
Abstract
Background:
An adjunctive infiltration between popliteal artery and capsule of the posterior knee (iPACK) block—an infiltration between the popliteal artery and posterior knee capsule—has been used in knee surgery to address posterior knee pain, complementing the anterior and medial sensory coverage of an adductor canal block (ACB). Its benefit in all-inside anterior cruciate ligament reconstruction (ACL-R) using quadriceps tendon (QT) autograft remains uncertain.
Purpose:
To compare acute postoperative pain, opioid consumption, and 6-week knee range of motion between patients receiving continuous ACB alone and continuous ACB plus a single-shot iPACK block.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
Patients undergoing primary all-inside ACL-R with QT autograft were randomized to either continuous ACB with placebo skin wheal (ACB group) or continuous ACB with iPACK (ACB-iPACK group). Demographic and surgical data were collected prospectively. The primary outcome was visual analog scale (VAS) pain scores during the first 72 postoperative hours. Secondary outcomes included opioid use (morphine milligram equivalents), achievement of full knee extension, and difference in maximal flexion between the surgical and nonsurgical limb at 6 weeks.
Results:
A total of 71 patients were analyzed (ACB, n = 33; ACB-iPACK, n = 38), with no significant group differences in baseline characteristics. Median VAS scores at discharge were significantly lower in the ACB-iPACK group (20 mm) versus the ACB group (32.5 mm) (P = .049). No further differences occurred between 12 and 72 hours postoperatively. Perioperative and postoperative opioid consumption did not differ between groups (perioperative, P = .52; postoperative, P = .47 to ≥.99). Rates of achieving full extension were similar. At 6 weeks, the difference in knee flexion between limbs was significantly smaller in the ACB-iPACK group (37.7°) compared with the ACB group (47.6°) (mean difference, 9.9°; P = .02). No perioperative regional anesthesia complications occurred.
Conclusion:
Adding an iPACK block to continuous ACB for all-inside ACL-R with QT autograft provided a slight reduction in pain at discharge (VAS difference, 12.5 mm) and improved knee flexion at 6 weeks. However, pain scores and opioid use beyond the immediate postoperative period were not significantly different between groups. These findings may help guide patient counseling regarding the expected benefits of incorporating an iPACK block in this surgical setting.
Registration:
NCT05498870 (ClinicalTrials.gov identifier).
Keywords
Anterior cruciate ligament (ACL) reconstruction (ACL-R) is one of the most common orthopaedic knee procedures, with an estimated 100,000 to 200,000 cases occurring each year in the United States alone. 5 ACL-R is most commonly performed on an outpatient basis, with the use of a multimodal analgesic regimen that incorporates regional anesthesia.15,21 While femoral nerve blocks (FNBs) were used historically, the adductor canal block (ACB) has emerged as a standard of care, as it has consistently been demonstrated to provide noninferior analgesia in comparison with FNB, while sparing quadriceps motor function.1,11 In comparison with an FNB, an ACB is performed more distally in the thigh, providing a sensory blockade of the saphenous nerve and nerve to the vastus medialis, providing effective analgesia to the anterior and medial compartments of the knee. 26 Both modalities fail to adequately address painful stimuli from the posterior aspect of the knee, however. 26
The performance of ACL-R in an outpatient setting and effective early postoperative rehabilitation is critically reliant on adequate pain control to achieve appropriate patient satisfaction, same-day discharge, and early mobilization for functional recovery. Therefore, various adjunctive modalities have been utilized to address painful stimuli from the posterior aspect of the knee, including sciatic nerve blocks (SNBs), selective tibial nerve blocks (TNB), and the adjunctive infiltration between popliteal artery and capsule of the posterior knee (iPACK) block. In comparison with SNB and TNB, the iPACK block is motor sparing and provides sensory-specific regional anesthetic coverage to the posterior knee by blocking sensory branches of the tibial, obturator, and common fibular nerves that form the popliteal plexus. 25 In the arthroplasty literature, the use of ACB and iPACK (ACB-iPACK) concomitantly has been demonstrated to result in improved subjective pain score, a shorter length of stay, and reduced mobilization latency outcomes.8,10,19,24
Comparisons of ACB with an adjunctive iPACK block in comparison with ACB alone or with other regional anesthesia techniques for ACL-R, however, have not been fully explored.2,6,20 Therefore, the primary objective of this current study was to perform a randomized controlled trial directly comparing visual analog scale (VAS) pain scores, opioid consumption, and knee range of motion (ROM) at 6 weeks postoperatively with the use of ACB-iPACK versus ACB alone in patients undergoing primary ACL-R with quadriceps tendon (QT) autograft utilizing an all-inside technique. Specifically, we hypothesized that patients receiving ACB-iPACK would report lower subjective pain scores (primary study outcome of interest) and demonstrate reduced total opioid consumption and improved early knee ROM (secondary study outcomes of interest) in comparison with patients receiving ACB alone.
Methods
Study Design
This prospective, single-center, double-blinded, randomized controlled trial was approved by the institutional review board at the Medical University of South Carolina. Eligible patients included those aged ≥12 years undergoing primary ACL-R with QT autograft. Exclusion criteria included patients with medical contraindication to receiving regional anesthesia, patients undergoing multiligamentous knee reconstruction surgery, preexisting infection at the injury site, chronic opioid treatments, preexisting sensory and/or motor deficit in the operative extremity, revision ACL-R, pregnant and/or lactating women, or a weight <40 kg. Patient enrollment and initial data collection took place at the Medical University of South Carolina. Subsequent data were collected via paper diary or secure text messaging system (Twilio) and in the orthopaedic clinic during routine, standard postoperative follow-up visits. Patient enrollment began August 25, 2022, and the study was completed on August 14, 2023. For participants <18 years of age, written informed consent was obtained from their parent or legal guardian, and assent was obtained from the participant herself or himself. Adults aged ≥18 provided written informed consent for themselves. After consent was obtained and patients were confirmed to meet eligibility criteria for inclusion, study participants were assigned a study ID in sequential order (1-82), and randomized to either ACB or ACB-iPACK by a study team member using the randomization function in REDCap (Vanderbilt University).
Randomization
Participants were randomized in a 1:1 ratio to receive either ACB alone or ACB with iPACK using the randomization module in REDCap. The allocation sequence was generated before study initiation by a study biostatistician using a computer-generated randomization schedule with stratification by biological sex to ensure balanced distribution between treatment arms. Block randomization was used to maintain approximate group balance throughout enrollment. The randomization schedule was uploaded into the REDCap randomization module, which automatically assigned treatment allocation after participant enrollment. Allocation concealment was maintained within REDCap, and study personnel responsible for enrolling participants did not have access to the underlying allocation sequence.
Blinding
Patients were blinded to group assignment. Postoperative patient-reported outcomes collected via text messaging or paper surveys were recorded electronically and did not indicate treatment allocation to study personnel involved in data handling. ROM measurements obtained during routine postoperative clinic visits were performed by clinic staff who were not involved in the study design or randomization process and were not informed of the patient's treatment allocation. Data analysis was conducted using deidentified group labels to minimize potential analytic bias.
Preoperative Anesthetic Care
Patients >70 kg, 45 to 70 kg, and < 45 kg received 1 g, 650 mg, and 500 mg of oral acetaminophen, respectively. One to 2 mg of midazolam and ≤20 mcg of dexmedetomidine were administered for preprocedure anxiolysis. With ultrasound guidance, all participants received an ACB consisting of a single injection of 20 mL of 0.25% ropivacaine followed by the placement of a continuous nerve block catheter. The ACB was administered via a continuous nerve block catheter with a 650-mL reservoir infusing 0.2% ropivacaine at 4 mL/hour for patients weighing <60 kg and 6 mL/hour for patients ≥60 kg. The infusion was delivered using a standardized institutional protocol. The pump also included a patient-controlled analgesic function allowing an additional 5-mL bolus with a 1-hour lockout interval. Under standard basal infusion conditions, the reservoir volume allowed for approximately 72 hours of continuous analgesia. Those randomized to ACB-iPACK received an additional injection of 20 mL of 0.25% ropivacaine between the popliteal artery and the posterior aspect of the capsule of the knee. To maintain blinding to the patient and surgeon, participants randomized to ACB received a skin wheal at the site of the iPACK block. All regional anesthetic procedures were performed by board-certified anesthesiologists (C.L.B., C.D.W., C.F.P.) with extensive experience in regional anesthesia. The sonographic anatomy of these nerve blocks can be seen in Figure 1.
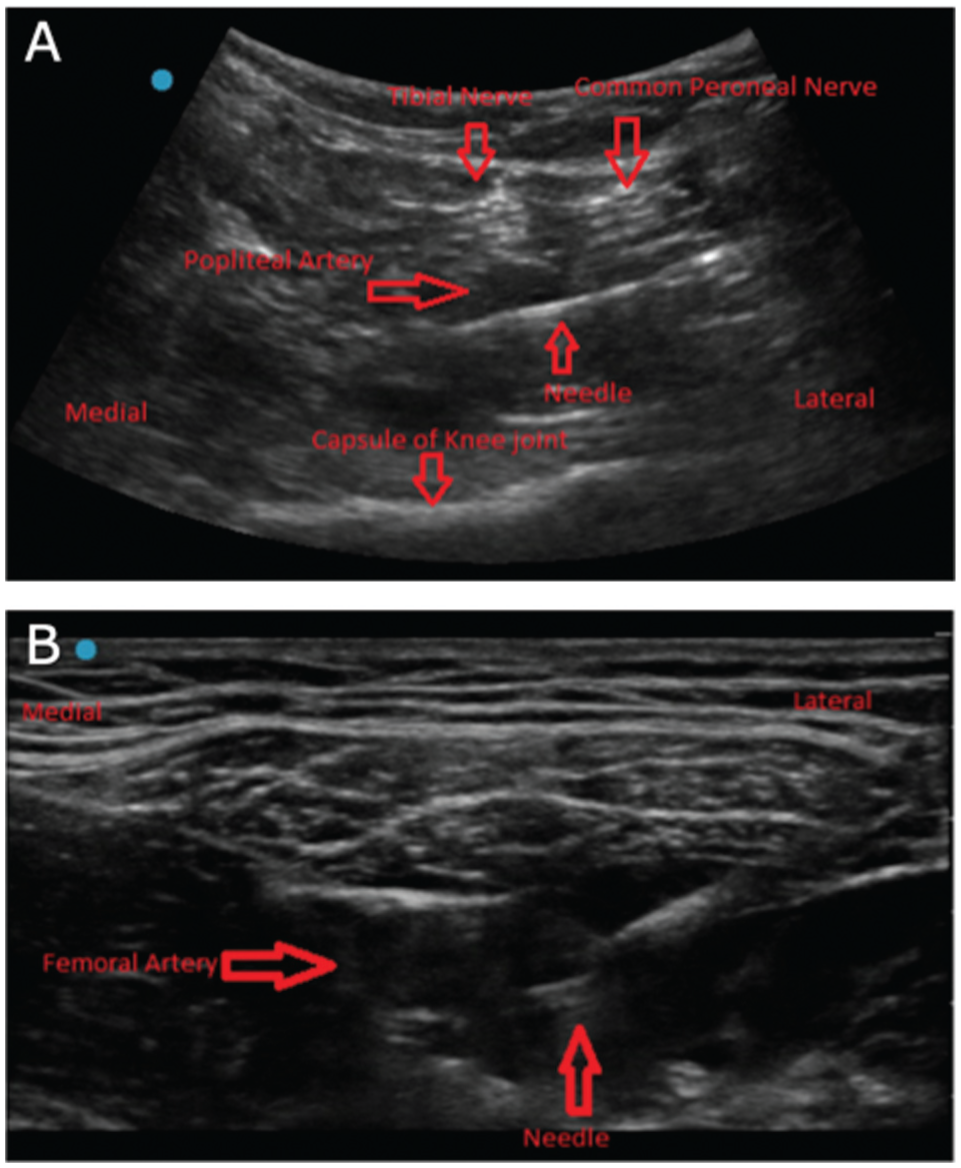
Sonographic anatomy of injection site for (A) the infiltration between popliteal artery and capsule of the posterior knee block (iPACK) block and (B) the adductor canal block. The iPACK block in this image is performed from the lateral to medial approach in the similar manner to which the popliteal nerve block is performed with the transducer placed in the popliteal fossa at the crease of the knee joint. The sciatic nerve has bifurcated into the tibial and common peroneal nerves at this location and the local anesthetic distribution can be seen a distance away from these nerves to prevent motor block. The iPACK block has also been described in the literature via a medial to lateral approach (not pictured). The adductor canal block is performed midthigh from the lateral to medial approach with the needle transversing through the sartorius and then the fascia lata and fascia iliaca before entering the adductor canal.
Intraoperative Anesthetic Care
All patients received a general anesthetic with a propofol induction and total intravenous anesthesia with propofol. Dexamethasone 0.1 mg/kg (max dose, 10 mg) and ketamine 0.5 mg/kg were given before incision. Hydromorphone was given as an intraoperative opioid based on the clinical judgment of the anesthesiologist. Before emergence, ketorolac 30 mg (15 mg if <60 kg) was given, as well as 4 mg of ondansetron for postoperative nausea and vomiting prophylaxis.
Surgical Technique
All patients underwent an all-inside ACL-R with QT autograft by 1 of 2 fellowship-trained orthopaedic sports medicine surgeons (W.M.P., H.S.S.) with extensive experience performing ACL-R. All QT autografts were harvested utilizing a standardized graft harvesting system (QuadPro Tendon Harvester; Arthrex Inc). Femoral and tibial tunnel reaming was performed in outside-in fashion using a retrograde reamer (FlipCutter II; Arthrex Inc). Intraoperatively, meniscal pathology and chondral pathology were treated at the discretion of the operating surgeon. Meniscal tears were treated with either repair or partial meniscectomy. When present, unstable and symptomatic partial-thickness chondral defects were treated with chondroplasty alone. In certain patients determined preoperatively to be at high risk for graft rupture postoperatively, a lateral extra-articular tenodesis (LET) was performed at the operating surgeon's discretion as an adjunctive procedure.
Postoperative Anesthetic and Surgical Care
In the postanesthesia care unit (PACU), participants were given intravenous hydromorphone and oxycodone as needed for pain. Patients who underwent isolated ACL-R or who underwent concomitant partial meniscectomy and/or chondroplasty were not placed in a brace postoperatively. Patients who underwent meniscal repair were placed in a hinged, ROM knee brace (X-ROM; Enovis) and instructed to keep the brace locked in extension while weightbearing, while ROM was permitted between 10° of hyperextension and flexion to 90° until 6 weeks postoperatively. Physical therapy prescription and rehabilitation protocols were provided at surgery discharge. The prescribed postoperative oral medication regimen was based on age and weight, per institutional protocol. Participants aged 12 to 18 and <70 kg were prescribed acetaminophen 650 mg q8h, naproxen 250 mg q8h, oxycodone 5 mg q4h as needed for pain, and aspirin 81 mg daily for deep vein thrombosis (DVT) prophylaxis. Participants ≥18 or older or >70 kg were prescribed acetaminophen 1000 mg q8h, naproxen 500 mg twice daily, oxycodone 5 to 10 mg q4h as needed for pain, and aspirin 325 mg daily for DVT prophylaxis.
Outcomes
Prospectively collected data included patient demographics, intraoperative surgical details (meniscal and cartilage treatment, performance of an LET, or other procedures), and perioperative outcomes of interest (pain rating using a VAS before discharge, opioid consumption while under care at the surgical center [intraoperative opioid administration and PACU opioid administration], PACU duration and time of discharge, and ROM at 2- and 6-week postoperative clinic follow-up visits). Intraoperative and postoperative opioids were converted to intravenous morphine milligram equivalents (MMEs) for comparison. Patient-reported data consisted of VAS pain ratings through 72 hours postoperatively and pain medications taken through 72 hours postoperatively, as stated previously.
Before discharge from the outpatient surgery center, participants were queried regarding their current pain score using a VAS from 0 to 100, with 0 being no pain and 100 being the worst pain possible. VAS measurements were taken by having patients mark on a 100-mm line (0 mm = no pain and 100 mm = worst pain). Beginning on postoperative day (POD) 1, extending through POD 3, participants were sent a text message twice daily that included a survey link by secure server (Twilio). 16 The survey asked participants to report their mean, highest (worst), and lowest (best) pain scores using a VAS, as well as to report any pain medications taken. Participants were asked to report all pain medications taken since the previous survey, including medication name and dose when available. Data recorded were housed in the participants' secure electronic data collection chart. Paper copies were given to participants who were unable or unwilling to receive text messages. Study team members would then call and have them report their responses. At the participants’ standard, routine 2- and 6-week postoperative follow-up clinic appointments, the operating surgeon recorded knee ROM, as measured with a goniometer. Postoperative complications were also recorded and included any event requiring medical evaluation or intervention during the postoperative follow-up period.
Statistical Analysis
Randomization was stratified on biological sex to ensure similar distributions of male and female participants in each treatment arm. An a priori power analysis using PASS (NCSS LLC) found n = 35 patients per treatment arm (70 total), with ≥3 measures of pain, provided 80% power to detect a difference in pain score of 20 mm at significance level α = .01 (Bonferroni corrected for 4 comparisons) and assuming a compound symmetric covariance structure with a conservative 30-mm SD and correlation within patient was ρ = 0.33. The study enrolled 41 patients (82 total) in each arm to allow for up to 15% attrition.
Descriptive statistics for patient demographics and surgical characteristics were separated by treatment arm. Categorical variables were measured as a number and percentage and further evaluated using chi-square or Fisher exact tests. Continuous variables were reported as either mean ± SD or median (IQR), and further evaluated using 2-sample t tests or Wilcoxon rank-sum tests.
Mean pain was evaluated using a series of linear mixed models (LMM). Models included fixed effects for preoperative pain score, block type, postsurgical time, and the interaction between block type and postoperative time. A random patient effect accounted for the correlation between pain scores collected on the same patient over time. The effect of postsurgical time on patient-reported pain was not linear, and thus, time was included as a categorical variable. The difference in patient-reported pain between block types for each postoperative time frame was evaluated using a series of linear contrasts. A Bonferroni adjustment was applied to control the type 1 error.
Secondary outcomes included postoperative opioid consumption over time, ROM, and terminal knee extension. Postoperative opioid consumption was determined at POD 0 after 12 PM, POD 1 before 12 PM and after 12 PM, and POD 2 before 12 PM and after 12 PM. Postoperative ROM, as assessed by the operating surgeon, was assessed based on (1) maximal flexion in the surgical knee relative to the healthy knee and (2) the ability to achieve full knee extension at the 2- and 6-week follow-up visits. Associations between postsurgery opioid consumption and maximal flexion by block type were evaluated using LMM, as previously described. Similar to the model for the primary outcome of interest, the model for opioid consumption included fixed effects for block type, time, the interaction between block type and time, and in-hospital opioid consumption (intraoperative and PACU). The effect of postsurgical time on opioid consumption was not linear, and thus time was included as a categorical variable. The LMM model of maximal knee flexion included fixed effects for block type, postoperative visit number (2- or 6-week postoperative clinic appointment), healthy versus surgical knee, and interactions between block type. The associations between the ability to achieve full extension with block type (continous adductor canal block alone vs continuous ACB combined with concomitant iPACK block) were evaluated using a generalized LMM (GLMM) approach using a logit link. The GLMM model included fixed effects for block type, time, the interaction between block type and time, and whether meniscal repair was performed.
Approximately 17% of observations for both primary and secondary outcomes were absent. Multiple imputation with 10 imputations was used to evaluate missing outcome values before all analyses, and results are reported based on the pooled estimates across imputations. Multiple imputation was performed under the assumption that data were missing at random. Patterns of missingness were explored and did not suggest a systematic relationship with outcome values. Additionally, sensitivity analyses demonstrated consistent results, supporting the robustness of the findings. Because of the absence of postdischarge data, as mentioned above, a post hoc analysis of in-hospital data was performed. This included VAS pain score at discharge from PACU and in-hospital opioid consumption (intraoperative, PACU, and intraoperative and PACU combined). Differences in pain at discharge and in-hospital opioid use were evaluated using Wilcoxon rank-sum test. As a sensitivity analysis, a complete case analysis was conducted, and the results were compared with the imputed data. All analyses were conducted in SAS Version 9.4 (SAS Institute).
Results
This study's CONSORT (Consolidated Standards of Reporting Trials) flow diagram is depicted in Figure 2. Of the 83 patients who consented to study enrollment, 1 patient was excluded before randomization because of incorrect surgery posting. Therefore, 82 patients were assigned to a study group (ACB, n = 41; ACB-iPACK, n = 41). Patient demographics and surgical characteristics by study group are reported in Table 1. No statistically significant differences existed between study groups regarding any demographic or surgical characteristics. In the ACB-iPACK arm (n = 41), 2 patients were excluded from the final analysis because of a perioperative decision to defer ACL-R. One patient was excluded as a result of the National Clinical Trial (NCT) number's not being available upon enrollment. Of the 38 patients available for analysis, 9 completed ≥1, but not all, postoperative outcome assessments. For these patients, their completed data were still used for analysis. In the ACB arm, 2 patients were excluded from analysis as a result of a perioperative decision to defer ACL-R; 5 patients did not complete postoperative follow-up, and 1 patient underwent ACL-R with bone-tendon-bone (BTB) autograft (the patient was inappropriately enrolled and randomized). Of the 33 patients available for analysis, 10 completed ≥1, but not all, postoperative outcome assessments. For these patients, their completed data were still used for analysis.
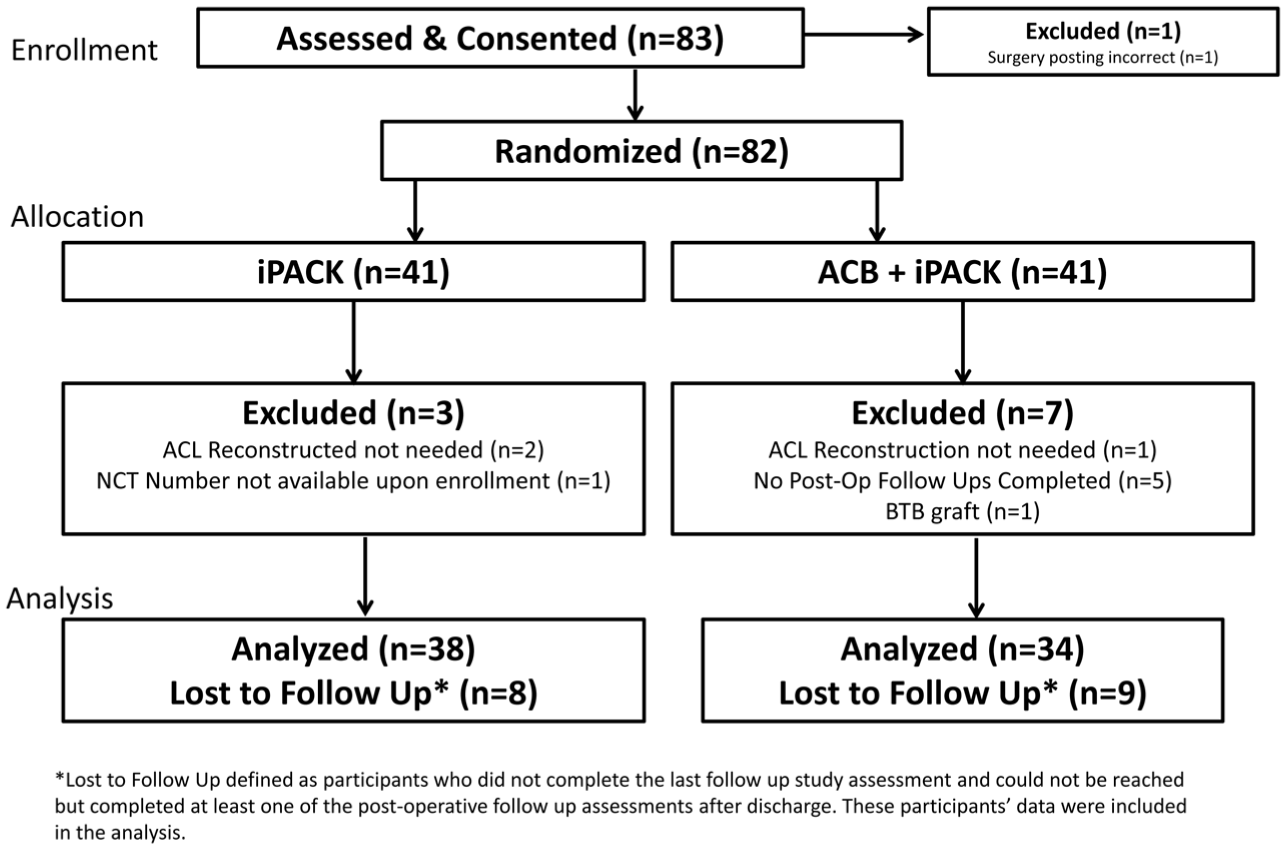
CONSORT (Consolidated Standards of Reporting Trials) flow diagram. *Lost to follow-up is defined as participants who did not complete the last follow-up study assessment and could not be reached but completed ≥1 of the postoperative follow-up assessments after discharge. These participants' data were included in the analysis. ACB, adductor canal block; ACL, anterior cruciate ligament; BTB, bone-tendon-bone; iPACK, infiltration between popliteal artery and capsule of the posterior knee block; NCT, National Clinical Trial.
Patient and Procedural Characteristics by Block Type a
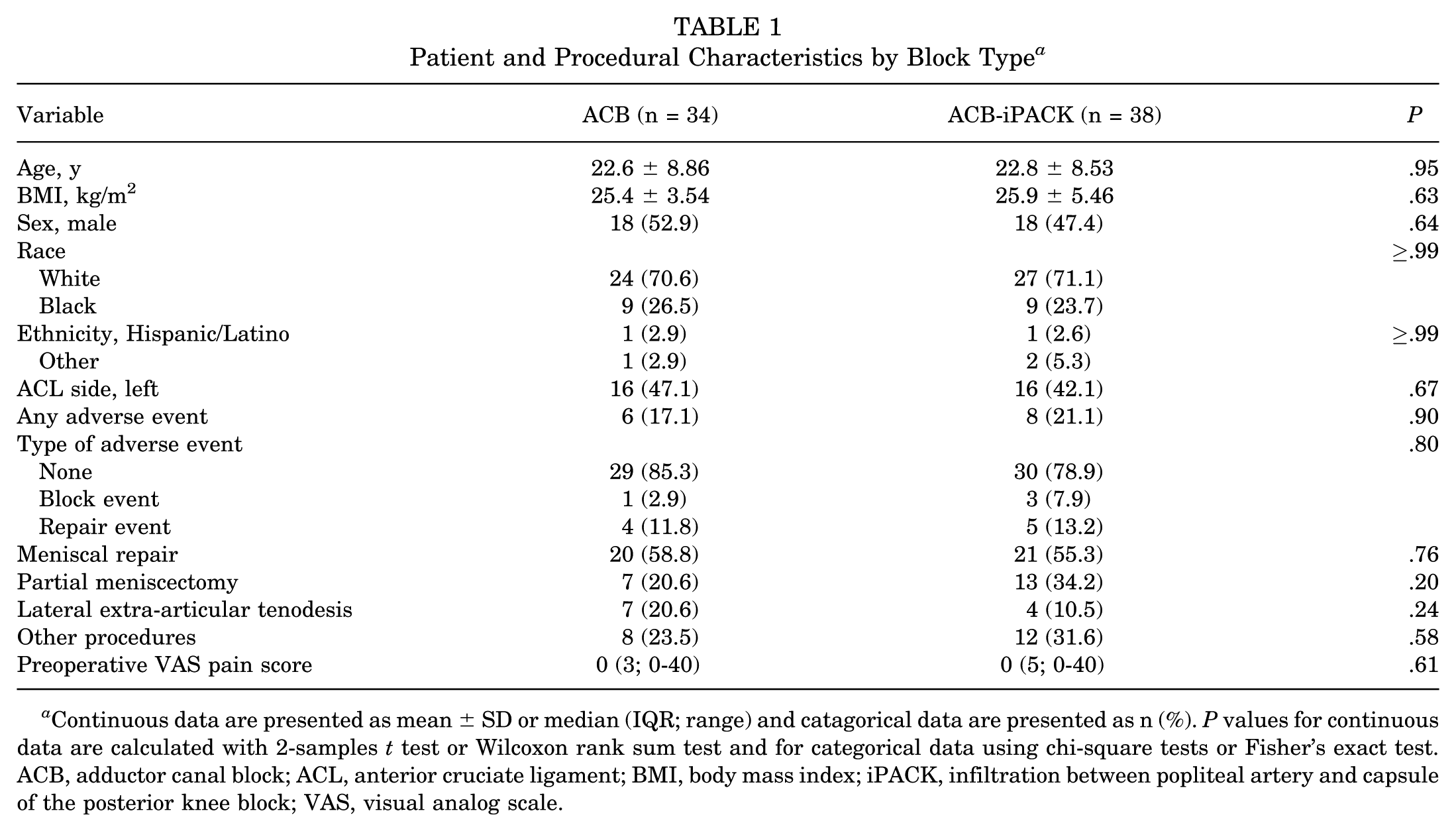
Continuous data are presented as mean ± SD or median (IQR; range) and catagorical data are presented as n (%). P values for continuous data are calculated with 2-samples t test or Wilcoxon rank sum test and for categorical data using chi-square tests or Fisher's exact test. ACB, adductor canal block; ACL, anterior cruciate ligament; BMI, body mass index; iPACK, infiltration between popliteal artery and capsule of the posterior knee block; VAS, visual analog scale.
Postoperative Pain
Reported pain at discharge differed significantly between the ACB-iPACK and ACB groups, with median VAS pain scores of 20 mm (IQR = 51.0 mm) and 32.5 mm (IQR = 40.0 mm), respectively (P = .049) (Table 2). Figure 3 depicts VAS pain scores at discharge for each treatment group. Mean patient-reported pain at follow-up between 12 and 72 hours postoperatively was higher for ACB-iPACK compared with ACB at all intervals; however, these differences were not significant after adjusting for multiple testing (Table 3). Mean pain scores for each postoperative time interval relative to the group are depicted in Figure 4. A sensitivity analysis based on patients who completed data collection fully was also conducted, with no changes in outcome.
In-Hospital Outcomes per Period by Block Type a
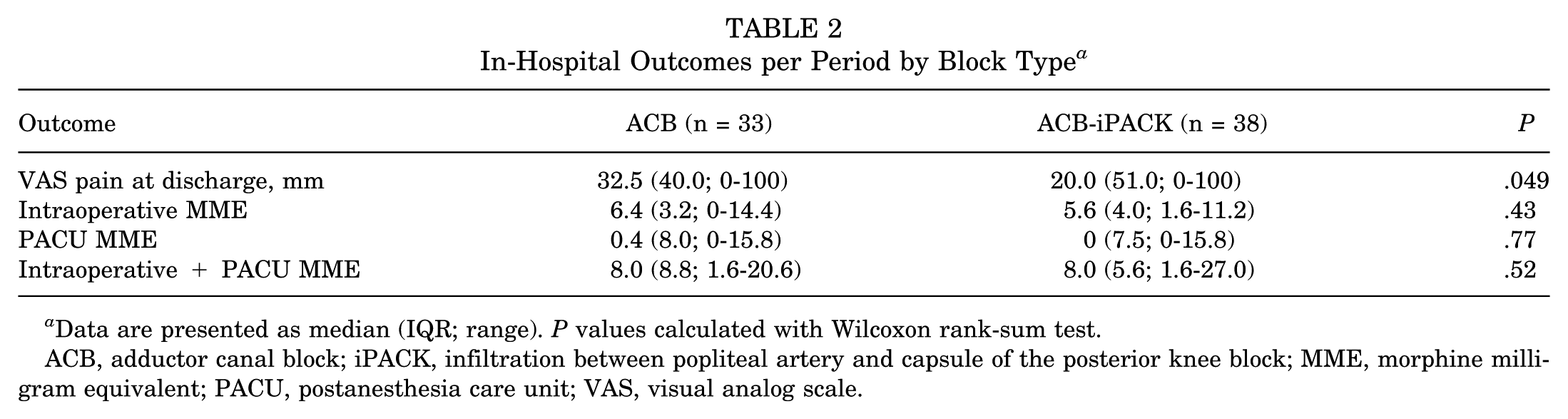
Data are presented as median (IQR; range). P values calculated with Wilcoxon rank-sum test.
ACB, adductor canal block; iPACK, infiltration between popliteal artery and capsule of the posterior knee block; MME, morphine milligram equivalent; PACU, postanesthesia care unit; VAS, visual analog scale.
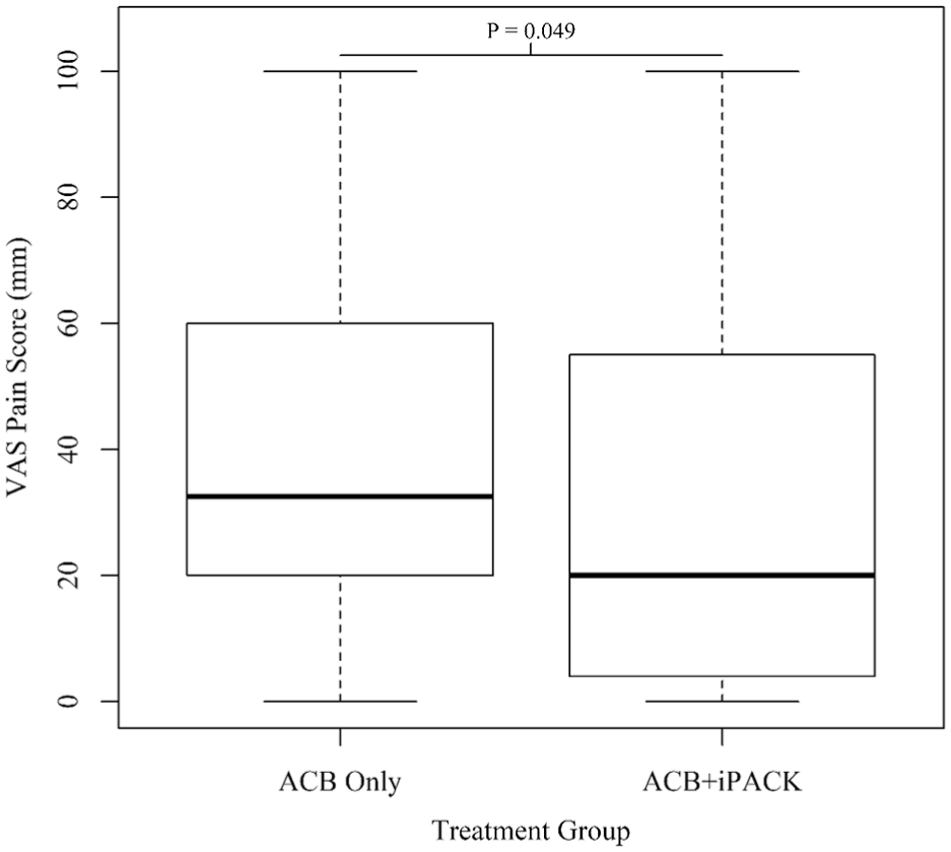
Boxplot of VAS pain score at discharge by treatment group. Boxes show the 25th, 50th, and 75th percentiles of the distribution. Whiskers extend 1.5 times the IQR from the median, and the point on the plot are those values that fall outside the median ± 1.5 × IQR. ACB, adductor canal block; iPACK, infiltration between popliteal artery and capsule of the posterior knee block; VAS, visual analog scale.
Mean Patient-Reported VAS Pain Scores by Postoperative Time Interval a
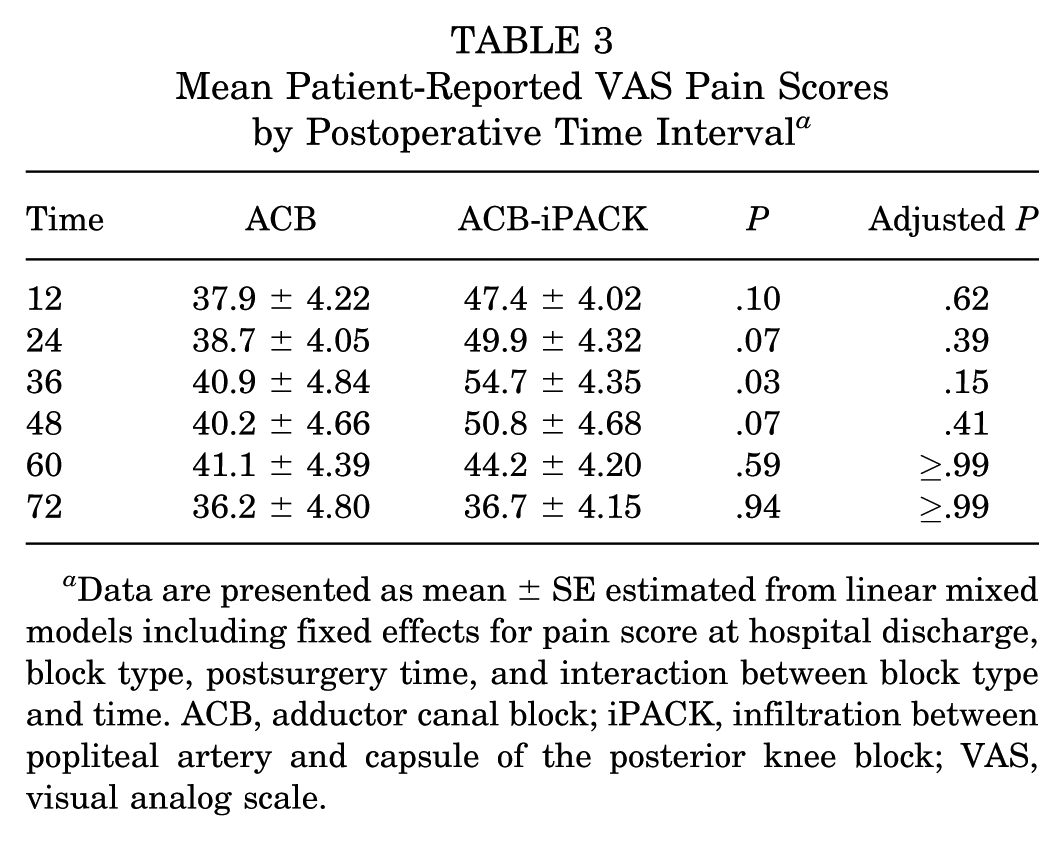
Data are presented as mean ± SE estimated from linear mixed models including fixed effects for pain score at hospital discharge, block type, postsurgery time, and interaction between block type and time. ACB, adductor canal block; iPACK, infiltration between popliteal artery and capsule of the posterior knee block; VAS, visual analog scale.
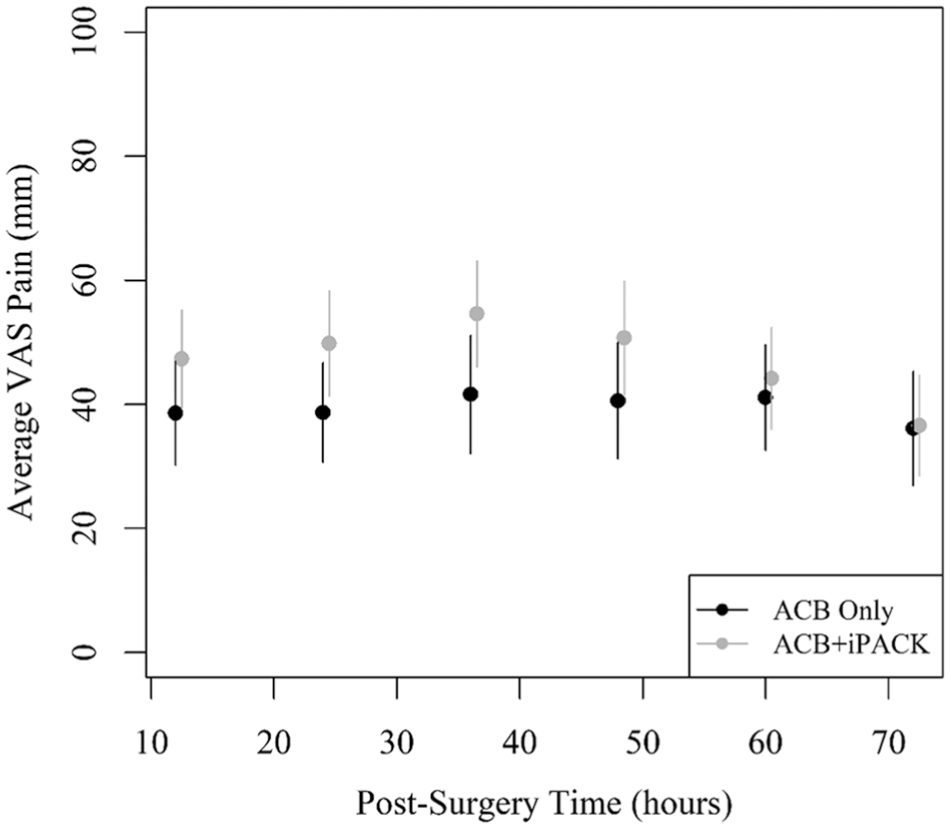
Mean patient-reported VAS pain scores with 95% confidence intervals at 12-hour postoperative intervals. Means are estimated from a linear mixed model including pain at discharge, treatment group, hours postsurgery, and the interaction between treatment group and hours postsurgery. ACB, adductor canal block; iPACK, infiltration between the popliteal artery and capsule of the posterior knee block; VAS, visual analog scale.
Postoperative Opioid Usage
In-hospital opioid consumption was similar between study groups intraoperatively (P = .43), in PACU (P = .77), and when combined between both settings (P = .52). Median opioid consumption intraoperatively, in PACU, and when combined is shown in Table 2, and the distribution of opioids consumed by the study group during the in-hospital time period is depicted in Figure 5. Mean postoperative opioid consumption was higher in the ACB-iPACK group in comparison with the ACB group at all postoperative intervals, after adjusting for in-hospital opioids. However, these differences were not significant either before or after adjusting for multiple testing. Opioid usage for each study group relative to the postoperative time interval is reported in Table 4 and depicted in Figure 6. A sensitivity analysis based on patients who completed data collection fully was also conducted, with no changes in outcome.
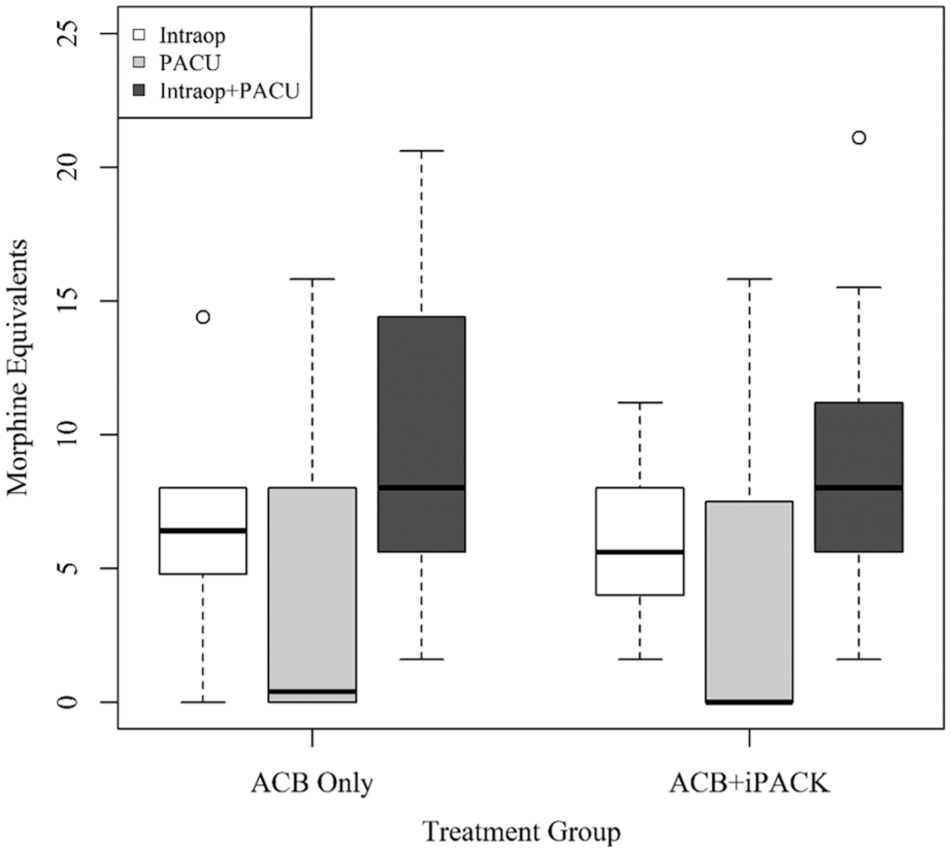
Boxplot of morphine milligram equivalent consumption per operative stage by treatment group. Boxes show the 25th, 50th, and 75th percentiles of the distribution. Whiskers extend 1.5 times the IQR from the median, and the points on the plot are those values that fall outside the median ± 1.5 × IQR. ACB, adductor canal block; iPACK, infiltration between the popliteal artery and capsule of the posterior knee block; PACU, postanesthesia care unit.
Postoperative Opioid Consumption (in MMEs) by Block Group Over Time a
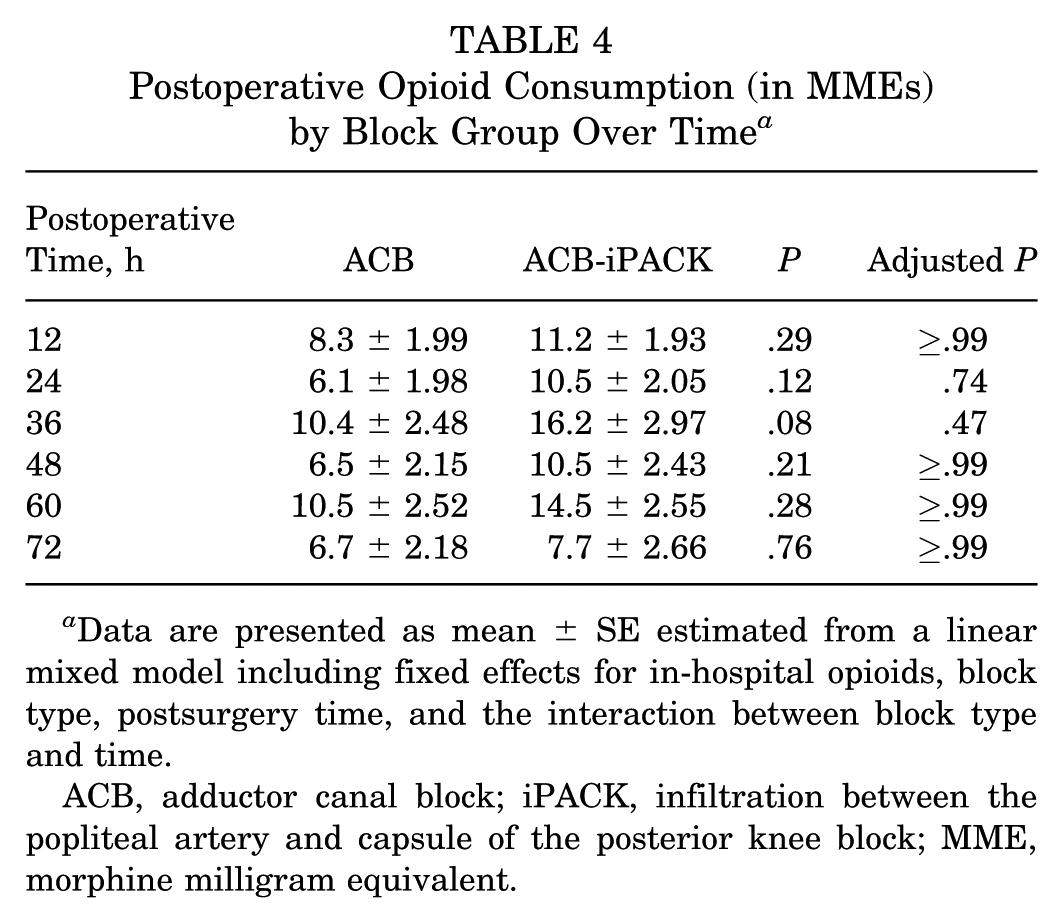
Data are presented as mean ± SE estimated from a linear mixed model including fixed effects for in-hospital opioids, block type, postsurgery time, and the interaction between block type and time.
ACB, adductor canal block; iPACK, infiltration between the popliteal artery and capsule of the posterior knee block; MME, morphine milligram equivalent.
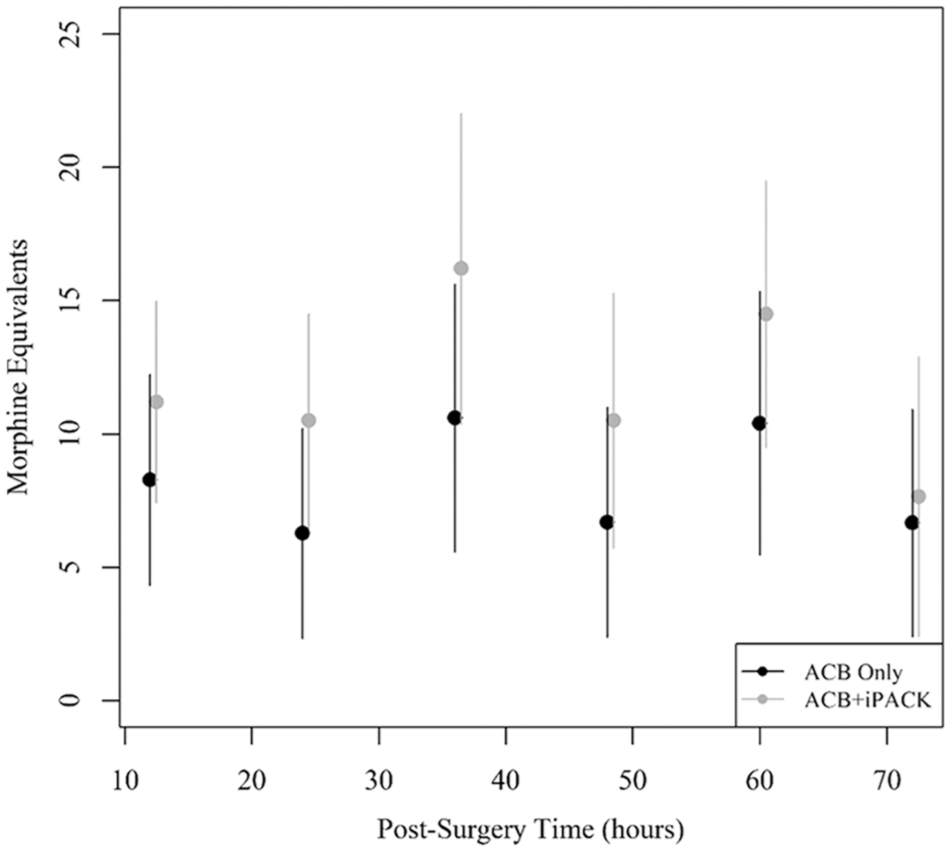
Mean postoperative morphine milligram equivalent consumption over 12-hour postoperative intervals by treatment group. Lines represent 95% CIs. ACB, adductor canal block; iPACK, infiltration between the popliteal artery and capsule of the posterior knee block.
Range of Motion
There was not a significant difference in the percentage of patients achieving full knee extension (0°) or hyperextension (0° to –10°) between study groups at either the 2- or the 6-week postoperative clinic visit. Both study groups demonstrated a decrease in the difference in ROM between the healthy versus surgical knees at the second postoperative visit relative to the first postoperative visit. Patients in the ACB-iPACK group demonstrated a smaller difference in ROM between the healthy knee and the surgical knee compared with the ACB-only group at 2 weeks postoperatively (mean difference, 9.9°) and 6 weeks postoperatively (mean difference, 9.9°). This difference between groups was significant at both time points (P = .02). The mean flexion in the healthy knee by treatment arm and in each study group by postoperative visit, the difference in ROM between the healthy versus healthy knee at each visit by study group, and the mean difference between the healthy versus surgical knee for each study group are shown in Table 5.
Postoperative Goniometric Maximal Flexion by Health Status of Knee, Block Type, and Time Point With Pre-Post Comparison a
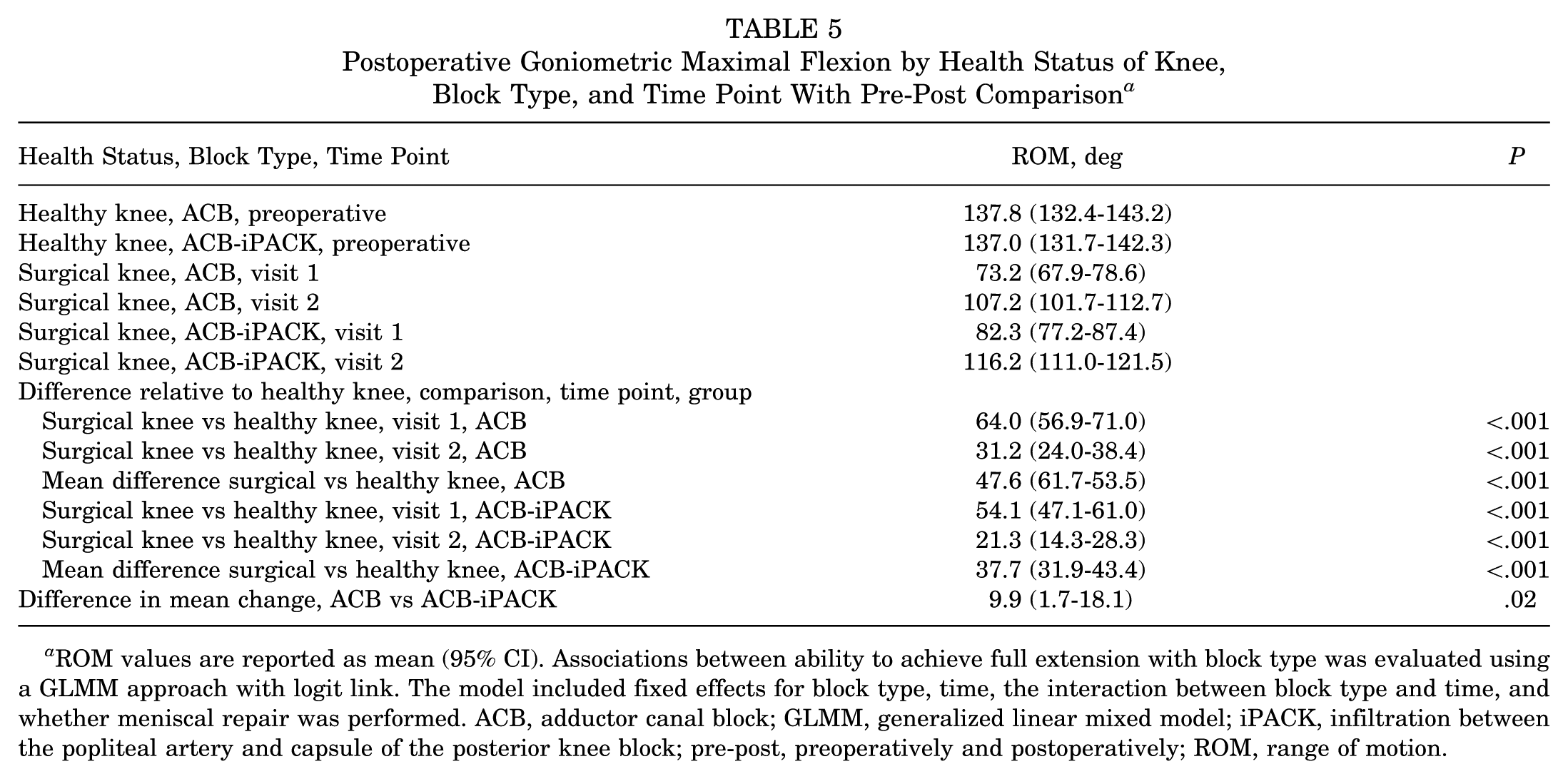
ROM values are reported as mean (95% CI). Associations between ability to achieve full extension with block type was evaluated using a GLMM approach with logit link. The model included fixed effects for block type, time, the interaction between block type and time, and whether meniscal repair was performed. ACB, adductor canal block; GLMM, generalized linear mixed model; iPACK, infiltration between the popliteal artery and capsule of the posterior knee block; pre-post, preoperatively and postoperatively; ROM, range of motion.
Complications
There were 2 observed perioperative block-related complications from regional anesthesia in the ACB group and 3 perioperative block-related complications from regional anesthesia in the ACB-iPACK group.
Discussion
The primary objectives of the current study were to compare acute VAS pain scores and opioid consumption, as well as knee ROM at 6 weeks postoperatively, with the use of continuous ACB with and without an iPACK block. The most significant findings of the current study were that the addition of an iPACK block to continuous ACB for all-inside ACL-R with QT autograft yielded a slight improvement in both pain control at the time of discharge and knee flexion at 6 weeks postoperatively. No significant advantages were observed relating to pain control or opioid consumption in the acute (≤72 hours) postoperative period.
Given that primary ACL-R is performed in the outpatient setting in ≥95% of cases, adequate pain control in the early postoperative period is of great importance to achieve appropriate patient satisfaction, same-day discharge, and effective mobilization, allowing for early functional recovery. 16 Presently, a multimodal anesthetic regimen, with the inclusion of regional anesthesia, is the standard of care to effectively control perioperative pain.2,3,6,13,15,17,20,23
Historically, an FNB was utilized to provide perioperative analgesia for patients undergoing ACL-R.13,14,17 While FNB generally provided efficacious early postoperative pain control and reduced postoperative opioid consumption, the concomitant motor blockade inhibited quadriceps muscle recovery and presented deleterious effects on rehabilitation that persisted beyond the immediate perioperative period.12,14 These effects led to the emergence of ACBs being used instead of FNBs, as ACBs provide a blockade of more distal branches from the femoral nerve, the saphenous nerve, and the nerve to the vastus medialis, which provides effective pain control to the anterior and medial aspect of the knee while sparing more proximal quadriceps motor function.1,3,13,17 Several high-level studies have investigated the analgesic efficacy of ACB in comparison with FNB.1,3,13 Abdallah et al 1 reported no significant differences in opioid consumption and pain scores in a prospective, double-blind, randomized controlled trial comparing 100 patients receiving ACB (n = 52) versus FNB (n = 48). In another prospective, randomized controlled trial of 60 patients undergoing primary ACL-R with BTB autograft, Lynch et al 13 reported decreased opioid consumption in the first 4 hours postoperatively with the use of ACB versus FNB. Pain scores and opioid requirements did not differ significantly between study groups beyond this time period, however. Similarly, in a prospective, randomized controlled trial, Bailey et al 3 reported no significant differences in pain control and opioid consumption in 90 patients randomized to receive an FNB or ACB for ACL-R with BTB autograft. The authors also found significantly greater rates of loss of knee extension in the FNB group (21.1%) compared with the ACB group (5.0%). 3 Collectively, due to its noninferior efficacy and avoidance of deleterious motor blockade, ACB was recommended by these authors to supplant FNB for perioperative pain control in ACL-R.1,3,13
Despite the validated effectiveness of ACB for acute, postoperative pain control after ACL-R, ACB doesn't provide effective analgesia from painful stimuli from the posterior aspect of the knee. 26 SNB, selective TNB, and the iPACK block have therefore been utilized in knee surgery to augment ACB by providing additional coverage to this region of the knee, supplied by the popliteal plexus. 25 In comparison with SNB and TNB, iPACK blocks confer the advantage of not inducing a blockade of motor function. 25 The analgesic efficacy of adjuvant iPACK block to ACB is best studied in the knee arthroplasty literature, where it has generally resulted in improved postoperative pain control and reduced opioid use and length of hospital stay.8,10,19,24
Relative to the arthroplasty literature, there currently exists a relative paucity of studies characterizing these effects of adjuvant iPACK blocks for ACL-R. Deis et al 6 performed a retrospective study in 184 patients undergoing ACL-R with allograft and QT, hamstring, and BTB autograft selections who received a single-shot FNB either with (n = 111) or without (n = 73) an iPACK block. The authors reported no significant differences in PACU pain scores or opioid consumption, but lower intraoperative anesthetic requirements and shorter postoperative stay by approximately 40 minutes in the study group receiving an iPACK block. 6 Amer 2 performed a prospective, randomized cohort study consisting of 246 patients undergoing ACL-R who received either a single-shot ACB and iPACK block (n = 123) or a single-shot ACB and an adjuvant periarticular anesthetic injection consisting of ropivacaine and dexamethasone (n = 123). The author reported significantly reduced opioid consumption and improved VAS pain scores in the acute perioperative period (up to 48 hours postoperatively) in the group of patients receiving ACB and iPACK block. Notably, the author did not specify the graft selection that patients received. Finally, Rao et al 20 reported the results from a single-center, randomized controlled trial comparing 96 patients undergoing ACL-R with BTB autograft with either single-shot ACB alone (n = 47) or single-shot ACB with an iPACK block (n = 49). Rao et al reported significantly decreased opioid consumption, improved postoperative pain scores, and improved patient satisfaction in patients receiving an additional iPACK block. Notably, the patient and anesthesiologist were not blinded to the study intervention, whereas the current study utilized a placebo skin wheal to effectively blind patients to whether or not they received an adjunctive iPACK block. The current study also provides a comparison of ROM at 6 weeks postoperatively between study groups, an outcome not characterized by Rao et al. Other important distinctions in the control treatment and graft selection exist between the current study (continuous ACB and ACL-R with QT autograft alone, respectively), and the studies by Deis et al, Amer, and Rao et al. Given the known differences in the pain profile depending upon ACL graft selection and differences in the length of analgesic effect of single-shot versus continuous peripheral nerve blocks, evaluating the need for an additional iPACK block is warranted.4,22 While the distinctions between this current study and the aforementioned literature on the addition of an iPACK block to either ACB or FNB limit direct comparison, the findings of the current study suggest a more subtle benefit from this addition in the setting of a continuous ACB and/or QT autograft selections. The difference in median VAS pain scores at discharge between groups in the current study was approximately 12.5 mm. Previous studies evaluating minimal clinically important differences (MCIDs) for acute pain measured on a 100-mm VAS have generally reported thresholds in the range of approximately 10 to 13 mm.9,18 As such, while the observed difference reached statistical significance, it is close to the lower estimates of MCID and may therefore represent only a small clinical effect. Further prospective study is required to better characterize its benefits in these relative settings.
Limitations
There are several limitations to the current study. First, the study may be marginally underpowered to detect small differences between groups, as the a priori power analysis indicated 35 patients per group was necessary to detect the prespecified effect size. Next, the anesthesiologist was not blinded to the study intervention, which could introduce a potential bias in perioperative opioid administration. Despite this, there were no differences in combined perioperative opioid usage between groups. Another potential limitation is the remote self-reporting of opioid usage and subjective pain levels by patients. In the current study, 17% of patients did not provide complete outcome data. A sensitivity analysis based on patients who completed data collection fully was also conducted, however, with no changes in outcome. Additionally, the 12-hour intervals used for capture of subjective pain assessments may fail to capture episodes of breakthrough pain. Despite this, the practicality of more frequent subjective assessment is limited in the outpatient setting. Certain outcomes were also examined post hoc, as specified, and the findings should be interpreted as hypothesis generating and warrant confirmation in future studies. The findings of the current study are also limited by their comparison with the use of continuous ACB and ACL-R with QT autograft, and therefore, the findings may not necessarily be extrapolated accurately to when an iPACK block is combined with single-shot ACB or ACL-R with other graft selections. It also cannot be ruled out that confounding variables influenced the study outcomes. While the numerical difference in LET frequency could represent a potential confounder, the magnitude of the imbalance was relatively small and did not appear to translate into a measurable clinical difference in early motion in our data set. Finally, the study is limited by its relatively small sample size and short follow-up period. However, the primary outcomes were early postoperative pain control, opioid utilization, and ROM differences, which were designed to be assessed in the short-term postoperative period. Longer-term functional outcomes, including sustained changes in knee ROM, are therefore unable to be determined.
Despite these limitations, the blinded and randomized controlled nature of the current study provides an effective comparison of the addition of an iPACK block in the specific setting of a continuous ACB for perioperative pain control for ACL-R with exclusively QT autograft and is appropriately powered for the primary outcome of interest. The results of the current study may be utilized to inform patients regarding risk-benefit assessments with the use of an adjunctive iPACK block to continuous ACB in the setting of ACL-R with QT autograft, given the potential complications of an iPACK block, including nerve injury, vascular injury or hematoma, anesthetic toxicity, and allergic reaction. 7
Conclusion
Adding an iPACK block to continuous ACB for all-inside ACL-R with QT autograft provided a slight reduction in pain at discharge (VAS difference, 12.5 mm) and improved knee flexion at 6 weeks. However, pain scores and opioid use beyond the immediate postoperative period were not significantly different between groups. These findings may help guide patient counseling regarding the expected benefits of incorporating an iPACK block in this surgical setting.
Footnotes
Acknowledgements
The authors acknowledge the Medical University of South Carolina Department of Anesthesia and Perioperative Medicine for helping to facilitate the study from conception to completion.
Final revision submitted March 9, 2026; accepted March 21, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by internal departmental support (Department of Anesthesia and Perioperative Medicine, Medical University of South Carolina). This project was also supported by the South Carolina Clinical & Translational Research Institute, Medical University of South Carolina This manuscript was supported in part by the National Institutes of Health (NIH), National Center for Advancing Translational Sciences, Grant Number UM1TR005294.
Ethical approval for this study was obtained from the institutional review board at the Medical University of South Carolina (June 21, 2022; No. Pro00121103).
Data Accessibility Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available because of privacy or ethical restrictions.