
Abstract
Background:
Magnetic resonance arthrography (MRa) is considered superior to magnetic resonance imaging (MRI) in detecting glenoid labral pathology, although both are used in clinical practice with varying accuracy. Diagnostic arthroscopy remains the gold standard. In the pediatric and young adult population, limited data exist comparing MRa/MRI to arthroscopy in detecting superior labrum anterior and posterior (SLAP) lesions in cases of shoulder instability.
Purpose:
To evaluate the effectiveness of MRa/MRI in identifying various labral pathologies in a pediatric and young adult population with shoulder instability.
Study Design:
Cohort study (Diagnosis); Level of evidence, 2.
Methods:
Patients who underwent shoulder stabilization surgery with MRa/MRI obtained prior to surgery were retrospectively reviewed. Lesions identified on imaging reports were compared to arthroscopic findings used as the gold standard, and sensitivity and specificity were calculated for both MRI and MRa for anterior, posterior, and SLAP lesions. The percentage of time the imaging report was fully correct in identifying the integrity of the glenoid labrum in all 3 regions was calculated.
Results:
A total of 340 cases met inclusion criteria (297 MRa, 43 MRI). The mean age at surgery was 16.9 ± 1.8 years. There were no statistically significant differences between MRI and MRa in the anterior, posterior, or SLAP lesion groups. The imaging report was correct in fully diagnosing the integrity of the glenoid labrum in all 3 regions 63% of the time.
Conclusion:
There is no significant difference between MRa and MRI in detecting anterior, posterior, or SLAP lesions in the pediatric/young adult population. Imaging fails to fully diagnose the integrity of the labrum 37% of the time, and caution should be taken when interpreting imaging reports prior to diagnostic arthroscopy.
It is estimated that up to 2% of the general population will experience a glenohumeral joint dislocation in their lifetime, with active adolescents and young adults making up a large proportion of those events.7,14,21 Common injuries seen in this population include Bankart lesions, posterior glenoid labrum tears, and superior labrum anterior and posterior (SLAP) tears.5,15,17 When there is clinical suspicion for these injuries, magnetic resonance imaging (MRI) and magnetic resonance arthrography (MRa) are usually the diagnostic imaging modalities of choice.16,30 MRI and MRa are considered appropriate studies for a suspected glenoid labrum lesion, but MRa is often preferred, as previous studies have shown improved sensitivity in detecting various labral pathologies by using MRa.1,3 However, MRa requires the additional step of administering an intra-articular injection prior to the study, which potentially delays scheduling of the study. Even so, both MRI and MRa remain imperfect, and thus diagnostic arthroscopy is still considered the gold standard for the diagnosis of glenoid labral pathology. 13
Previous studies have assessed the sensitivity and specificity of MRI and MRa compared to arthroscopy for numerous shoulder pathologies with wide variability in the reported values (Table 1). It is important to note, however, that most of these studies relied on musculoskeletal (MSK)-trained radiologists and included a primarily adult population, which may not be applicable to clinical practices with limited resources or to clinicians treating the pediatric/young adult population. Specific to the pediatric/young adult population, there is a paucity of data comparing MRa/MRI to arthroscopy in detecting anterior labral and SLAP lesions in cases of shoulder instability.5,6
Sensitivity and Specificity of MRI and MRa as Reported in the Literature a

ABER, abduction external rotation; MRa, magnetic resonance arthrography; MRI, magnetic resonance imaging; MSK, musculoskeletal; NA, not available; SLAP, superior labrum anterior and posterior.
Types of glenoid tears by study: Jonas et al 11 (at least 1 of the following: anterior, posterior, SLAP), Jensen et al 10 (any type of tear, including Bankart), Saqib et al 23 (labral tear regardless of position), and Shafiei et al 24 (any labral injury).
Meta-analysis.
Pediatric study, ages ≤18 years.
Same set of patients received both MRa and MRI.
The purpose of this study was to evaluate the effectiveness of MRa and MRI as diagnostic tools prior to shoulder stabilization surgery in the pediatric and young adult population. We hypothesized that MRa would have greater sensitivity for the diagnosis of shoulder labral pathology.
Methods
This is an institutional review board-approved retrospective review of patients who had shoulder stabilization surgery at a single pediatric institution between January 2012 and June 2022. Potential patients were identified by querying the institutional database using arthroscopic and open procedure Current Procedural Terminology codes (29806, 29807, 29999, 23450, 23455, 23460, 23462, 23065, 23066, 23929). Cases were included if the patient had an MRa or MRI performed at the institution. Cases were excluded if the imaging occurred more than 6 months before surgery, the MRa or MRI reports were inconclusive, the patient had prior ipsilateral shoulder stabilization surgery or significant congenital labral defects, or the chart had incomplete or insufficient data.
Both 1.5 and 3.0 Tesla (T) MRI scanners were in use during the study period. Standard injection protocol was carried out for MRa imaging using intermittent fluoroscopy via an anterior or posterior approach, depending on the performing provider. Accurate placement into the joint was confirmed through detection of a small amount of Isovue-300 (0.5-2.0 mL) via spot fluoroscopic imaging. Then, 6 to 10 mL of the arthrogram mixture (5 mL saline, 5 mL 1% lidocaine, 8 mL Isovue-300, and 0.2 mL Dotarem) was injected into the joint. A steroid injection was added at the time of arthrogram, based on the patient's request. If requested, 40 mg (1 mL) Kenalog was injected prior to injection of the arthrogram mixture, which now included bupivacaine instead of lidocaine (5 mL saline, 5 mL 0.5% bupivacaine, 8 mL Isovue-300, and 0.2 mL Dotarem).
Charts were reviewed for patient demographics and data related to imaging and surgery. The description of the labral pathology was obtained from pertinent imaging reports from non-MSK-trained radiologists and operative notes from 1 of 3 board-certified orthopaedic surgeons at a single institution. Lesion type was classified based on the location of the tear using conventional clock face nomenclature, with lesions defined as follows, regardless of laterality: superior, 10 to 2 o’clock; anterior, 3 to 6 o’clock; and posterior, 6 to 10 o'clock (Figure 1). Other pathology identified on imaging or during surgery was not analyzed. For patients who had 2 or more lesions, each lesion was counted separately. The use of the term fraying or equivocal words such as maybe or possible was considered negative. A tear that partially extended into another region, as defined by the clock face classification, was considered positive only for the primary region.
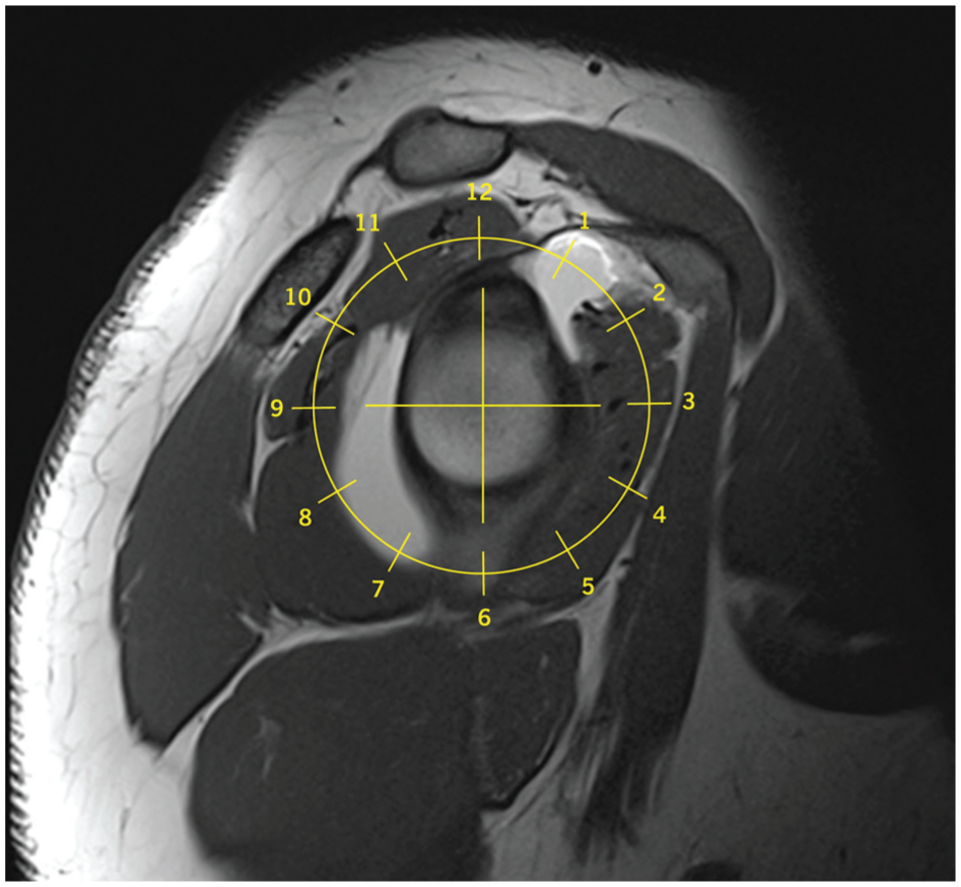
Three lesion types based on a clock face: superior, 10 to 2 o’clock; anterior, 3 to 6 o’clock; and posterior, 6 to 10 o'clock.
Lesions identified on imaging reports were compared to arthroscopic findings used as the gold standard and classified as true positive (TP), true negative (TN), false positive (FP), and false negative (FN). Sensitivity and specificity were calculated for each lesion type and imaging method. For each imaging method, the sample size for sensitivity was the number of positives according to the arthroscopic findings (TP + FN); for specificity, it was the number of negatives according to the arthroscopic findings (TN + FP). The percentage of time the imaging report was fully correct in identifying the integrity of the glenoid labrum in all 3 regions was calculated.
For each of the 3 lesion types studied, MRa and MRI were compared on sensitivity and specificity with versions of the Fisher exact test designed for that purpose. A P value < .05 was considered significant. A power analysis was conducted for 2-tailed tests at the 5% level of significance. The power to detect a 20-percentage-point difference of 90% versus 70% was calculated. The 95% confidence intervals were calculated for sensitivity and specificity for both types of imaging. They represent intervals likely to contain the true sensitivity/specificity in the population of patients from which this sample was taken. MRa and MRI were also compared on the percentage of correct diagnoses by lesion type and for the patient overall using the likelihood ratio chi-square test.
Results
Population Description
There were 340 cases (324 patients) included in the study (Figure 2). The mean age at surgery was 16.9 ± 1.8 years (10.4-25.6 years), and the mean time from imaging to surgery was 1.8 ± 1.3 months. In total, 71% were male, 80% were White (14% African American/Black, 6% other), and 96% were of non-Hispanic/Latino ethnicity. There were 350 lesions identified during arthroscopy: 200 (57%) anterior, 90 (26%) posterior, and 60 (17%) SLAP. An MRa was obtained in 297 (87%) cases and an MRI in 43 (13%) cases. A 3.0 T scanner was used in 173 cases (140 MRa, 33 MRI), a 1.5 T scanner was used in 112 cases (110 MRa, 2 MRI), and it was not documented in 55 cases.
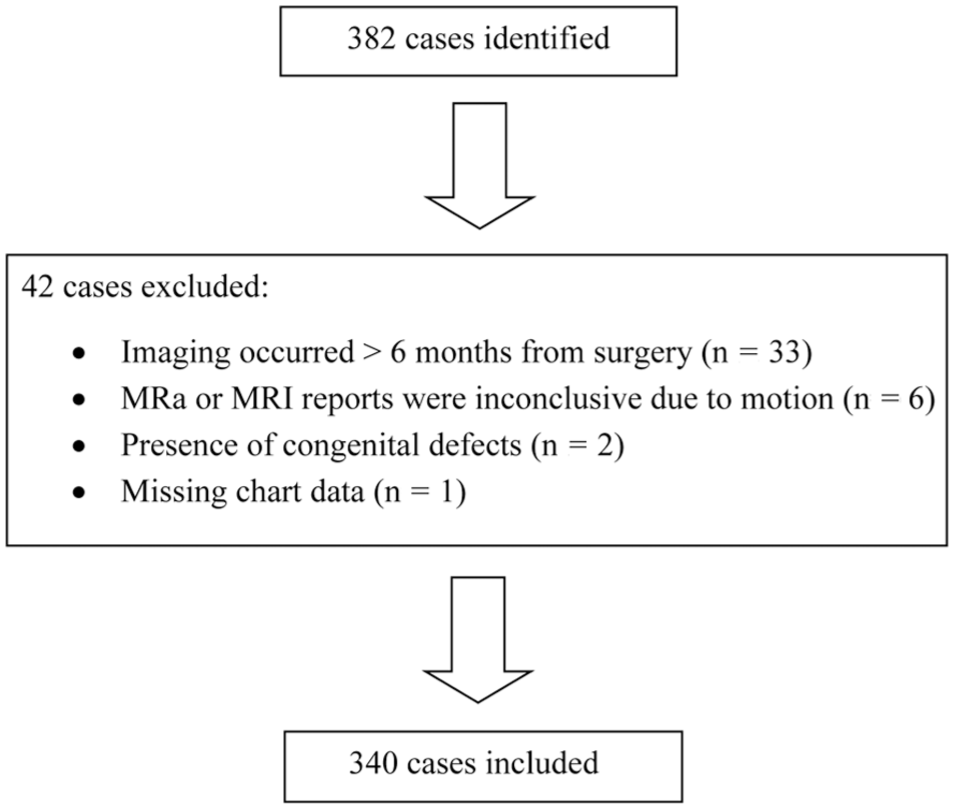
Study enrollment flowchart.
Sensitivity and Specificity
The sensitivity and specificity of MRa in detecting lesions in each region are as follows, respectively: anterior lesions, 86% and 81%; posterior lesions, 71% and 93%; and SLAP lesions, 68% and 88%. Sensitivity and specificity of MRI in detecting lesions in each region are as follows, respectively: anterior lesions, 84% and 91%; posterior lesions, 50% and 94%; and SLAP lesions, 29% and 97% (Table 2).
Comparison of Sensitivity and Specificity of MRa and MRI for Detecting Anterior, Posterior, and SLAP Lesions a

MRa, magnetic resonance arthrography; MRI, magnetic resonance imaging; SLAP, superior labrum anterior and posterior.
Fisher exact test.
Power for detecting 90% versus 70%.
The 95% exact binomial confidence intervals.
In comparing the sensitivity and specificity of MRa to MRI for anterior, posterior, or SLAP lesions, no significant differences were found (Table 2). There were also no statistically significant differences between the MRa and MRI groups with regard to patient demographics such as age, sex, distribution of lesion type (anterior, posterior, SLAP), race, ethnicity, or laterality. The only statistically significant differences were for the time from imaging to surgery and the time from order to imaging. The wait for surgery after imaging was significantly longer for MRI than for MRa (2.1 months vs 1.7 months, P = .019). The time from order to imaging was significantly longer for MRa than for MRI (18.1 days vs 11.4 days, P < .001).
Imaging Report
When comparing all imaging reports to arthroscopic findings used as the gold standard, the imaging report was correct in fully diagnosing the integrity of the glenoid labrum in all 3 regions 63% of the time. Further analysis comparing the percentage of correct diagnoses for MRa versus MRI for different lesion types is listed in Table 3. There were no statistically significant differences in the percent correct.
Analysis of Percent Correct by Imaging Type and by Patient a

MRa, magnetic resonance arthrography; MRI, magnetic resonance imaging; SLAP, superior labrum anterior and posterior.
Discussion
Our analysis suggests that there may be no differences between MRa and MRI in detecting anterior, posterior, or SLAP lesions in the pediatric/young adult population. To our knowledge, only 2 other studies have reported the accuracy of MRa imaging in detecting anterior or SLAP lesions compared to diagnostic arthroscopy in the adolescent population.5,6 To our knowledge, this is the first study to report the MRI accuracy on posterior labral lesions, as well as the first to compare the effectiveness of MRa to MRI in this particular cohort.
Overall, the literature presents convincing evidence to suggest an advantage of MRa in detecting anterior and posterior labral pathology,1,26 but superior labral pathology has produced conflicting results. A 2017 systematic review and meta-analysis of the effectiveness of MRI in detecting SLAP lesions suggests that MRa is superior to MRI. 3 In that study, MRa was shown to be more sensitive and specific compared to MRI. A 2018 systematic review and meta-analysis by Ajuied et al 1 analyzed the effectiveness of MRI in detecting labral pathology, broken down based on region within the labrum, and demonstrated similar sensitivity but decreased specificity of MRa compared to MRI in detecting SLAP lesions. Ajuied et al 1 also found increased sensitivity for MRa in detecting anterior and posterior labral tears compared to MRI. It should be noted that of the 8 studies reporting the mean age of patients included in the meta-analysis, the pooled mean age was 41 years compared to 16.9 years in our study.
Discrepancies in the literature regarding the best modality to detect SLAP lesions may be attributed to interpretive errors associated with normal anatomic variants near the superior labrum, such as the presence of a sublabral foramen. 4 The introduction of contrast to this area may lead to higher rates of false positives, thus lowering specificity compared to MRI. With this in mind, MRI should continue to have a role in clinicians’ diagnostic algorithms in cases of shoulder instability. Other advantages of using MRI over MRa include lower costs, decreased wait time to obtain imaging, and avoidance of inherent risks associated with the invasiveness of MRa procedures, the latter of which may be of particular importance in the context of the adolescent and young adult population.11,20 With regard to wait time, our study results mirror those previously reported in the literature: there is a longer wait time from order to imaging for MRa compared to MRI. 20 Interestingly, however, time from MRI to surgery was longer in our cohort compared to MRa. We postulate that this may be a function of the wait time found between order and imaging. Overall time from ordering advanced imaging modality to shoulder stabilization surgery is similar between the groups.
Compared to the literature, our results consistently demonstrated lower sensitivities and specificities for both MRa and MRI in identifying various labral pathologies. A plausible explanation for this—and what is considered a strength of this study—is the fact that non-MSK-trained radiologists individually interpreted the MRa/MRI results and generated the imaging reports used in this study. In contrast, most previously published studies analyzing MRa/MRI sensitivity and specificity relative to diagnostic arthroscopy have used MSK-trained radiologists as part of its methodology.5,8,9,11 In addition, other studies have used a group model, asking radiologists to interpret the imaging results in consensus with a colleague.5,9,19,29 Our methodology may more accurately represent clinical practice as access to MSK-trained radiologists is limited, and reaching a consensus with radiology colleagues on a case-by-case basis is impractical. Previous work supports this concept and has demonstrated improved diagnostic performances by subspecialized radiologists with greater shoulder MRI experience.13,28 In fact, in a study by Theodoropoulos et al, 28 general radiologists achieved a maximum sensitivity of 69% for detecting labral pathology, whereas musculoskeletal radiologists reached a sensitivity of 94% for the same imaging. Our results align with those of the general radiologists in Theodoropoulos et al 28 and may be more representative of what can be expected in a community setting.
In all, the imaging report was accurate in fully diagnosing the existing labral pathology only 63% of the time. Subanalysis of detecting individual lesion types for both MRa and MRI was correct over 80% of the time. The results by patient were lower because being labeled as correct meant correctly identifying pathology in all 3 regions of the labrum. Strikingly, this is higher than previous studies that have reported as low as 30% accuracy in preoperative interpretation of advanced imaging for labral pathology. 2 This is important for patients, families, and providers to be aware of, given that the imaging report accessible within the electronic medical record may misdiagnose 1 or more regions of the glenoid labrum prior to definitive diagnostic arthroscopy. A misdiagnosis could lead to undue stress caused by a preconceived opinion in favor of or against the need for surgical intervention prior to being formally evaluated by an orthopaedic surgeon. These results also reinforce the need for orthopaedic surgeons to personally interpret imaging, in the context of the patient's history and physical examination, rather than relying solely on radiologist interpretation for diagnosis and treatment planning. It is standard practice at this institution for orthopaedic surgeons to independently interpret imaging when indicating patients for surgery; however, these data were not captured in our study. Future studies should examine the accuracy of orthopaedic surgeons’ advanced imaging interpretation compared to diagnostic arthroscopy using methods similar to those in our study.
Of note, positive predictive values or negative predictive values were not calculated in this study because these values depend on the prevalence of lesions in the population of patients with symptoms. All that is known within the boundaries of our study is the prevalence of lesions in patients who received surgery. This would be expected to be higher than the prevalence in the population with symptoms (because surgery would be performed only if a lesion was suspected). Therefore, predictive values calculated solely from this sample would likely be inaccurate and were not obtained.
Our study is limited by the retrospective design of the review and by its single geographic region. The operative reports that were written by 1 of 3 surgeons had variability in the format of what was reported. All 3 surgeons were available for any questions regarding the interpretation of the operative reports. It is worth mentioning that the gold standard used in this study, arthroscopy, is variable in itself, and interpretation of operative findings may be subject to error. The risk of this was mitigated by the participating surgeons, who combined for over 60 years of orthopaedic sports medicine experience. Due to a lack of a control group, there was a selection bias in that all patients included in this study had symptoms related to shoulder instability.
The study's statistical power was limited by the relatively small number of cases with MRI, which was further reduced since only true positives are relevant for comparing sensitivities and only true negatives are used to compare specificities. Our statistical methods were further limited by the fact that, in some cases, multiple lesions per patient were treated as independent observations. While we believe that these lesions should be treated independently from one another, in reality, certain factors, such as poor image quality, could have led to inaccurate interpretation by the radiologist.
Lastly, it is important to note that data regarding the field strength of the MRI scanner were not documented in 55 patients, which is a limitation of a retrospective study. Therefore, a complete analysis comparing the accuracy of 1.5 T and 3.0 T in our cohort could not be completed. Future studies should investigate the difference between 3.0 T MRa versus 3.0 T MRI in the adolescent/young adult population to determine if any difference exists between the modalities.
Conclusion
Our data demonstrated no significant difference between MRa and MRI in detecting anterior, posterior, or SLAP lesions in the pediatric/young adult population. In our sample, sensitivity tended to favor MRa for all 3 types of lesions, whereas specificity tended to favor MRI for both SLAP and anterior lesions. Our results consistently demonstrated lower sensitivities and specificities for both MRa and MRI in identifying various labral pathologies compared to other publications, which almost ubiquitously have used MSK-trained radiologists as part of their methodology. Our findings may more accurately represent clinical practice as access to MSK trained radiologists is limited. Lastly, imaging failed to fully diagnose the integrity of the labrum 37% of the time, and caution should be taken when interpreting imaging reports prior to diagnostic arthroscopy.
Footnotes
Acknowledgements
The authors thank Saif Haque for his contributions to the study from which this one developed and Kristi Overgaard for her assistance with manuscript preparation and submission.
Final revision submitted March 26, 2026; accepted April 11, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Akron Children's Hospital (2022-138).