
Abstract
Background:
Anterior cruciate ligament reconstruction (ACLR) is time-sensitive, as surgical delays exceeding 120 days are associated with an increased risk of secondary meniscal injury. Insurance type is a known determinant of health care access; however, its specific impact on time to ACLR is poorly characterized.
Purpose:
To determine the effect of insurance type on the known increased risk of surgical delay >120 days in patients undergoing ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A dual-center retrospective cohort study was conducted, including 2030 patients (age, 9-73 years) who underwent primary ACLR between 2013 and 2023 at 2 centers. Patients were stratified by insurance type: private (n = 1619), public (n = 362), self-pay (n = 27), and workers’ compensation (n = 22). The primary outcome was surgical delay, defined as >120 days from injury to surgery. This threshold was selected a priori based on institutional data linking this threshold to increased risk of secondary meniscal injury. Multivariable logistic regression, including 2008 patients (private, public, and self-pay), was used to estimate adjusted odds ratios (aORs) with 95% CIs for the risk of delay. The model compared patients with public insurance and self-pay status to those with private insurance (the reference group) and was adjusted for confounding effects of patient age, biological sex, and injury type (sports-related vs nonsports-related). The multivariable logistic regression was restricted to patients with private, public, and self-pay insurance; the workers’ compensation cohort was omitted from this analysis due to sample size considerations.
Results:
Descriptive statistics revealed substantial differences in median wait times by insurance type: privately insured patients (median, 55 days [interquartile range, IQR, 90.5]), publicly insured patients (median, 106 days [IQR, 247]), self-pay patients (median, 145 days [IQR, 420]), and workers’ compensation (median, 97.5 days [IQR, 136]). Multivariable logistic regression confirmed that insurance type was a significant factor for surgical delay (>120 days). Compared with patients with private insurance, those with public insurance were 1.86 times more likely (95% CI, 1.43-2.43; P < .001), and self-pay patients were 2.75 times more likely (95% CI, 1.25-6.27; P = .013) to experience surgical delay.
Conclusion:
This study demonstrates that insurance status is a significant independent factor of delayed ACLR. Patients with public or self-pay insurance experience significantly longer wait times and are at markedly higher risk of surgical delays exceeding 120 days compared with privately insured patients, highlighting a substantial inequity in access to timely orthopaedic sports medicine care.
Keywords
Anterior cruciate ligament (ACL) rupture is a common, debilitating knee injury. Surgical reconstruction (ACLR) is the standard of care for active individuals and those with functional instability, aiming to restore knee kinematics, facilitate return to activity, and mitigate the risk of secondary joint injury.
The timing of anterior cruciate ligament reconstruction (ACLR) is a critical component of clinical management. A delay between injury and surgery is associated with several adverse outcomes—including increased rates of concomitant meniscal tears, chondral injuries, and the development of new meniscal tears.4,6-11,17,20 These secondary injuries can alter the natural history of the knee, complicate the surgical procedure, and potentially accelerate the progression of posttraumatic osteoarthritis.1,2 Consequently, identifying and addressing modifiable factors that contribute to surgical delay is a significant priority in orthopaedic sports medicine.
In the United States health care system, insurance status is a well-established social determinant of health and a principal factor influencing access to care. Numerous studies across surgical specialties have documented disparities in wait times, access to specialists, and receipt of operative care based on a patient's insurance provider.3,5,12,14,15,16,18,19 Patients with public insurance or those who are self-pay often face greater barriers to care than their privately insured counterparts.3,5,12,14,15,16,18,19
While the detrimental effects of delayed ACLR are well-documented, and the impact of insurance on health care access is broadly recognized, the specific relationship between insurance type and time to ACLR remains poorly characterized. A clear understanding of this relationship is essential to identify systemic barriers and develop targeted interventions to ensure equitable care.
Therefore, this study aimed to examine the association between insurance type and the length of surgical wait times in patients undergoing ACLR. We hypothesized that patients with public insurance or self-pay status would experience significantly longer delays to surgery than those with private insurance.
Methods
Study Design and Patient Selection
After obtaining institutional review board approval
The exclusion criteria included previous ipsilateral ACLR, relevant previous knee surgery (eg, tibial tubercle osteotomy, meniscal repair/surgery), concurrent procedures other than meniscal/chondral treatment, tibial plateau or avulsion fractures (eg, posterior cruciate ligament [PCL] reconstruction), and patient primary residence outside of Oregon or Washington. Patients with no documented injury date in the electronic health record were also excluded from the analysis.
Variable and Data Collection
Demographic data collected included patient age at the time of surgery and biological sex. The primary exposure variable was insurance type, which was categorized into 4 groups: (1) private insurance (n = 1619); (2) public insurance (including Medicaid, Medicare, and Tricare, n = 362); (3) self-pay (n = 27); and (4) workers’ compensation (n = 22). The primary outcome was surgical delay, defined as the time from injury to surgery exceeding 120 days. This threshold was established based on internal institutional review of clinical outcomes and is consistent with the established understanding that prolonged delays increase the risk of secondary knee pathology.
Given the distinct nature of workers' compensation claims and the small sample sizes in the workers' compensation group, the primary analysis focused on comparing public and self-pay patients with the privately insured reference group. Descriptive statistics are reported for all groups for transparency.
Statistical Analysis
Descriptive statistics were calculated for the entire cohort and stratified by insurance group. Continuous variables were reported as means with standard deviations or medians with interquartile ranges (IQR) based on normality, assessed using the Shapiro-Wilk test. Categorical variables were reported as frequencies and percentages. Unadjusted differences in time to surgery across insurance groups were compared using the Kruskal-Wallis H test, as the data were non-normally distributed.
A multivariable logistic regression model was constructed to determine the independent association between insurance type and the odds of experiencing a surgical delay (>120 days). The model compared patients with public insurance and self-pay status with those with private insurance, which served as the reference group. The workers’ compensation cohort was excluded from this regression analysis due to its small size, which would preclude stable and reliable parameter estimates.
The regression model was adjusted for potential confounding variables identified a priori through clinical relevance. These covariates included patient age (continuous), sex (categorical: male or female), and injury type (categorical: sports-related or nonsports-related). The regression results are presented as adjusted odds ratios (aORs) with corresponding 95% CIs. A 2-tailed P < .05 was considered statistically significant for all analyses. All statistical analyses were performed using RStudio (Version 2025.1.513; RStudio, Inc).
Results
Patient Cohort
This study included 2030 patients (mean age, 30.6 ± 12.7 years; 50.6% male) undergoing primary ACLR between 2013 and 2023. A total of 532 patients were excluded due to previous ipsilateral knee surgery, residence outside the study region, concomitant fracture, missing injury date, or missing insurance status. The cohort comprised 76.4% sports-related injuries.
Unadjusted Analysis of Time to Surgery
The overall median time from injury to surgery was 62 days (IQR, 112.5). Unadjusted analysis revealed substantial, statistically significant differences in time to surgery across insurance groups (P < .001; Kruskal-Wallis test). As detailed in Table 1, median wait times were shortest for privately insured patients (55 days) and markedly longer for those with public insurance (106 days), self-pay status (145 days), and workers’ compensation (97.5 days). The proportion of patients experiencing a surgical delay exceeding 120 days for each insurance group is presented in Table 2.
Time to Surgery by Insurance Type a

The mean time to surgery is substantially higher than the median for all groups, indicating a right-skewed distribution, where a minority of patients experienced very prolonged delays. IQR, interquartile range.
Baseline Patient Characteristics by Insurance Type a
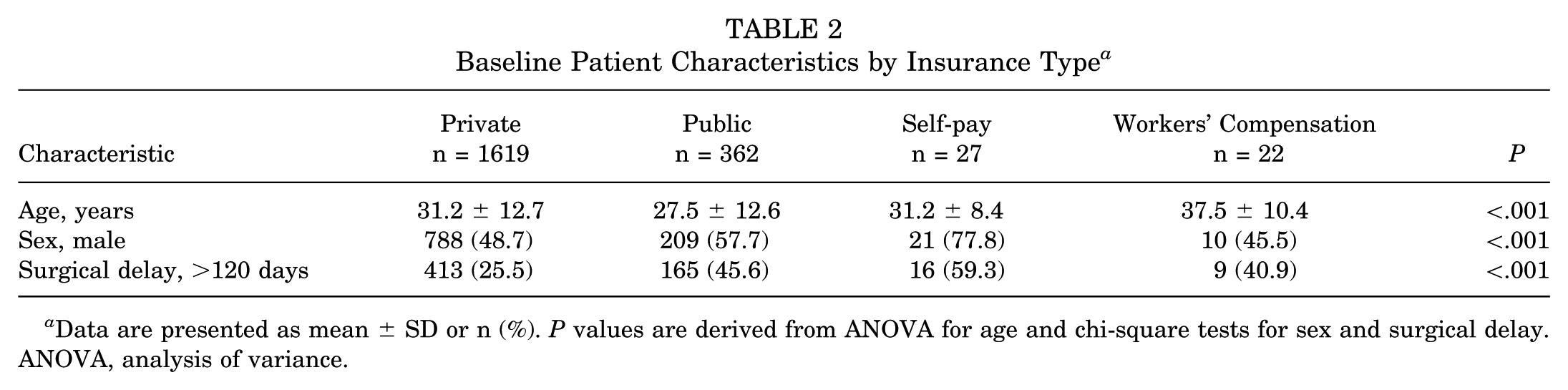
Data are presented as mean ± SD or n (%). P values are derived from ANOVA for age and chi-square tests for sex and surgical delay. ANOVA, analysis of variance.
Multivariable Logistic Regression for Surgical Delay
In the multivariable model adjusted for age, sex, and injury type, insurance type was a significant independent factor of surgical delay exceeding 120 days.
Compared with patients with private insurance (reference group), patients with public insurance had 1.86 times the odds of experiencing a surgical delay (aOR, 1.86 [95% CI, 1.43-2.43]; P < .001).
Self-pay patients had 2.75 times the odds of a significant delay compared with the privately insured reference group (aOR, 2.75 [95% CI, 1.25-6.27]; P = .013).
Secondary analysis also identified nonsports-related injury mechanism (aOR, 3.20 [95% CI, 2.34-4.39]; P < .001), increasing patient age (aOR, 1.02 per year [95% CI, 1.02-1.03]; P < .001), and male sex (aOR, 1.24 [95% CI, 1.02-1.52]; P = .036) as significant independent factors of surgical delay. The full results of the multivariable regression analysis are presented in Table 3.
Multivariable Logistic Regression Analysis of Factors Associated with Surgical Delay (>120 Days) a

This model presents the adjusted odds of surgical delay (>120 days) for patients undergoing ACLR. The model demonstrates that public insurance, self-pay status, nonsports-related injury mechanism, increasing age, and male sex are independent risk factors for delayed surgery. Workers’ compensation was excluded from the regression model due to the small sample size. aOR, adjusted odds ratio.
Discussion
The major findings of this study demonstrated that insurance status is a powerful, independent factor of delayed ACLR, revealing significant disparities in access to timely orthopaedic care. After adjusting for age, sex, and injury mechanism, patients with public insurance had 1.86 times the odds of experiencing a surgical delay exceeding 120 days (aOR, 1.86 [95% CI, 1.43-2.43]; P < .001), while self-pay patients had 2.75 times the odds (aOR, 2.75 [95% CI, 1.25-6.27]; P = .013), compared with their privately insured counterparts. These findings underscore that financial and systemic barriers, rather than clinical factors alone, are primary drivers of surgical timing for ACL injury. Notably, the median wait time for publicly insured patients (106 days) approached the 120-day threshold, while self-pay patients (145 days) exceeded it, suggesting that these populations are at substantially increased risk for secondary intra-articular damage associated with prolonged delay.4,6-11,17,20
These results are consistent with previous literature demonstrating that insurance status is a strong determinant of health care access.3,5,12,14,15,18,19 Previous studies have indicated that wait times, utilization of advanced imaging techniques, and the likelihood of receiving surgical intervention for patients seeking orthopaedic services depend on the insurance payer.3,5,12,14,15,16,18,19 However, limited research has been conducted on how types of insurance affect ACLR. Given that delayed ACLR is associated with increased rates of chondral and meniscal injury in the ACL-deficient knee, the disparities identified in the present investigation suggest that publicly insured and self-pay patients may be at increased risk of developing further intra-articular damage.4,6,11,17,20
The mechanisms driving these disparities are multifactorial, stemming from both systemic structures and patient-level factors. 21 Lower reimbursement rates and complex administrative hurdles for public insurance often limit provider participation and appointment availability.3,5,12,14,15,18,19,21 For self-pay patients, the substantial out-of-pocket cost of surgery is likely a prohibitive barrier, leading to a detrimental postponement. 3 Furthermore, our analysis revealed that a nonsports-related injury mechanism was the strongest factor of delay (aOR, 3.20). This may reflect systemic factors, such as scheduler perceptions of injury acuity or legitimacy, as well as patient-level factors, including differential motivation to expedite care. Specifically, athletes often have a clear goal of returning to sport, which may drive them to seek and prioritize surgery more aggressively than individuals whose primary goal is a return to activities of daily living.
Clinically, these findings highlight a systemic issue in which access to timely care is influenced by insurance type.3,5,12,14,15,16,18,19 Therefore, solutions may be most effective at a systems level rather than an individual practitioner level. Implementing institutional support structures, such as patient navigation programs and standardized social risk screening, could help identify patients at high risk for delay and facilitate access to resources. Broader policy reforms aimed at making public insurance more viable for providers may also be necessary to expand network access and ultimately reduce these care delays. 13
Addressing these inequities requires a multifaceted approach that targets the systemic structures within the health care system. Lower reimbursement rates for public and workers’ compensation insurance compared with private insurance may disincentivize timely care, contributing to surgical delays. Increasing reimbursement rates could incentivize providers and hospitals to deliver more equitable, timely ACLR to these patient populations.
The findings of this study highlight several critical avenues for future research. First, prospective studies are needed to evaluate targeted interventions, such as patient navigation programs, designed to mitigate delays in high-risk populations. Second, qualitative investigations exploring the decision-making processes of both patients and schedulers could provide deeper insight into the root causes of these disparities. Finally, dual-center collaborative efforts are necessary to establish an externally validated, evidence-based definition of a clinically significant delay in ACLR, moving beyond single-institution thresholds.
This investigation has several limitations inherent to its design. The retrospective nature introduces potential for selection bias and reliance on inaccurate documentation. Although the study was dual-center, its inclusion of patients solely from Oregon and Washington may limit the generalizability of the findings to other geographic regions or care settings with different health care dynamics. Importantly, we could not account for key socioeconomic confounders, such as income, education, health literacy, or access to transportation, which may influence both insurance status and health care engagement. Additionally, we were unable to capture patient-specific factors that may influence surgical timing, such as delaying surgery to coincide with school breaks, summer vacation, or work schedules. These factors may disproportionately affect younger patients and families regardless of insurance status.
Furthermore, while we excluded patients with concomitant ligament injuries requiring repair or reconstruction (eg, PCL, multi-ligament injuries), we could not reliably account for medial collateral ligament injuries treated nonoperatively, which may contribute to surgical delay independent of insurance status. However, the proportion of patients with such injuries in our cohort was likely small. Additionally, while we adjusted for age as a continuous variable in our regression model, we did not perform subgroup analyses by specific age categories (eg, pediatric, adolescent, geriatric) that may have different delay thresholds or risk profiles. Despite adjusting for available clinical variables, unmeasured confounding remains a concern. Finally, the 120-day threshold for defining surgical delay, while based on institutional clinical experience and consistent in identifying prolonged delays, has not been externally validated. Future dual-center studies could work to establish a standardized, evidence-based definition of significant delay.
Despite these limitations, our study strengths include a large sample size, a decade-long cohort, strict inclusion criteria, and a multivariate analysis that controlled for key clinical variables. In conclusion, this study provides robust evidence that insurance type is a primary, independent determinant of access to timely ACLR.
Conclusion
This study demonstrates that insurance status is a significant independent factor of delayed ACLR. Patients with public or self-pay insurance experience significantly longer wait times and are at markedly higher risk of surgical delays exceeding 120 days compared with privately insured patients, highlighting a substantial inequity in access to timely orthopaedic sports medicine care.
Footnotes
Final revision submitted February 18, 2026; accepted March 20, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Oregon Health and Science University (IRB 25784).