
Abstract
Background:
The optimal graft choice for anterior cruciate ligament reconstruction (ACLR) remains a subject of ongoing debate. In practice, graft selection in ACLR is multifactorial, with patient characteristics, activity level, and surgeon preference/training background all playing a crucial role in the clinical decision-making process. While graft trends have been reported across select professional sports leagues, none have focused specifically on professional soccer.
Purpose:
To report current trends in graft preference for ACLR among Major League Soccer (MLS) surgeons.
Study Design:
Cross-sectional study.
Methods:
A 39-question survey was distributed to 27 orthopaedic surgeons affiliated with MLS teams in January 2025. The questionnaire captured each respondent's preferences regarding ACLR management in both the general population and high-level/professional soccer athletes. Descriptive statistics were used to summarize responses.
Results:
Surgeons averaged 7.7 years caring for MLS teams and performed a mean of 80 ± 27 ACLRs annually. In primary ACLR for professional soccer athletes, the bone-patellar tendon-bone (BPTB) autograft was preferred (74%), followed by the quadriceps tendon (QT) autograft (22.2%). The hamstring tendon (HT) autograft was uncommon (3.7%). Similar trends were reported for the general population: BPTB autograft (70%), QT autograft (22.2%), and HT autograft (3.7%). For revision procedures, QT autograft was favored (48.2%), followed by BPTB autograft (25.9%) and BPTB allograft (11.1%). Contralateral autografts were more common in revisions (44.4%) than in primary cases (7.4%). Lateral extra-articular augmentation (LEA) was performed in 31.5% of primary cases and 76% of revision cases; iliotibial band tenodesis was favored over anterolateral ligament reconstruction (74.1% vs 25.9%). LEA utilization increased compared with 5 years prior (6.4% vs 29.4%).
Conclusion:
Among orthopaedic surgeons caring for MLS athletes, BPTB autografts were the preferred graft for primary ACLR. QT autografts were preferred over HT autografts in primary ACLR, and QT autografts were most commonly used in revision surgery. HT autografts were rarely used in primary ACLR and were not preferred in revision scenarios. LEA procedures were widely used among professional soccer athletes.
Keywords
The anterior cruciate ligament (ACL) is a dense, fibrous band of connective tissue within the knee joint that originates from the posteromedial aspect of the lateral femoral condyle and inserts onto the anterior intercondylar area of the tibia. It consists of 2 distinct functional bundles, the anteromedial and posterolateral bundles, named for their insertion site on the proximal tibia. The ACL serves as the primary restraint to anterior tibial translation relative to the femur and also contributes to rotational stability, particularly during cutting, pivoting, and landing.10,18,28,41
ACL injury rates in the general population are variable, but a population-based study reported an annual incidence rate of 68.6 per 100,000 person-years. 31 Among competitive athletes, incidence also varies by sport, sex, and level of play. In elite soccer, the incidence rate of ACL injuries is 2 to 3 times higher in female athletes than in male athletes, 37 with reported 4 rates of 0.057 and 0.10 per 1000 match hours, for males and females, respectively. Most injuries are noncontact and occur during pivoting, cutting, or landing maneuvers, while contact injuries (often related to tackling) account for a smaller proportion.3,4 Although not all ACL injuries require surgery, patients with symptomatic instability or those seeking expeditious return to high-level sport are typically indicated for surgery.
The American Academy of Orthopaedic Surgeons strongly advocates that surgical candidates with acute isolated ACL tears undergo reconstruction within 3 months to minimize the risk of secondary meniscal or chondral injury. 6 Reconstruction is preferred over repair due to lower revision rates, with autografts recommended over allografts for primary procedures. 6 Bone-patellar tendon-bone (BPTB) autografts are moderately recommended over hamstring tendon (HT) and quadriceps tendon (QT) autografts, as BPTB grafts may be associated with lower failure rates. 6 Furthermore, moderate evidence supports consideration of anterolateral ligament (ALL) reconstruction or lateral extra-articular tenodesis (LET) to improve short-term function, provide additional rotatory stability, and reduce graft failure in select patients. 6 In patients with a primary HT reconstruction, the addition of LET decreased the rate of rerupture from 11% to 4% at 2 years. 16
Although these guidelines are supported by systematic reviews and expert consensus, they are based on heterogeneous populations. Evidence specific to elite and professional athletes remains limited, leaving team physicians largely reliant on clinical experience when managing these injuries. The present study aimed to survey team physicians in Major League Soccer (MLS) to evaluate current surgical practices and trends in ACL injury management. While these findings represent expert opinion rather than formal evidence, they may help guide the care of high-level soccer athletes in one of the world's most widely played sports.
Methods
A 39-question survey was distributed to orthopaedic surgeons affiliated with MLS teams across the United States in January of 2025. The survey was created with SurveyMonkey and distributed to 27 MLS-affiliated surgeons who previously agreed to participate in this project. The questionnaire asked each respondent for their time served as a MLS orthopaedic surgeon, as well as numerous questions about their preferences for managing ACL reconstruction (ACLR) operations in both their general practice and high-level/professional soccer athletes. ACLR timing, anesthesia protocols, graft selection, use of augmentation techniques, indications for LET, and return-to-play timelines were among the themes covered by the survey. A full list of survey questions is available in Appendix 1. Questions were predominantly multiple choice, with a write-in option if the respondent's preferences were not listed. Survey questions were framed in the context of an isolated ACL injury and did not specifically address multiligamentous injuries. Descriptive statistics were used to summarize responses.
Results
Operational Logistics
All 27 surgeons who received the survey responded. The mean time in practice as a MLS orthopaedic surgeon was 7.7 years. Across this cohort, surgeons performed a mean of 80 ± 27 ACLRs per year. When performing ACLR, delayed surgical intervention was preferred, with 48% of respondents reporting their ideal time to operation as 3 to 10 weeks after injury, 44.4% opting for surgery between 8 days and 3 weeks, and only 7% preferring surgery between 2 and 8 days. Most respondents (92.6%) reported use of general anesthesia, with a few opting for spinal anesthesia with monitored anesthesia care (MAC). All respondents used a peripheral nerve blockade, with 57.7% preferring an adductor canal block, 12% choosing a femoral nerve block, 4% opting for multiple nerve blocks, and 26.9% using only local infiltration anesthesia. There were no responses for saphenous nerve blockade. Surgeons preferred to utilize a tourniquet intraoperatively, with 73% choosing to keep the tourniquet inflated throughout the entire duration of the case. These findings are summarized in Figure 1.
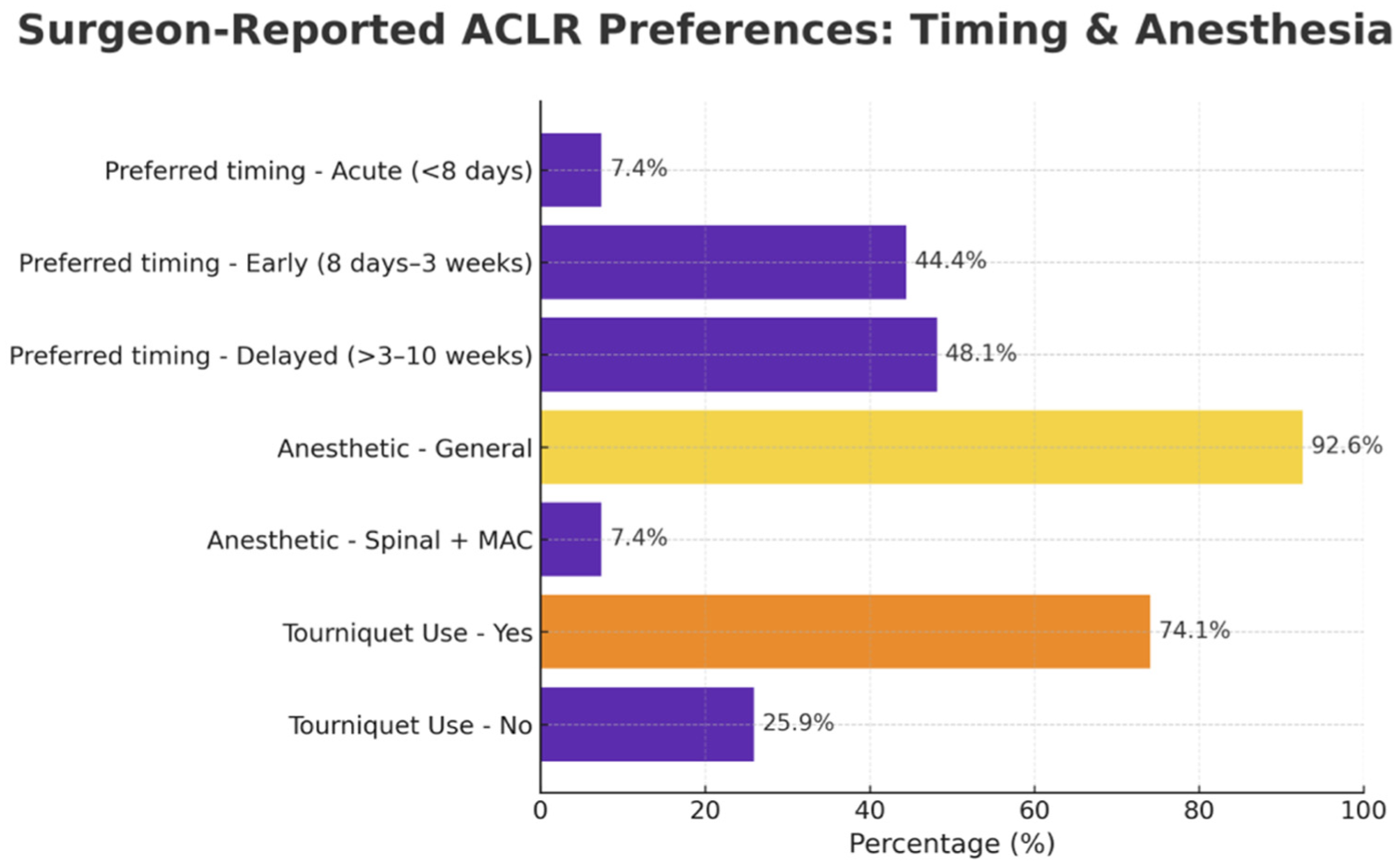
Surgeon-reported preferences regarding timing of ACLR, anesthetic approach, and tourniquet use among MLS orthopaedic surgeons. ACLR, anterior cruciate ligament reconstruction; MLS, Major League Soccer; MAC, monitored anesthesia care.
Grafts
Graft choice is summarized in Figure 2. For the general population, the preferred graft for primary ACLR was BPTB autograft (70%), followed by QT autograft (22.2%), HT (4-strand semitendinosus-gracilis) autograft (3.7%), and ipsilateral BPTB or QT autograft (3.7%). In revision ACLR, QT autograft (48.2%) was the predominant choice, followed by BPTB autograft (25.9%), BPTB allograft (11.1%), soft tissue allograft (3.7%), and ipsilateral BPTB or QT autograft (3.7%), with 7.4% responding that their decision would depend on the athlete's sport and the primary graft utilized. Contralateral autografts were rarely utilized in index operations (7.4%), but were more commonly employed in revision settings (44.4%). Graft tensioning varied among respondents, with 22.2% of surgeons tensioning at full extension (hyperextension), 29.6% at 0° of flexion, 18.5% at 10°, 18.5% at 20°, 11.1% at 30°; no respondent reported tensioning beyond 30° of flexion.
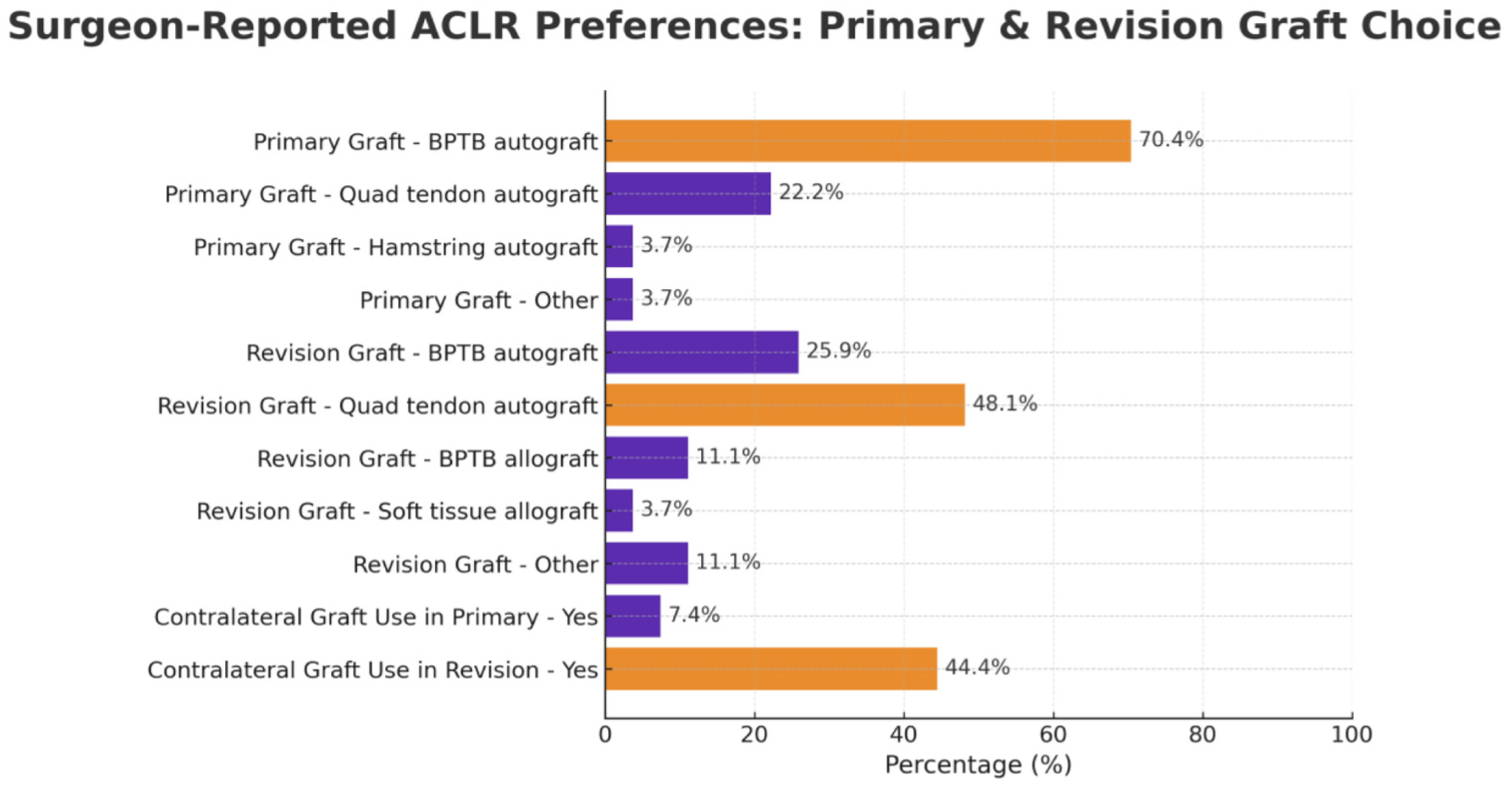
Surgeon-reported preferences for graft choice in primary and revision ACLR, including the use of contralateral autografts. ACLR, anterior cruciate ligament reconstruction; BPTB, bone-patellar tendon-bone. *Primary graft other: BPTB or quadriceps tendon autografts (both ipsilateral). *Revision graft other: Depends on primary, sport, and available tissue. Almost always an autograft.
Augmentation Procedures
Suture brace augmentation in primary ACLR was preferred by a small cohort (14.8%); however, those who used it did so on average 67% of the time. Suture brace augmentation was more common in ACLR revision surgery (25.9%), and augmentation was performed at a similar rate (69.3% of cases). Lateral extra-articular augmentation (LEA) was considered in most cases (92.6%); although, ultimately performed in about one-third of primary cases (31.5%). In revision cases, all but 1 respondent (96.3%) indicated willingness to consider augmentation with LET or ALL reconstruction, with 76% ultimately opting to perform the procedure. Among surgeons performing LEA, iliotibial band (ITB) tenodesis was the most preferred technique (74.1%), with ALL reconstruction with allograft (14.8%) and ALL reconstruction with autograft (11.1%) comprising the remainder. Overall, study participants reported performing a substantially larger proportion of combined ACLR/LET procedures compared to 5 years ago (6.4% vs 29.4%). These findings are summarized in Figure 3.
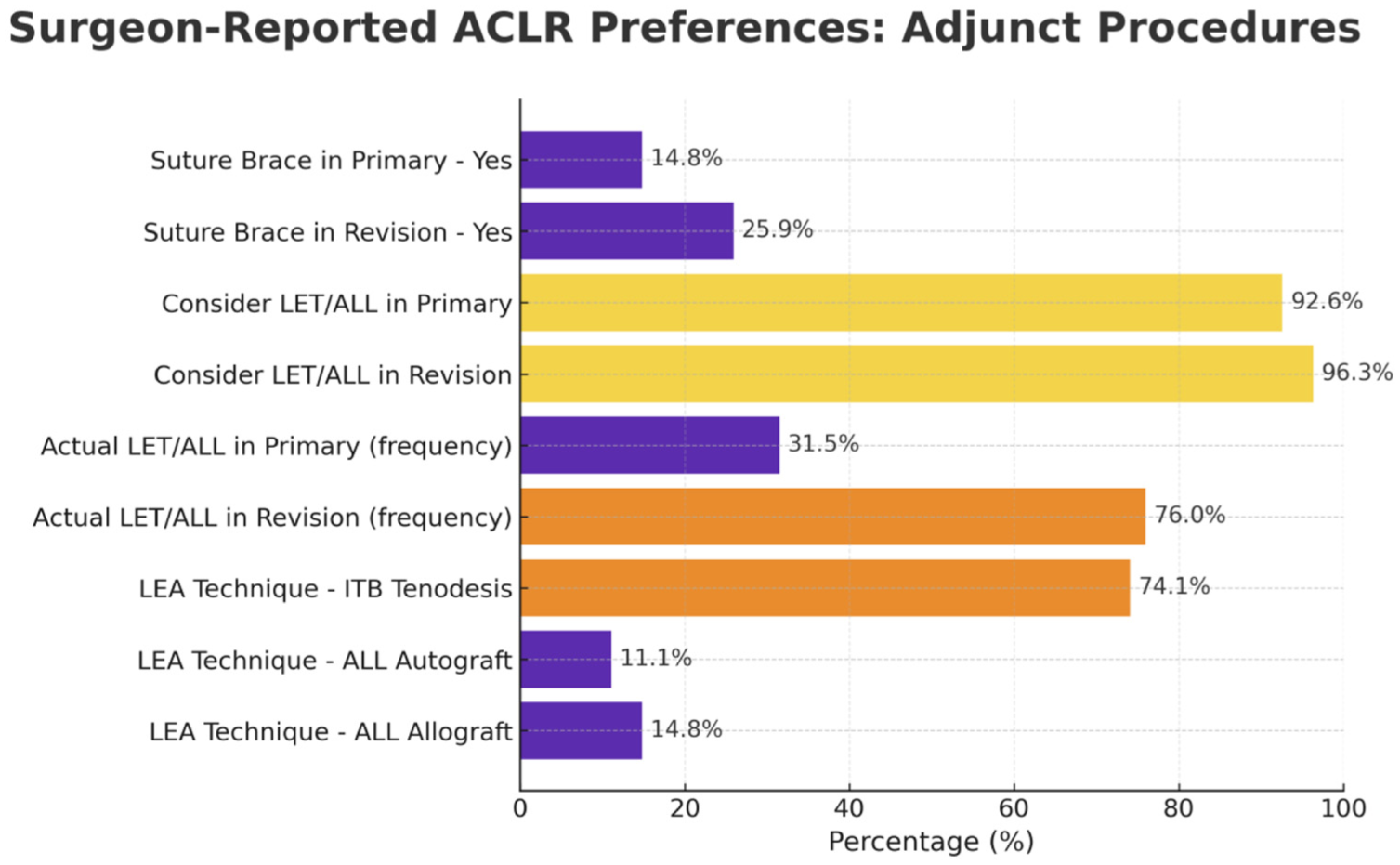
Surgeon-reported preferences for adjunct procedures. Bars reflect reported use of suture brace augmentation, consideration versus actual frequency of lateral extra-articular augmentation (LEA) in primary and revision settings, and preferred techniques.
A series of yes/no questions regarding factors with potential implications for operative planning were also included in the survey. A slight majority (51.9%) of respondents indicated they would not perform LET in primary ACLR for soccer athletes with a posterior tibial slope >13° or for soccer athletes with a concomitant medial meniscal deficiency. Interestingly, 51.9% of surgeons reported not performing LET during primary ACLR in elite/professional soccer athletes, but 85.2% indicated they would perform LET during an ACLR revision in the same demographic.
Recovery and Rehabilitation
For isolated ACLR, 77.8% of surgeons reported prescribing postoperative bracing, with a minimum expected time to return to sport (RTS) of 8.4 months ± 1.1 months. The mean expected RTS duration was reported as 10.1 ± 1.2 months, with the caveat that 92.6% of respondents stated that postoperative functional tests were considered in the RTS decision.
Soccer Athletes
When caring for high-level adolescent soccer athletes indicated for ACLR, survey participants had similar preferences. For a hypothetical male patient <15 years of age or female patient <14 years of age with open physes, the most common graft choice for ACLR was QT autograft (77.8%), followed by HT autograft (18.5%). The final respondent reported not routinely performing such procedures. In elite adult soccer athletes requiring ACLR, more surgeons preferred BPTB autograft (74%) versus QT autograft (22.2%), with HT autograft (3.7%) being the least common, regardless of sex. In ACLR for soccer athletes, femoral tunnel drilling was most frequently performed via an anteromedial portal (59.3%), followed by a 2-incision outside-in approach (25.9%). A small portion of respondents (14.8%) reported a preference for a transtibial approach.
When queried about slope-reduction osteotomies for elite soccer athletes, a majority of surgeons (77.8%) elected not to perform such a procedure for cases with a posterior tibial slope between 15° and 20°. However, once the posterior tibial slope exceeded 20°, a slight majority (51.9%) of respondents stated they would perform an anterior closing wedge osteotomy. Finally, a majority (74%) of the surgeons indicated they would not perform a medial meniscus transplant in the context of a medial meniscus-deficient professional soccer athlete during a revision ACLR.
Discussion
The principal findings of this study are as follows: surgeons who care for MLS and other high-level soccer athletes generally prefer BPTB autografts (~70%) as the primary graft for ACLR across all demographics. QT autografts are also utilized (~22%), but HT autografts are infrequently employed (~4%). In revision cases, QT autografts (~48%) are most common, followed by either BPTB autografts (~26%) or allografts (~11%). Among skeletally immature patients, QT autografts are preferred (~78%). Surgeons report performing LEA procedures in approximately 33% of primary ACLRs and up to 76% of revision cases in the general population, but do so more frequently in professional and high-level soccer athletes, for both index operations (~48%) and revisions (~85%). Anterior closing-wedge osteotomies are uncommon, even in hypothetical patients with a posterior tibial slope >20°.
ACL injury and reinjury rates among elite soccer athletes may inform graft preferences among MLS surgeons. Previous studies investigating the rate of subsequent ipsilateral or contralateral ACL injury after index ACLR in the Union of European Soccer Associations report9,14 rates of 12% to 17.8%, which are higher than those observed in the general population. 39 Although established guidelines exist to inform ACLR, 6 surgeon-reported preferences continue to demonstrate variability, highlighting the influence of training, experience, and practice style.
Among the various considerations in ACLR, graft selection continues to generate debate, owing to the lack of conclusive evidence favoring one option over another, particularly in unique subpopulations such as elite soccer athletes. The 27 MLS-affiliated surgeons who responded to this survey indicated their ideal graft choice is largely consistent, regardless of whether they are treating a high-level soccer athlete or a patient in the general population. Across both high-level athletes and general practice patients, BPTB autograft is chosen 4 times more commonly than QT autograft, with only 1 surgeon indicating they would select HT autograft for a primary ACLR in a skeletally mature individual.
Contemporary evidence from systematic reviews and meta-analyses provides important context for ACL graft preferences among MLS-affiliated surgeons. While multiple studies demonstrate that BPTB, QT, and HT autografts yield comparable patient-reported outcomes, joint laxity, and RTS rates, important differences in graft failure rates exist.7,38,42 BPTP autografts consistently show lower rates of graft failure when compared with HT autografts, particularly in younger patients and high-level athletes, which may account for the graft preferences observed among MLS-affiliated surgeons.29,34
Our results align with the graft preferences reported by National Football League (NFL) orthopaedic surgeons, who nearly unanimously (94%) would choose BPTB autograft for an elite football running back. When treating a 25- or 35-year-old recreational athlete, NFL-affiliated surgeons’ preference for BPTB autografts decreased to 65% and 39%, respectively, with a subsequent increase in the utilization of QT autografts (19% to 25%). 17 The predilection for BTPB autografts is similarly observed among orthopaedic surgeons affiliated with the National Basketball Association (NBA), National Hockey League (NHL), MLS, and United States Olympic team, choosing BPTB on average 70% of the time in index ACLR.13,25
These trends are notably divergent from national trends in ACLR, where HT autografts are mostly utilized. A 2024 meta-analysis by Yang et al 40 reported that HT autografts account for over half of grafts (52%) in the United States, while BPTB autografts account for 43% and QT autografts account for 5%. Internationally, HT autografts for ACLR are strongly preferred, with utilization rates of approximately 60% in Europe and South America and >70% in Asia. 35 Although BPTB has historically been considered the benchmark standard due to its reliable fixation, 2 HT utilization gained popularity in the early 2000s with randomized control trials and meta-analyses citing similar clinical outcomes for BPTB and HT.2,19 The added benefits of reduced anterior knee pain, an established side effect of BPTB surgery, along with less donor site morbidity and retention of the knee extensor mechanism, serve as attractive arguments for HT utilization.2,19,38 The verdict on BPTB versus HT remains uncertain, with some studies reporting higher rates of revision surgery and increased lateral laxity among patients who undergo HT autograft.15,22,40 In contrast, other meta-analyses report equivalent outcomes in these metrics.26,38 There is also the re-emergence of QT grafts within the BPTB versus HT debate. Recent studies demonstrate comparable clinical outcomes among the 3 graft options, with QT grafts exhibiting biomechanical properties equal or superior to those of the other 2 with less donor-site morbidity.1,8,26,27,32,40
The surgeons in this study appear to favor the BPTB autograft, given its proven track record of success across decades of research, demonstrating low rates of revision, predictable graft integration, biomechanical properties, reliable stability, and favorable RTS rates.7,22,30 Furthermore, the growing body of research demonstrating clinical equivalency and diminished donor site morbidity for QT autografts may explain this increased preference,1,8,26,27,32,40 deviating from national standards. 40 In the context of revision surgeries, QT autograft is the most reported choice of graft, with the caveat that this decision depends on the index operation and availability of remaining graft options. The large graft size, lower donor-site morbidity, and biomechanical advantages of QT grafts over BPTB and HT likely contribute to their more frequent use (48%) in ACL revisions. 1,8,26,27,32,40 Interestingly, no respondents reported using HT autografts in the revision setting. The only instance in which ≥1 surgeon chose HT autograft is in the context of a skeletally immature athlete with open physes; however, even in this instance, the frequency of QT was still 4 times that of HT. Of note, no surgeons elected to use BPTB autograft or allograft in this context, as both constructs are generally avoided in younger, skeletally immature patients due to concerns about physeal growth arrest and overgrowth.11,12,21
A commonly debated aspect of ACLR is the role of LEA. LET and ALL reconstruction are LEA techniques used to address persistent anterolateral rotatory instability and may reduce the risk of graft failure in select patients. The frequencies reported by surgeons in our study are generally consistent with previous literature. Respondents indicated they would perform LEA in approximately 33% of primary ACLR cases, with a preference for ITB tenodesis (74%) over ALL reconstruction (~26%). Lewis et al 24 reported similar trends, noting a likelihood of LEA utilization ranging from 10% to 23% depending on practice volume, with 27.5% of respondents favoring ALL reconstruction and the remainder selecting LET techniques. In the revision setting, an even larger proportion of our participants (76%) indicated they would perform LEA. When specifically considering MLS athletes, respondents reported performing LEA in 46% of index ACLRs and 85% of revisions. This result aligns with the overwhelming majority (84%) of NFL surgeons who prefer adding LEA to an index ACLR in an elite football running back when specific clinical indications are met. 17 The frequencies of LEA utilization in revision ACLRs do not appear to have been directly reported. However, a recent meta-analysis by Jones et al 20 found that in 52% of included studies, revision surgery alone was cited as an indication for LET. While a positive pivot shift is the most common clinical indication, participation in general or competitive sport is also noted to be an indication for LEA. 20 Given that return to high-level sport and frequent engagement in pivoting activities are associated with increased graft rupture risk, 5 MLS athletes, who routinely perform pivoting, cutting, and jumping, are excellent candidates for LEA to enhance rotational stability and reduce ACL graft loads. 16
Additionally, this study investigated the role of slope reduction osteotomies in revision ACLR. Interestingly, the majority of survey respondents (81%) indicated they would not perform a slope-reduction osteotomy in a revision ACLR for an elite soccer athlete with a posterior tibial slope of 15° to 20°. Once the posterior tibial slope exceeds 20°, half of the participants indicated the need for surgery. Although historically reserved for rerevisions, recent literature proposes a favorable safety and complication profile, and improved patient-reported outcomes with slope-reducing osteotomies in first revision cases23,33,36 with posterior tibial slope >12°. It appears that most surgeons remain conservative in their application of these more recently described procedures in professional and high-level athletes.
Limitations
While this study provides an intriguing perspective on the management of ACL tears from surgeons who care for high-level MLS athletes, it has notable limitations. First, the findings of this study are entirely observational and do not aim to comment on the scientific superiority of any given technique. The combined opinions of renowned experts within the field may display current trends in ACLR management; however, these findings are subject to response bias from a small cohort of surgeons who elected to participate in this survey. Second, the variation in responses to the clinical decision-making scenarios in this survey may be secondary to training bias, which was not explicitly controlled for in this investigation. Third, this cohort represents preferences from MLS-affiliated surgeons and may not be representative of ACL injury management in other geographic regions or across other professional sports leagues. Moreover, given the focus of the present analysis on MLS athletes, differences in sex-specific graft preferences across the skeletally mature general population were not explicitly interrogated. With the relatively small number of professional-athlete injuries and high stakes surrounding RTS, opportunities for formal experimental trials to establish treatment superiority are limited, and observational studies may therefore represent the most feasible approach.
Conclusion
Among orthopaedic surgeons who care for MLS and other high-level athletes, the BPTB autograft is the most preferred graft when performing primary ACLR. QT autografts are favored over HT autografts in primary reconstruction and are the most common choice of graft in revision surgery. HT autografts are utilized infrequently in index operations and not preferred in revisions. Surgeons indicated LET or ALL reconstruction in one-third of primary and 75% of revision ACLRs within the general population. LEA procedures were performed more frequently among professional soccer athletes, occurring in 46% of index operations and 85% of revisions. Tibial slope-reducing osteotomies, despite gaining popularity in the literature, remained an uncommonly reported procedure in the management of ACL injuries in elite soccer athletes. Surgeons generally treated professional and nonprofessional injuries similarly, suggesting that the preferences discussed in this study may be applicable to a broad patient population undergoing ACLR.
Footnotes
Appendix
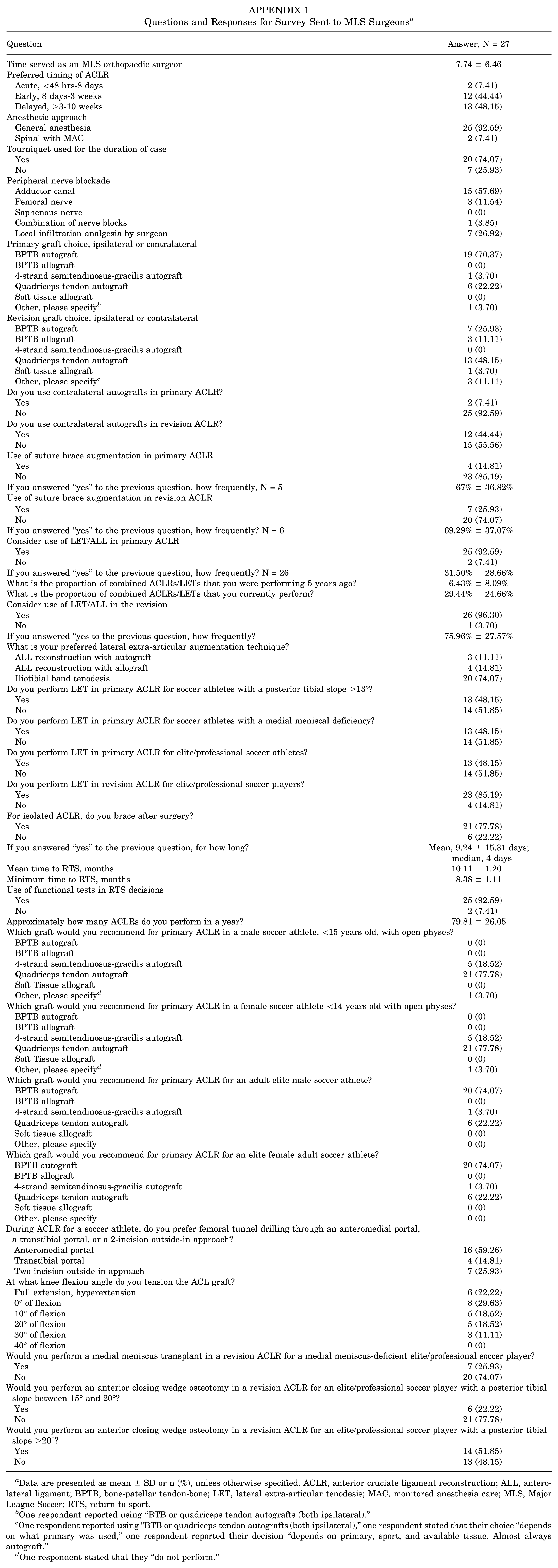
Questions and Responses for Survey Sent to MLS Surgeons a
| Question | Answer, N = 27 |
|---|---|
| Time served as an MLS orthopaedic surgeon | 7.74 ± 6.46 |
| Preferred timing of ACLR | |
| Acute, <48 hrs-8 days | 2 (7.41) |
| Early, 8 days-3 weeks | 12 (44.44) |
| Delayed, >3-10 weeks | 13 (48.15) |
| Anesthetic approach | |
| General anesthesia | 25 (92.59) |
| Spinal with MAC | 2 (7.41) |
| Tourniquet used for the duration of case | |
| Yes | 20 (74.07) |
| No | 7 (25.93) |
| Peripheral nerve blockade | |
| Adductor canal | 15 (57.69) |
| Femoral nerve | 3 (11.54) |
| Saphenous nerve | 0 (0) |
| Combination of nerve blocks | 1 (3.85) |
| Local infiltration analgesia by surgeon | 7 (26.92) |
| Primary graft choice, ipsilateral or contralateral | |
| BPTB autograft | 19 (70.37) |
| BPTB allograft | 0 (0) |
| 4-strand semitendinosus-gracilis autograft | 1 (3.70) |
| Quadriceps tendon autograft | 6 (22.22) |
| Soft tissue allograft | 0 (0) |
| Other, please specify b | 1 (3.70) |
| Revision graft choice, ipsilateral or contralateral | |
| BPTB autograft | 7 (25.93) |
| BPTB allograft | 3 (11.11) |
| 4-strand semitendinosus-gracilis autograft | 0 (0) |
| Quadriceps tendon autograft | 13 (48.15) |
| Soft tissue allograft | 1 (3.70) |
| Other, please specify c | 3 (11.11) |
| Do you use contralateral autografts in primary ACLR? | |
| Yes | 2 (7.41) |
| No | 25 (92.59) |
| Do you use contralateral autografts in revision ACLR? | |
| Yes | 12 (44.44) |
| No | 15 (55.56) |
| Use of suture brace augmentation in primary ACLR | |
| Yes | 4 (14.81) |
| No | 23 (85.19) |
| If you answered “yes” to the previous question, how frequently, N = 5 | 67% ± 36.82% |
| Use of suture brace augmentation in revision ACLR | |
| Yes | 7 (25.93) |
| No | 20 (74.07) |
| If you answered “yes” to the previous question, how frequently? N = 6 | 69.29% ± 37.07% |
| Consider use of LET/ALL in primary ACLR | |
| Yes | 25 (92.59) |
| No | 2 (7.41) |
| If you answered “yes” to the previous question, how frequently? N = 26 | 31.50% ± 28.66% |
| What is the proportion of combined ACLRs/LETs that you were performing 5 years ago? | 6.43% ± 8.09% |
| What is the proportion of combined ACLRs/LETs that you currently perform? | 29.44% ± 24.66% |
| Consider use of LET/ALL in the revision | |
| Yes | 26 (96.30) |
| No | 1 (3.70) |
| If you answered “yes to the previous question, how frequently? | 75.96% ± 27.57% |
| What is your preferred lateral extra-articular augmentation technique? | |
| ALL reconstruction with autograft | 3 (11.11) |
| ALL reconstruction with allograft | 4 (14.81) |
| Iliotibial band tenodesis | 20 (74.07) |
| Do you perform LET in primary ACLR for soccer athletes with a posterior tibial slope >13°? | |
| Yes | 13 (48.15) |
| No | 14 (51.85) |
| Do you perform LET in primary ACLR for soccer athletes with a medial meniscal deficiency? | |
| Yes | 13 (48.15) |
| No | 14 (51.85) |
| Do you perform LET in primary ACLR for elite/professional soccer athletes? | |
| Yes | 13 (48.15) |
| No | 14 (51.85) |
| Do you perform LET in revision ACLR for elite/professional soccer players? | |
| Yes | 23 (85.19) |
| No | 4 (14.81) |
| For isolated ACLR, do you brace after surgery? | |
| Yes | 21 (77.78) |
| No | 6 (22.22) |
| If you answered “yes” to the previous question, for how long? | Mean, 9.24 ± 15.31 days; median, 4 days |
| Mean time to RTS, months | 10.11 ± 1.20 |
| Minimum time to RTS, months | 8.38 ± 1.11 |
| Use of functional tests in RTS decisions | |
| Yes | 25 (92.59) |
| No | 2 (7.41) |
| Approximately how many ACLRs do you perform in a year? | 79.81 ± 26.05 |
| Which graft would you recommend for primary ACLR in a male soccer athlete, <15 years old, with open physes? | |
| BPTB autograft | 0 (0) |
| BPTB allograft | 0 (0) |
| 4-strand semitendinosus-gracilis autograft | 5 (18.52) |
| Quadriceps tendon autograft | 21 (77.78) |
| Soft Tissue allograft | 0 (0) |
| Other, please specify d | 1 (3.70) |
| Which graft would you recommend for primary ACLR in a female soccer athlete <14 years old with open physes? | |
| BPTB autograft | 0 (0) |
| BPTB allograft | 0 (0) |
| 4-strand semitendinosus-gracilis autograft | 5 (18.52) |
| Quadriceps tendon autograft | 21 (77.78) |
| Soft Tissue allograft | 0 (0) |
| Other, please specify d | 1 (3.70) |
| Which graft would you recommend for primary ACLR for an adult elite male soccer athlete? | |
| BPTB autograft | 20 (74.07) |
| BPTB allograft | 0 (0) |
| 4-strand semitendinosus-gracilis autograft | 1 (3.70) |
| Quadriceps tendon autograft | 6 (22.22) |
| Soft tissue allograft | 0 (0) |
| Other, please specify | 0 (0) |
| Which graft would you recommend for primary ACLR for an elite female adult soccer athlete? | |
| BPTB autograft | 20 (74.07) |
| BPTB allograft | 0 (0) |
| 4-strand semitendinosus-gracilis autograft | 1 (3.70) |
| Quadriceps tendon autograft | 6 (22.22) |
| Soft tissue allograft | 0 (0) |
| Other, please specify | 0 (0) |
| During ACLR for a soccer athlete, do you prefer femoral tunnel drilling through an anteromedial portal, a transtibial portal, or a 2-incision outside-in approach? | |
| Anteromedial portal | 16 (59.26) |
| Transtibial portal | 4 (14.81) |
| Two-incision outside-in approach | 7 (25.93) |
| At what knee flexion angle do you tension the ACL graft? | |
| Full extension, hyperextension | 6 (22.22) |
| 0° of flexion | 8 (29.63) |
| 10° of flexion | 5 (18.52) |
| 20° of flexion | 5 (18.52) |
| 30° of flexion | 3 (11.11) |
| 40° of flexion | 0 (0) |
| Would you perform a medial meniscus transplant in a revision ACLR for a medial meniscus-deficient elite/professional soccer player? | |
| Yes | 7 (25.93) |
| No | 20 (74.07) |
| Would you perform an anterior closing wedge osteotomy in a revision ACLR for an elite/professional soccer player with a posterior tibial slope between 15° and 20°? | |
| Yes | 6 (22.22) |
| No | 21 (77.78) |
| Would you perform an anterior closing wedge osteotomy in a revision ACLR for an elite/professional soccer player with a posterior tibial slope >20°? | |
| Yes | 14 (51.85) |
| No | 13 (48.15) |
Data are presented as mean ± SD or n (%), unless otherwise specified. ACLR, anterior cruciate ligament reconstruction; ALL, anterolateral ligament; BPTB, bone-patellar tendon-bone; LET, lateral extra-articular tenodesis; MAC, monitored anesthesia care; MLS, Major League Soccer; RTS, return to sport.
One respondent reported using “BTB or quadriceps tendon autografts (both ipsilateral).”
One respondent reported using “BTB or quadriceps tendon autografts (both ipsilateral),” one respondent stated that their choice “depends on what primary was used,” one respondent reported their decision “depends on primary, sport, and available tissue. Almost always autograft.”
One respondent stated that they “do not perform.”
Final revision submitted March 23, 2025; accepted March 30, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for the present study.