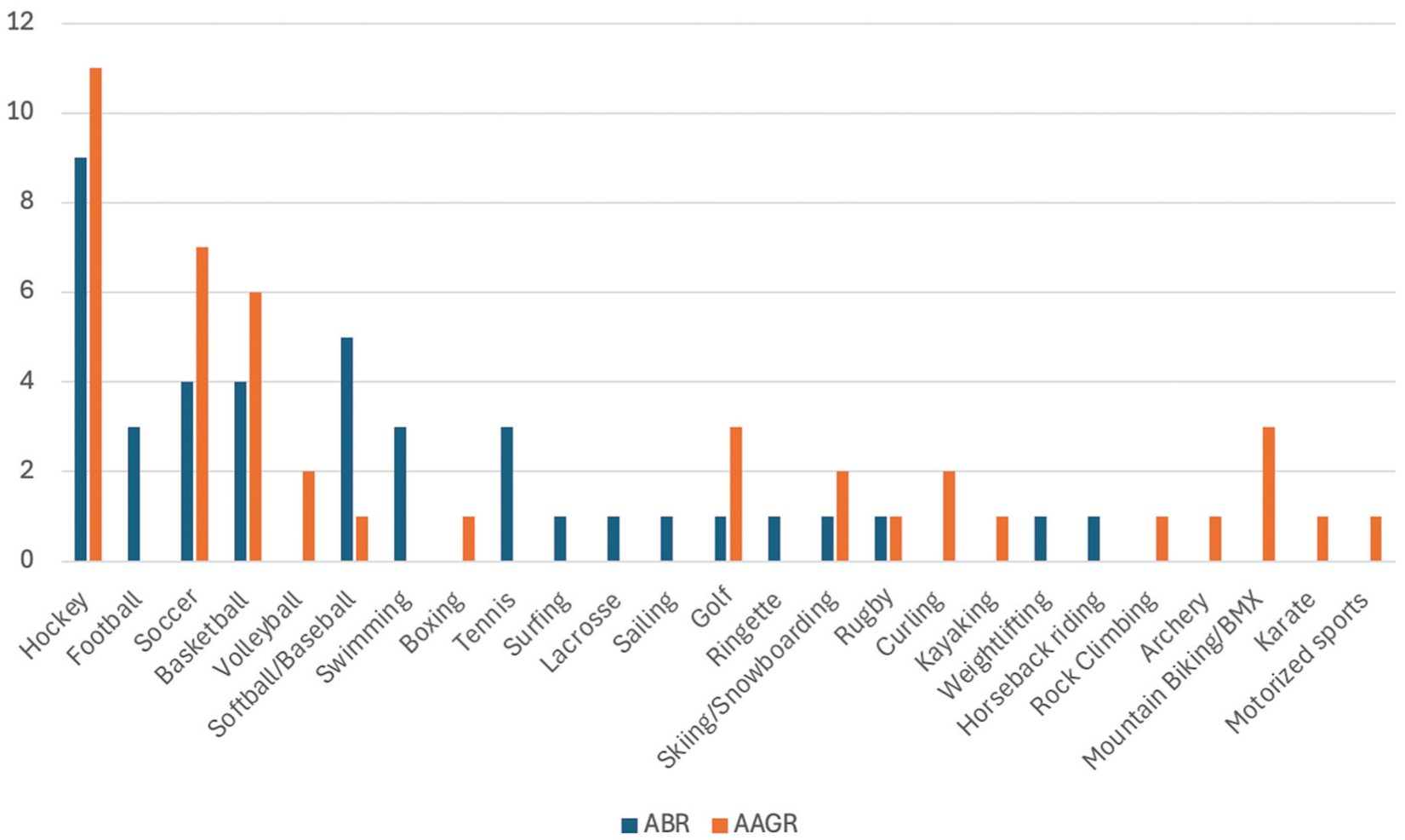
Patient self-identification of sports played at the recreational or competitive levels between the ABR group and the AAGR Group.AAGR, arthroscopic anatomic glenoid reconstruction; ABR, arthroscopic Bankart repair.
Return to Sports
At a minimum follow-up of 24 months, the overall percentage of patients who returned to sports was higher in the AAGR group than in the ABR group (P = .038). Absolute numbers and percentages are presented in Figure 3. The time to RTS among those who did return was not normally distributed; therefore, medians and 95% CIs are presented. For those who returned to sports, the median (± 95% CI) time to RTS was 9.11 ± 3.2 months in the ABR group and 9.60 ± 3 in the AAGR group (P = .514).
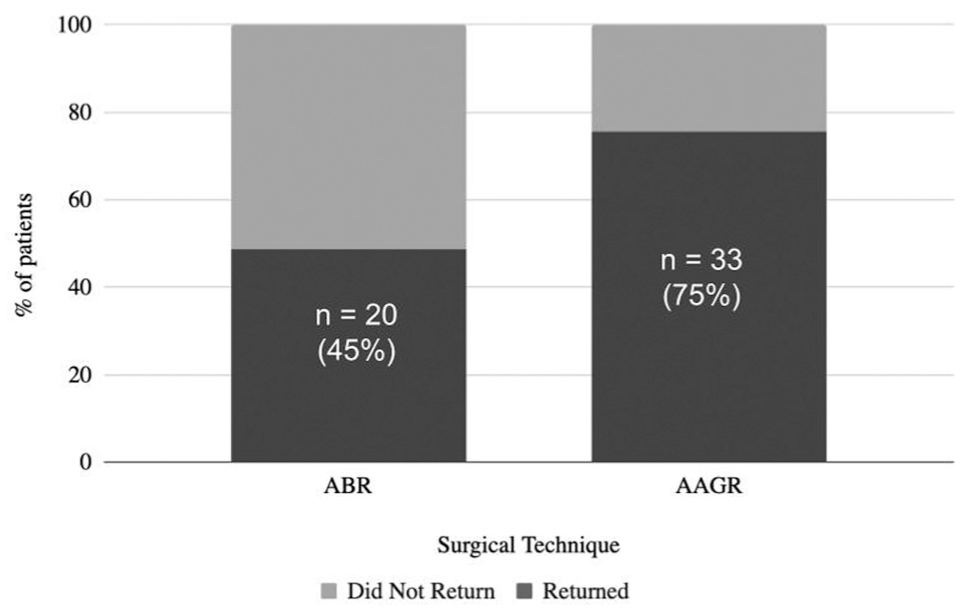
RTS rate as a percentage of patients who returned for ABR (50%) and AAGR (75%). AAGR, arthroscopic anatomic glenoid reconstruction; ABR, arthroscopic Bankart repair.
Reasons for Not Returning to Sports
Table 2 provides the number of patients in each group who did not RTS and the self-reported reasons for not returning. When excluding patients who did not return for non-shoulder-related reasons, the calculated RTS rates were 61% (ABR) and 80% (AAGR), respectively, with P = .11.
Number of Patients Within Each Group Who Did Not RTS a
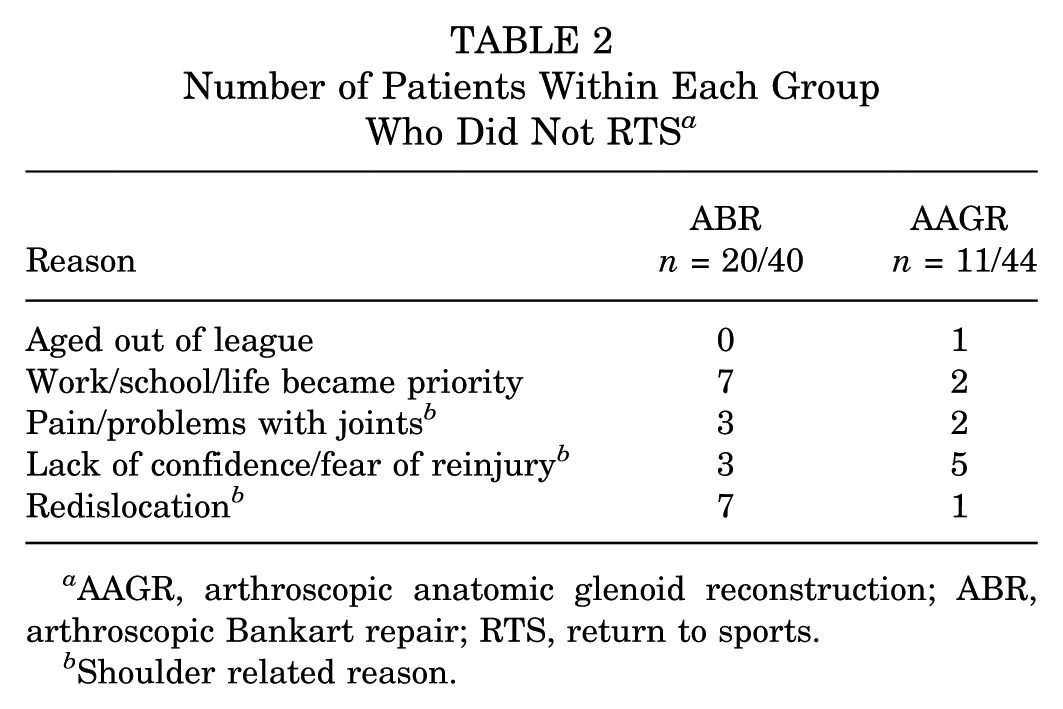
AAGR, arthroscopic anatomic glenoid reconstruction; ABR, arthroscopic Bankart repair; RTS, return to sports.
Shoulder related reason.
Complications
In total, 7 of 40 (17.5%) patients in the ABR group experienced a redislocation during follow-up, whereas only 1 of 44 (2.3%) in the AAGR with DTA group experienced redislocation (P = .025). Only 1 subluxation/subjective instability was reported in addition to the redislocations in the ABR group.Otherwise, no other complications were reported.
Discussion
This study’s major finding was that AAGR patients returned to sports at a higher rate than ABR patients, with 75% of AAGR patients and 50% of ABR patients returning to sports at a minimum of 24 months postoperatively. This finding is notable given that AAGR patients had more glenoid and humeral bone loss than ABR patients.
In the present study, patients with anterior shoulder instability who underwent AAGR with DTA demonstrated a higher RTS rate than those undergoing ABR, consistent with the study’s hypothesis. While there was no difference in time to RTS, AAGR patients experienced less postoperative recurrent instability than ABR patients while otherwise maintaining a high safety profile. Despite having larger (deeper) Hill-Sachs lesions (with no increased rate of concomitant remplissage), in addition to significantly more GBL, AAGR outperformed ABR for RTS. When comparing AAGR and ABR, our findings suggest that AAGR has an advantage in returning patients to sports.
There was a high level of RTS in the AAGR group.Specifically, 75% of AAGR patients returned to their sports in full, and when non-shoulder-related reasons were excluded, this rate increased to 80%. The adjusted RTS rate for AAGR is on par with previously reported RTS rates after the Latarjet procedure4,22,35 (54% to 100%). In contrast, the ABR group’s RTS rate was lower at 50%, improving to 61% after excluding non-shoulder-related factors. These values are within the previously reported2,12,34 RTS range for ABR (44% to 94%), where differences likely influence variations in patient populations, methodological quality, and the degree to which GBL was addressed. 16 Moreover, RTS rates in the literature have been shown to be significantly greater in patients who had a concurrent remplissage (77.8%) compared 13 with an ABR alone (50%). This concept aligns with the growing theory that Remplissage reduces overall redislocation rates. 23
Within the AAGR group, it is notable that nearly three-quarters of the 25% of patients who did not return to sports cited shoulder-related concerns, including redislocation (2.3%), shoulder pain (4.6%), or apprehension due to fear of reinjury (11.7%). Previous studies have reported that 40% to 63% of patients were fearful of reinjury after an ABR ± Remplissage or an open Latarjet, but this fear did not appear to affect the rate of RTS or other clinical outcomes.11,23 Such fears can be deeply psychological and may require interventions beyond physical rehabilitation to address. Similar patterns are observed in athletes recovering from other orthopaedic procedures.3,6 Although rehabilitation can address biomechanical deficits, psychological readiness is equally important and may require targeted interventions beyond the standard physical therapy protocol.
Our secondary outcome showed no statistically significant difference between AAGR and ABR in the timeline to RTS. Athletes in both cohorts returned to sports after approximately 9 months. Differences in our findings compared with previous evidence could be due to variations in postoperative care, rehabilitation protocols, and the types of sports referenced, which can further complicate direct comparisons.2,5,10,20 However, after the Latarjet procedure, time to RTS is often reported earlier than our findings, which are consistent with previous evidence showing that RTS timelines after an open or arthroscopic Latarjet procedure are approximately 5 months.1,7,19 Time to RTS after Bankart procedures has also previously been reported as lower than seen in our study.1,13 As an example, Fabre etal 12 reported a high rate of RTS (82%) at a mean postoperative time of 4.6 months, but also reported recurrent dislocations after returning to sports. Reasons for these discrepancies are multifold. For one, the RTS dates included in this study correspond to the time participants returned to sports “in full,” rather than “to practice,” which would occur sooner, and the possibility of recall bias could reduce the accuracy of these dates altogether. Additionally, it is noteworthy that roughly one-quarter of this study’s participants played hockey, a seasonal sport, which may affect RTS time. Nonetheless, this study’s direct comparison of AAGR and ABR under similar postoperative conditions indicates that the “invasiveness” of bone grafting is not necessarily one such factor that extends RTS time. The analysis of our data paints a detailed picture of the intricacies involved in an athlete’s decision to RTS, building on the foundation of previous research. 39
Our tertiary outcome highlighted that the redislocation rate in the AAGR group (2.3%) was lower than the ABR group (17.5%), reflecting the improved stability that AAGR offers in the setting of GBL. While concomitant remplissage is thought to improve the recurrence rate of ABR, 23 it should be noted that AAGR patients actually had larger (deeper) Hill-Sachs lesions than ABR patients, despite both groups having low rates of remplissage. Previous research has shown that procedures like the Latarjet generally yield lower redislocation rates than Bankart repair, 6 and the results of this study suggest that AAGR may achieve similarly favorable stability outcomes, 38 benefiting patients who wish to RTS. These findings are further contextualized by a meta-analysis comparing ABR and Latarjet, which demonstrated that Latarjet has lower recurrence rates, better patient-reported outcomes, and a quicker RTS, but is associated with more complications. 18 Although the Latarjet excels at mitigating recurrent instability, it is associated with a higher complication profile. As such, the current study’s results indicate that AAGR with DTA may achieve stability and RTS benefits similar to Latarjet without the increased complication risk. Future studies should directly compare AAGR with other bony augmentation procedures, such as the Latarjet procedure, to establish their comparative effectiveness.
Overall, a multifaceted approach to understanding RTS decisions is echoed in findings related to other medical procedures.21,37 For example, athletes recovering from surgeries like the Bankart repair 21 or anterior cruciate ligament reconstruction 37 often grapple not just with the physical aspects of their recovery, but also with the psychological and situational factors that can influence their desire or ability to reengage with competitive sports. The broader picture, thus, is one of complex interplay between physical healing, psychological readiness, and life circumstances.
Strengths and Limitations
The strengths of this study include the comparison of 2 groups, ABR and AAGR, for investigating RTS in patients with anterior shoulder instability. Although the degree of GBL differed between groups, their mean GBL was in line with the respective indications for each procedure, allowing a practical comparison. This study leverages intraoperative glenoid AP width to precisely quantify the glenoid width defect and, subsequently, compare the extent of bone loss among participants, offering a comprehensive understanding of baseline conditions. Only half of the patients had a preoperative CT scan, and GBL was measured only to help characterize the cohorts and was not the main outcome of the study. The study’s data originate from a single location where a single surgeon performed the procedures, ensuring uniformity in surgical methods, postoperative care, and subsequent monitoring. Despite this strength, the study’s retrospective nature means there was no preplanned allocation of surgical procedures. Due to the participants’ young age, maintaining consistent follow-ups proved difficult. Yet, our hospital’s province-wide imaging system (picture archiving and communication system [PACS]) ensured that all postoperative imaging for participants’ shoulders was available for assessment and that almost all complications requiring surgical attention were documented. Another limitation is the absence of data on the specific number of preoperative dislocations, symptom duration, and time to surgery, which could be confounding variables. Furthermore, collecting RTS outcomes via email survey rather than objective measurement (eg, surgeon clearance) may be a limitation due to potential information or recall biases. However, other previous studies have also used survey-based collection methods for RTS for shoulder instability populations.15,21 Future studies should further examine the precise level at which patients returned to sports, as this may be associated with patient satisfaction and surgical success. Lastly, future studies should compare AAGR to ABR + remplissage or the Latarjet procedure, which could not be completed in the present study since ABR + remplissage was not regularly performed during the study’s retrospective timeframe.
Conclusion
In patients with anterior shoulder instability, our study showed that AAGR demonstrated superior patient-reported RTS rates and lower redislocation rates than ABR, with comparable recovery timelines, despite the AAGR group having higher GBL. These findings suggest that a bone block procedure may achieve higher RTS rates than ABR alone. This study provides valuable guidance for clinicians advising athletes on surgical options by establishing appropriate RTS expectations and demonstrating that AAGR provides suitable RTS in the presence of GBL.
Footnotes
Final revision submitted February 23, 2026; accepted March 19, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: I.W. receives personal fees from DePuy Mitek Inc, Smith & Nephew Inc, CONMED Corp, Bioventus LLC, Arthrex, and VALD, outside the submitted work; and is an editorial board member of the American Journal of Sports Medicine, Arthroscopy, and The HIVE Musculoskeletal Journal; is a board or committee member of the Arthroscopy Association of North America, the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine, and Arthroscopy Association of Canada; and is an associate editor of the Orthopaedic Journal of Sports Medicine.
Ethical approval for this study was obtained from Queen Elizabeth Health Sciences Center in Halifax, Nova Scotia (REB No. 1027255).