
Abstract
Background:
Meniscal pathology often presents with concomitant anterior cruciate ligament (ACL) injury. During ACL reconstruction (ACLR), “cycling the knee” has been shown to help reduce graft creep after femoral fixation. Pullout of successfully deployed all-inside meniscal repair implants after knee “cycling” has been observed, but is sparsely documented in the setting of ACLR with concomitant meniscal pathology.
Purpose:
To investigate the frequency of and contributions to intraoperative meniscal repair failure during concurrent ACLR.
Study Design:
Cross-sectional study.
Methods:
A brief survey was distributed to members of the Pediatric Research in Sports Medicine Society. Participants met the inclusion criteria if they self-identified as orthopaedic surgeons who perform ACLR. The primary objective of the survey was to assess surgeons’ experience with meniscal implant failure and its relationship to practice patterns (ie, cycling the knee).
Results:
Of the 52 surveys distributed, 44 orthopaedic surgeons completed the survey after 3 months of data collection, representing a 84.6% response rate. The majority of participants reported treating patients primarily in the second or third decade of life. Participants unanimously reported they would address the meniscal pathology before performing the ACLR. Thirty-three (75%) participants reported cycling the knee before graft fixation. Nineteen (43.2%) respondents endorsed reinspection of the meniscus after ACL graft fixation, and among them, 7 (36.8%) reported at least 1 instance of meniscal implant failure. Meniscal implant failure was associated with fewer years in practice: surgeons who reported implant pullout had a median of 2 to 5 years in practice, while those who did not report implant pullout had a median of 5 to 10 years in practice (P = .027). No other factors were associated with meniscal implant failure. The sample size was insufficient to analyze the possible association of implant failure with cycling alone or hyperflexion alone.
Conclusion:
Meniscal repair with concomitant ACLR is a common surgery for orthopaedic sports medicine specialists. Although these procedures often result in favorable outcomes, this study concludes that failure of meniscal implants does occur and may be more common early in practice. Therefore, further investigation into optimal procedural strategies to address meniscal tears in the setting of ACLR is necessary.
Meniscal pathology seen with concomitant anterior cruciate ligament (ACL) injury has been reported in up to 60% of cases.1,2,3,9,11,19 Meniscal repair in the setting of ACL reconstruction (ACLR) is often performed with favorable long-term outcomes.10,20,21,15,24,25 During ACLR creep of the graft has been well studied during graft tensioning, but the methods of tensioning and the amount of tension vary significantly.8,13,14,18“Cycling the knee” has been shown to help diminish creep after femoral fixation during ACLR; however, there is a paucity of literature on when to cycle the knee, how much to cycle, and through what range of motion. 5
Pullout of successfully deployed all-inside meniscal repair implants after knee cycling has been observed, requiring re-repair, but is sparsely documented (Figure 1). It is unknown whether tissue quality, implant type, repair configuration, or the amount and range of knee cycling are the culprits. Meniscal implant failures after ACLR may be more common than we think. Studies have shown that extending the knee beyond 120° of flexion places undue tension on the posterior meniscocapsular junction.12,16,17 Therefore, the effects of cycling the knee in ACLR on concurrent meniscal repairs necessitate further biomechanical and clinical investigation.
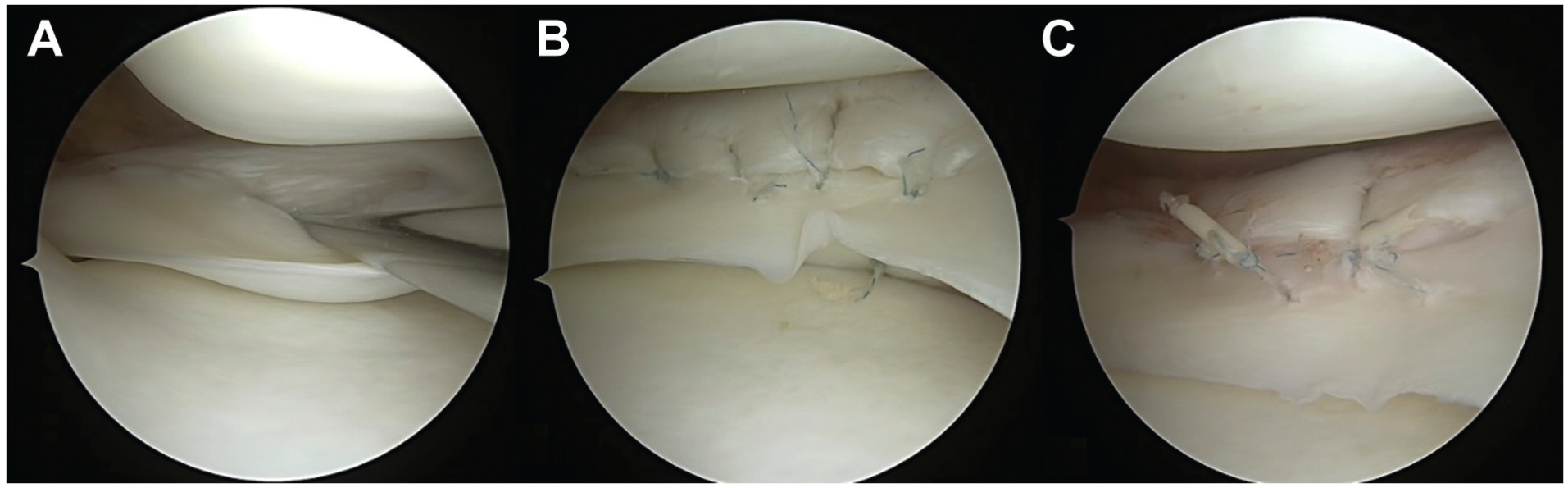
(A) Medial meniscal posterior horn vertical tear. (B) All inside repair. (C) Pullout of successfully deployed all-inside meniscal repair implants after “cycling” of the right knee.
This study aimed to survey Pediatric Research in Sports Medicine (PRiSM) Society members on the current trends and practices in ACLR with concurrent meniscal repair, particularly as they relate to cycling the knee and meniscal repair implant pull-out. The secondary purpose of this study was to characterize cycling techniques, frequency of meniscal repair reinspection, type of meniscal implant used, and order of operative steps in ACLR with concurrent meniscal repair. We hypothesized that respondents would report infrequent meniscal implant pullout upon reinspection after ACLR and knee cycling.
Methods
Study Design
This was a cross-sectional survey-based study distributed to 52 members of PRiSM. An institutional review board exemption was obtained before the survey was disseminated. Before accessing the survey, each participant acknowledged and provided consent to participate after a description of the study and the survey's purpose. All survey responses were anonymous and did not contain any identifiers. Standardized guidelines for reporting surveys using the CHERRIES (Checklist for Reporting Results of Internet E-Surveys) checklist were utilized. 4
Procedures
Following PRiSM's approval, the online survey was distributed to PRiSM members via email in August of 2024. The survey was conducted through REDCap (Research Electronic Data Capture, Vanderbilt University). After the initial distribution of the survey, 3 reminder emails were sent to participants to increase the response rate. Responses from the survey were accepted for 3 months. The survey was voluntary, and no incentives were offered.
Survey Design
The purpose of the survey was to elucidate the methodology for performing ACLR with concomitant meniscal repair, including the use and unintended effects of knee cycling. The survey was developed in collaboration among 5 orthopaedic surgeons with backgrounds in pediatric sports medicine. The survey was distributed to orthopaedic surgeons who indicated that they perform ACLRs.
The survey consisted of up to 38 items with branching logic in a fixed order. Survey items were related to the characteristics of the surgeon's practice, training, experience, and techniques related to ACLR and meniscal repair. The question formats included multiple-choice, select-all-that-apply, checkbox, and free-text. The survey was estimated to take 10 to 15 minutes to complete. Respondents could review answers before submission, but were limited to a single submission. Only complete questionnaires were used in the final analysis.
The questions relating to the surgeon's practice captured the percentage of their patient population that was adult versus pediatric, the age range of their ACLR patients, their region of practice, and the setting of their practice. The survey also captured information regarding the surgeon's fellowship training and years in practice. Respondents were asked about their preferred graft type for ACLR, their preferred order of concurrent meniscal repair and ACLR, their preferred order of concurrent medial and lateral meniscal repair, their preferred implant for meniscal repair and frequency of use, and their preferred suture technique for all inside repairs of vertical posterior meniscal horn tears and frequency of use. Additionally, they were asked whether they hyperflex the knee when drilling the femoral tunnel for the ACL graft, whether they cycle the knee before final fixation of the ACL graft, how many cycles they perform, and to what degree of flexion. Finally, the respondents were queried about when and whether they reinspect the meniscal repair, whether they have ever witnessed a meniscal repair implant pullout upon reinspection, and whether they associate any particular implant with a higher propensity to fail. A copy of the survey is available as supplementary material.
Data Analysis
REDCap survey data were exported to an Excel spreadsheet (Microsoft Excel 2013; Microsoft), and analyses were performed by an independent biostatistician. Responses to survey questions were reported as frequencies and percentages. Descriptive statistics were calculated. Analysis of interval variables was performed using a Mann-Whitney U nonparametric test, and analysis of categorical variables was performed using the χ2 test or the Fisher exact test, as appropriate. A power analysis was performed. An alpha level was set at P < .05 to declare significance. All analyses were performed using SPSS Version 27 (IBM Corp).
Results
Of the 52 surveys distributed, 44 were completed and included in the analysis, representing an 84.6% response rate. The majority of respondents (97.7%) were fellowship-trained in pediatric orthopaedics, sports medicine, or pediatric sports medicine (Table 1). There was a representative distribution of practice location across the Northeast, Southern, and Western United States. Over 70% of respondents (31 of 44) reported 5 or more years of experience. All respondents worked with the pediatric population, with 31.8% (14 of 44) also working with adult patients. Most participants reported treating patients primarily in the second or third decade of life.
Respondent and Practice Characteristics (N = 44) a
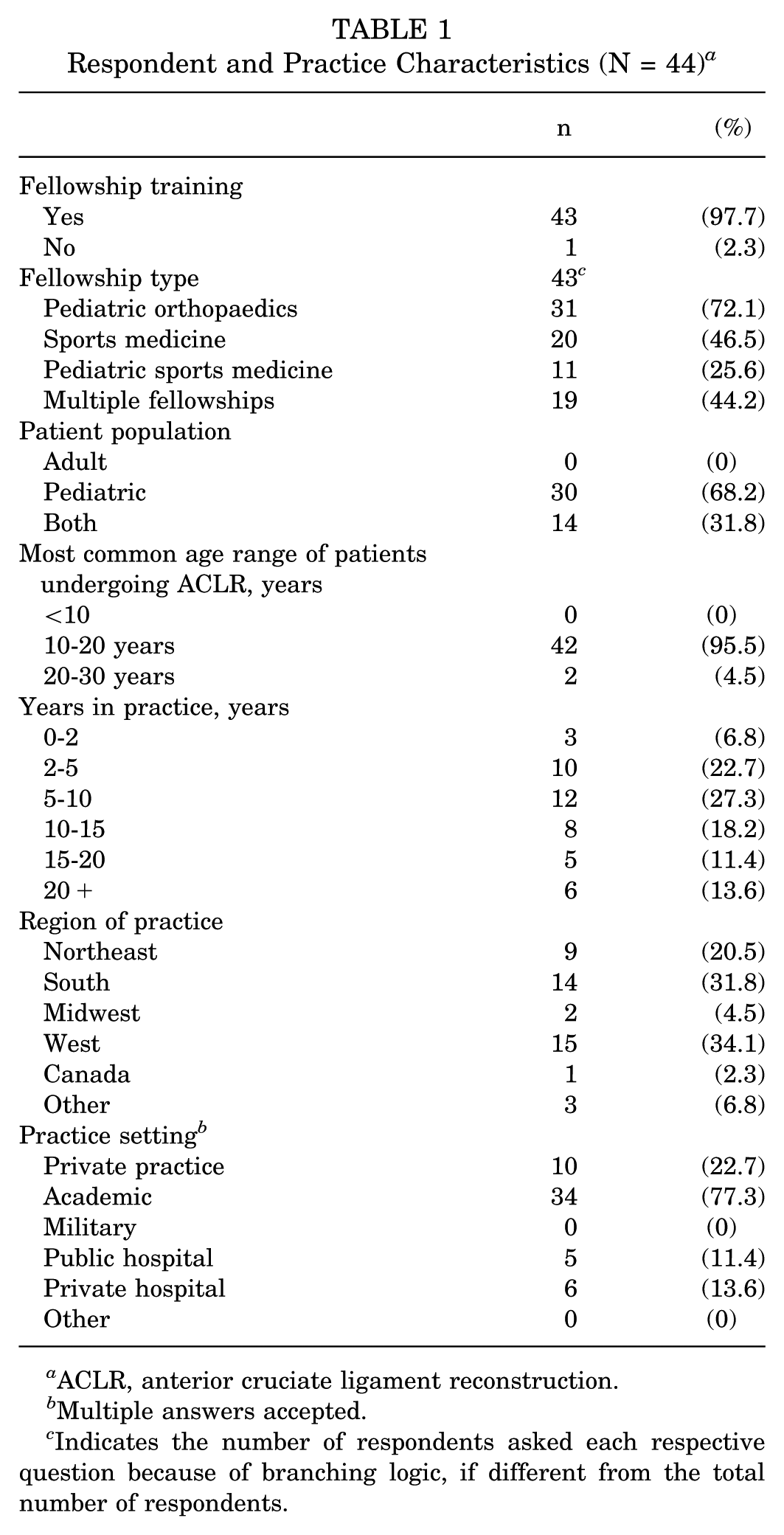
ACLR, anterior cruciate ligament reconstruction.
Multiple answers accepted.
Indicates the number of respondents asked each respective question because of branching logic, if different from the total number of respondents.
The 3 most frequently reported ACLR graft types were quadriceps autograft (all soft tissue), patellar tendon bone-to-bone autograft, and iliotibial band physeal sparing (Table 2). The majority of surgeons (34/44 [77.3%]) did not report hyperflexing the knee during femoral tunnel drilling. Participants unanimously reported they would address the meniscal pathology before performing the ACLR. If repairs are indicated for both medial and lateral meniscus, the majority (28/44 [63.6%]) had no preference in the order of repair (Table 3). For an all-inside repair of a vertical tear of the posterior meniscal horns, most reported that they would address it with a vertical mattress technique (32/44 [72.7%]).
ACLR Preferences (N = 44) a
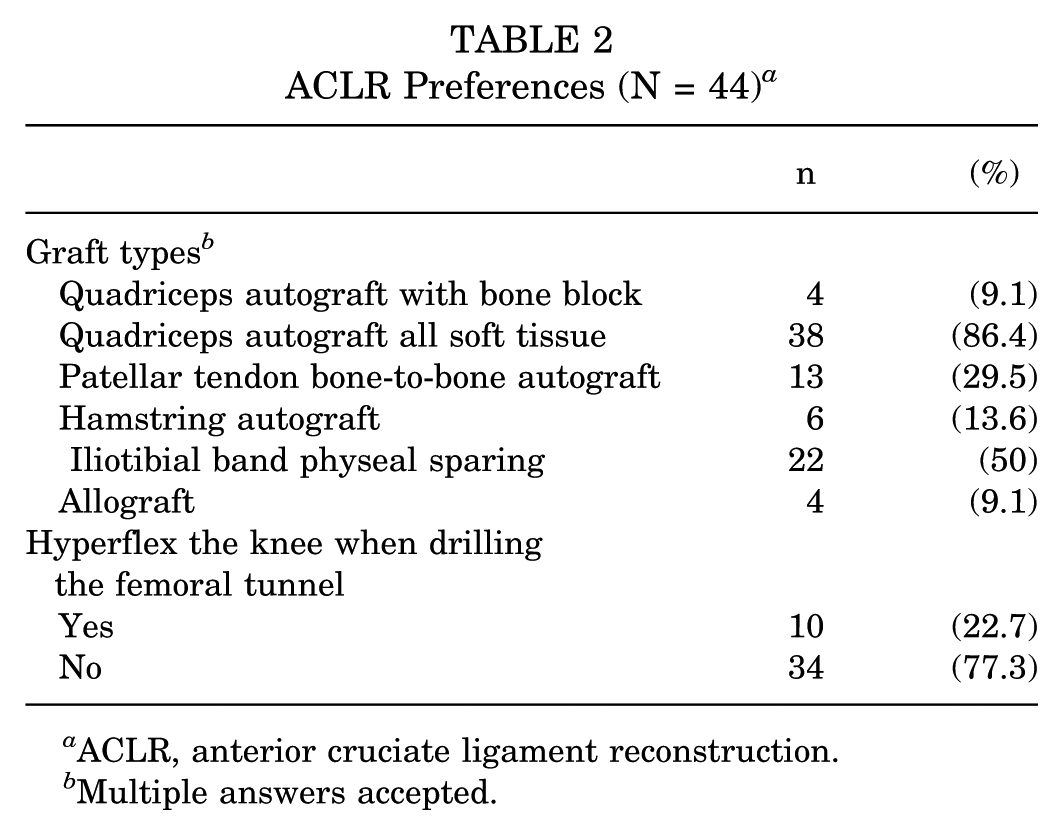
ACLR, anterior cruciate ligament reconstruction.
Multiple answers accepted.
Meniscal Repair Preferences (N = 44) a
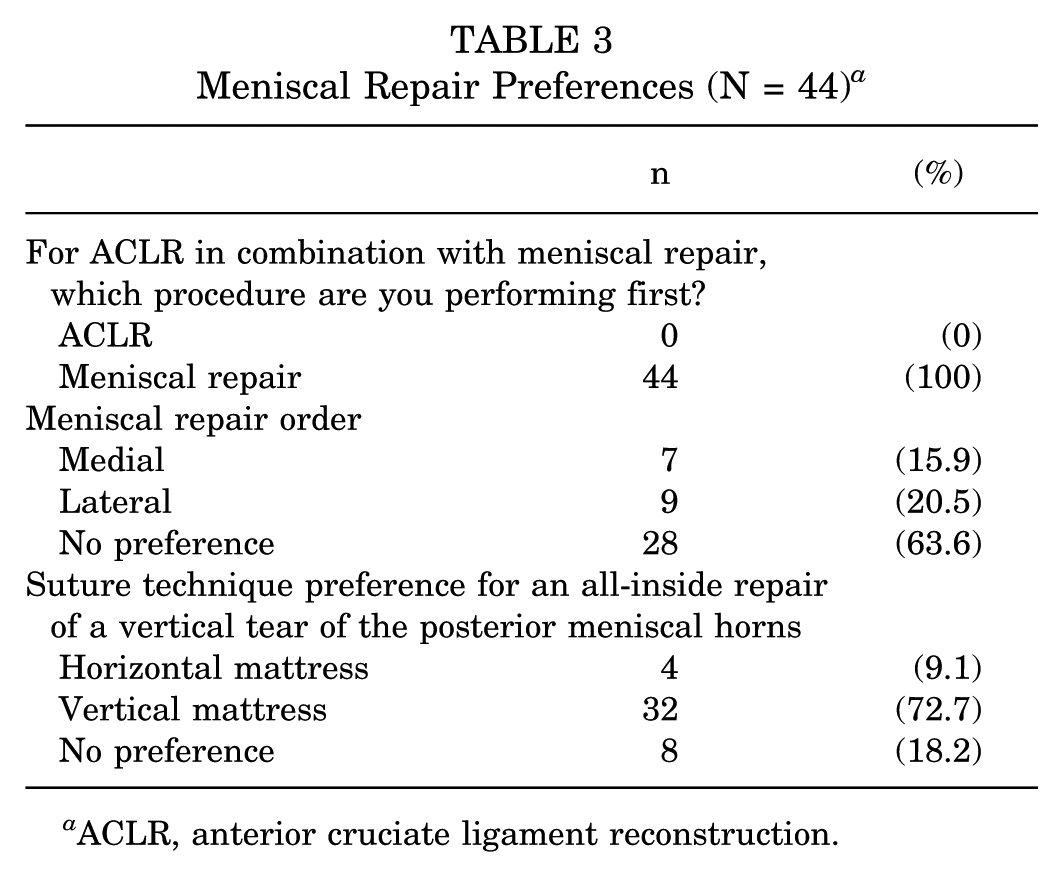
ACLR, anterior cruciate ligament reconstruction.
Of the 44 participants, 75% reported cycling the knee before final graft tensioning and fixation in ACLR. Of those who reported cycling the knee, most perform between 6 and 10 cycles or 11 and 20 cycles. There was a similar distribution of respondents who reported flexing the knee between 60° and 90° and 90° and 120° when cycling (Table 4). Only 19 (43.2%) of respondents reported reinspection of the meniscal repair after ACLR. Of those 19 respondents, 73.7% reported reinspection of the meniscus after cycling and final fixation of the ACL graft. In contrast, the remaining respondents did not cycle the knee but did reinspect after final fixation of the ACL graft (Table 5). Following reinspection of the meniscal repair, 7 (36.8%) participants reported having observed meniscal implant pullout at least once.
Knee Cycling Preferences (N = 44) a
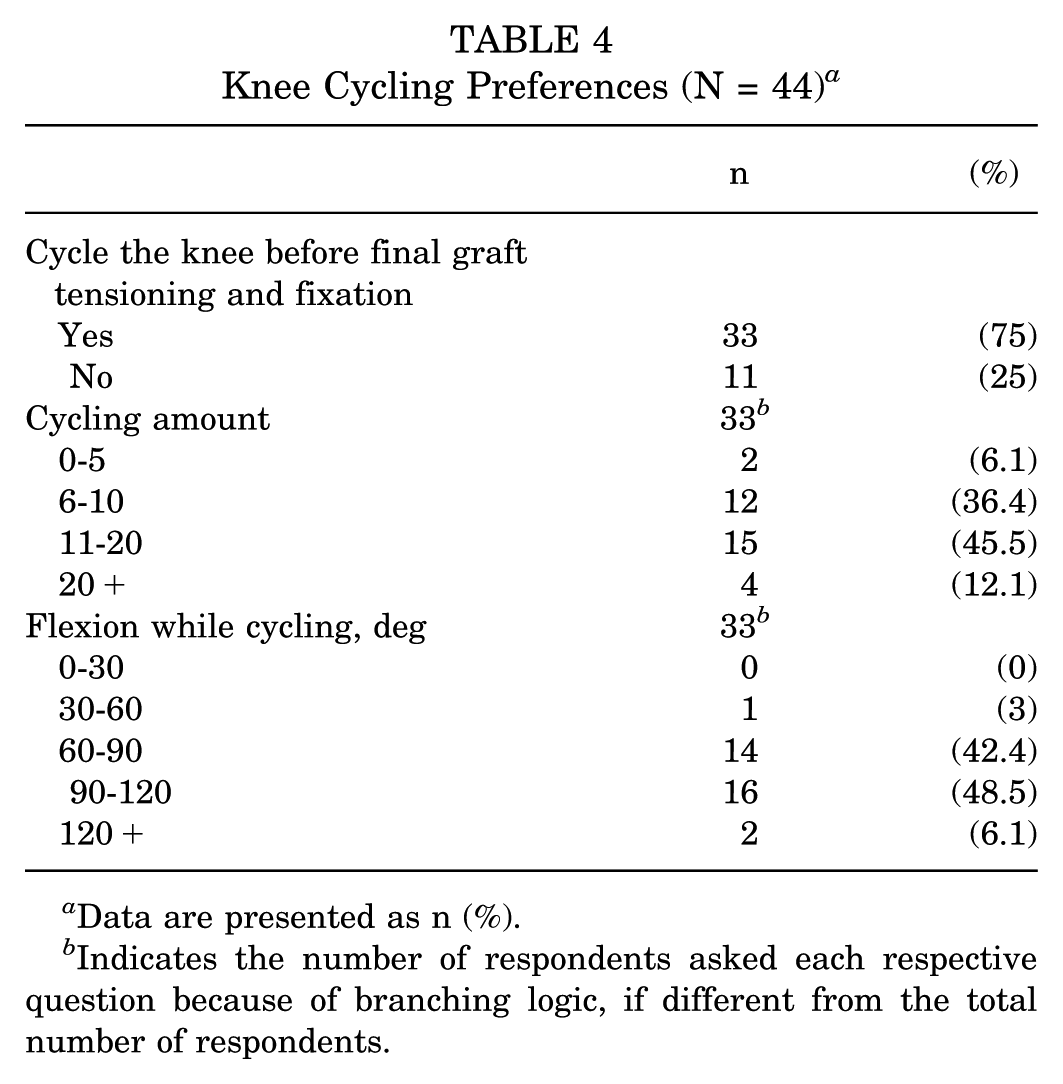
Data are presented as n (%).
Indicates the number of respondents asked each respective question because of branching logic, if different from the total number of respondents.
Meniscal Reinspection and Implant Failure (N = 44) a
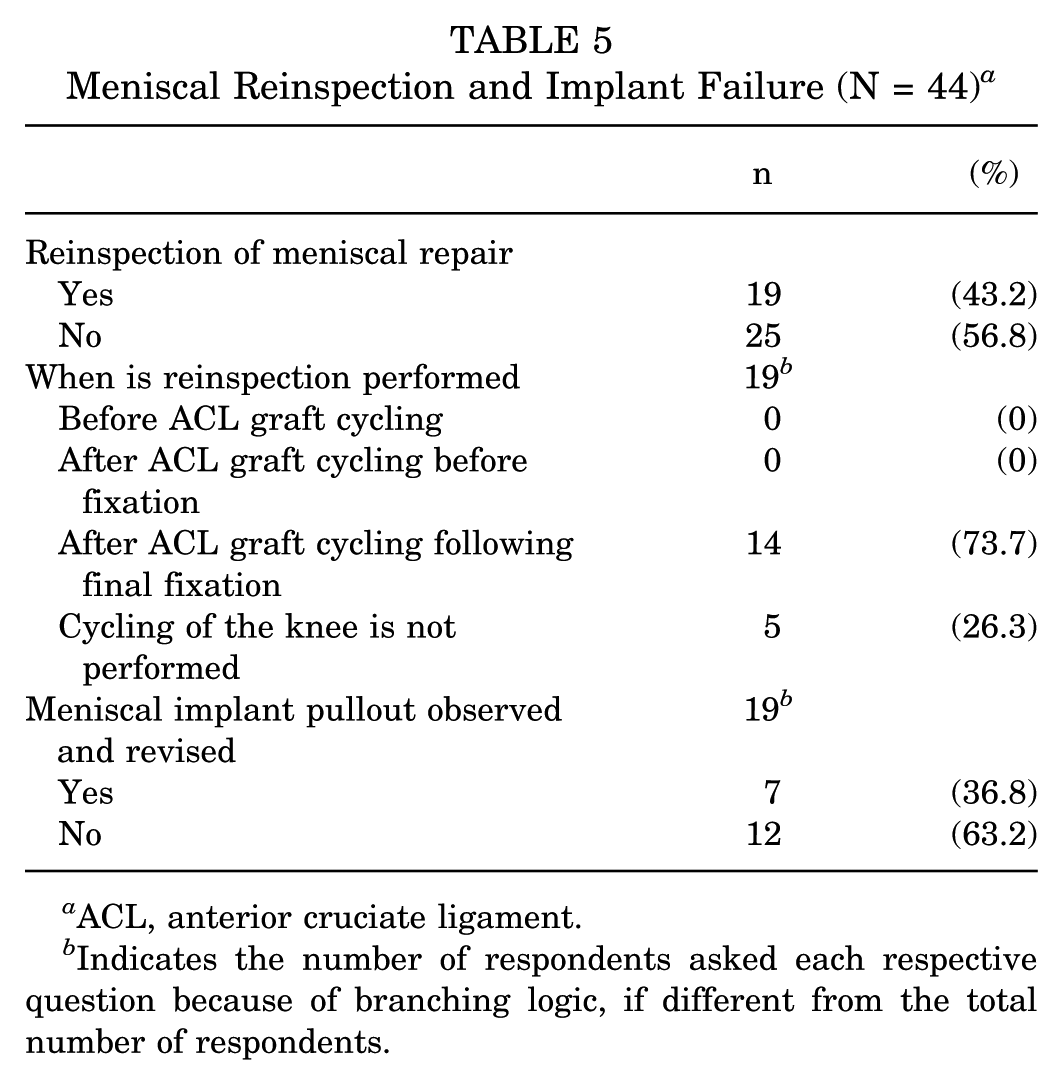
ACL, anterior cruciate ligament.
Indicates the number of respondents asked each respective question because of branching logic, if different from the total number of respondents.
The top 3 preferred meniscal implants included the Arthrex Meniscal Fiberstitch, Smith & Nephew Fast-Fix Flex, and Smith & Nephew Fast-Fix 360 (Table 6). Respondents who reported using >1 implant were asked whether they noticed a higher failure rate with 1 implant than with the others. Of the 6 respondents who used multiple implants, 83.3% reported a higher implant pullout rate with Arthrex Meniscal Fiberstitch, with 1 respondent reporting a higher pullout rate with Smith & Nephew Fast-Fix Flex.
Preferred Meniscal Implant and Implant Failure a
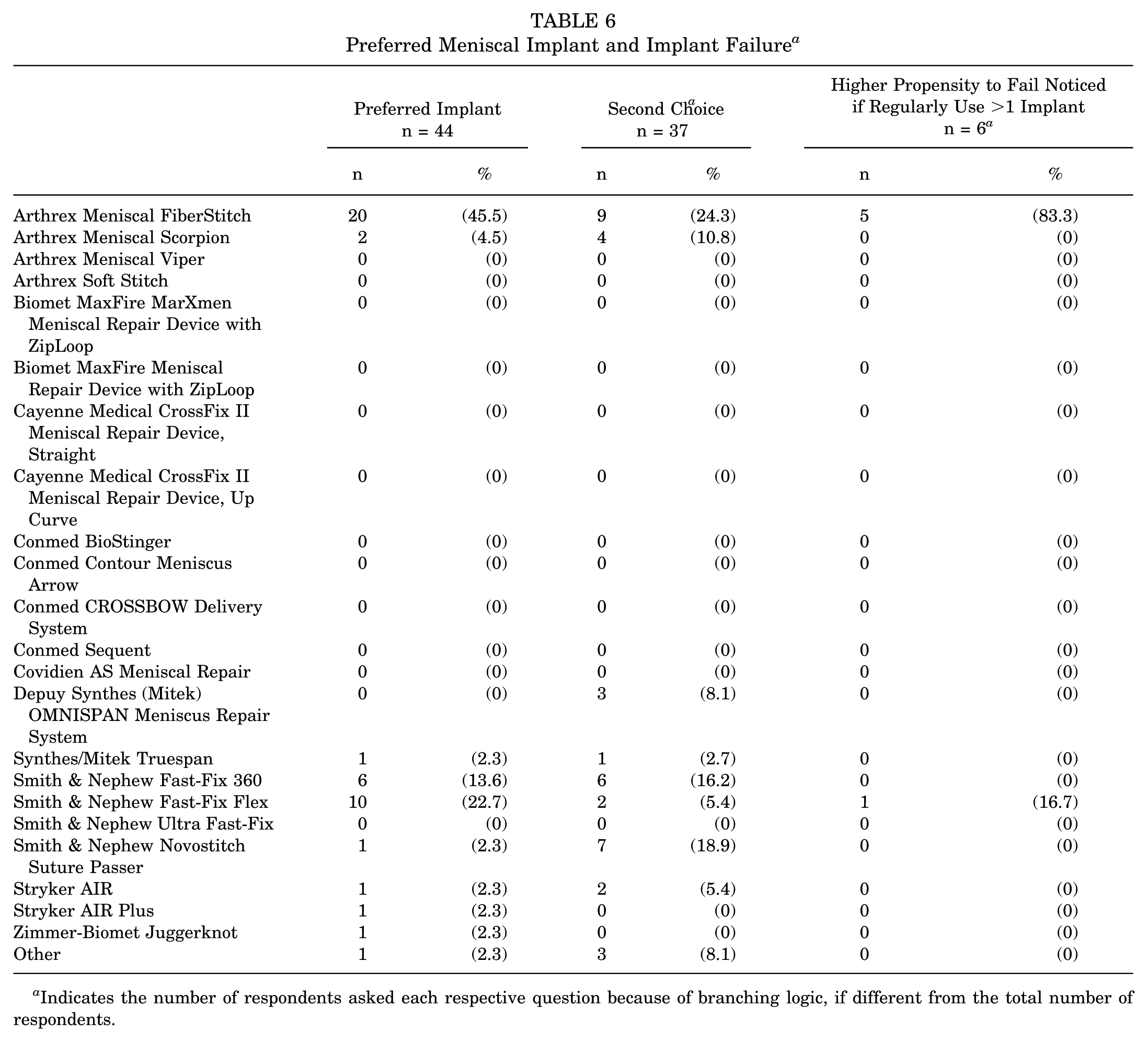
Indicates the number of respondents asked each respective question because of branching logic, if different from the total number of respondents.
There were no associations between the decision to hyperflex the knee during drilling of the femoral tunnel, cycling the knee, or reinspection of the meniscal repair and respondents’ practice characteristics (Table 7). Additionally, no associations were observed between the rate of meniscal implant pullout and respondents’ practice characteristics or techniques (Table 8).
Associations Between Practice Characteristics and Hyperflexing, Cycling, and Reinspection a
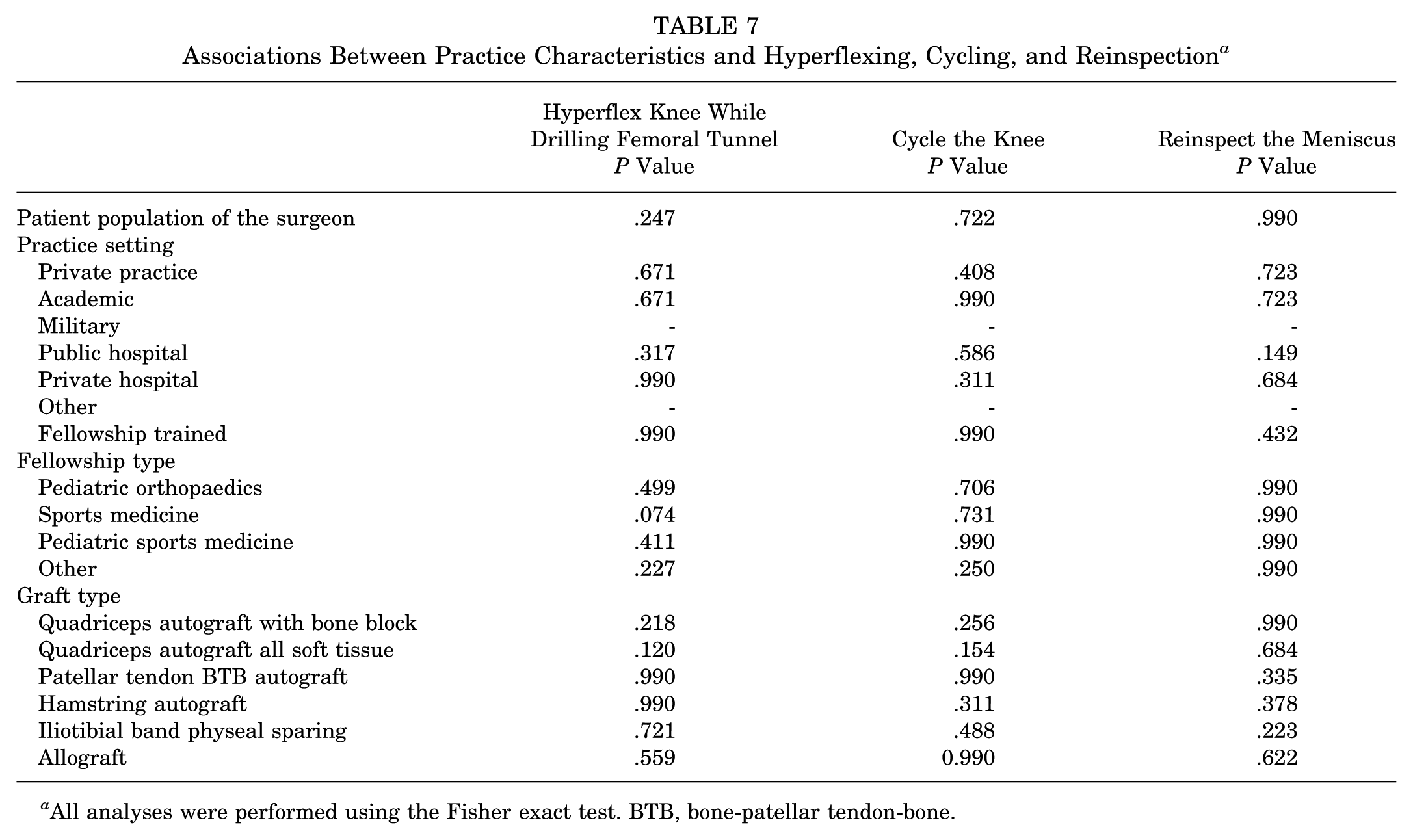
All analyses were performed using the Fisher exact test. BTB, bone-patellar tendon-bone.
Associations Between Practice Characteristics and Meniscal Repair Revisions a
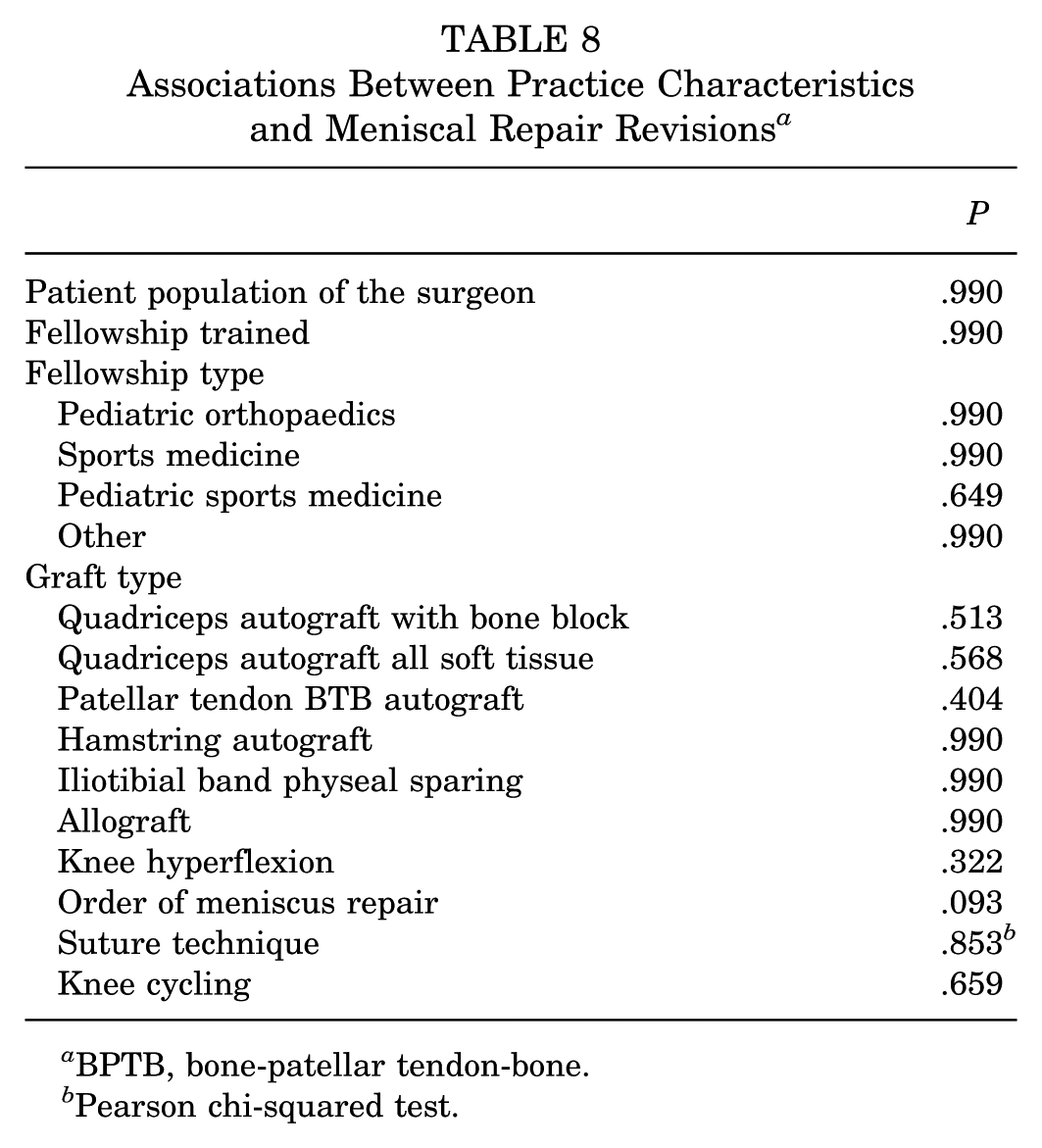
BPTB, bone-patellar tendon-bone.
Pearson chi-squared test.
In further analysis, the outcome of meniscal repair implant pullout was significantly associated with fewer years in practice, where surgeons who reported implant pullout had a median of 2 to 5 years in practice, while those who did not report implant pullout had a median of 5 to 10 years in practice (P = .027). There were no significant associations between meniscal implant pull-out and the number of knee cycles or the degree of knee flexion during cycling (P = .260 and P = .424, respectively).
Table 9 summarizes the breakdown of surgical techniques and preferences by the surgeon's years in practice.
Surgical Technique by Years in Practice a
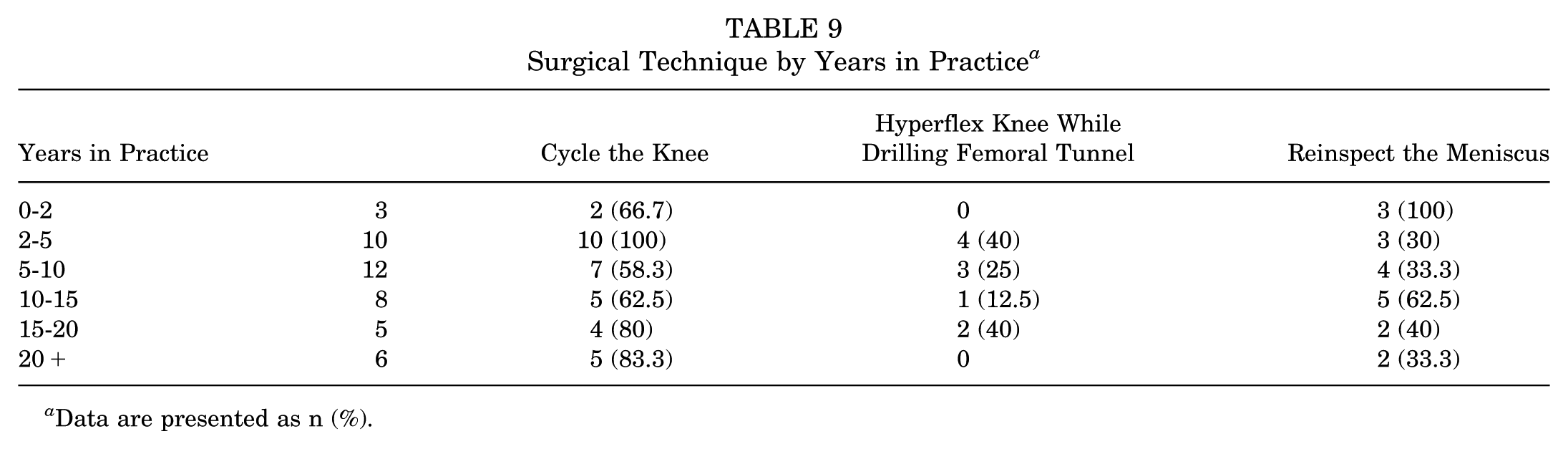
Data are presented as n (%).
A post hoc power analysis showed that, to achieve 80% power to evaluate meniscal implant failure as it relates to knee cycling, a sample size of 245 respondents per group would be required.
Discussion
Our goal was to identify the frequency and contributing factors of meniscal repair implant pullout during ACLR, which, based on the findings, may be associated with fewer years in practice. Although no associations were observed secondary to hyperflexing or cycling the knee, the study would need a larger sample size to more confidently report these associations. However, failures were still identified by about 37% of those who reinspected the knee after “knee cycling” at least once. This percentage may differ if everyone reexamined the meniscal repairs after final graft fixation post “knee cycling.” These findings reiterate the need to “take a second look” and reinspect meniscal repairs after final graft fixation, as repair failure may be more prevalent than we see. While meniscal implant failure after final ACL graft fixation is a rare finding, it is relatively easy to identify. It should therefore ideally be part of standard scope/ACLR techniques in most cases. The paucity of literature on this topic makes it vital to delve deeper into knee cycling during ACLR to identify and assess its clinical relevance to meniscal implant failure.
Knee cycling during ACLR is commonly used to help reduce graft creep after femoral fixation. A recent study evaluated the degree of tensile loosening of the ACL autologous hamstring graft after intraoperative knee cycling. 5 They found that the magnitude of loosening decreased with each consecutive round of 10 knee cycles intraoperatively before final ACL graft fixation, up to a combined 30 cycles. They suggest that 30 knee cycles may be adequate to maintain initial graft tension in ACLR, although they did not evaluate clinical outcomes. A similar study assessed the number of knee cycles required to achieve a stable hamstring autograft length in situ during ACLR. 6 They found a significant elongation of graft length from 0 to 30 cycles, but stabilization of tendon length after 30 cycles. A third study evaluating in situ pretensioning of semitendinosus and gracilis grafts for ACLR with knee cycling found that minimization of graft creep was achieved after 25 cycles. 7 Notably, the majority of literature on knee cycling describes the use of hamstring grafts. In contrast, the majority of respondents in this study reported the use of quadriceps autograft or the iliotibial band physeal sparing technique. All 3 of the aforementioned studies flexed the knees during cycling from 0° to 110°. The clinical application of these findings differs from the current practice reported by respondents in our study: only 12.1% (4 of 33) regularly perform ≥20 knee cycles. Of the 33 respondents who cycle, 42.4% flex the knee between 60° and 90°, 48.5% flex the knee 90° to 120°, and 6.1% regularly flex the knee past 120° during knee cycling.
While the goal of this study was to analyze surgeons’ reported preferences and techniques regarding intraoperative failure of meniscal repairs during concurrent ACLR, the success of meniscal repairs depends on many factors. There are multiple techniques to consider when performing a meniscal repair that can contribute to implant failure rates. While the survey items of this study primarily focused on all-inside repair implants, many might prefer inside-out or outside-in. A previous study showed failure rates of all-inside technique to be 14.9% (31/208), inside-out technique to be (1/19 [5.3%]), and outside-in technique to be (1/6 [16.7%]). 23 Given these varying failure rates by technique, it is possible that varying rates of intraoperative failure could also be observed. Further studies are needed to characterize intraoperative failure rates based on repair technique.
A previous study demonstrated, using magnetic resonance imaging, that flexing the knee to 120° induced a posterior shift of the meniscocapsular structure. 16 However, only 6.1% (2 of 33) of surgeons in the present study reported regularly flexing the knee past 120° during cycling. It remains unclear to what extent the meniscocapsular structure is affected at less than 120° of flexion and what effects this motion would have on meniscal repairs. However, no significant association was found between the extent of flexion during cycling and meniscal repair implant pullout.
This study aimed to describe potential insults to the meniscal repair during concurrent ACLR. Of the 44 respondents, 100% preferred to repair the meniscus before ACLR. The current literature is unclear about the justification for performing meniscal repair first. Some suggest it is customary or intended to improve exposure during the meniscal repair. 22 However, Vertullo et al 22 suggest an alternative, that ACL graft placement and tensioning be performed before meniscal repair for improved visualization of the medial meniscus. Whether the order of concurrent meniscal repair and ACLR is arbitrary or provides a technical advantage remains to be determined.
This study is subject to limitations. Given that this was a cross-sectional survey-based study, it is subject to cognitive, recall, reporting, and sampling bias. The study was limited to a single orthopaedic society, which may not be fully generalizable to national or international trends of techniques and practices in ACLR with concurrent meniscal repairs. Additionally, the survey questions consisted of multiple-choice and checkbox responses, which may not represent all possible choices in practice. However, an “other” option was included where appropriate to capture these responses. The underpowered nature of our study may curtail the significance of our findings. The sample size was insufficient to analyze the possible association between implant failure and cycling alone or hyperflexion alone. Furthermore, this study cannot identify why or when a meniscal implant might fail intraoperatively. Still, it highlights potential practice/technique trends associated with meniscal implant failure as areas for further study.
Future studies should assess the biomechanical properties and pullout strength of meniscal repair implants in the setting of knee cycling and other factors. In addition, future work may focus on the prospective collection of outcomes after ACLR with concurrent meniscal repair, including whether surgeons cycle the knee and other factors, through prospective studies and multivariate analysis.
Conclusion
Pediatric and sports medicine orthopaedic surgeons from PRiSM who were surveyed reported high rates of knee cycling after ACLR. In ACLR cases with concurrent meniscal repairs, more surgeons with fewer years in practice reported meniscal implant failure at least once; however, there is no apparent relationship between reported meniscal implant pullout rates and factors such as knee cycling, suture technique, or surgeon practice characteristics and preferences. Despite this, there were still reports of experiencing meniscal implant pullout after final fixation of the ACL graft. Therefore, we support a second look at the meniscal repair after cycling the knee and ACLR.
Footnotes
Acknowledgements
The authors would like to acknowledge Tracey Bryan, MA, for performing the statistical analysis. Rady Children's Health—San Diego, San Diego, California, USA.
Final revision submitted April 3, 2026; accepted April 9, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.E.H. has received consulting fees from Imagen Technologies Inc, Arthrex, and Kairos Surgical and royalties from Springer Science and Business Media; and owns stock in Imagen Technologies.
Ethical approval was not sought for the present study.