
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are common, yet the specific risk factors that distinguish patients who sustain bilateral injuries from those with unilateral injuries remain poorly characterized. Identifying these factors is crucial for targeted prevention strategies.
Purpose:
To identify demographic and clinical factors associated with bilateral ACL injuries compared with unilateral ACL injuries.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This retrospective cohort study utilized the PearlDiver database to identify patients with unilateral (ACL-ALONE; n = 359,491) or bilateral (ACL-BOTH; n = 3115) ACL injuries. A 2-stage analytical approach was employed. First, demographics and comorbidities were compared between cohorts in the entire population. Second, the analysis was restricted to the female subpopulation to evaluate the specific role of amenorrhea. Multivariable logistic regression models were constructed for both stages to identify factors independently associated with bilateral injury, controlling key confounders.
Results:
Analysis of the full cohort (N = 362,606) revealed that patients with bilateral ACL injuries were significantly younger than those with unilateral injuries (28.8 vs 31.0 years; P < .001). In the full cohort multivariable model, significant independent risk factors for bilateral injury included the 15- to 19-year age group (adjusted odds ratio [aOR], 1.62; 95% CI, 1.35-1.94; P < .001), tobacco use (aOR, 1.24; 95% CI, 1.13-1.35; P < .001), vitamin D deficiency (aOR, 1.31; 95% CI, 1.14-1.50; P < .001), and hypermobility (aOR, 1.83; 95% CI, 1.18-2.82; P = .006). In the female-specific analysis (n = 179,923), amenorrhea was a significant independent factor (aOR, 1.39; 95% CI, 1.16-1.64; P < .001), while hypermobility showed a strong, nonsignificant trend (aOR, 1.65; 95% CI, 0.99-2.77; P = .05).
Conclusion:
This study identifies a distinct and multifactorial risk profile for bilateral ACL injury. Independent risk factors in the overall population include younger age (15-19 years), tobacco use, vitamin D deficiency, and hypermobility. In the female subpopulation, amenorrhea emerged as a significant sex-specific risk factor, associated with a 39% increase in the adjusted odds of bilateral injury. The association for hypermobility, while significant in the full cohort, demonstrated a strong, nonsignificant trend in the female-only analysis, suggesting a complex interaction. These findings indicate that bilateral ACL injury etiology extends beyond biomechanics, implicating a confluence of demographic, endocrine, constitutional, and modifiable lifestyle factors.
Keywords
Anterior cruciate ligament (ACL) injuries represent a significant clinical and public health issue, with profound implications for athletic participation, long-term joint health, and health care costs. While the risk factors for an initial ACL injury, including female sex, neuromuscular deficits, and genetic predisposition, have been extensively studied, the understanding of which patients progress to bilateral ACL injuries remains comparatively limited.1-5,7-10,15,16 Bilateral ACL tears are particularly devastating, as it leads to extended time away from sport and an increased risk of posttraumatic osteoarthritis in both knees.11,14,17,21 Identifying the factors associated with this outcome is a crucial step toward developing targeted prevention strategies.
Current literature on bilateral ACL injury risk is sparse and often focused on isolated or demographic factors.11,14,17,21 Some evidence suggests a potential role for constitutional factors such as generalized joint hypermobility, while other investigations imply a genetic component or younger age at first injury.6,20,22 However, a systematic analysis of the concurrent contribution of modifiable clinical comorbidities is lacking. Furthermore, the systemic endocrine dysfunction characteristic of the female athlete triad and relative energy deficiency in sport (REDs) is a well-established cause of impaired bone health, but its relationship to soft tissue integrity and ligamentous injury is poorly defined.7-10,12,13,15,19 Consequently, a notable gap exists in understanding the comprehensive demographic and clinical profile, encompassing age, sex, constitutional factors, and key comorbidities, that distinguishes patients who sustain bilateral injuries from those with unilateral injuries.
Therefore, the primary objective of this study was to perform a large-scale, comparative analysis to identify the independent risk factors associated with bilateral ACL injuries. Using a national administrative database, we employed a 2-stage analytical approach. 18 First, we compared demographics and a range of clinical comorbidities between unilateral and bilateral injury cohorts in the entire patient population. Second, we conducted a focused analysis on the female subpopulation to evaluate the role of amenorrhea as a sex-specific endocrine risk factor. This methodology aimed to determine whether bilateral injuries are associated with a distinct risk profile involving younger age, hypermobility, substance use, nutritional deficiencies, and, in female patients, menstrual dysfunction. We hypothesized that bilateral ACL injuries would be associated with a distinct demographic and clinical profile compared with unilateral injuries, with specific risk factors including younger age, hypermobility, and in female patients, a history of amenorrhea.
Methods
Study Design and Data Source
This was a retrospective cohort study conducted using the PearlDiver Mariner database, 18 a national, all-payer claims database containing deidentified patient records from 2010 to 2020. The database was queried using International Classification of Diseases, 9th and 10th revisions (ICD-9, ICD-10) and Current Procedural Terminology codes. As this study was conducted at Oregon Health & Science University in 2025 and used only deidentified data, it was granted exemption by the institutional review board.
Patient Selection and Cohorts
The study population comprised patients who underwent treatment for primary ACL injuries. Patients were stratified into 2 mutually exclusive cohorts based on procedural coding history:
Unilateral ACL injury cohort (ACL-ALONE): patients with a single, unilateral ACL injury and no subsequent contralateral injury during the study period (n = 359,491).
Bilateral ACL injury cohort (ACL-BOTH): patients who underwent ACL injury on both knees, indicated by 2 distinct ACL injuries at 2 different time points (n = 3115).
Variable Definition
The primary outcome was cohort assignment (ACL-BOTH vs ACL-ALONE). Demographic factors included age (analyzed as a categorical variable: 15-19, 20-24, 25-29, 30-34 [reference], 35-39, 40-44, 45-49, and 50-54) and sex. Clinical comorbidities of interest were identified using relevant ICD-10 codes and included obesity, underweight, thyroid disorders, tobacco use, alcohol use, vitamin D deficiency, and hypermobility syndrome. Amenorrhea was included as a sex-specific comorbidity for the female subanalysis. A complete list of comorbidity codes is available in Appendix Table A1. All variables of interest were fully populated in the database; therefore, no missing data handling was required.
Statistical Analysis
Statistical analyses were performed using R software within the PearlDiver platform. A 2-stage analytical approach was employed:
Full cohort analysis: descriptive statistics summarized patient demographics and comorbidities. Bivariate comparisons between cohorts were performed using Welch t test for continuous age and chi-square tests for categorical variables. The primary multivariable binary logistic regression model was constructed with age analyzed as a categorical variable (groups: 15-19, 20-24, 25-29, 30-34 [reference], 35-39, 40-44, 45-49, 50-54). This model included age category, sex, and all clinical comorbidities (excluding amenorrhea) as independent variables. A secondary model with age as a continuous variable was run for sensitivity analysis.
Female-specific analysis: the analysis was repeated on the female subpopulation (n = 179,923). The primary model for this cohort used categorical age groups and included amenorrhea alongside the same clinical covariates.
For all regression models, results are reported as adjusted odds ratios (aORs) with 95% CI. A 2-sided P value of <.05 was considered statistically significant for all analyses.
Results
Patient Characteristics
The study identified 359,491 patients in the unilateral ACL injury cohort (ACL-ALONE) and 3115 in the bilateral injury cohort (ACL-BOTH). ICD-10 codes are listed in Appendix Table A2. The bilateral cohort was significantly younger (mean age, 28.8 ± 12.4 years; P < .001). The distribution across age categories differed significantly between groups (P < .001), with a higher proportion of bilateral injuries in the 15- to 19-year age range (30.2% vs 23.8%). In unadjusted analyses, the prevalence of several clinical factors was significantly higher in the bilateral injury cohort, including amenorrhea (8.9% vs 6.3%; P < .001), tobacco use (26.5% vs 24.5%; P = .01), vitamin D deficiency (18.2% vs 15.0%; P < .001), and hypermobility (0.7% vs 0.3%; P = .002). Obesity, underweight, and thyroid disorders did not differ significantly between cohorts (Table 1). ICD-10 codes are listed in Appendix Table A1.
Patient Demographics and Clinical Characteristics a
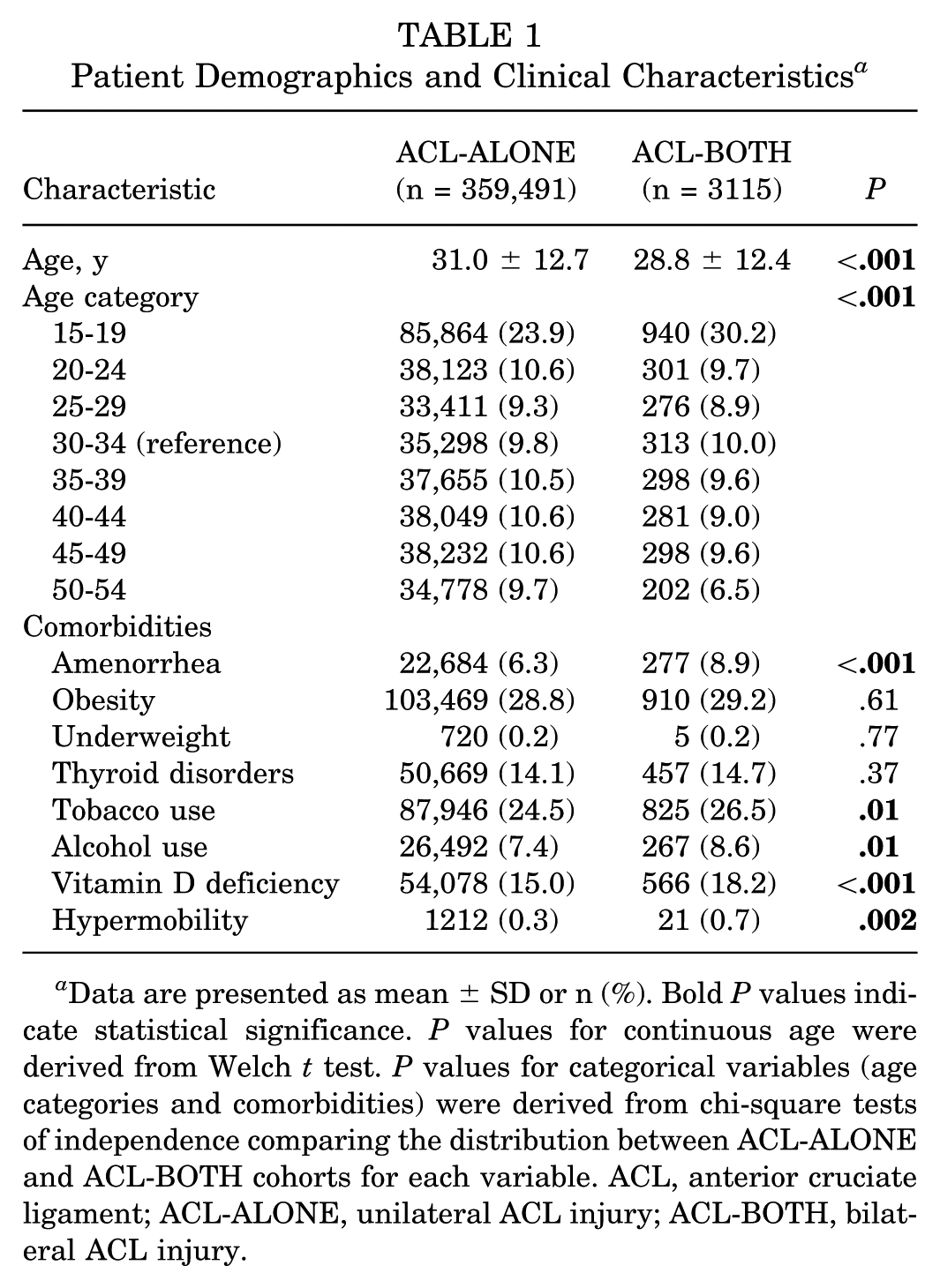
Data are presented as mean ± SD or n (%). Bold P values indicate statistical significance. P values for continuous age were derived from Welch t test. P values for categorical variables (age categories and comorbidities) were derived from chi-square tests of independence comparing the distribution between ACL-ALONE and ACL-BOTH cohorts for each variable. ACL, anterior cruciate ligament; ACL-ALONE, unilateral ACL injury; ACL-BOTH, bilateral ACL injury.
Independent Risk Factors in the Full Cohort
In the full cohort multivariable model, significant independent risk factors for bilateral ACL injury included the youngest age category (15-19 years: aOR 1.62; 95% CI, 1.35-1.94; P < .001), tobacco use (aOR, 1.24; 95% CI, 1.13-1.35; P < .001), vitamin D deficiency (aOR, 1.31; 95% CI, 1.14-1.50; P < .001), and hypermobility (aOR,1.83; 95% CI, 1.18-2.82; P = .006). Older age categories (40-44 and 50-54) were associated with significantly decreased odds. Male sex was associated with slightly lower odds of bilateral injury (aOR, 0.91; 95% CI, 0.85-0.98; P = .01). Obesity, underweight, and thyroid disorders were not independent risk factors (Table 2).
Unadjusted Odds Ratios for Bilateral ACL Injury a
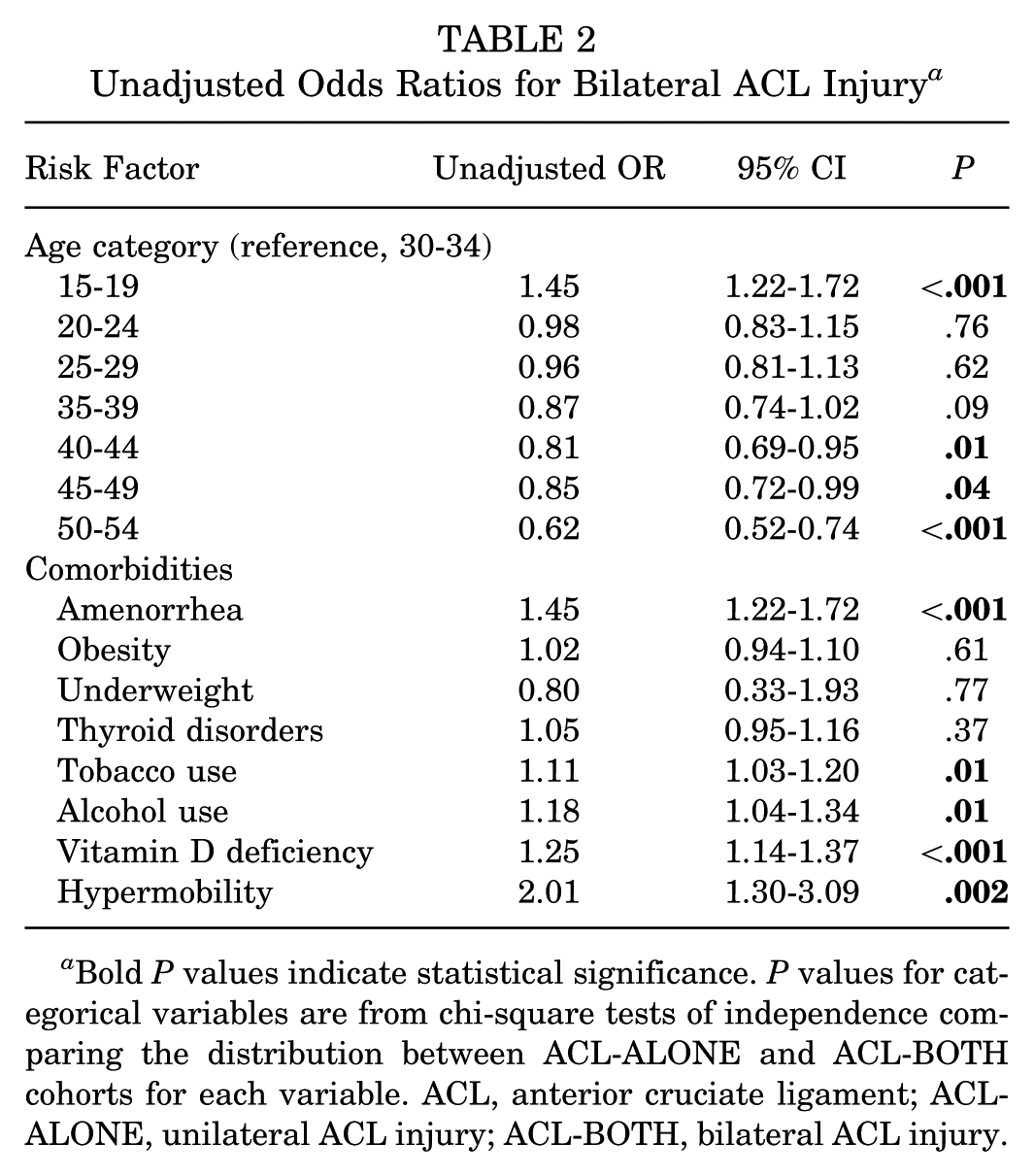
Bold P values indicate statistical significance. P values for categorical variables are from chi-square tests of independence comparing the distribution between ACL-ALONE and ACL-BOTH cohorts for each variable. ACL, anterior cruciate ligament; ACL-ALONE, unilateral ACL injury; ACL-BOTH, bilateral ACL injury.
Female-Specific Analysis and the Role of Amenorrhea
In female subpopulation analysis (n = 179,923), a diagnosis of amenorrhea was a significant independent factor of bilateral ACL injury (aOR, 1.39; 95% CI, 1.16-1.64; P < .001) after controlling for age, obesity, tobacco use, vitamin D deficiency, and hypermobility. In this female-only model, hypermobility demonstrated a strong association that did not reach statistical significance (aOR, 1.65; 95% CI, 0.99-2.77; P = .05). The associations for younger age, tobacco use, and vitamin D deficiency remained consistent with the full cohort model (Table 3).
Multivariable Logistic Regression: Adjusted Factors of Bilateral ACL Injury a
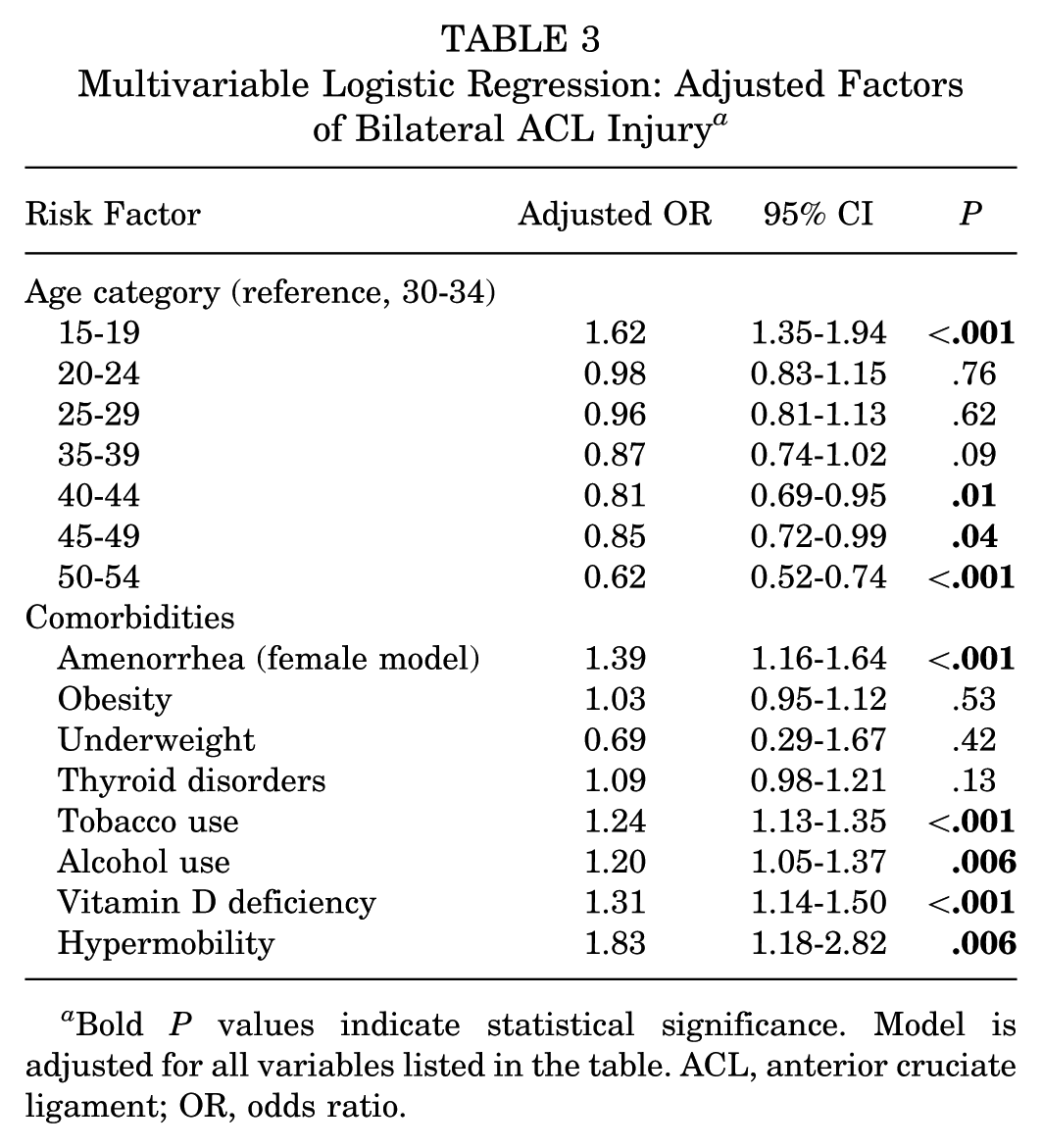
Bold P values indicate statistical significance. Model is adjusted for all variables listed in the table. ACL, anterior cruciate ligament; OR, odds ratio.
Discussion
This large-scale comparative analysis identifies a distinct multifactorial risk profile for bilateral ACL injury, differentiating it from unilateral injury. The primary findings reveal that bilateral injuries are independently associated with adolescent age, tobacco use, vitamin D deficiency, hypermobility, and in female patients, amenorrhea. This risk profile extends beyond the traditional biomechanical and neuromuscular paradigm for primary ACL injury, implicating a confluence of demographic, endocrine, constitutional, and modifiable lifestyle factors.
The most novel finding of this study is the identification of amenorrhea as a significant, independent risk factor for bilateral ACL injury in the female subpopulation. While the association between amenorrhea and impaired bone health is well-established within the REDs, this is among the first studies to link this endocrine dysfunction specifically to bilateral soft tissue injury. The observed 39% increase in adjusted odds suggests that the hypoestrogenic state and broader metabolic dysfunction of low energy availability may contribute to a systemic vulnerability in ligamentous integrity. This expands the clinical concern for athletes with menstrual dysfunction beyond bone stress injuries to include a potentially heightened risk for severe, bilateral ligamentous ruptures. This finding necessitates a paradigm shift in clinical evaluation, positioning a history of amenorrhea as a critical element in the risk stratification of female athletes.
Our results also reinforce and quantify the role of other significant, yet modifiable, risk factors. Tobacco use and vitamin D deficiency emerged as strong independent risk factors. Nicotine's vasoconstrictive effects and impairment of collagen synthesis provide a plausible biological mechanism for its association with bilateral injury. Similarly, vitamin D's role in muscle function, proprioception, and inflammatory regulation may explain its link to injury susceptibility. The association with hypermobility in the full cohort underscores the importance of constitutional collagen disorders, suggesting an inherent connective tissue vulnerability. The attenuation of this association to a nonsignificant trend in the female-only model may reflect reduced statistical power or genuinely weaker effect in female patients, warranting further investigation.
These findings argue compellingly for a holistic, multifactorial approach to ACL injury prevention, particularly for athletes identified as high risk for a first injury. Screening protocols should be expanded beyond biomechanical assessment to include evaluation for menstrual dysfunction, nutritional status (specifically vitamin D), tobacco use, and hypermobility. For female athletes, a history of amenorrhea should trigger a comprehensive evaluation for low energy availability and referral to a multidisciplinary team. Integrating screening for these factors into clinical practice represents a crucial step toward targeted prevention for this devastating injury pattern. Future prospective studies are needed to establish causality and to investigate whether interventions addressing these risk factors such as nutritional counseling, smoking cessation, or vitamin D supplementation, can reduce the incidence of primary or subsequent ACL injury.
Limitations
This study has limitations inherent to its retrospective design and use of administrative data. The reliance on ICD codes for comorbidities may lead to misclassification or underreporting, particularly for conditions like amenorrhea. The database lacks detailed information on athletic activity, training load, biomechanics, diet, and hormonal levels, which are important potential confounders. While multivariable analysis controlled for numerous factors, residual confounding from unmeasured variables is possible. Importantly, our bilateral cohort may underrepresent the true population of patients with bilateral ACL injuries, as the strict criteria of having 2 separate ACL injuries hospital encounters. The number of patients with bilateral ACL injuries was lower compared to the unilateral cohort, which may have limited statistical power to detect smaller effect sizes. Furthermore, the database is unable to evaluate surgical factors that may influence contralateral risk, such as graft type and surgical techniques, as a potential modifier of contralateral injury rates. Other prospective studies should include these surgical variables to provide a more complete understanding of bilateral injury risk. Finally, the data establish association but cannot prove causation.
Conclusion
This large-scale comparative analysis identifies a distinct and multifactorial risk profile associated with bilateral ACL injuries. Significant independent risk factors include adolescent age (15-19 years), tobacco use, vitamin D deficiency, and generalized joint hypermobility. Within the female subpopulation, a diagnosis of amenorrhea emerged as a robust and independent sex-specific risk factor. These findings suggest that the etiology of bilateral ACL injury extends beyond isolated biomechanical causes, implicating a confluence of demographic, endocrine, constitutional, and modifiable lifestyle factors. Consequently, clinical risk assessment and prevention strategies should be expanded for at-risk athletes, and targeted, multidisciplinary interventions should be implemented to mitigate the risk of this devastating injury pattern.
Footnotes
Appendix
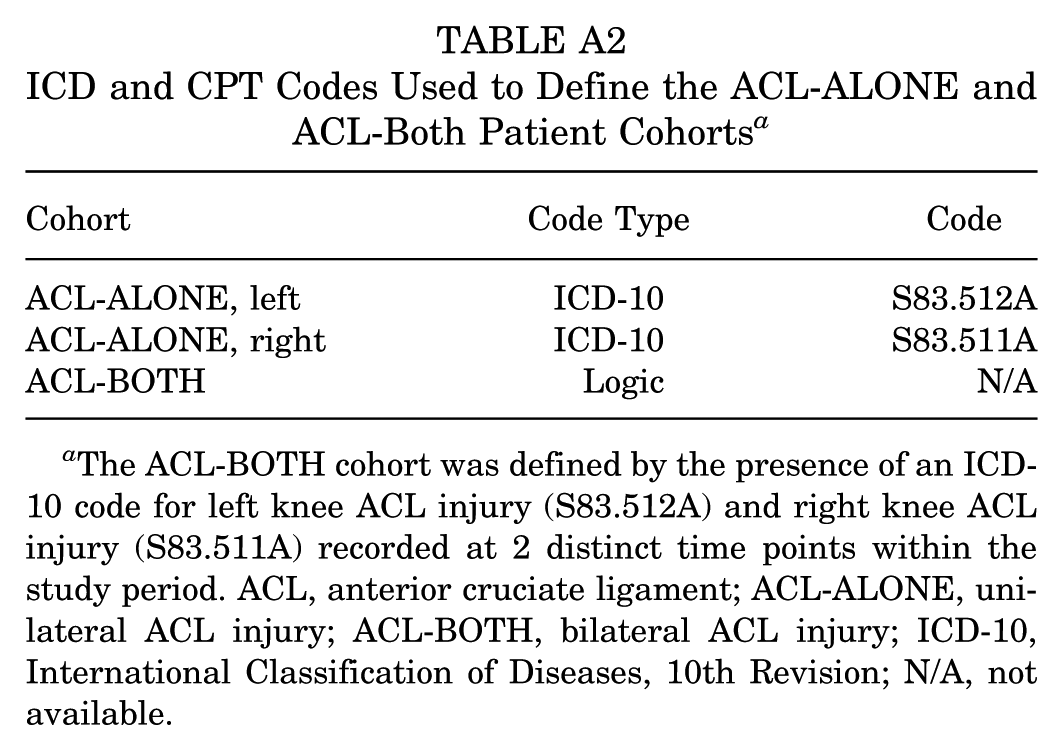
ICD and CPT Codes Used to Define the ACL-ALONE and ACL-Both Patient Cohorts a
| Cohort | Code Type | Code |
|---|---|---|
| ACL-ALONE, left | ICD-10 | S83.512A |
| ACL-ALONE, right | ICD-10 | S83.511A |
| ACL-BOTH | Logic | N/A |
The ACL-BOTH cohort was defined by the presence of an ICD-10 code for left knee ACL injury (S83.512A) and right knee ACL injury (S83.511A) recorded at 2 distinct time points within the study period. ACL, anterior cruciate ligament; ACL-ALONE, unilateral ACL injury; ACL-BOTH, bilateral ACL injury; ICD-10, International Classification of Diseases, 10th Revision; N/A, not available.
Final revision submitted March 31, 2026; accepted April 7, 2026.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Oregon Health & Science University.