
Abstract
Background:
Knee osteoarthritis (KOA) is a common degenerative condition that leads to pain, disability, and reduced quality of life. Medial opening-wedge high tibial osteotomy (MOWHTO) is a surgical procedure designed to correct alignment and alleviate symptoms by redistributing load. While previous studies have focused on the coronal plane, the impact of MOWHTO on sagittal plane biomechanics and trunk posture remains unclear.
Hypothesis/Purpose:
The purpose of this study was to evaluate 3-dimensional biomechanical changes in the knee joint and trunk posture after MOWHTO. It was hypothesized that MOWHTO would result in significant biomechanical changes not only in the coronal plane but also in the sagittal plane, along with changes in trunk posture.
Study Design:
Case series; Level of evidence, 4.
Methods:
This retrospective study included 55 patients (55 knees) with medial compartment KOA (Kellgren-Lawrence grade ≥2) who underwent MOWHTO. Preoperative and postoperative gait analyses were conducted using a 3-dimensional motion capture system and force plates to assess knee joint kinetics and kinematics including trunk posture. Knee joint moments (knee adduction moment [KAM], knee flexion moment [KFM], and knee rotation moment [KRM]) and total joint moment (TJM), along with relative contributions of each moment, were assessed. Radiographic parameters such as hip-knee-ankle (HKA) angle, percentage of mechanical axis (%MA), and femorotibial angle (FTA) were evaluated. Clinical outcomes were assessed using the Japanese Knee Osteoarthritis Measure and Knee Society Score. Paired t tests were performed for statistical analysis between pre- and postoperative results. A P value <.05 was considered statistically significant.
Results:
Postoperatively, significant reductions in KAM (P < .01) and TJM (P < .001) were observed, with a shift in the proportional contribution from KAM to KFM. KFM remained unchanged pre- and postoperatively. Knee varus angles decreased (P < .01), and trunk flexion angles significantly decreased, indicating better postural alignment (P < .01). Radiographic analysis demonstrated increased HKA angles and %MA, along with reduced FTA (P < .01). Clinical outcomes showed significant pain relief and functional improvement (P < .01).
Conclusion:
MOWHTO was associated with significant changes in 3-dimensional gait biomechanics, including knee joint moments and trunk posture, highlighting its comprehensive role in restoring functional alignment in patients with medial compartment KOA, although the case series design may limit generalizability.
Keywords
Knee osteoarthritis (KOA) is a degenerative disease that affects >300 million individuals worldwide. 55 In its advanced stages, KOA leads to joint dysfunction, malalignment, stiffness, deformity, and knee flexion contracture.8,47 These pathological changes culminate in persistent pain, restricted daily activities, and disability, particularly among older patients, contributing to frailty and adversely impacting healthy life expectancy.1,8,17,39 The onset and progression of KOA are significantly influenced by the mechanical environment of the knee joint. As the disease progresses, changes in knee alignment occur, leading to alterations in the joint's biomechanics. Therefore, a thorough understanding of external knee joint moments is crucial when evaluating the pathology, considering treatment options, and assessing treatment efficacy.
Medial opening-wedge high tibial osteotomy (MOWHTO) is a well-established treatment for patients with medial compartment KOA and varus malalignment, aimed at preserving the joint.19,24,45 This procedure aims to realign the mechanical axis and reduce stress on the medial compartment, ultimately relieving pain, improving joint function, and slowing the progression of KOA. Studies utilizing gait analysis have been conducted for MOWHTO, and most of them focused on changes in coronal alignment. While MOWHTO has frequently been characterized as a 2-dimensional surgical procedure, recent studies suggest that it alters the knee joint environment in 3 dimensions.16,31,53 In particular, changes in the sagittal plane have garnered increasing attention. Several studies have demonstrated that the hinge position and the osteotomy inclination angle in the sagittal plane, as quantified using 3D computed tomography, significantly affect the postoperative posterior tibial slope (PTS).11,16,32 Alterations in PTS may, in turn, influence knee joint kinematics, including knee flexion range of motion (ROM) and dynamic stability. Some reports have suggested that sagittal plane realignment affects KFMs during gait. 31 Nonetheless, the 3-dimensional biomechanical effects of MOWHTO remain poorly understood, and many aspects require further investigation.
In addition, it is known that KOA affects trunk posture. 50 Previous studies have demonstrated that as KOA severity progresses, compensatory trunk flexion during standing and gait becomes more pronounced, likely as an adaptive strategy to reduce knee joint loading and pain.42,48,50 In severe cases of KOA, knee varus deformity, knee contracture, and trunk flexion may occur, potentially contributing to sagittal imbalance. These findings suggest that trunk posture reflects compensatory biomechanical adaptations associated with disease progression. However, although the relationship between KOA severity and trunk posture has been described, it remains unclear how surgical realignment procedures such as MOWHTO influence these compensatory mechanisms during gait. This gap in the literature motivated the present study. If MOWHTO may be associated with changes in trunk flexion, it is important to consider treatment strategies that account for other joints and overall balance. Understanding this relationship could greatly enhance the ability to devise optimal treatment strategies.
Therefore, the present study aimed to clarify the change in 3-dimensional knee joint biomechanics and trunk posture after MOWHTO. We hypothesized that MOWHTO changes knee biomechanics 3-dimensionally and is associated with changes in trunk posture.
Methods
This retrospective study was produced in accordance with our institutional ethics policy. The institutional review board of Hakodate Orthopedic Clinic approved this study (No. HOC-C03). The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed written consent was obtained from all patients for providing patient information and any accompanying supplements and for publication.
Participants
From February 2016 to November 2019, patients aged >40 years who were diagnosed with medial compartment KOA in at least 1 knee and who underwent MOWHTO and were able to perform gait analysis pre- and postoperatively were included in the study. KOA was defined as Kellgren-Lawrence (K-L) grade 27 ≥2 on radiographs, along with clinical findings, including knee pain, consistent with KOA. At our institution, the hip, ankle, and spine are routinely evaluated at the initial consultation through medical history taking and clinical examination. In addition, full-length standing radiographs of the lower extremities and spinal radiographs obtained for preoperative anesthetic assessment were reviewed. Based on these evaluations, patients with hip or ankle osteoarthritis (OA) or spinal disorders that could potentially influence gait biomechanics were excluded. Patients with disability preventing walking without support, predominantly lateral compartment KOA, neurological deficits, or any previous fractures were excluded from the study. Patients who underwent any previous orthopaedic surgery were also excluded from this study. Patients aged ≤70 years were indicated for MOWHTO when they had symptomatic medial compartment KOA (K-L grade 2 or 3) with varus malalignment that was refractory to nonoperative treatment. Patients were included only when the lateral tibiofemoral compartment and patellofemoral joint were asymptomatic and showed no radiographic evidence of OA.
Preoperative Planning
Preoperative planning was performed using the Miniaci method as previously described.35,44,54 An appropriate correction angle of the tibia is determined through use of a standing, full-length, lower limb anteroposterior radiograph. The percentage of mechanical axis (%MA), which represents the intersection point between the mechanical axis—a line drawn from the center of the femoral head to the center of the ankle—and the tibial plateau, expressed as a percentage from the medial edge (0%) to the lateral edge (100%), was also measured. A line was drawn from the center of the femoral head passing through a point located at 62.5% of the tibial plateau width from the medial edge. The hinge point was located at approximately 5 mm medial from the tibiofibular joint on the lateral tibial condyle. From the hinge point P, a second line was drawn to the center of the talar dome. Using the hinge point as the center and the length of this line as the radius, we created an arc to intersect the first line. The line connecting the hinge point and the intersection point defined the correction line, and the angle between this line and the line to the talar dome represented the medial opening-wedge correction angle.
Surgical Treatment
All surgeries were performed at a single institution by a single senior attending surgeon (K.S.) who was sufficiently trained in sports medicine fellowship. Surgery was performed under general anesthesia. Arthroscopy was performed before osteotomy to confirm the indication for HTO.
The MOWHTO procedure was performed as previously described. 40 The proximal tibia was exposed through a 7-cm medial longitudinal incision. After complete release of the distal attachment of the superficial medial collateral ligament, 3 pairs of Kirschner wires were inserted into the tibia using a parallel guide from the pes anserinus notch toward the proximal tibiofibular joint for accurate osteotomy and hinge fracture prevention. A biplanar tibial osteotomy was then performed, and the osteotomy gap was gradually opened according to the preoperatively planned correction angle using a dedicated spreader (Olympus Terumo Biomaterials). The opening gap was calculated using trigonometric calculations based on the tibial osteotomy length and the target correction angle. Under fluoroscopic guidance, a long alignment rod connecting the center of the femoral head and the center of the ankle joint was used to confirm the mechanical axis. The correction was adjusted until the mechanical axis passed through 62.5% of the tibial plateau width from the medial edge. Two wedge-shaped β-tricalcium phosphate spacers (Osferion 60; Olympus Terumo Biomaterials) were inserted into the osteotomy gap, and the osteotomy was stabilized with a locking plate (Tomofix; DePuy Synthes) using 8 locking screws
Physical and Radiological Evaluation
Knee ROM was measured for physical evaluation. Radiological evaluation was assessed by a single, blinded, sufficiently trained orthopaedic surgeon using anteroposterior radiographs. Radiographic parameters included hip-knee-ankle (HKA) angle, femorotibial angle (FTA), and %MA in full-length bilateral standing anteroposterior radiographs, and PTS angle 52 in the lateral view. As for the clinical score, visual analog scale (VAS; %), Japanese Knee Osteoarthritis Measure (JKOM), 2 and the Knee Society Score (KSS) 46 were used.
Gait Analysis
The participants performed 3 sets of overground walking trials at their self-selected normal walking speeds. Gait data were collected as described previously.5,25,36,50 Gait motion data were captured using a 3-dimensional motion analysis system with 8 infrared light cameras (ProReflex; Qualisys AB). Ground-reaction force was measured in 3 dimensions in the global coordinate system using 2 multicomponent force plates (OR6; Advanced Mechanical Technology) embedded in an 8-m walkway. Motion and force data were synchronized and collected at 120 Hz. Three-dimensional motion data were processed using Qualisys Track Manager 3D (Qualisys AB). Force data were used for identifying heel strike time in each gait cycle. The gait cycle was defined as the interval between heel strikes on the ipsilateral side.
Kinematic data were collected using the point cluster technique as previously described. 15 A total of 56 light-reflective markers, 14 mm in diameter, were placed by physical therapists well trained in localizing the anatomical landmarks and were used to calculate knee motion in 6 degrees of freedom with no constraints, as previously described. 22 The markers were arranged on 2 limb segments, creating separate cluster groups of 13 markers on the thigh and 15 on the shank. 3 The angle of trunk flexion was calculated as the angle between the vertical axis and the line segment connecting the midpoints of both acromion markers and the midpoint of the bilateral anterior superior iliac spine markers in the sagittal plane of the global coordinate system, as previously described.23,50 The software application BioMove (Stanford University) was used to calculate the joint kinetics during walking. External joint moments were calculated using standard inverse dynamics and normalized to each participant's body weight and height. 10 Each gait cycle was time-normalized to 100% of the gait cycle, where the initial contact of a limb inside a force plate was defined as 0%, and the following ground contact of the same limb was defined as 100%.
The values extracted from 3 walking trials were averaged. The extracted external knee joint moments included knee adduction moment (KAM), knee flexion moment (KFM), and knee rotation moment (KRM).9,37 Similar to the knee index, the total joint moment (TJM) was calculated during each frame of the stance phase by taking the square root of the sum of the squares of the KFM, KAM, and KRM (TJM = √(KAM 2 + KFM 2 + KRM 2 ). The first peak of TJM (TJM1) was defined as the maximum TJM during the first half of the stance, and the second peak of TJM (TJM2) was defined as the maximum TJM during the second half of the stance. At the time of the TJM peaks, the proportions of KFM (%KFM), KAM (%KAM), and KRM (%KRM) contributing to the TJM were calculated as the square of the planar moment at the time of the peak divided by the square of the total moment at the time of the peak, multiplied by 100 (%KAM = KAM 2 /TJM 2 *100). 5
Statistical Analysis
Radiographic measurements were independently performed by 2 orthopaedic surgeons (Y.S. and Y.O.). To assess measurement reliability, intra- and interobserver reliability were evaluated using intraclass correlation coefficients (ICCs). ICC values were calculated based on a 2-way random-effects model for absolute agreement. Statistical tests for comparing pre- and postoperative kinetic and kinematic data were assessed using paired t tests. Specifically, the first and second peaks of KAM, KFM, KRM, and TJM during the stance phase were extracted for each participant. Chi-square analysis followed by Bonferroni test was used for analyzing relative contributions of each moment component. To assess whether the observed changes extended beyond discrete peak values, we performed supplementary waveform analyses using statistical parametric mapping (SPM), with the SPM1D package (Version 0.4; www.spm1d.org 41 ) implemented in MATLAB (MathWorks). Time-normalized waveforms (0%-100% of the gait cycle for kinematics) were compared between preoperative and postoperative conditions using SPM{t} paired t tests. To evaluate whether the postoperative increase in gait speed influenced our findings, we performed a supplementary linear regression analysis with gait speed change (postoperative minus preoperative) as a covariate. For each outcome, the change score was regressed on gait speed change, and the speed-adjusted mean change (intercept) was tested for significance. All analyses were performed using the JMP software (SAS). A P value <.05 was considered statistically significant. All figures were made by Adobe Illustrator CC 2020.
Results
Patient Characteristics and Surgical Outcomes
A total of 4,883 patients (6,203 knees) were diagnosed with KOA at our facility from February 2016 to November 2019. MOWHTO was performed in 91 patients (99 knees) during the period. Of these, 36 patients (44 knees) were excluded due to exclusion criteria. Therefore, 55 patients (55 knees; 25 male, 30 female) were eligible for this study (Figure 1). The descriptive data and surgical outcomes of the participants are shown in Table 1. Intraobserver reliability was excellent for all parameters (ICC, 0.98 to 0.99), and interobserver reliability was also high (ICC, 0.97 to 0.98), indicating good reproducibility of the radiographic measurements. The mean age was 58.2 ± 6.1 years (range, 46 to 68 years), and the mean BMI was 26.6 ± 2.8 kg/m2 (range, 21.7 to 34.9 kg/m2). The mean postoperative follow-up interval at the time of gait analysis was 12.4 ± 1.6 months (range, 11 to 17 months). Gait speed increased from 1.16 ± 0.16 m/s (range, 0.72 to 1.51 m/s) to 1.24 ± 0.17 m/s (range, 0.93 to 1.60 m/s) (P < .01). Radiographic parameters showed that the mean HKA angle increased from −3.8°± 2.5° (range, −8.0° to −0.1°) to 3.6°± 1.2° (range, 0.5° to 6.4°) (P < .01), the mean %MA increased from 32.8% ± 9.2% (range, 8.0% to 49.4%) to 63.6% ± 6.2% (range, 47.5% to 77.1%) (P < .01), and the mean PTS increased from 8.9°± 3.2° (range, 74.1° to 90.4°) to 11.4°± 3.4° (range, 71.2° to 88.8°) (P < .01), whereas the mean FTA decreased from 178.6°± 2.0° (range, 173.7° to 183.8°) to 171.4°± 2.2° (range, 165.6° to 175.5°) (P < .01). All patient-reported outcome measures improved significantly, with the mean VAS score decreasing from 52.3 ± 25.4 (range, 8 to 100) to 11.8 ± 13.2 (range, 0 to 61) (P < .01), the mean JKOM score decreasing from 33.5 ± 13.9 (range, 11 to 66) to 11.2 ± 7.5 (range, 1 to 29) (P < .01), and the mean KSS increasing from 90.8 ± 21.0 (range, 53 to 137) to 132.8 ± 22.9 (range, 84 to 174) (P < .01). No significant difference was observed in mean knee ROM (136.4°± 20.3° [range, 0° to 155°] vs 136.7°± 20.5° [range, −5° to 155°]; P = .44).
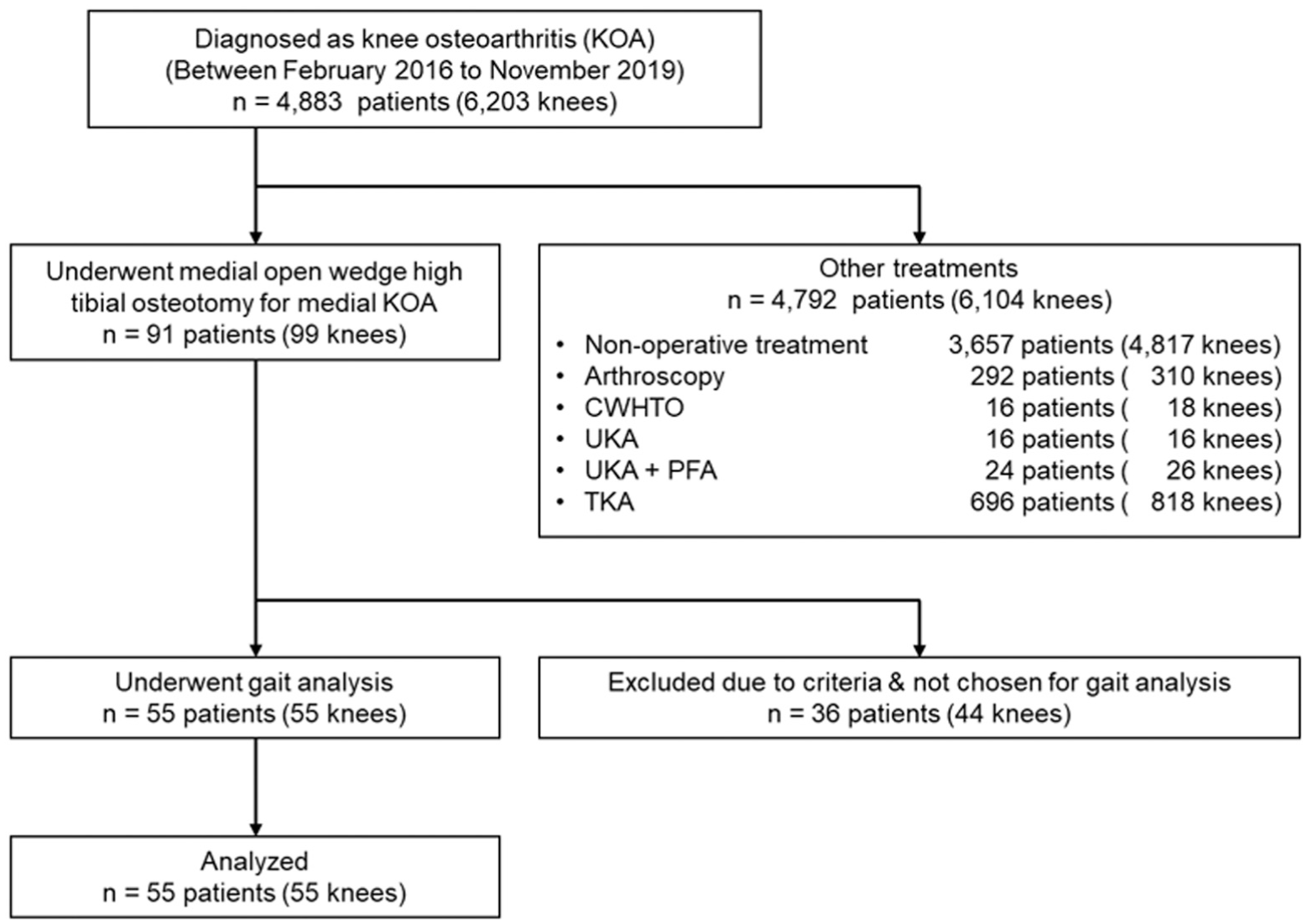
Flowchart of the present study.
Background and Radiographic Data of Participants a
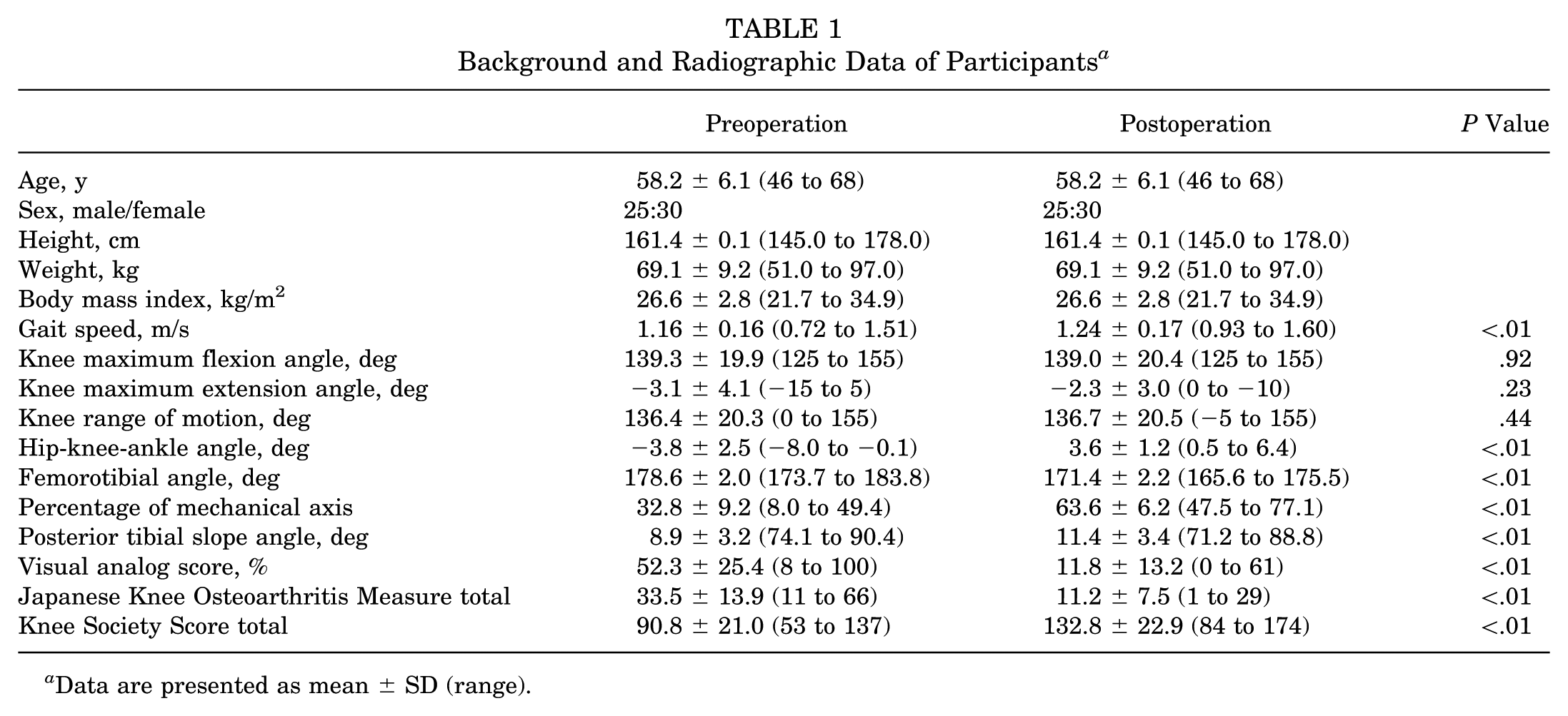
Data are presented as mean ± SD (range).
Kinetics
External Knee Moments
KAM and KFM both showed bimodal peak patterns at early- and late-stance phases pre- and postoperatively (Figure 2, A and B). KAM was lower at both the first and second peak values postoperatively compared with preoperative values (P < .0001). KFM showed the moment peak during the loading response phase and then decreased and converted to the extension moment in the midstance phase, followed by the second peak in the late-stance phase both pre- and postoperatively. There was no significant difference between pre- and postoperative KFMs. KRM showed transition from a positive value in the early-stance phase to a negative value in the late-stance phase (Figure 2C). KRM was significantly higher postoperatively at the first peak (P < .001).
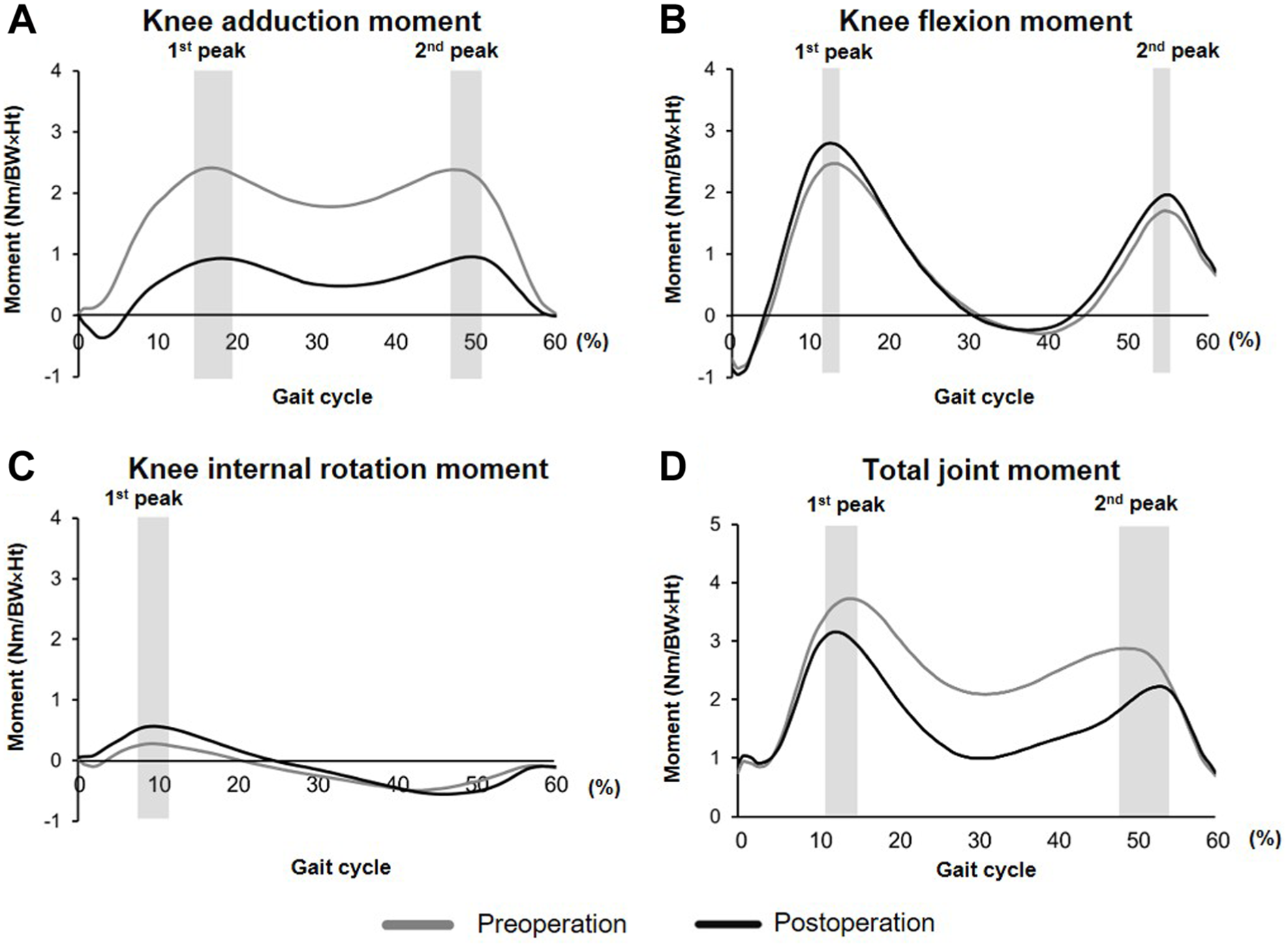
Pre- and postoperative external knee moments and total joint moments (TJMs). (A) The knee adduction moment significantly decreased postoperatively compared with preoperative values at both the first and second peaks (P < .0001). (B) There was no significant difference in knee flexion moment between the pre- and postoperative periods. (C) The knee rotation moment increased at the first peak postoperatively (P < .0001). (D) The TJM significantly decreased at the first and second peaks postoperatively (P < .0001). BW, body weight; Ht, height; Nm, number.
TJM and Relative Contributions of Each Moment Component
TJM showed bimodal peak patterns through the stance phase before and after surgery (Figure 2D). TJM was significantly lower postoperatively compared to preoperatively at the first peak and second peaks (P < .0001). Referring to relative contribution, %KAM decreased and %KFM significantly increased at both peaks postoperatively (Figure 3, A and B) (P < .001). As a result, preoperative KAM dominance changed to KFM dominance postoperatively at TJM2. Additionally, %KRM significantly increased at the TJM first peak (P < .001).
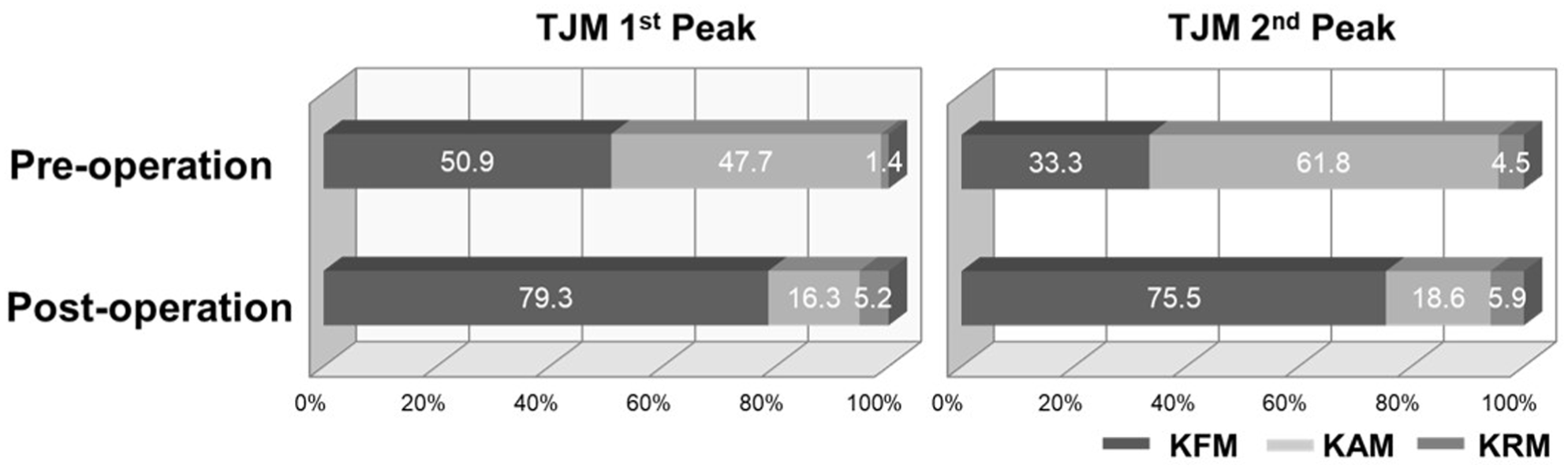
Pre- and postoperative relative contributions of each moment component at the first and second total joint moment (TJM) peak. Pre- versus postoperative knee adduction moments (KAMs) in both the first and second peaks (P < .0001). Pre- versus postoperative knee flexion moments (KFMs) in both the first and second peaks (P < .0001). Pre- versus postoperative knee rotation moments (KRMs) in the first peak (P < .0001).
Kinematics
For kinematics over the gait cycle, knee flexion angle showed a similar bimodal peak pattern during the gait cycle both pre- and postoperatively; there was no significant difference (Figure 4A, Supplementary Figure S1). Knee varus angle significantly decreased postoperatively throughout the gait cycle (P < .001), and knee rotation angle differed across the entire gait cycle (P < .001) (Figure 4B).
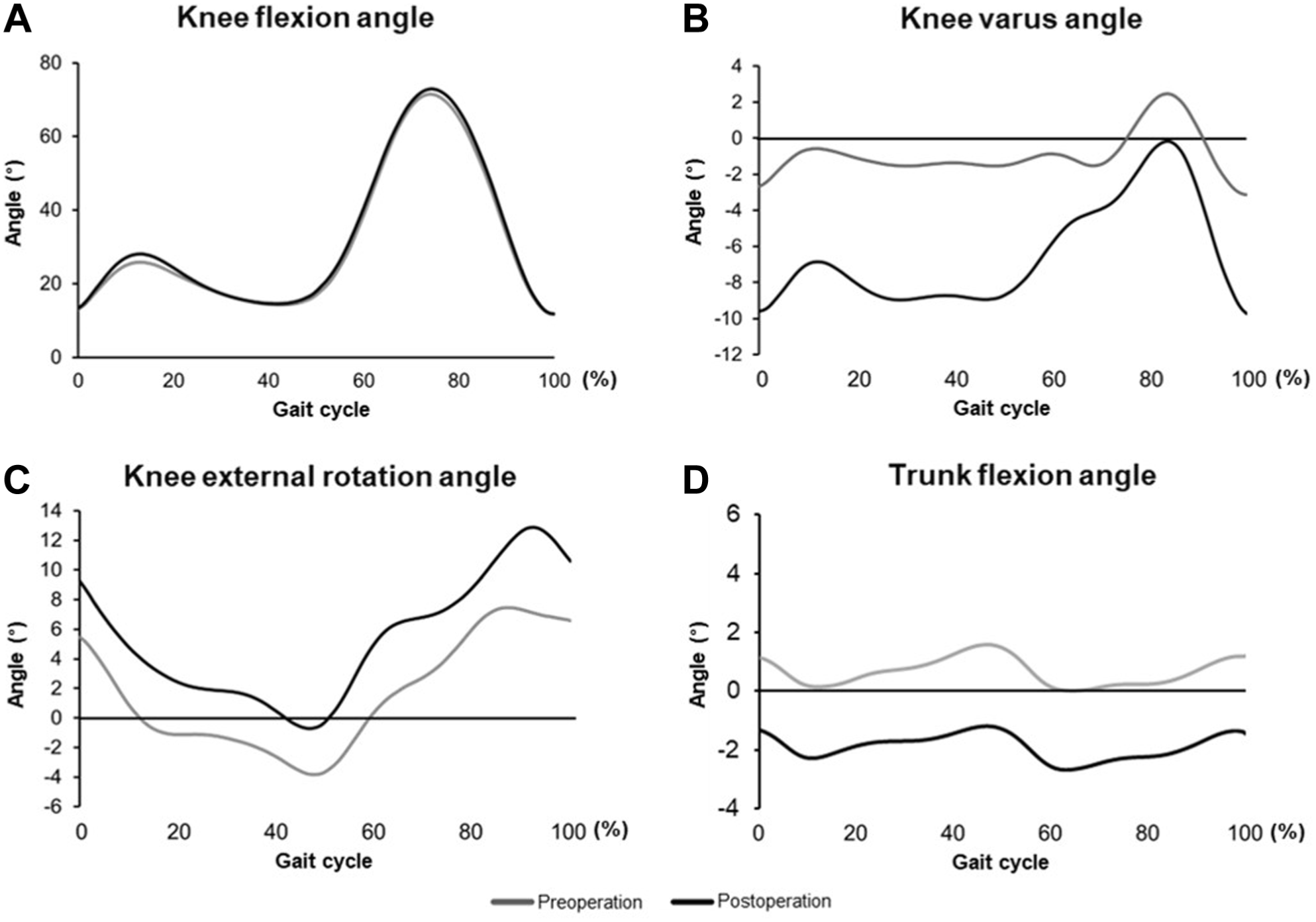
Pre- and postoperative knee kinematics. (A) The knee flexion angle showed no significant difference (P > .05). (B) Knee varus angle. (C) Knee external rotation angle. Both the knee varus and knee external rotation angles were small and large postoperatively throughout the gait cycle (P < .01). (D) Trunk flexion angle decreased throughout the gait cycle postoperatively (P < .01).
Trunk Posture
Trunk flexion angle showed a negative peak in the early-stance phase and then a positive peak in the late-stance phase pre- and postoperatively (Figure 4D). Trunk flexion significantly decreased postoperatively throughout the gait cycle (P < .01).
Results After Adjustment for Gait Speed
To account for the potential influence of gait speed, additional analyses were performed adjusting for changes in gait speed. After adjustment, all results were consistent with the original analyses. The reductions in KAM (first peak: adjusted P < .001; second peak: adjusted P < .001), TJM (first peak: adjusted P < .001; second peak: adjusted P < .001), and trunk flexion angle (adjusted P < .001) all remained statistically significant. KFM showed no significant change after adjustment (first peak: P = .642; second peak: P = .919). Gait speed change was not a significant predictor of changes in KAM (P = .395 and P = .252) or trunk flexion (P = .772), but was significantly associated with changes in KFM (P < .001 and P = .002) and TJM (P < .001 and P = .001).
Discussion
We investigated the 3-dimensional biomechanical changes before and after MOWHTO. Postoperatively, both KAM and %KAM decreased, whereas %KFM increased along with KFM2, although KFM1 remained unchanged. TJM also decreased after surgery, indicating an overall reduction in knee joint load. In terms of kinematics, the knee varus angle decreased postoperatively. Additionally, the trunk flexion angle decreased postoperatively compared to the preoperative angle.
MOWHTO is a surgical procedure that corrects knee varus alignment to valgus alignment, shifting load from the medial compartment to the lateral compartment and reportedly reducing KAM.26,28 This KAM reduction may result from a shortened moment arm, as previously described. 49 In this study, postoperative increases in HKA and %MA, along with a decrease in KAM, confirmed that MOWHTO achieves corrective effects in the coronal plane, consistent with previous findings. 29
In medial KOA, previous studies have demonstrated a strong correlation between pain and elevated KAM.6,14 Consistent with these findings, our study showed postoperative pain relief according to patient-reported outcomes. During midstance, the body's weight shifts onto the affected limb due to single-leg support. 4 Alignment correction, which reduced the KAM, might lead to pain relief and allow for adequate weightbearing on the affected limb, thereby improving function and increasing walking speed. Postoperatively, the TJM also decreased significantly, likely due to the reduction in KAM, as KAM accounted for the largest portion of the preoperative joint moment. Thus, MOWHTO was associated with a reduction in KAM through both pain relief and alignment correction.
The impact of MOWHTO on KFM has been reported previously. Lind et al 33 conducted gait analysis on 11 patients with medial KOA who underwent MOWHTO, noting an increase in both knee flexion angle and KFM after surgery. Similarly, da Silva et al 13 compared gait dynamics before and 6 months after MOWHTO and found a decrease in knee extension angle and an increase in KFM. On the other hand, Marriott et al 34 conducted gait analysis 5 years after MOWHTO and reported a decrease in KFM. Consistent with our findings demonstrating a postoperative increase in PTS, previous studies have reported that changes in tibial slope influence knee joint kinematics and loading conditions, particularly in the sagittal plane. 7 MOWHTO addresses not only coronal plane deformities but also sagittal plane alignment. 16 The variability in postoperative KFM findings across studies may be attributed to factors influencing KFM, such as body weight, walking speed, knee flexion angle, PTS angle, and trunk posture.
Several factors can influence the KFM, including quadriceps activity, pain, gait speed, PTS, and trunk inclination. In this study, all these parameters changed postoperatively in ways that could have competing effects on KFM, and although the mean KFM value increased postoperatively, our study showed no significant difference between pre- and postoperative KFMs. This may be because multiple factors contribute to KFM in different ways, and both the magnitude and direction of the knee flexion-extension moment vary substantially throughout the stance phase.12,56 Pain relief, as reflected by improved VAS scores, may have enabled increased quadriceps activation and more physiological knee loading during gait, which could contribute to an increase in KFM.18,38,43 Similarly, the observed increase in gait speed is known to be associated with higher joint moments and may also have contributed to increased KFM. 21 In contrast, the increase in PTS may have altered sagittal plane mechanics in a more complex manner. Increased PTS has been reported to facilitate anterior tibial translation and modify the quadriceps-hamstring force balance, thereby influencing knee flexion-extension moments during gait. 20 However, the effect of increased PTS on KFM is not unidirectional and is likely context dependent. While increased PTS may increase flexion demand in some conditions, it may also redistribute joint loading or alter moment arms, potentially reducing or masking changes in KFM. In addition, improvements in trunk posture may have reduced compensatory forward inclination, which can also influence sagittal plane loading. Taken together, these opposing influences may have resulted in a net effect in which absolute KFM did not change significantly despite multiple biomechanical alterations. This complexity may also explain why previous studies have reported inconsistent findings regarding KFM changes after MOWHTO. In contrast, KAM is largely influenced by the knee varus angle, and changes in this angle may have a more direct effect on KAM outcomes.
Preoperatively, KFM values were likely lowered as a compensatory response to trunk flexion, potentially reducing compressive forces on the tibiofemoral and patellofemoral joints to alleviate pain. However, this posture negatively impacted both the back and knees. 50 Trunk flexion is known to occur as a consequence of limited knee joint ROM or pain.30,50 In the present study, trunk flexion improved by approximately 3° after surgery, accompanied by a significant reduction in postoperative VAS scores, suggesting that the improvement in trunk inclination may be associated with pain relief.30,51 Postoperative pain relief may enable better knee function, evidenced by improved clinical scores, while the resolution of trunk flexion may be associated with improved overall posture. Although the reduction in trunk flexion angle was relatively small (approximately 2°-3°), even modest changes in trunk posture may be clinically meaningful. Previous studies have suggested that trunk flexion is a compensatory strategy associated with pain and altered knee loading.50,51 Therefore, its improvement may reflect a reduction in compensatory mechanisms and contribute to better overall postural alignment and functional mobility. This reduction in compensatory mechanisms may help alleviate the cycle of adverse effects on both the knee and the back.
Kuwahara et al 30 reported that excessive trunk flexion during gait was reduced after total knee arthroplasty (TKA) in patients with medial KOA, indicating a shift toward a more upright trunk posture. In the present study, trunk flexion also decreased postoperatively after MOWHTO, suggesting a similar reduction in compensatory trunk flexion. In the present study, trunk flexion also decreased postoperatively after MOWHTO, which is consistent with the concept that surgical treatment for medial KOA may be associated with improvements in proximal gait adaptations. However, the clinical background and biomechanical objectives differ between TKA and MOWHTO. Whereas TKA replaces the articular surface in end-stage disease, MOWHTO preserves the native joint and primarily aims to realign the lower limb. Therefore, the similarity in postoperative trunk changes should be interpreted cautiously as an association rather than a shared causal mechanism. These findings suggest that trunk-related adaptations are an important component of postoperative gait changes after knee surgery.
Asay et al 5 examined the relationship between KOA progression and gait changes over a 5-year period in patients with medial KOA, introducing and emphasizing the importance of considering relative contribution in kinetics. In this current study, although KFM itself did not change, the contribution rates shifted significantly postoperatively, with %KAM decreasing and %KFM increasing. Relative contribution reflects the proportion of each moment component relative to the TJM, and %KAM, %KFM, and %KRM are influenced not only by their own magnitudes but also by changes in the other moment components. Therefore, changes in relative contribution do not necessarily correspond to changes in the absolute magnitude of each moment. MOWHTO is believed to have indirectly induced changes in the mechanical environment in the sagittal plane. Kinetic patterns change in stage 2 KOA, before the onset of deformities, with %KFM dominating in stage 2 and %KAM in stage 3. 50 This finding suggests that HTO may restore biomechanics to a state resembling the preonset stage of early KOA, supporting its effectiveness in addressing initial biomechanical changes in KOA. By introducing the concept of relative contribution, we highlighted the postoperative shift from KAM to KFM. While MOWHTO is typically considered a procedure to improve coronal plane parameters in medial KOA, our findings suggest it also has a significant impact on sagittal plane parameters, indicating a 3-dimensional effect on the mechanical environment of the knee joint during gait. Importantly, the increase in %KFM does not indicate an increase in the absolute magnitude of KFM. In the present study, absolute KFM did not change significantly postoperatively. Rather, the observed shift reflects a redistribution of joint moment contributions, likely due to the reduction in KAM. Therefore, evaluation of relative contribution provides complementary information on 3-dimensional load distribution, rather than absolute loading.
The present study provides novel insight into the biomechanical effects of MOWHTO by integrating 3-dimensional joint moment analysis with relative moment contribution and trunk posture assessment. To our knowledge, no previous study has simultaneously combined these approaches within a single cohort. While changes in sagittal plane kinetics and kinematics were modest in terms of absolute magnitude, the analysis revealed a significant redistribution of joint moment contributions, with a shift from %KAM dominance to %KFM dominance. This indicates that sagittal plane loading became relatively more important within the overall joint moment environment, despite minimal changes in absolute values. Furthermore, the observed reduction in trunk flexion suggests that the biomechanical effects of MOWHTO extend beyond the knee joint, reflecting alterations in global gait strategy. Together, these findings provide a more comprehensive understanding of how MOWHTO influences 3-dimensional gait mechanics beyond conventional coronal plane evaluation.
There are several limitations to the present study. First, the number of participants is small. However, the primary aim of this study was to clarify the biomechanical changes associated with MOWHTO, and comparison of pre- and postoperative data led to meaningful new findings. Second, the present study is a case series without a control group, which may limit generalizability and leave the extent to which MOWHTO restores nonpathological kinetics postoperatively unclear. Nonetheless, our focus was primarily on the differences between pre- and postoperative conditions, and we have elucidated the biomechanical advantages in this context. Finally, we used self-selected walking speeds for gait analysis. Gait parameters are sensitive to walking speed; however, imposing a fixed speed could itself alter natural gait characteristics. To address this, we performed a supplementary analysis with gait speed change as a covariate and confirmed that all primary findings remained robust after adjustment. Given the longitudinal, within-participant design and the consistent results of the speed-adjusted analysis, we consider this limitation substantially mitigated. Moreover, we assessed not only changes in external moments but also the relative contributions of each moment, along with kinematic data, and trunk flexion providing new insights into the effects of MOWHTO.
Conclusion
This study elucidated the 3-dimensional biomechanical changes during gait before and after MOWHTO. We found that MOWHTO reduces the overall load on the knee joint and, by decreasing KAM, results in a transition from %KAM dominance to %KFM dominance. Additionally, the trunk flexion observed preoperatively decreased postoperatively, indicating that MOWHTO not only affects the biomechanics in the coronal plane but also is associated with changes in the sagittal plane. These findings indicate that MOWHTO significantly impacts the gait in 3-dimensional moment changes and is associated with changes in trunk flexion.
Footnotes
Appendix
Acknowledgements
The authors have no financial or proprietary interest in the subject matter of this article. Special thanks to Akane Iwadate and our health care team members for their efforts and valuable assistance.
Final revision submitted March 30, 2026; accepted April 11, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Hakodate Orthopedic Clinic.
Data Accessibility Statement
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.