
Abstract
Background:
Stress fractures are common in young athletes and a major cause of time lost from training. While epidemiological data exist from Western countries, reports from Asian regions, particularly in subtropical settings, are limited, as year-round training may influence injury risk.
Purpose:
To assess stress fracture characteristics among adolescent and recreational athletes in Okinawa.
Study Design:
Descriptive epidemiology study.
Methods:
A retrospective review of medical records from orthopaedic clinics and sports medicine centers across Okinawa Prefecture, Japan, between 2018 and 2019 was conducted. Athletes aged <50 years who were diagnosed with imaging-confirmed stress fractures were included. Data on age, sex, sport, fracture site, and return to training (RTT) (defined as symptom-free resumption of sport-specific practice) were collected.
Results:
A total of 309 stress fractures were identified in 303 athletes (mean age, 15.6 ± 5.9 years; 47% women). The tibia (31%), metatarsals (28%), and tarsal bones (18%) were the most frequently affected sites. Soccer (21%), basketball (21%), and track and field (14%) accounted for the majority of cases. The median RTT time was 7 weeks (interquartile range [IQR], 4-8 weeks). High-risk fracture sites, such as the fifth metatarsal bone and patella, required significantly longer recovery (median, 8 weeks [IQR 4-12 weeks]; P < 0.01).
Conclusion:
This is the first epidemiological study on stress fractures in a subtropical region of Japan. The findings highlight sport- and site-specific patterns and demonstrate that high-risk anatomic sites require prolonged recovery before a safe return. These results provide important evidence for the development of region-specific prevention and rehabilitation strategies for adolescents and recreational athletes.
Stress fractures are among the most common overuse injuries, accounting for up to 20% of all sports injuries.13,32 Stress injuries occur when bones are repeatedly subjected to submaximal loading without adequate rest during training and competition, leading to an imbalance between bone formation and resorption.4,17,29 Stress fractures predominantly occur in the lower extremities, except the lumbar spine. 37 Many stress fractures heal without complications, but competitive athletes may face prolonged return to play (RTP), ranging from several weeks to months, depending on the injury site. If complete bone union is not achieved before returning to full activity, the athlete is at risk of delayed union or nonunion. 5 Stress fractures are clinically classified as low- or high-risk. Low-risk stress fractures usually heal without major complications, allowing for the early initiation of progressive RTP. In contrast, high-risk stress fractures require a more cautious treatment strategy because of the greater tensile load and limited blood supply to the injury site. McInnis and Ramey 27 defined high-risk stress fractures as those occurring in the femoral neck, patella, anterior tibial shaft, proximal fifth metatarsal, medial malleolus, navicular tarsal, talus, or the sesamoids of the great toe. High-risk stress fractures may require longer healing times and surgery, as described by Hoenig et al 19 in a systematic review and meta-analysis.
The epidemiology of stress fractures has been well-described in large cohorts from North America and Europe.7,23,24,26,36,38,40 However, data from Asian populations remain limited, despite the growing participation of adolescents and young adults in organized sports. Environmental and cultural factors may influence the incidence and anatomic distribution of stress fractures. Climate, dietary habits, and training culture are particularly relevant considerations when interpreting regional variations in injury risk.
Okinawa Prefecture, located in Japan's subtropical region, offers a unique setting for studying the epidemiology of stress fractures. This region is characterized by annual participation in outdoor sports and school-based athletic programs and has the highest levels of ultraviolet exposure in Japan. 21 Moreover, high school baseball, soccer, basketball, and handball are popular. Japanese school club activities, “bukatsu,” can range from low-frequency participation to highly intensive training schedules, including after-school and weekend sessions, and participation is typically described as voluntary within educational guidance; we therefore explicitly describe this exposure context when interpreting epidemiology in youth athletes. 22 These factors suggest that the epidemiological profile of stress fractures in Okinawa may differ from that in mainland Japan and Western countries.
Therefore, we aimed to investigate the incidence, anatomic distribution, sports-specific patterns, and return-to-training (RTT) timelines of stress fractures among adolescent and recreational athletes in Okinawa Prefecture. By providing the first epidemiological data from a subtropical Asian population, this study may contribute to international understanding of stress fracture risk and inform clinicians and policymakers in developing regions to develop region-specific prevention and rehabilitation strategies for young athletes.
Methods
Study Design and Setting
This retrospective population-based epidemiological study was conducted in Okinawa Prefecture, Japan. Medical record-based data were collected from 34 orthopaedic clinics, sports medicine centers, and 14 hospitals that routinely manage sports-related injuries across the prefecture. Japan has statutory universal health insurance with broad access to medical institutions; therefore, this study is a multicenter, region-wide retrospective chart review rather than a single unified health system registry. 31 The study period was from January 2018 to December 2019.
Case Identification and Extraction
Potential cases were identified by querying the electronic medical billing databases of participating clinics and hospitals using International Classification of Diseases, 10th Revision codes related to stress fractures of the lower extremity (eg, M84.3 for stress fracture, with site-specific subcodes). To ensure comprehensive capture, we also performed keyword searches within the electronic medical records for the following terms: "stress fracture"; "stress injury"; "fatigue fracture"; and "overuse injury" in combination with anatomic locations (eg, "patella"; "tibia"; "metatarsal"). After the initial automated retrieval, 2 independent investigators manually reviewed clinical charts and imaging reports (radiographs, magnetic resonance imaging [MRI], and/or computed tomography [CT]) to confirm the diagnosis and exclude acute traumatic fractures or insufficiency fractures related to underlying metabolic bone disease. Any discrepancies in case inclusion were resolved through consensus.
Participants
Athletes aged >6 years old and <50 years who were actively participating in organized sports at the elementary, junior-high, high school, collegiate, or recreational levels were eligible. The lower age limit was set at 6 years to broadly capture pediatric as well as adolescent sports-related stress fractures. Although stress fractures are less common in younger children than in adolescents, pediatric cases have been reported, 6 and recent epidemiologic studies have included children aged 6 to 18 years. 33 We also justify this criterion in terms of focusing on an athletic population and excluding typical insufficiency fracture epidemiology observed in older adults. The inclusion criteria were as follows: (1) diagnosis of pelvic or lower extremity stress fracture confirmed by imaging, plain radiographs, MRI, ultrasonography (US), or CT; (2) participation in athletic training, competition, or recreational sports activity at the time of injury; and (3) complete medical records documenting the clinical course and RTT status. The exclusion criteria included pathological fractures, metabolic bone disease, and incomplete medical records.
Data Collection
Medical charts were reviewed to extract data on demographic characteristics (age and sex), sport type, and fracture site. Fracture locations were classified as tibia, fibula, metatarsals, tarsal bones (navicular, calcaneus), femur, pelvis, patella, sesamoid bones, and multiple sites. Sports were categorized as track and field, baseball, soccer, basketball, volleyball, badminton, jogging, tennis, karate, and others. RTT was defined as the first documented date of physician-permitted training resumption and/or the first documented patient-reported resumption of structured training of sport-specific practice (running, drills, or team practice) regardless of competition readiness.
Diagnosis and Imaging
Stress fractures were assessed by orthopaedic specialists. Clinical examination of the affected limb revealed localized bone tenderness. Diagnosis was performed using radiographs, US, CT, and MRI. Imaging was accessed via a local picture archiving and communication system at each clinic or hospital, and whether images were reviewed for research purposes by orthopaedic surgeons. The primary diagnostic modalities employed were conventional radiography and ultrasonography. When these initial findings were inconclusive for a stress fracture, an MRI or a CT was subsequently performed to confirm the diagnosis. Radiographs revealed periosteal thickening or sclerosis, cortical changes, callus formation, endosteal thickening, sclerosis, and fracture lines. US identified a hypoechoic hematoma with periosteal elevation, soft tissue edema, and cortical break. CT showed peri- and endosteal thickness and fracture lines. MRI showed linear hypointense fracture lines on T1-and T2-weighted images, with adjacent bone marrow and soft-tissue hyperintensity on T2 fat–saturated sequences, corresponding to bone edema.2,13 For MRI assessment, Fredericson Grade 4 was categorized as a stress fracture. These diagnostic standards were strictly unified across all study sites.
Outcome Measures
The primary outcome was the time from diagnosis to RTT (in weeks). Secondary outcomes included fracture rate ratio comparing sex-comparable sports, anatomic distribution of stress fractures, and sport-specific injury patterns. Athletes were stratified into high-risk and low-risk fracture groups based on the McInnis and Ramey 27 classification. High-risk stress fractures are those occurring in the femoral neck, patella, tibial shaft of the anterior cortex, proximal fifth metatarsal, medial malleolus, tarsal navicular, talus, or great toe sesamoids. Others are classified as low-risk stress fractures. Two independent investigators performed a manual review, and any discrepancies in case inclusion were resolved through consensus.
Statistical Analysis
Statistical analyses were performed using JMP Pro 15.0.0. (SAS). Ages are expressed as means ± standard deviations. RTT was analyzed using Kaplan-Meier survival curves, with log-rank tests used for unadjusted comparisons between sports and between high- and low-risk groups. Descriptive statistics for RTT are reported as medians and interquartile ranges (IQR). For adjusted analyses, Cox proportional hazards regression was used to estimate hazard ratios and 95% CIs, accounting for potential confounders, including age and fracture site. Statistical significance was set at P < .05.
Ethics
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and was approved by the institutional review board (IRB) of our institution (IRB No. 1619). Informed consent was waived owing to the retrospective nature of the study.
Results
Study Population
A total of 450 patient records were obtained. Patients who were injured during unrelated sports activities and those aged >50 years were excluded. A total of 130 patients whose clinical course could not be followed were excluded. Finally, 303 patients were included in this study (Figure 1).

Flowchart showing the number of athletes participating in this study.
A total of 309 stress fractures were identified in 303 athletes (mean age, 15.6 ± 5.9 years; 47% women; 142 cases) during the 2-year study period. The proportions among cases are as follows: soccer (n = 64/303; 21%); basketball (n = 64/303; 21%); and track and field (n = 43/303; 14%), accounting for a majority of cases, with the highest proportions in men's soccer (n = 51/303; 16.8%), men's baseball (n = 40/303; 13.2%), and women's basketball (n = 41/303; 13.5%) (Table 1).
Total Number of Stress Fractures by Sport and Ratio of Proportions by Sex Among Cases a

Other: American football (n = 1), dance (n = 2), golf (n = 1), triathlon (n = 1), ballet (n = 1), fitness (n = 1), marching band (n = 3), judo (n = 1), gymnastics (n = 2). M, men; NA, not applicable; W, women.
In all sports, stress fractures occurred more often in men (n = 160/303; 53.3%) than in women (n = 142/303; 46.7%). Men showed higher stress fracture rates in baseball (ratio of proportions, 0.05; comparing the stress fracture ratio between sex-comparable girls’ and boys’ sports [women/men]), soccer (ratio of proportions, 0.25), and jogging (ratio of proportions, 0.25), whereas women showed higher ratios of proportions in badminton (ratio of proportions, 5.5), volleyball (ratio of proportions, 3.5), and basketball (ratio of proportions, 1.78) (Table 1).
Anatomic Distribution
The most frequent injury sites were the tibia (n = 95/303; 31.3%), metatarsals (n = 84/303; 28%), and tarsals (n = 53/303; 17.4%), followed by the pelvis (n = 20/303; 6.6%), femur (n = 15/303; 5%), and patella (n = 15/303; 5%) (Table 2). The tibia was the most frequently affected site across most sports, including soccer, track and field, and handball. Locations in the tibia included the medial condyle (n = 5), proximal tibia (n = 2), distal and proximal thirds of the tibia (n = 59), central tibia (n = 18), central anterior cortex (n = 1), distal tibia (n = 3), and medial malleolus (n = 9). Metatarsals were the second most commonly affected site: first (n = 7), second (n = 17), third (n = 26), fourth (n = 15), and fifth (n = 10) metatarsals, and multiple metatarsal locations (n = 10). Tarsals were the third most commonly affected site: cuboid (n = 12), calcaneus (n = 12), navicular (n = 11), cuneiforms (n = 7), talus (n = 4), and multiple tarsal locations (n = 5).
Location of Stress Fracture Injuries by Sport (n = 303 Injuries) a

Multiple: Tarsals + metatarsal (n = 4), metatarsals + sesamoid (n = 1), tibia + tarsals (n = 1). Other: Kendo (n = 3), marching band (n = 3), dance (n = 2), gymnastics (n = 2), judo (n = 1), American football (n = 1), ballet (n = 1), triathlon (n = 1), fitness (n = 1).
Six patients had multiple stress fractures of the lower legs: tarsals and metatarsals (n = 4), metatarsals and sesamoids (n = 1), and tibia and tarsals (n = 1).
Return to Training
The median RTT was 7 weeks (IQR, 4-8 weeks), with no significant difference between men (median, 7 weeks [IQR, 4-8]) and women (median, 7 weeks; IQR, 4-8; log-rank P = .77). Details of the RTT after training are shown in Figure 2A. Sport-specific analysis revealed median RTT of 7 weeks (IQR, 4-8) for soccer players, 7.5 weeks (IQR, 4-10) for basketball players, and 8 weeks (IQR, 4-8) for runners.

Duration to RTT. (A) RTT by sport. (B) RTT by anatomic distribution. RTT, return to training.
The longest RTT times were 14 weeks (IQR, 8-16), 8 weeks (IQR, 8-10), and 8 weeks (IQR, 7.5-10) for karate, jogging, and women's softball, respectively. On the contrary, the shortest RTT was 4 (IQR, 3-8) weeks for both handball and tennis. Details of RTT by injury site are shown in Figure 2B. The longest RTT were 8 weeks (IQR, 8-12), 8 weeks (IQR, 8-8), and 8 weeks (IQR, 4-12) for injuries to the patella, multiple sites, and fibula, respectively.
High-Risk and Low-Risk Stress Fractures
In the present study, 70 high-risk stress fractures occurred in 40 men and 30 women. A significant difference in RTT and age was observed between the high-risk and low-risk groups. Patients who had high-risk stress fractures were younger (13.9 ± 3 years; P = .0009) and required longer RTT (median, 8; IQR, 4-12) weeks; P = .0073) than did those with low-risk stress fractures (16.1 ± 6.5 years; median 7; IQR, 4-8 weeks) (Table 3A).
High-Risk Stress Fractures a

A: Comparison of high-risk and low-risk stress fractures. B: Return to training for high-risk stress fractures in anatomic distribution. IQR, interquartile range; RTP, return to play.
Details of high-risk stress fractures are presented in Table 3B. The patella (n = 15), fifth metatarsal (n = 14), and navicular (n = 13) were common sites of high-risk stress fractures. A fifth metatarsal stress fracture had the longest RTT time (median, 9.5 weeks [IQR, 6-12]). Four patients underwent intramedullary nailing surgery; all were men (3 patients were aged 18 years, and 1 patient was aged 12 years), with 2 playing basketball and 2 playing soccer. All the participants were able to RTP. The median age of the 15 patients with patellar stress fractures was 13 years (IQR, 11-15 years), comprising 10 male and 5 female athletes. The distribution of sports activities included basketball (n = 4), soccer (n = 3), and 2 cases each for baseball, karate, and volleyball, while track and field and badminton accounted for one case each. In our cohort, patellar stress fractures were more prevalent among younger male athletes.
Discussion
To our knowledge, this is the first population-based epidemiological study of stress fractures in adolescent and recreational athletes in a subtropical Asian population. During the 2-year study period, 450 stress fractures were recorded, with the tibia, metatarsals, and tarsal bones being the most frequently affected sites. The median RTT time was 7 weeks; however, recovery was significantly prolonged in athletes with high-risk fracture sites (such as the femoral neck, fifth metatarsal, and patella). These findings provide novel region-specific data from a subtropical Asian population and highlight the importance of fracture location in predicting recovery timelines.
During the study, 450 stress fractures of the pelvis and lower extremities were recorded 30 in Okinawa (population ~1.5 million in 2020), of which 433 were sports-related. Previous epidemiological studies on stress fractures have been generally focused on specific cohorts, such as single-center or clinic-based studies,26,40 high school athlete cohorts,7,31,38 collegiate athletes, 36 and elite athletic programs. 24
The reported incidence of stress fractures varies widely. Changstrom et al 7 reported 389 stress fracture cases (0.8% of all injuries) over 7 years in the United States high school athletes, with an overall rate of 1.54 per 100,000 athlete exposures, while Ruddick et al 38 identified 181 stress fractures in 152 Australian high-performance athletes over 3 years (0.15% of all sports injuries). Similarly, Rizzone et al 36 noted a higher incidence of stress fractures in female than in male National Collegiate Athletic Association athletes. 36 These differences likely reflect variations in study populations (general vs selected), age ranges, and activity levels. According to regional data, the high school student population in Okinawa totaled 90,533 during the 2018-2019 period. 41 Based on the 188 high school cases identified in our cohort (Supplemental Table 1), the estimated incidence rate is 0.21%. We must emphasize, however, that this represents a crude incidence for the entire student population. Among the 433 cases of sports-related stress fractures in our cohort, only 15.2% (n = 66/433) occurred in individuals aged >18 years. The university advancement rate for high school students in Okinawa Prefecture 34 is approximately 49%. The collegiate sports system primarily centers around recreation and extracurricular clubs. This low proportion is likely related to changes in the volume of sports activity exposure after high school graduation.
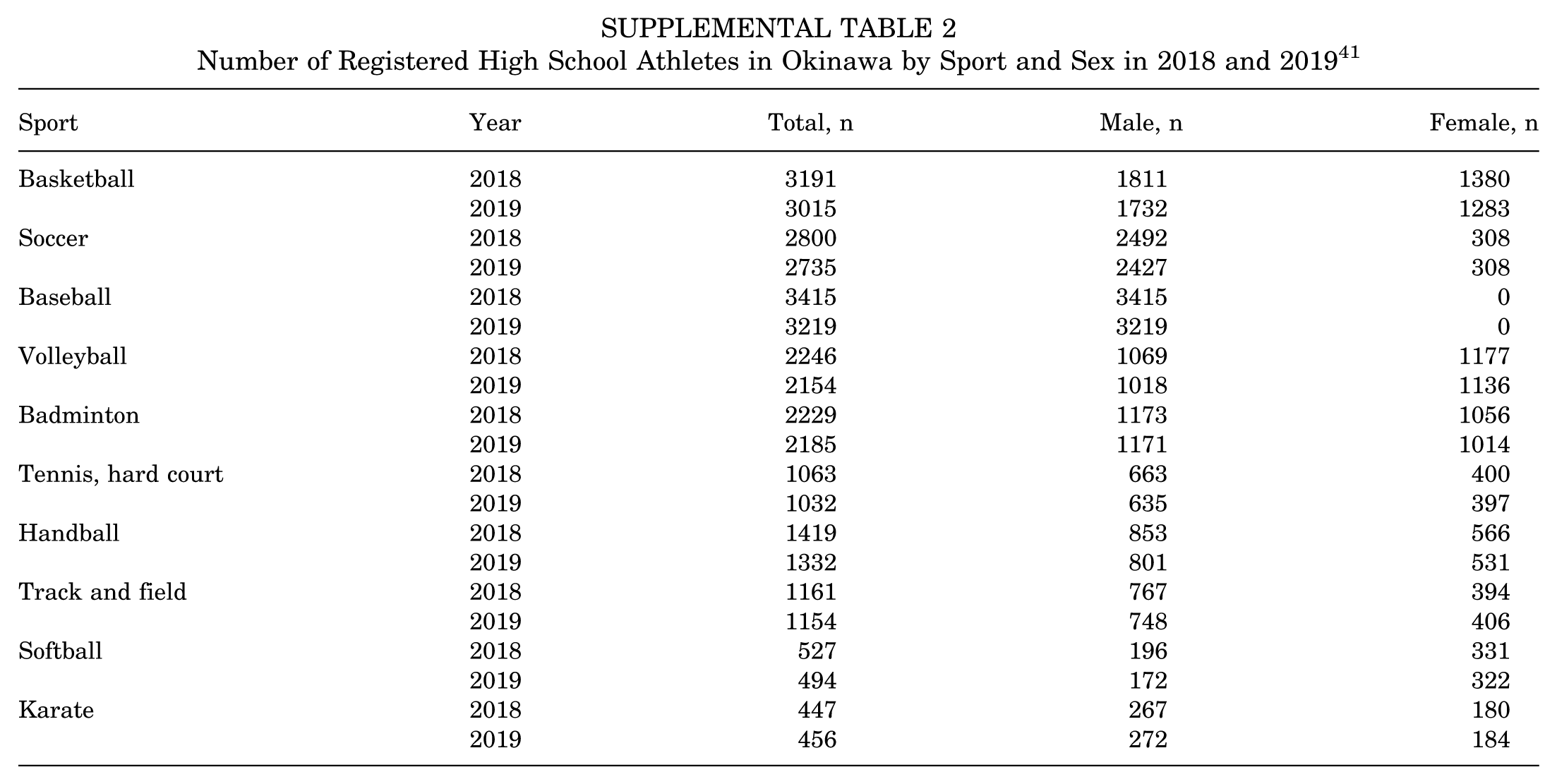
The mean age of the patients in our cohort was 15.6 years, similar to previous reports in young athletes.23,24 The peak bone mass is generally attained toward the end of the second decade, and adolescents may be vulnerable to fractures during periods of rapid growth when mineralization can lag behind somatic growth; thus, age and skeletal maturity may modify stress fracture epidemiology. 18 Many previous studies have revealed that female sex is a risk factor for stress fractures.36,38 Accordingly, we have included a new table (Supplemental Table 2) showing the number of registered high school athletes in Okinawa by sport and sex for 2018 and 2019. These data support the high number of stress fractures observed in sports with high female participation, such as badminton, basketball, and volleyball. Differences in participation rates may influence the absolute number of stress fractures observed. This phenomenon also extends to comparisons between countries. In our study of Okinawa athletes, male soccer players, female basketball players, and male baseball players had the highest rates of stress fractures. In contrast, high school athletes in the United States have been reported to sustain stress fractures most frequently in sports such as American football, girls’ basketball, and girls’ track and field. 7 However, among Australian high-performance athletes, gymnastics, track and field, and field hockey have been reported as the sports with the highest number of lower extremity stress fractures. 38 These differences likely reflect varying sports popularity and training practices across regions, highlighting that the profile of stress fracture risk sports is not the same worldwide.
Regarding anatomic location, the most common sites of stress fractures in our study were the tibia (n = 95/303; 31.3%), metatarsals (n = 84/303; 28%), and tarsals (n = 53/303; 17.4%). This distribution aligns with previous reports from Western cohorts, which found that the tibia and metatarsals were the most frequently affected sites.6,7,33,36,38,40 However, the proportion of patellar fractures in our study (approximately 5% of 303 cases) was somewhat higher than that reported in most European and North American studies. While Devas 8 primarily highlighted running-related stress fractures in young adults, our cohort reflects a younger demographic (mean age, 13 years) engaged in high-impact jumping and multidirectional sports, such as basketball and soccer. The predominance of male athletes in our study aligns with Devas's initial observations. However, the occurrence in sports like karate and baseball suggests that patellar stress injuries in the pediatric population are not limited to traditional “running” sports but are closely tied to repetitive, high-velocity loading of the extensor mechanism during critical phases of patellar ossification.
Siddiqi et al 39 demonstrated that Japanese femora are significantly shorter in maximum bone length and have a smaller neck-shaft angle than those of Caucasians. Furthermore, the people of the Ryukyu Islands (Okinawa) are characterized by even shorter and more robust long bones, reflecting the retention of Jomon skeletal traits.14,16 A smaller neck-shaft angle increases the bending moment and resultant shear stress on the femoral neck. Additionally, a shorter femoral length may alter the muscle lever arm and load distribution across the lower extremity. These structural factors are considered inherent predispositions for the stress distribution patterns observed in this region. Moreover, the sports participation patterns may be attributed to Okinawa, where soccer and karate are highly popular, both of which involve repetitive kicking and high stress on the anterior knee.
Regarding recovery, the mean RTT was 7 weeks with no significant difference between male and female athletes. We examined RTT by sport type and found that athletes in karate, jogging, and softball had the longest mean RTT durations, although the sample sizes in these sports were small. In contrast, sports with larger case numbers—soccer (n = 64), basketball (n = 64), and track and field (n = 43)—had mean RTT times of approximately 7 to 8 weeks, roughly mirroring the overall mean. However, there is a paucity of literature comparing RTT across sports.9,15,35
We also evaluated RTT by injury site. The longest recovery periods were observed for fractures of the patella (median, 8 weeks [IQR, 8-12]), multiple concurrent sites (median, 8 weeks [IQR, 8-8]), and the fibula (median, 8 weeks [IQR, 4-12]). In comparison, stress fractures in more common locations, such as the tibia, fibula, or metatarsals, tended to heal more quickly (often allowing RTT in approximately 6 to 8 weeks). These findings align with previous reports of prolonged recovery for certain sites. 28
Multiple authors have suggested classifying stress fractures as “high-risk” or “low-risk” based on the fracture's anatomic site and likelihood of complications.10,19,27 In general, high-risk stress fractures are those with a propensity for poor natural healing and complications, such as delayed union, nonunion, complete fracture, avascular necrosis, or recurrent injury. In our study, 70 patients (approximately 23% of all documented stress fracture cases) had high-risk fracture sites. Athletes with high-risk fractures were significantly younger on average (13.9 ± 3 years) and had a longer RTT (median, 8 weeks [IQR, 4-12]) compared with those with low-risk fracture sites. The most common high-risk locations in our cohort were the patella, the fifth metatarsal, and the navicular. Our series included a single case of a femoral neck stress fracture in a 29-year-old female marathon runner. Although initial plain radiographs failed to identify a fracture line, subsequent MRI led to a diagnosis of a compression-type injury. The patient was managed nonoperatively with a complete cessation of impact activities. No fracture propagation was observed during the clinical course, and the patient successfully returned to training at 26 weeks after diagnosis. Previous studies have corroborated the need for prolonged recovery from high-risk stress fractures. Hoenig et al 19 conducted a systematic review and meta-analysis comparing RTP outcomes between low- and high-risk stress fractures. Across 76 studies (covering 2974 bone stress injuries), tarsal navicular and femoral neck injuries were identified as injuries with the longest mean time to RTT (127 and 135 days, respectively), a pattern similar to that observed in our local population. Identifying whether a stress fracture is high- or low-risk is clinically important to guide management. Low-risk stress fractures generally heal well with nonoperative treatment and a period of rest after impact activities, allowing a relatively prompt RTT. In contrast, high-risk stress fractures often require more aggressive management, such as longer periods of immobilization or nonweightbearing, careful rehabilitation protocols, and sometimes surgical intervention to prevent complications and ensure healing. Our findings reinforce the idea that high-risk stress fractures require a longer recovery time before returning to competition, and treatment plans should be made with this in mind.
Okinawa is a subtropical region with high ultraviolet exposure; this environmental factor alone may not necessarily result in a lower incidence of stress fractures. Although we did not directly measure variables, such as actual outdoor exposure time, dietary intake, body mass index, or serum vitamin D levels, the existing literature 3 suggests that vitamin D insufficiency can be prevalent among Japanese youth even in summer. 25 Furthermore, because stress fractures are multifactorial, any potential protective effect of the subtropical climate might be offset by high training loads and repetitive mechanical stress. The extent to which these unmeasured biological and lifestyle factors influenced our findings warrants further investigation, but they may help explain why the incidence in our cohort was comparable with that reported in Western populations.
Our study has a few limitations. First, it has a rather small sample size with a large dropout rate. A total of 130 patients (29.8%) did not return for their next scheduled clinic or hospital visit. The reasons for these dropouts are unclear, which is a limitation inherent to the retrospective study design. Excluding patients without follow-up documentation may introduce selection bias in RTT estimates if follow-up completeness is associated with injury severity, sport level, or access to care. While we provided an explicit operational definition of RTT—defined as the first documented date of clinician-permitted resumption and/or patient-reported resumption of structured training—we acknowledge that return-to-sport (RTS) constructs lack a standardized definition across the orthopaedic sports medicine literature. This inherent variability may affect comparability across studies. Furthermore, data regarding full return to RTS were often sparse or inconsistently documented in clinical charts. Consequently, RTT should be interpreted as a clinical milestone of rehabilitation progress rather than a comprehensive metric of restored athletic performance. Second, we were unable to calculate injury incidence per athlete-exposure because detailed training and participation data, as well as athlete-level data, were unavailable. Injury rates are often expressed per athlete's exposure (eg, per training session or competition) to account for differences in time at risk. The International Olympic Committee consensus statement recommends using exposure data (eg, athlete days) to more accurately estimate injury incidence. 4 Although some epidemiological studies included such data provided by coaches or athletic trainers,7,15,36 this was not feasible in our study, which relied on retrospective data from medical records across the region. Third, this study did not include a standardized grading system for stress fractures based on imaging findings. The participating medical facilities used various imaging modalities (radiographs, US, CT, and MRI) to diagnose stress fractures; however, we did not have a uniform system to classify injury severity (eg, by MRI grade or cortical involvement). Previous studies have shown that stress fracture severity on imaging correlates with recovery time.11,13,19,20 Integrating imaging-based classifications, such as the grading system by Fredericson et al 12 or Arendt et al, 1 with fracture location (high- vs low-risk) may improve the prediction of RTP for individual patients. A prospective study to systematically evaluate imaging severity and track recovery outcomes would be valuable for further refining RTT guidelines.
Conclusion
This study provides the first population-based epidemiological data on stress fractures among adolescent and recreational athletes in Okinawa, Japan, establishing a regional benchmark for incidence and recovery patterns. In this study, stress fractures occurred most frequently in male soccer players, followed by female basketball players and male baseball players. The most common anatomic sites involved were the tibia, metatarsals, and tarsal bones, in descending order of frequency. Notably, 23% (n = 70/303) of cases were categorized as high-risk stress fractures, among which patellar fractures were the most prevalent and associated with the longest RTT. Furthermore, patellar stress fractures were predominantly observed in young male patients. These findings emphasize the importance of early recognition and site-specific management, particularly for patellar injuries in young male athletes, to optimize rehabilitation timelines.
Footnotes
Appendix
Number of Registered High School Athletes in Okinawa by Sport and Sex in 2018 and 201941
| Sport | Year | Total, n | Male, n | Female, n |
|---|---|---|---|---|
| Basketball | 2018 | 3191 | 1811 | 1380 |
| 2019 | 3015 | 1732 | 1283 | |
| Soccer | 2018 | 2800 | 2492 | 308 |
| 2019 | 2735 | 2427 | 308 | |
| Baseball | 2018 | 3415 | 3415 | 0 |
| 2019 | 3219 | 3219 | 0 | |
| Volleyball | 2018 | 2246 | 1069 | 1177 |
| 2019 | 2154 | 1018 | 1136 | |
| Badminton | 2018 | 2229 | 1173 | 1056 |
| 2019 | 2185 | 1171 | 1014 | |
| Tennis, hard court | 2018 | 1063 | 663 | 400 |
| 2019 | 1032 | 635 | 397 | |
| Handball | 2018 | 1419 | 853 | 566 |
| 2019 | 1332 | 801 | 531 | |
| Track and field | 2018 | 1161 | 767 | 394 |
| 2019 | 1154 | 748 | 406 | |
| Softball | 2018 | 527 | 196 | 331 |
| 2019 | 494 | 172 | 322 | |
| Karate | 2018 | 447 | 267 | 180 |
| 2019 | 456 | 272 | 184 |
Final revision submitted March 29, 2026; accepted April 6, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Institutional Review Board (IRB) at the University of the Ryukyus (IRB No.1619).
Data Availability
The data that support the findings of this study are not publicly available due to privacy and ethical restrictions, but are available from the corresponding author upon reasonable request.