
Abstract
Background:
As indications for anterior cruciate ligament reconstruction (ACLR) expand to older and more metabolically comorbid patients, diabetes mellitus (DM) has emerged as a potential determinant of surgical outcomes. However, existing evidence remains fragmented, with limited pooled data quantifying postoperative risk.
Purpose/Hypothesis:
The purpose was to systematically review evidence comparing postoperative complications between patients with and without DM undergoing ACLR. It was hypothesized that DM would be associated with an increased incidence of overall complications, but not of revision.
Study Design:
Systematic review and meta-analysis; Level of evidence, 3.
Methods:
The PubMed, Embase, Web of Science, and Scopus databases were searched through March 2025 following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and MOOSE (Meta-analysis Of Observational Studies in Epidemiology) guidelines. Observational studies reporting postoperative outcomes in patients with and without DM undergoing ACLR were included. Pooled risk ratios (RRs) with 95% CIs were calculated using fixed- or random-effects models, as appropriate. The primary outcome was revision, and secondary outcomes included infection, surgical-site infection (SSI), readmission, and venous thromboembolism (VTE). For studies with zero events in 1 arm, a continuity correction of 0.5 was applied to enable computation of pooled estimates and avoid division-by-zero errors. Risk of bias assessment across included studies was conducted using the Risk of Bias Assessment tool for Non-randomized Studies of Interventions Version 2.
Results:
A total of 25 studies met the inclusion criteria. Compared with patient without DM, those with DM had significantly higher risks of postoperative infection (after sensitivity analysis, RR, 7.25 [95% CI, 3.07-17.08]; P < .001; I2 = 17.9%), SSI (RR, 3.18 [95% CI, 1.74-5.81]; P = .0002; I2 = 0%), readmission (RR, 2.04 [95% CI, 1.66-2.50]; P < .0001; I2 = 0%), and VTE (RR, 2.19 [95% CI, 1.48-3.25]; P < .0001; I2 = 0%). Revision rates did not differ significantly (RR, 0.68 [95% CI, 0.41-1.14]; P = .15; I2 = 22.2%). Among the included studies, 18 had a moderate risk of bias, 5 had a low risk of bias, and 2 had a serious risk of bias.
Conclusion:
DM is associated with substantially increased risks of infection, SSI, readmission, and VTE after ACLR, although there was no significant difference in revision rates. These findings highlight the need for optimized perioperative strategies, including strict glycemic control, thoughtful graft selection, and tailored surgical protocols to improve safety and outcomes in patients with DM.
Registration:
CRD420251119493.
Keywords
Anterior cruciate ligament (ACL) tears have a significant impact on quality of life, mobility, and work absenteeism, affecting an estimated 200,000 cases annually in the United States alone.21,25,36,47 As ACL reconstruction (ACLR) expands to older and more comorbid patients, metabolic disorders such as diabetes mellitus (DM) are increasingly encountered in sports surgery.11,41,50 DM is a well-established risk factor for postoperative complications across orthopaedic procedures,1,45,54,57 including arthroplasty and fracture fixation,6,17,39,53 due to its effects on vascularity, collagen remodeling, and immune function. 49 However, its influence on ACLR outcomes remains uncertain.
The ACLR environment is unique: it involves intra-articular graft placement within a synovial milieu that is highly sensitive to infection, tissue healing, and local inflammatory balance. 14 Even a low incidence of complications such as deep infection or graft failure can profoundly affect outcomes in a young, active population. Despite several large-database analyses and institutional reports, evidence regarding the relationship between DM and ACLR outcomes is fragmented and sometimes conflicting, as some studies suggest that patients with DM experience increased rates of surgical-site infection (SSI), readmission, and venous thromboembolism (VTE) after ACLR, whereas others report contrasting results.8,9,24,30,48 These discrepancies may reflect differences in study design, population characteristics, or definitions of DM. Therefore, the purpose of this systematic review and meta-analysis was to systematically review the evidence on postoperative complications between patients with and without DM undergoing ACLR. We hypothesized that DM would be associated with an increased incidence of overall complications, but not of revision.
Methods
The present systematic review and meta-analysis was performed in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and MOOSE (Meta-analysis of Observational Studies in Epidemiology) guidelines.7,43 The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD420251119493).
Search Strategy
A comprehensive search of the PubMed/Medline, Scopus, Web of Science, and Embase databases was conducted from inception to March 13, 2025. The strategy combined controlled vocabulary and free-text terms related to “anterior cruciate ligament reconstruction,”“ACL,”“knee ligament,” and “diabetes mellitus.” Reference lists of eligible studies and relevant reviews were manually screened to identify additional publications. The full search syntax is available in Appendix Table 1.
Study Selection
Two reviewers (A.A.F. and D.S.) independently screened titles/abstracts, followed by full-text review of potentially eligible studies. We included all studies that reported outcomes of ACLR in patients with DM. Studies were excluded if they: (1) did not stratify outcomes by DM status, (2) lacked an ACLR population, (3) reported insufficient outcome data, or (4) were conference abstracts, reviews, editorials, or case reports. Discrepancies were resolved through discussion with a third senior reviewer (F.V.). The review included studies; the reference list was not provided.
Risk of Bias Assessment
We evaluated the risk of bias in nonrandomized studies using the Risk of Bias Assessment tool for Non-randomized Studies of Interventions (ROBINS-I V2) tool. 51 This tool evaluates 7 critical domains: (1) confounding; (2) participant selection; (3) intervention classification; (4) deviations from intended interventions; (5) missing data; (6) outcome measurement; and (7) selective reporting. Each domain was judged as low, moderate, serious, or critical risk of bias, with an overall study rating based on the most severe domain-level judgment. Two reviewers (A.A.F. and D.S.) independently applied ROBINS-I V2, resolving discrepancies through discussion. Persistent disagreements were arbitrated by a third reviewer (F.V.). Results were visualized via robvis-generated traffic light and summary plots. 37
Data Extraction
Data were extracted into a standardized table, including study characteristics (first author, year, and location), characteristics (cohort sizes, age, body mass index, and sex distribution), and all reported complications. The primary outcome was revision rate, and secondary outcomes included infection, SSI, readmission, VTE, patient-reported outcomes, and subsequent surgery rates with event rates. SSI was defined as any infection occurring within the follow-up period in the skin or soft tissue of the incision site. Revision was defined as the subsequent surgical procedure performed to replace, repair, or reconstruct a failed primary ACLR graft.
Statistical Analysis
Effect measures were expressed as risk ratios (RRs) with corresponding 95% CIs. Separate meta-analyses were conducted for each outcome. For infection, a random-effects model was applied; fixed-effect models were used for all other outcomes, consistent with the observed heterogeneity. Pooled effect estimates were obtained using the Mantel-Haenszel method. Statistical heterogeneity was quantified using the I2 statistic with 95% CIs and tested using Cochran’s Q. Analyses were performed in R (Version 4.3.1) using the meta and metafor packages. For each outcome, we generated forest plots, funnel plots, and Egger’s regression test for small-study effects. Sensitivity analyses were performed with a leave-one-out (LOO) approach, sequentially excluding each study and recalculating the pooled effect size, P value, and I2 to assess the robustness of the findings. For studies reporting zero events in 1 arm, a continuity correction of 0.5 was applied to enable computation of pooled effect sizes and to avoid computational instability caused by zero-cell counts. Funnel plot contours were added to aid the interpretation of asymmetry. All figures were exported at high resolution for publication.
Results
Study Selection
In total, 5770 studies were identified using the search strategy described previously in the methods section. After removing 2929 duplicate records, 2841 studies entered the title-abstract screening. A total of 314 studies entered the full-text screening phase, of which 289 were excluded for various reasons: 238 records lacked data on patients with DM, 28 were review articles, 19 were abstracts for oral/poster presentations, and 4 lacked ACLR-related data. No study was excluded because of language restriction or full-text availability. The process is summarized in Figure 1.
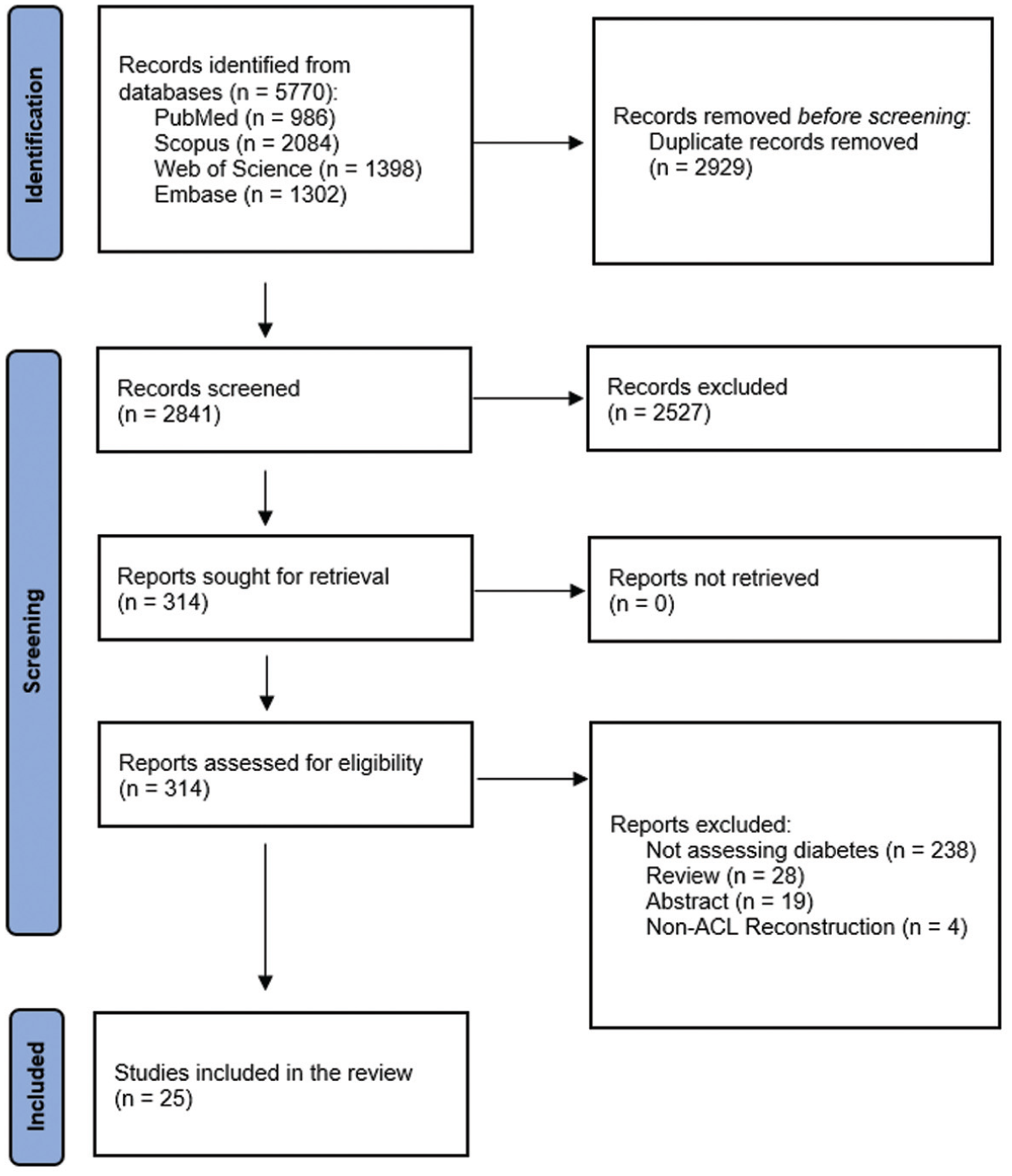
PRISMA flow diagram for inclusion of the studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Characteristics
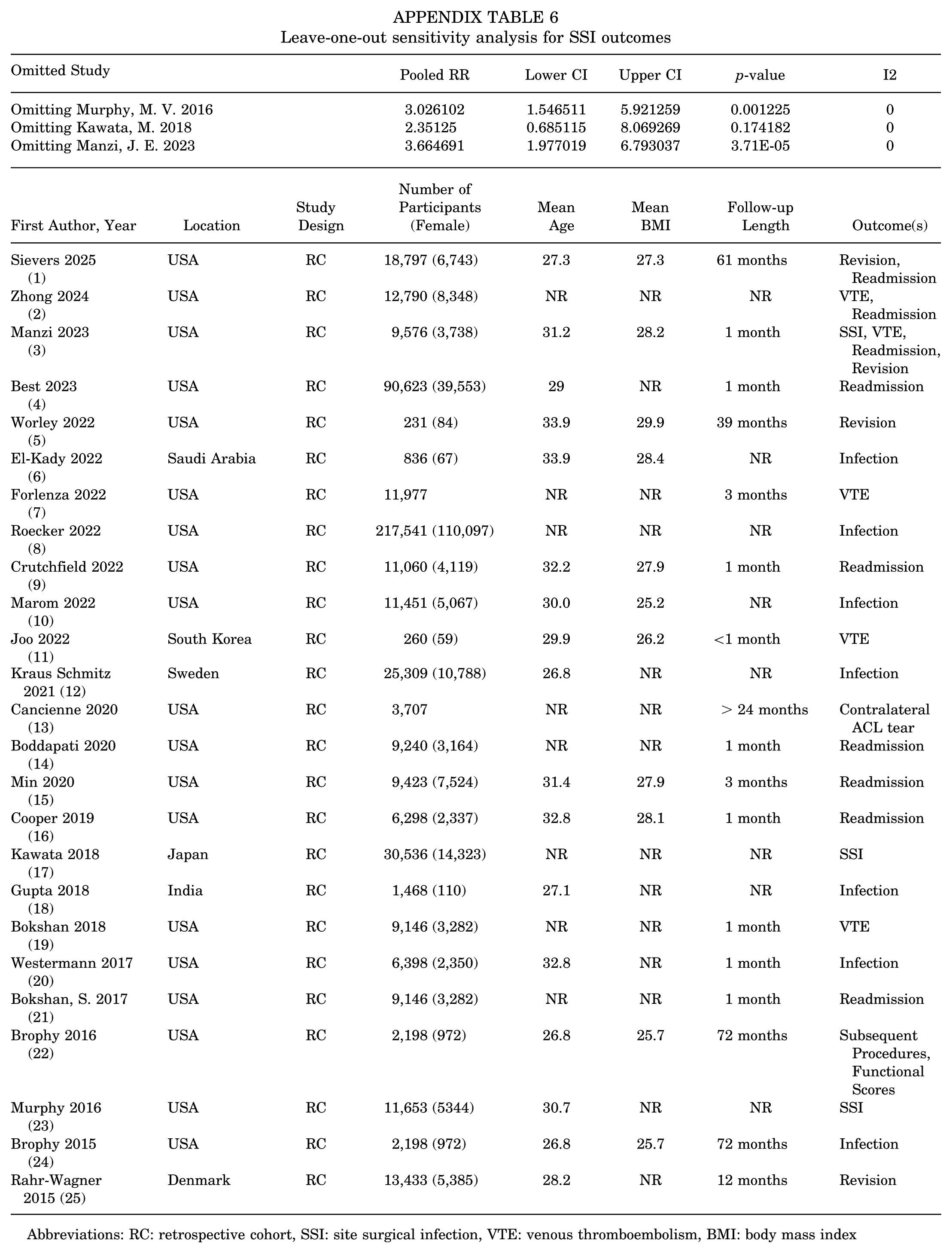
The current systematic review and meta-analysis included 513,951 participants from 25 observational studies, of which 19 were performed in the United States, †† 1 in Saudi 19 Arabia, 1 in South 27 Korea, 1 in Sweden, 30 1 in Japan, 28 1 in Denmark, 44 and 1 in India (Table 1). 24 The mean age of participants ranged from 26.8 to 33.9 years, while 8 studies did not report the mean age.3-5,10,22,28,46,58 Various outcomes regarding the association between DM and ACLR outcomes were reported, ranging from revision, readmission, thromboembolism, and infection to concomitant procedures. Two pairs of cohort overlaps were found by Bokshan et al4,5 and Brophy etal,8,9 yet each reported different outcome measures. Hence, none were excluded from this review, and their populations were counted once in the total sum of the included studies’ populations.
Characteristics of Included Retrospective Cohort Studies a
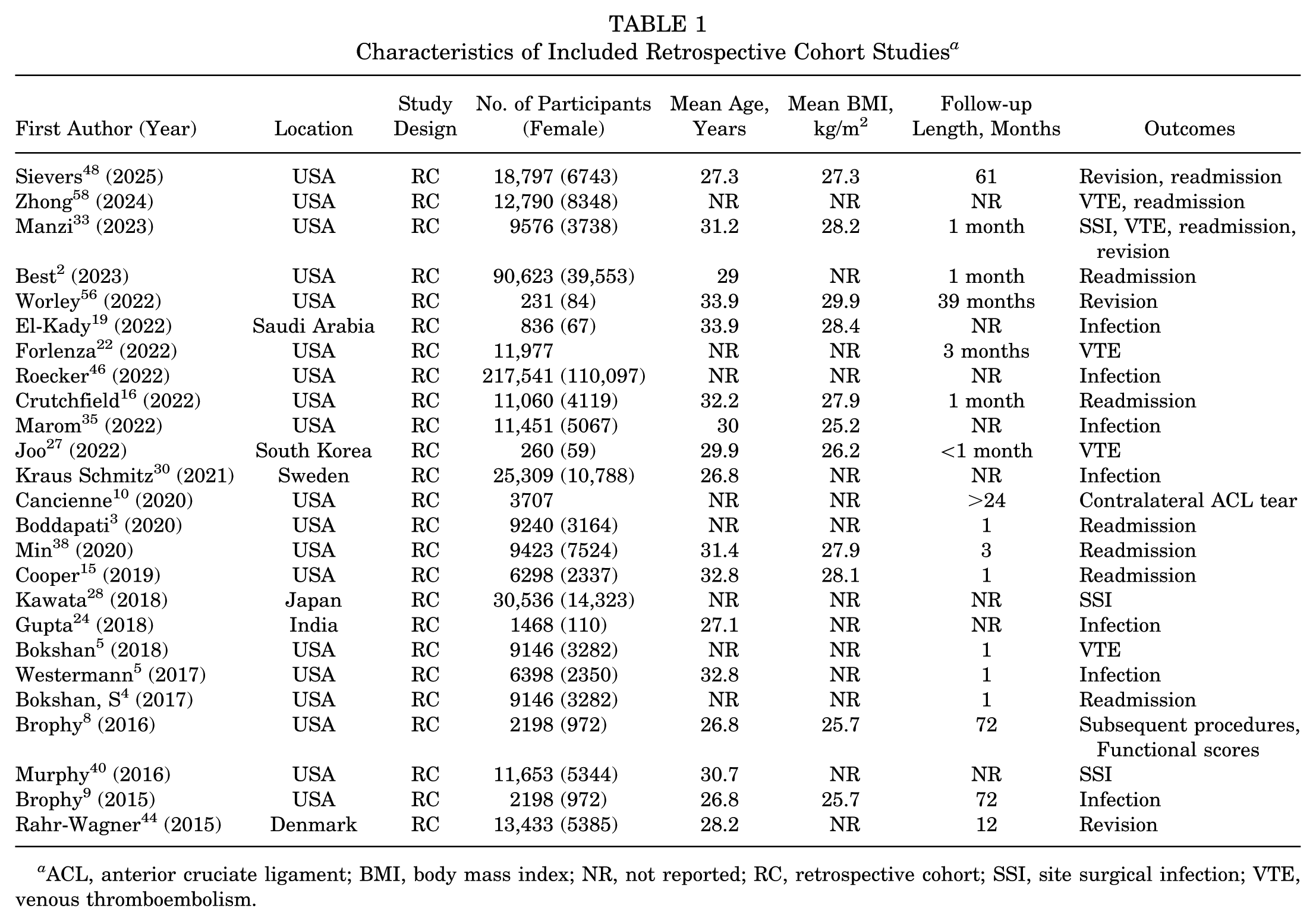
ACL, anterior cruciate ligament; BMI, body mass index; NR, not reported; RC, retrospective cohort; SSI, site surgical infection; VTE, venous thromboembolism.
Risk of Bias Assessment
Among the 25 included observational studies, 18 had a moderate risk of bias, 5 had a low risk of bias, and 2 had a serious risk of bias. A majority of studies had a moderate risk in the first and fifth domains of ROBINS-I V2. The traffic-light plot and summary plot are illustrated in Figure 2.
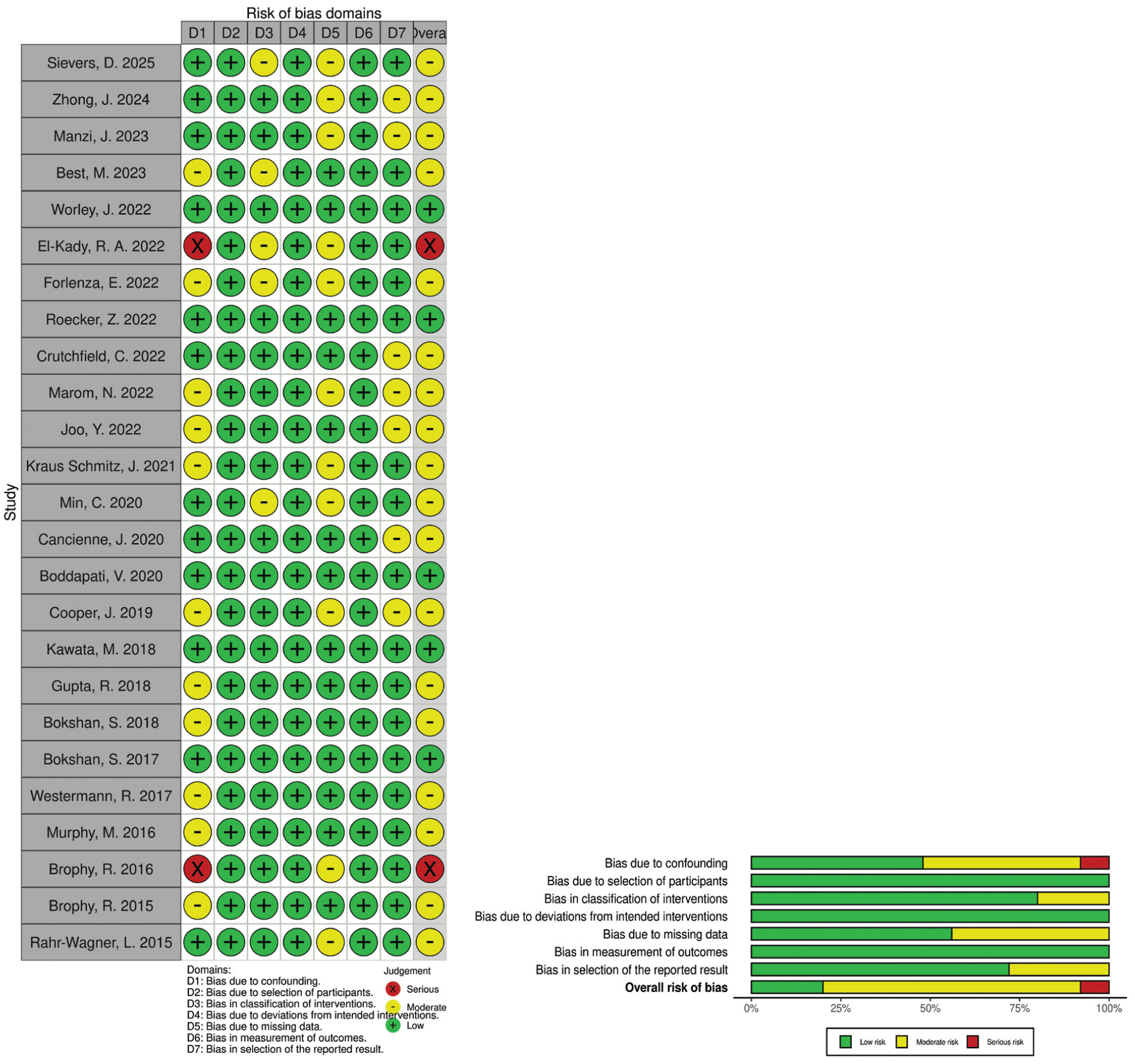
Traffic-light and summary plots for observational studies risk of bias assessment.
Infection
Seven studies reported articular infection in patients with and without DM.9,19,24,28,35,46,55 At first, the meta-analysis showed that infection was not significantly more prevalent among patients with DM than those without (RR, 3.61 [95% CI, 0.92-14.15]) (Appendix Figure 1). The observed between-study heterogeneity was high (I2 = 78.4%; P = .07). Additionally, the funnel plot was shown to be symmetrical, indicating that no significant publication bias was found (Appendix Figure 2). Due to high heterogeneity, LOO sensitivity analysis was performed. After removing the study by Kraus Schmitz etal, 30 infection was significantly more prevalent among patients with DM than among those without (RR, 7.25 [95% CI, 3.07-17.08]; P < .0001; I2 = 17.9%) (Figure 3 and Appendix Table 2).
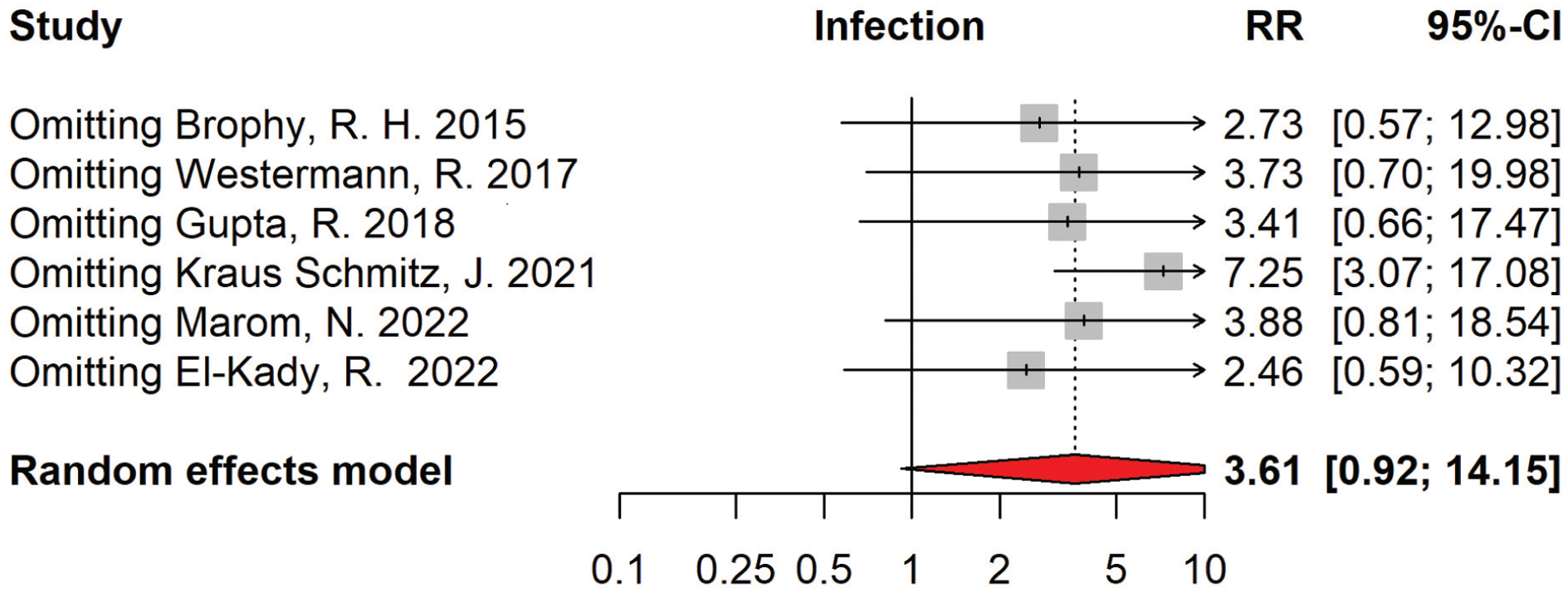
Leave-one-out sensitivity analysis plot showing pooled infection rates among patients with and without diabetes mellitus undergoing anterior cruciate ligament reconstruction, leading to the removal of the study by Kraus Schmitz etal. 30 RR, risk ratio.
Roecker etal 46 reported that both type 1 and type 2 DM increased the risk of infection insignificantly (odds ratio [OR], 1.44 [95% CI, 0.92-2.26] and OR, 1.16 [95% CI, 0.93-1.44]).
Venous Thromboembolism
Four studies reported pulmonary embolism and/or deep vein thrombosis, which were all merged as VTE outcomes.5,22,27,33 Our analysis demonstrated that postoperative VTE incidence was significantly higher among patients with DM (RR, 2.19 [95% CI, 1.48-3.25]; P < .0001) (Figure 4). The observed between-study heterogeneity was low (I2 = 0%; P = .71). The funnel plot was symmetrical, and publication bias was not significant (Appendix Figures 3 and 4; Appendix Table 3).

Forest plot showing pooled venous thromboembolism (VTE) incidences among patients with and without diabetes mellitus who underwent anterior cruciate ligament reconstruction. RR, risk ratio.
Revision
Data from 5 out of 6 studies regarding revision ACLR were pooled.8,33,44,48,56,59 No significant difference was observed between patients with and without DM (RR, 0.68 [95% CI, 0.41-1.14]; P = .15) (Figure 5). No significant heterogeneity was detected among studies’ outcomes (I2 = 22.2%; P = .27), and this was also true for publication bias (Appendix Figures 5 and 6; Appendix Table 4).

Forest plot showing pooled revisions among patients with and without diabetes mellitus undergoing anterior cruciate ligament reconstruction. RR, risk ratio.
Moreover, Rahr-Wagner etal 44 reported an adjusted hazard ratio of 0.89 (95% CI, 0.13-6.38) in 13,433 participants for revision in patients with DM undergoing ACLR. 44
Readmission
Data from 6 out of 8 studies reporting readmission in patients with DM undergoing ACLR were pooled.5,15,16,33,38,48 Meta-analysis demonstrated that readmission was significantly higher among patients with DM undergoing ACLR (RR, 2.04 [95% CI, 1.66-2.50]; P < .0001) (Figure 6). No significant publication bias or heterogeneity was found between studies (I2 = 0%; P = .27) (Appendix Figures 7 and 8; Appendix Table 5).
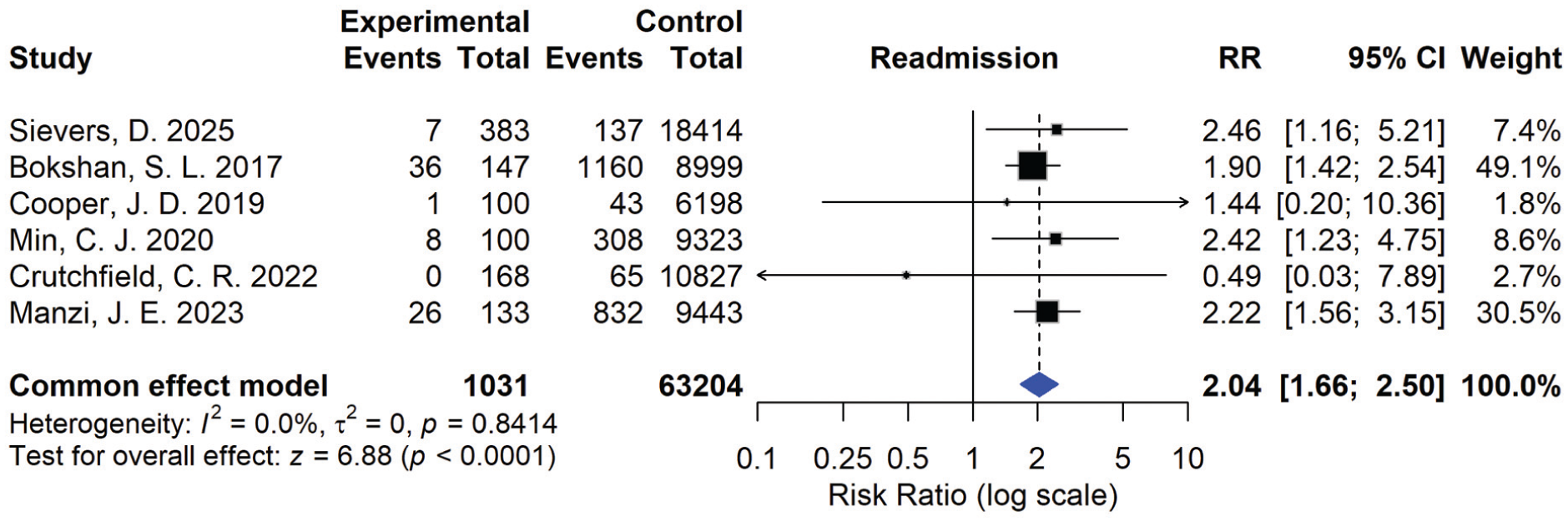
Forest plot showing pooled readmissions among patients with and without diabetes mellitus undergoing anterior cruciate ligament reconstruction. RR, risk ratio.
Best etal 2 reported that patients with DM had significantly higher readmission rates in both univariate and multivariate analyses (ORs of 3.42 [95% CI, 2.60-4.52] and 2.57 [95% CI, 1.91-3.46], respectively) among 90,623 participants. 2 However, Boddapati etal 3 reported an insignificant effect of DM on readmission rate within 9240 ACLR candidates (adjusted OR, 0.85 [95% CI, 0.11-6.65]).
Surgical Site Infection
Three studies reported SSI rates in DM and non-DM ACLR patients.28,33,40 SSI was significantly higher in patients with DM (RR, 3.18 [95% CI, 1.74-5.81]; P = .0002) (Figure 7). Additionally, no significant heterogeneity was present (I2 = 0%; P = .61) (Appendix Figures 9 and 10; Appendix Table 6).
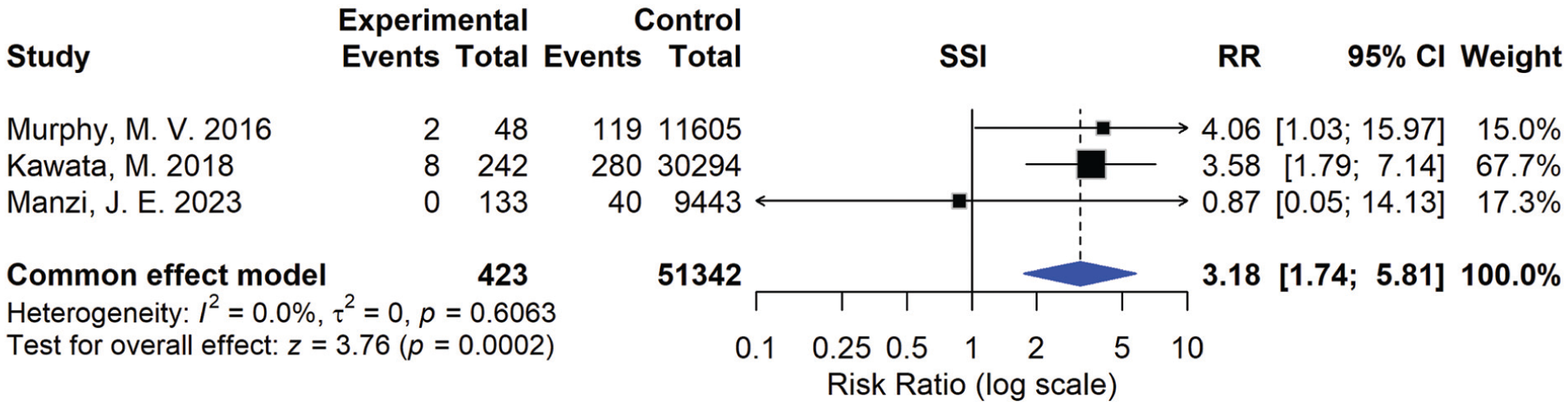
Forest plot showing pooled surgical site infection (SSI) among patients with and without diabetes mellitus undergoing anterior cruciate ligament reconstruction. RR, risk ratio.
Patient-Reported Outcomes
Because of insufficient data, no pooling and meta-analysis were feasible. Brophy etal 8 reported that in a 2-year follow-up, patients with DM experienced lower International Knee Documentation Committee scores (P = .04) and Knee injury and Osteoarthritis Outcome Score (KOOS) pain (P = .02), activities of daily living (P = .03), and sports/recreation (P = .02) subscale scores in the adjusted model. The knee-related quality of life and symptoms subdomain of KOOS was not significantly different (P = .18 and .13, respectively).
Subsequent Procedures
Brophy etal 8 reported that the subsequent surgery rate on either the ipsilateral or contralateral knee was not significantly different between DM and non-DM ACLR candidates up to 2 years after ACLR. Cancienne etal 10 reported that neither type 1 nor type 2 DM was associated with a higher risk of contralateral ACL tear.
Discussion
In this meta-analysis of 25 observational studies (nearly 500,000 patients), patients with DM undergoing ACLR faced markedly higher risks of postoperative adverse events: notably infection/septic arthritis, surgical site complications, readmission, and VTE. In contrast, we found no consistent increase in revision ACLR rates among patients with DM compared with those without DM.
Our pooled data demonstrate a significantly elevated infection risk in patients with DM (after sensitivity analysis: RR ≈ 7.3 [95% CI, 3.07-17.08]). This is biologically plausible because hyperglycemia impairs neutrophil function, increases vascular permeability and oxidative stress, and compromises soft-tissue healing.20,26,29 While much of the orthopaedic infection literature arises from arthroplasty, the intra-articular, graft-incorporation environment of ACLR demands equal vigilance. In this analysis, the study by Kraus Schmitz etal 30 was removed after the sensitivity analysis. The cohort with diabetes was very small and based on self-reported diabetes status, introducing potential misclassification and limited statistical power. The wide confidence intervals and the risk of type 2 error associated with the low number of participants with DM may have disproportionately influenced pooled estimates and contributed to heterogeneity. Although ACLR infections are rare, with reports 42 ranging from 0.32% to 1.80%, they carry devastating functional consequences in a young, athletic population. For surgeons treating ACLR in patients with DM, rigorous perioperative glycemic optimization seems mandatory. Postoperative wound surveillance should be intensified, and any signs of wound erythema or effusion should trigger prompt evaluation to detect infection.
We found a doubling of readmission risk (RR ≈ 2.04) and a more than 2-fold increase in VTE (RR ≈ 2.19) among patients with DM. DM induces a hypercoagulable state via endothelial dysfunction, increased platelet aggregation, and impaired fibrinolysis. 12 While ACLR is perceived as a “low-risk” sports procedure in patients with comorbidity (including DM), these findings argue for tailored perioperative protocols. In patients with DM who underwent ACLR, VTE prophylaxis consultation with hematology/medicine may be considered if there are additional known risk factors (age >35 years, BMI >30 kg/m2, smoking, heavy graft or osteotomy augmentations). 23 Therefore, as DM increases VTE risk, a more intense VTE prophylaxis strategy may be required in ACLR candidates with DM, 60 with consideration of an extended duration thromboprophylaxis (eg, beyond standard 14 days). 34
Our finding of no significant difference in revision ACLR between DM and non-DM patients (RR ≈ 0.68 [95% CI, 0.41-1.14]; P = .15) may appear reassuring. However, this must be interpreted cautiously: revision is a coarse endpoint, driven by graft failure and reinjury, not exclusively biological graft incorporation. It is possible that patients with DM self-select out of high-demand sports, or their lower activity mitigates reinjury risk.13,32 We cannot infer that graft biology is unaffected in DM. Surgeons should not assume “normal” graft healing in DM; instead, they should closely monitor functional milestones and counsel patients about the risk of microinstability or delayed graft incorporation despite apparent mechanical stability.
Although our meta-analysis cannot define a specific HbA1c threshold for ACLR, the broader surgical literature offers guidance. Preoperative glycated hemoglobin (HbA1c) <7% has been associated with reduced infectious complications across surgical specialties (adjusted OR ≈ 2.13 for HbA1c ≥7%). 18 In arthroplasty, HbA1c thresholds of 7.7% to 8% have been identified as inflection points for increased PJI rates. 52 Some studies suggest even stricter thresholds (HbA1c ≤6.6%) for optimal outcomes in ACLR. 31 For elective ACLR in patients with DM, we recommend targeting HbA1c ≤7% (ideally ≤6.5%) when feasible and perioperative glucose <180 mg/dL, recognizing patient-specific factors. Some other factors may also be considered for a more controlled operation, such as fasting insulin, C-peptide, or homeostatic model assessment of insulin resistance, despite the need for more research. If surgical delay is unacceptable (eg, elite athlete), then real-time multidisciplinary glycemic management must be employed, and risk mitigation must be intensified.
Given the elevated biological risk in people with DM, surgical strategy should be deliberately optimized: favor autograft where possible (less healing burden and lower infection risk compared with allograft/infection reports), minimize operative time, and reduce the use of accessory procedures that may lengthen exposure or blood loss, apply meticulous hemostasis, layered closure, and possibly enhance antibiotic prophylaxis protocols.
Our analysis is constrained by limitations inherent to database/registry studies: a lack of detailed glycemic data (type 1 vs type 2 DM, insulin use, DM duration, HbA1c values), potential coding errors, and heterogeneity in surgical technique and graft types. A significant number of studies had follow-ups of <1 month or did not report follow-ups, highlighting the need for longer follow-ups in future studies. Moreover, no ACLR-specific prospective dataset currently defines optimal glycemic thresholds. Future directions include prospective ACLR cohorts stratified by HbA1c and glucose control, with standardized graft type and rehabilitation.
Conclusion
Patients with DM undergoing ACLR face higher risks of infection (after sensitivity analysis), SSI, VTE, and readmission, although there was no significant difference in revision rates. Despite the heterogeneity and the need for caution while interpreting these outcomes, these findings call for optimized perioperative management through strict glycemic control, careful graft selection, and tailored follow-up.Developing ACLR-specific glycemic thresholds and standardized protocols may improve safety and outcomes in this growing patient population.
Footnotes
Appendix
Leave-one-out sensitivity analysis for SSI outcomes
| Omitted Study | Pooled RR | Lower CI | Upper CI | p-value | I2 | ||
|---|---|---|---|---|---|---|---|
| Omitting Murphy, M. V. 2016 | 3.026102 | 1.546511 | 5.921259 | 0.001225 | 0 | ||
| Omitting Kawata, M. 2018 | 2.35125 | 0.685115 | 8.069269 | 0.174182 | 0 | ||
| Omitting Manzi, J. E. 2023 | 3.664691 | 1.977019 | 6.793037 | 3.71E-05 | 0 | ||
| First Author, Year | Location | Study Design | Number of Participants (Female) | Mean Age | Mean BMI | Follow-up Length | Outcome(s) |
| Sievers 2025 (1) |
USA | RC | 18,797 (6,743) | 27.3 | 27.3 | 61 months | Revision, Readmission |
| Zhong 2024 (2) |
USA | RC | 12,790 (8,348) | NR | NR | NR | VTE, Readmission |
| Manzi 2023 (3) |
USA | RC | 9,576 (3,738) | 31.2 | 28.2 | 1 month | SSI, VTE, Readmission, Revision |
| Best 2023 (4) |
USA | RC | 90,623 (39,553) | 29 | NR | 1 month | Readmission |
| Worley 2022 (5) |
USA | RC | 231 (84) | 33.9 | 29.9 | 39 months | Revision |
| El-Kady 2022 (6) |
Saudi Arabia | RC | 836 (67) | 33.9 | 28.4 | NR | Infection |
| Forlenza 2022 (7) |
USA | RC | 11,977 | NR | NR | 3 months | VTE |
| Roecker 2022 (8) |
USA | RC | 217,541 (110,097) | NR | NR | NR | Infection |
| Crutchfield 2022 (9) |
USA | RC | 11,060 (4,119) | 32.2 | 27.9 | 1 month | Readmission |
| Marom 2022 (10) |
USA | RC | 11,451 (5,067) | 30.0 | 25.2 | NR | Infection |
| Joo 2022 (11) |
South Korea | RC | 260 (59) | 29.9 | 26.2 | <1 month | VTE |
| Kraus Schmitz 2021 (12) | Sweden | RC | 25,309 (10,788) | 26.8 | NR | NR | Infection |
| Cancienne 2020 (13) |
USA | RC | 3,707 | NR | NR | > 24 months | Contralateral ACL tear |
| Boddapati 2020 (14) |
USA | RC | 9,240 (3,164) | NR | NR | 1 month | Readmission |
| Min 2020 (15) |
USA | RC | 9,423 (7,524) | 31.4 | 27.9 | 3 months | Readmission |
| Cooper 2019 (16) |
USA | RC | 6,298 (2,337) | 32.8 | 28.1 | 1 month | Readmission |
| Kawata 2018 (17) |
Japan | RC | 30,536 (14,323) | NR | NR | NR | SSI |
| Gupta 2018 (18) |
India | RC | 1,468 (110) | 27.1 | NR | NR | Infection |
| Bokshan 2018 (19) |
USA | RC | 9,146 (3,282) | NR | NR | 1 month | VTE |
| Westermann 2017 (20) |
USA | RC | 6,398 (2,350) | 32.8 | NR | 1 month | Infection |
| Bokshan, S. 2017 (21) |
USA | RC | 9,146 (3,282) | NR | NR | 1 month | Readmission |
| Brophy 2016 (22) |
USA | RC | 2,198 (972) | 26.8 | 25.7 | 72 months | Subsequent Procedures, Functional Scores |
| Murphy 2016 (23) |
USA | RC | 11,653 (5344) | 30.7 | NR | NR | SSI |
| Brophy 2015 (24) |
USA | RC | 2,198 (972) | 26.8 | 25.7 | 72 months | Infection |
| Rahr-Wagner 2015 (25) | Denmark | RC | 13,433 (5,385) | 28.2 | NR | 12 months | Revision |
Abbreviations: RC: retrospective cohort, SSI: site surgical infection, VTE: venous thromboembolism, BMI: body mass index
Acknowledgements
The authors acknowledge using artificial intelligence solely for language correction purposes. AI generation functions were not used in this study.
Final revision submitted April 2, 2026; accepted April 5, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for this study.