
Abstract
Background:
Anterior tibial translation (ATT) is a reported risk factor for residual pivot shift after anterior cruciate ligament (ACL) reconstruction. However, longitudinal postoperative changes in ATT are not well defined. This study aimed to evaluate the longitudinal changes in postoperative static ATT assessed under weightbearing conditions and to identify prognostic factors associated with residual static ATT.
Purpose:
To evaluate the longitudinal changes in postoperative static ATT assessed under weightbearing conditions and to identify prognostic factors associated with residual static ATT.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent primary anatomic ACL reconstruction between 2017 and 2023 with a minimum follow-up of 24 months were included. Static ATT was measured using lateral weightbearing radiographs preoperatively and at 6, 12, and 24 months postoperatively. A linear mixed-effects model estimated marginal predicted changes in static ATT over time, and additional mixed-effects models identified prognostic factors associated with postoperative static ATT. The association between postoperative static ATT at 24 months and residual postoperative pivot shift was analyzed.
Results:
In total, 95 patients were included. Static ATT significantly decreased at 6 months compared with preoperative values (P < .01) and remained stable at 12 and 24 months, with no significant differences among the postoperative time points. The predicted change in static ATT from preoperative to 24 months was −1.32 mm (95% CI, −1.93 to −0.70; P < .01). Multivariate linear mixed-effects regression analysis revealed that female sex (estimate, 1.45 mm; P = .03) and a greater lateral posterior tibial slope (estimate, 0.28 mm per degree; P = .01) were independently associated with increased postoperative static ATT. At 24 months, greater static ATT was associated with residual pivot shift (odds ratio, 1.45; 95% CI, 1.10-1.92; P = .01).
Conclusion:
Static ATT improved after ACL reconstruction and remained stable through 24 months. Female sex and a steeper lateral PTS were independently associated with less postoperative improvement in static ATT. Greater postoperative static ATT was also associated with residual pivot shift.
Keywords
Despite generally favorable outcomes after anterior cruciate ligament (ACL) reconstruction, residual instability and graft failure remain important clinical concerns. Anterior tibial translation (ATT) has been proposed as a potential contributor to these unfavorable outcomes.16,27 ACL deficiency allows anterior displacement of the tibia relative to the femur, and ATT represents an abnormal sagittal-plane tibiofemoral relationship. ATT is typically assessed using magnetic resonance imaging or radiography, whereas dynamic instability is evaluated using the pivot shift and Lachman tests. Several factors, including revision surgery,14,32 posterior tibial slope (PTS),4,28 injury chronicity,8,21 and meniscal lesions,17,35 have been reported to increase ATT. Increased ATT is associated with a positive preoperative pivot shift, which is considered one of the most clinically relevant indicators of knee stability. 13 More recently, static ATT has been recognized as a measure of ATT under weightbearing conditions. 6 Excessive preoperative static ATT has been linked to residual pivot shift or graft failure. 20 However, the clinical significance of postoperative static ATT remains unclear.
Although anatomic ACL reconstruction restores knee stability and improves the abnormal tibiofemoral relationship, 18 longitudinal changes in ATT after surgery have not been well characterized. Prior studies have primarily examined the relationship between preoperative ATT and clinical outcomes,20,27 and no study has longitudinally evaluated changes in static ATT after anatomic ACL reconstruction.
The primary purposes of this study were (1) to evaluate the longitudinal changes in static ATT after ACL reconstruction and (2) to identify prognostic factors associated with postoperative static ATT. A secondary purpose was to examine the association between postoperative static ATT and the pivot shift test. We hypothesized that anatomic ACL reconstruction would reduce static ATT over time but that greater PTS would be associated with increased residual static ATT and a higher likelihood of residual pivot shift.
Methods
This study was approved by the institutional ethical review board, and informed consent was obtained from all participants. A retrospective review of the institutional database was performed from November 2017 to September 2023 to identify patients who underwent primary ACL reconstruction using bone–patellar tendon–bone (BPTB) autografts and had a minimum follow-up of 24 months. Exclusion criteria were (1) posterior tibial sagging or abnormal varus or valgus instability, (2) revision ACL reconstruction before completion of the 2-year follow-up, and (3) inadequate radiographic data for longitudinal assessment of static ATT, defined as <2 available radiographic measurements available across different time points. All procedures were performed by multiple knee surgeons using a standardized surgical technique, with an experienced senior surgeon (S.T.) involved in all the procedures as either the chief surgeon or first assistant.
Radiographic Evaluation
Static ATT was measured on weightbearing lateral radiographs obtained with the patient standing in a monopodal stance with the knee in full extension. 1 Adequate lateral radiographs were defined by superimposition of the posterior femoral condyles. Static ATT was measured as the distance between 2 lines drawn parallel to the posterior tibial cortex: one line tangent to the posterior aspect of the medial tibial plateau and the other tangent to the posterior femoral condyles (Figure 1). 5

Measurement of static anterior tibial translation (ATT) on lateral weightbearing radiographs. A reference line is drawn parallel to the posterior tibial cortex. A second line, parallel to the reference line, is depicted tangent to the most proximal part of femoral condyle. A third parallel line (dotted line) is drawn tangent to the most proximal part of the medial tibial plateau. Static ATT is the shortest perpendicular distance (A) between the line of the femoral condyle and tibial plateau.
PTS was measured separately for the medial and lateral compartments using computed tomography (CT) as previously described. 19 CT scans were obtained at 1 week postoperatively as part of routine follow-up in all patients (institutional protocol) to evaluate bone tunnel position and were not performed specifically for the purposes of this retrospective study. All CT scans were performed using a 320-slice CT scanner (Aquilion ONE; Canon Medical Systems) with a slice thickness of 1 mm. The longitudinal tibial axis was determined on the central sagittal slice using 2 best-fit circles positioned 5 and 10 cm distal to the joint line. Midsagittal images of the medial and lateral compartments were then selected on the coronal view. Medial and lateral PTS were defined as the angle between a line perpendicular to the tibial axis and a line connecting the most proximal anterior and posterior subchondral bone points in each compartment (Figure 2).
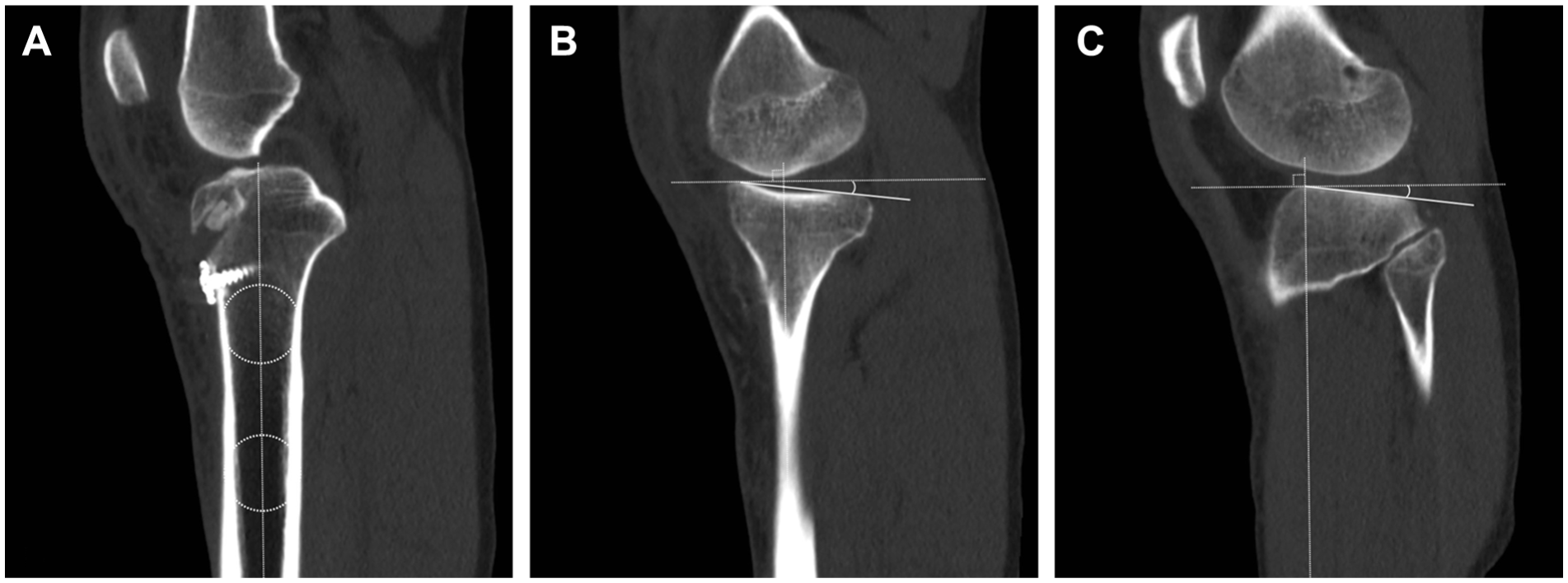
Posterior tibial slope (PTS) measurement on computed tomography images. (A) The longitudinal tibial axis was determined by drawing 2 circles tangent to the anterior and posterior borders at 5- and 10-cm points distal to the joint line. A line connecting the centers of the 2 circles defined the longitudinal tibial axis. (B) Medial PTS was measured as the angle between a line perpendicular to the longitudinal axis and the line connecting the most proximal anterior and posterior subchondral bone points of the medial tibial plateau. (C) Lateral PTS was measured in the same manner using the lateral tibial plateau.
Clinical Evaluation
Covariates included sex, age, body mass index (BMI), time to surgery (within 3 months [acute] vs beyond 3 months [chronic]), meniscal status, and cartilage lesions, defined as International Cartilage Regeneration & Joint Preservation Society grade ≥2 in any compartment. 15 The pivot shift test was assessed preoperatively and at the 24-month postoperative follow-up in the awake state. Pivot shift grades were classified as grade 0 (negative), grade 1 (glide), grade 2 (clunk), and grade 3 (gross). Consistent with previous studies,7,11 a grade of ≥1 was defined as residual pivot shift.
Surgical Procedure
The anatomic rectangular tunnel ACL reconstruction using a BPTB autograft was performed arthroscopically according to the technique described by Shino et al. 26 After a 10 mm–wide autologous BPTB graft was harvested from the central portion of the patellar tendon, the femoral bone plug was shaped into a 6 × 10–mm rectangle. 30 The femoral tunnel was created as posterior and proximal as possible within the ACL femoral footprint, whereas the tibial tunnel was created as anterior and medial as possible within the ACL tibial footprint. Both tunnels were rectangular in shape (6 × 10 mm), created by connecting 2 parallel cylindrical drill holes using a dilator, as previously described. 30
Femoral fixation was achieved using an Endobutton (Smith & Nephew), with the femoral bone plug positioned within the femoral tunnel, with its distal end 1 mm from the intra-articular surface. Tibial fixation was performed using a small double-spike plate (Smith & Nephew) and a half-threaded 5-mm cancellous screw. The tibial bone plug was positioned within the tibial tunnel and secured using a pull-out fixation technique, in which the graft was drawn distally through the tibial tunnel and fixed over the anterior tibial cortex. Graft fixation was completed at 20° of knee flexion using a ligament tensioner that had been calibrated to apply a force equivalent to 80 N at full knee extension. As a result, the actual tension applied at 20° knee flexion varied among patients and ranged from 5 to 20 N.
Postoperative Rehabilitation
Range of motion exercises were initiated immediately after surgery. Partial weightbearing was permitted on postoperative day 2, and full weightbearing was allowed at 1 week. A functional knee brace was worn for 6 weeks postoperatively. Running was permitted at 4 months, and return to sports was allowed at a mean of 8 to 9 months after surgery. In patients who underwent concomitant repair of a meniscus radial tear, full weightbearing was delayed until 6 weeks. Other rehabilitation routines and daily activities were adjusted accordingly.
Statistical Analysis
Statistical analyses were performed using R software (Version 4.5.1; R Foundation for Statistical Computing). Longitudinal changes in static ATT were analyzed using a linear mixed-effects model (lme4 package) with a random intercept for each patient. Estimated marginal mean values of static ATT over time were calculated for the entire cohort. Pairwise comparisons between time points were performed using estimated marginal means derived from the linear mixed-effects model with Bonferroni adjustment for multiple comparisons (emmeans package).
To identify prognostic factors associated with residual static ATT at 24 months, candidate predictors were initially evaluated using univariate linear mixed-effects regression. Variables with P < .25 in the univariate analysis were considered potential predictors. 10 Age, sex, and BMI were included in all multivariate models as a priori adjustment variables.
The association between static ATT at 24 months and postoperative residual pivot shift was examined using binary logistic regression. A 2-sided P value <.05 was considered statistically significant.
To assess measurement reliability, 20 knees were randomly selected from the study cohort. For intraobserver reliability, the primary examiner (an experienced orthopaedic surgeon) repeated all measurements after a 1-month interval, blinded to the initial results. For interobserver reliability, a second independent examiner (also an experienced orthopaedic surgeon) performed the measurements in a blinded manner. Intraclass correlation coefficients (ICCs) were calculated using a 2-way random-effects model with absolute agreement (single measures) for static ATT, medial PTS, and lateral PTS. Intraobserver reliability demonstrated excellent agreement, with ICC values of 0.96 for static ATT, 0.95 for medial PTS, and 0.95 for lateral PTS. Interobserver reliability was also excellent, with ICC values of 0.95 for static ATT, 0.93 for medial PTS, and 0.92 for lateral PTS.
Results
In total, 112 patients who underwent primary ACL reconstruction with a BPTB autograft were initially enrolled. Seventeen patients were excluded based on the predefined exclusion criteria: four patients for criterion 1, two patients for criterion 2, and 11 patients for criterion 3. Consequently, 95 patients were included in the final analysis (Figure 3). The cohort consisted of 54 male and 41 female participants, with a mean age of 28.9 years (range, 15-66 years). Patient characteristics and surgery-related variables are summarized in Table 1.
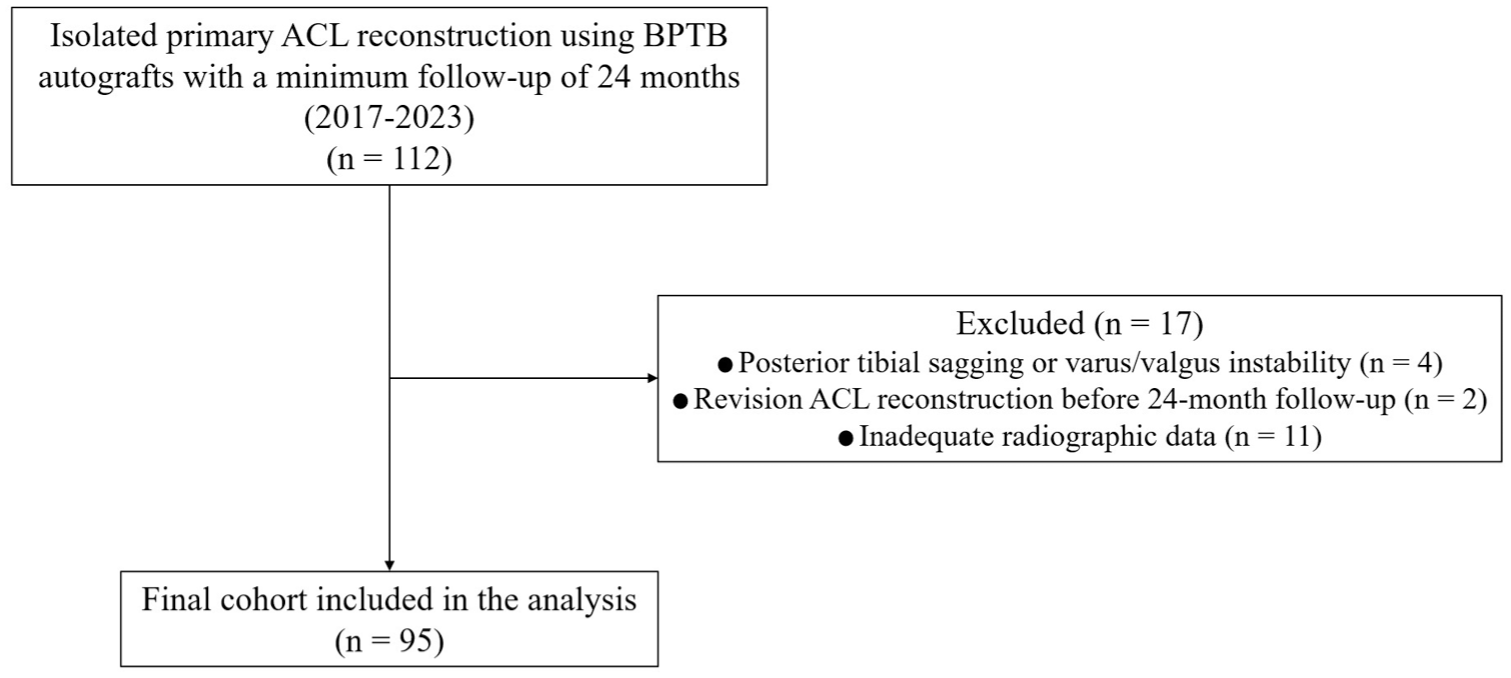
Flow chart for patient inclusion and exclusion. ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone.
Patient Demographic Data a
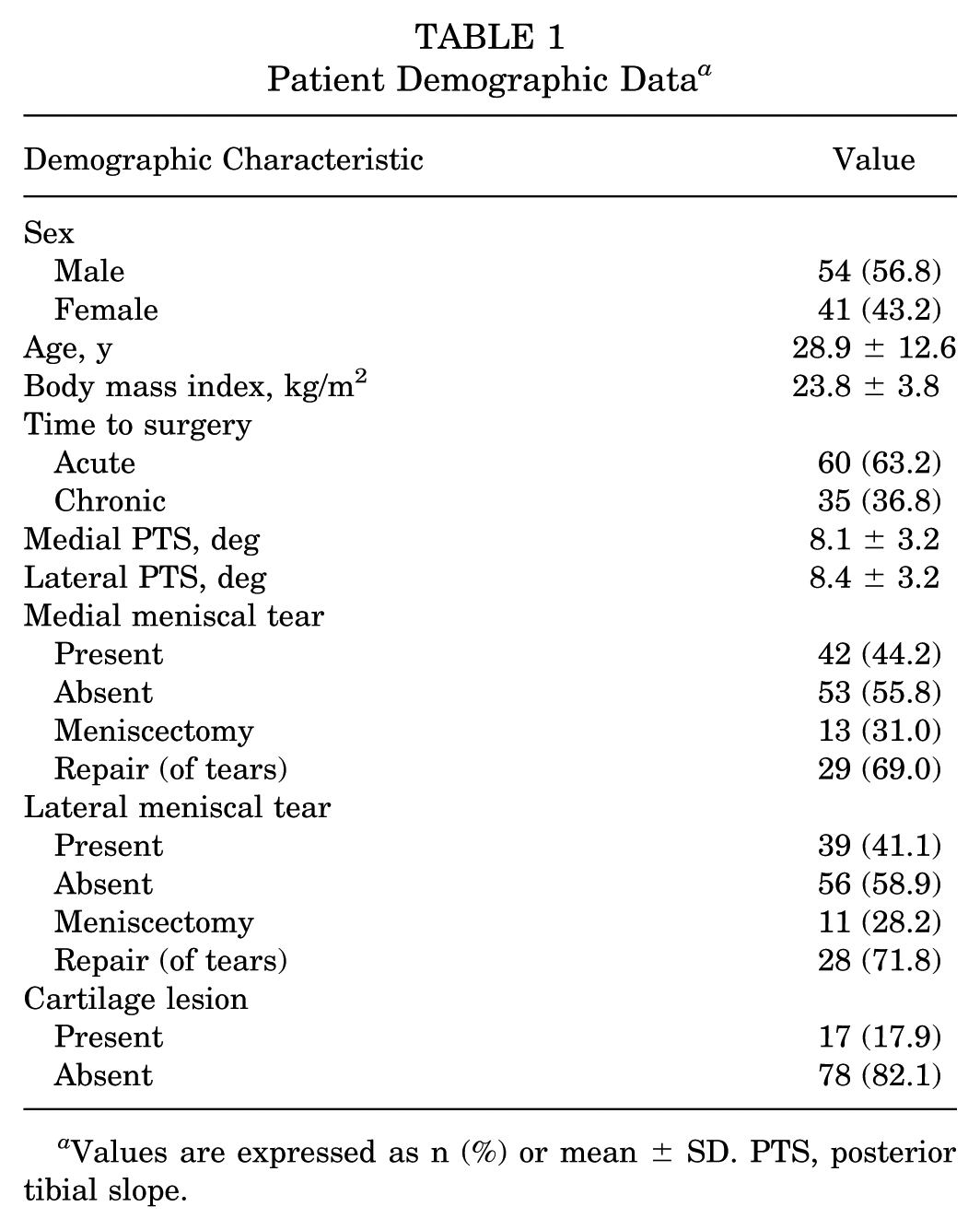
Values are expressed as n (%) or mean ± SD. PTS, posterior tibial slope.
Static ATT measurements were available in 88 patients preoperatively, 84 at 6 months, 91 at 12 months, and 89 at 24 months. Static ATT significantly decreased at 6 months after surgery compared with preoperative values (P < .01). This reduction was maintained at 12 and 24 months, with no significant differences observed among the postoperative time points. In the linear mixed-effects model, the predicted change in static ATT from preoperative to 24 months was −1.32 mm (95% CI, −1.93 to −0.70; P < .01) (Figure 4).
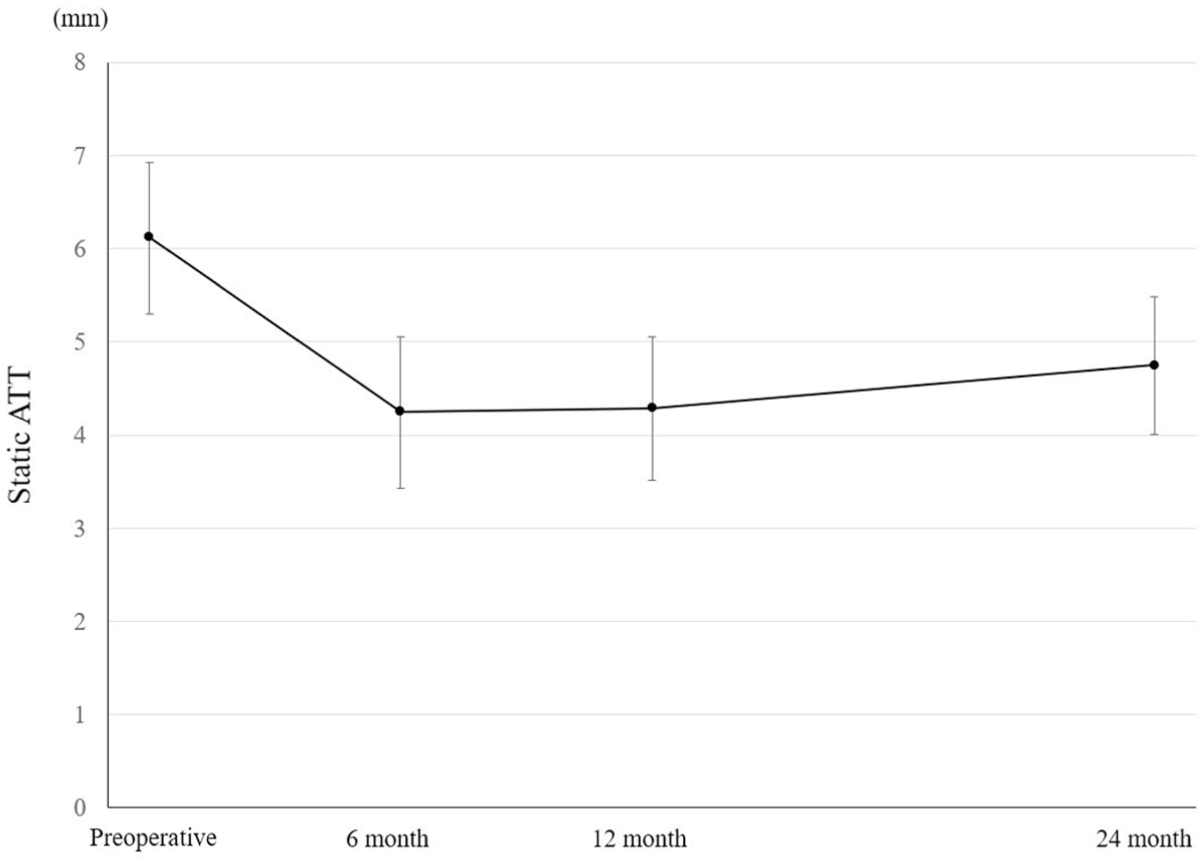
Marginal predicted changes in static anterior tibial translation (ATT). The marginal predicted changes in static ATT over the follow-up period were evaluated using a linear mixed-effects model with random effects.
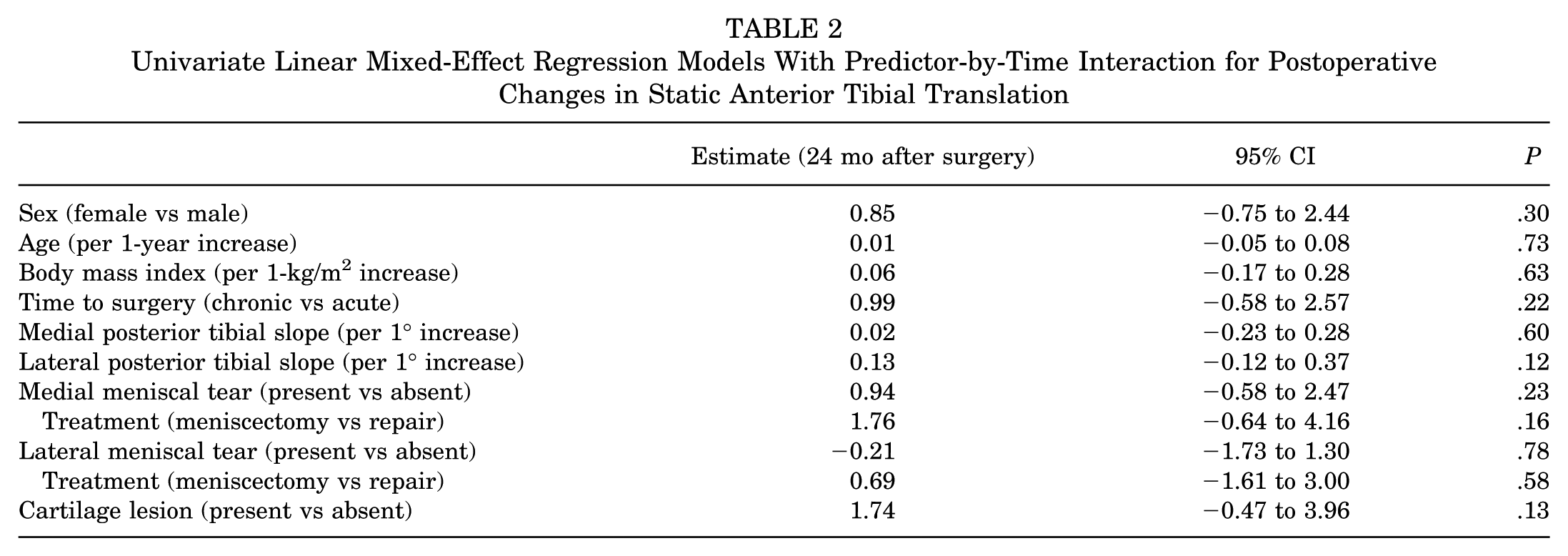
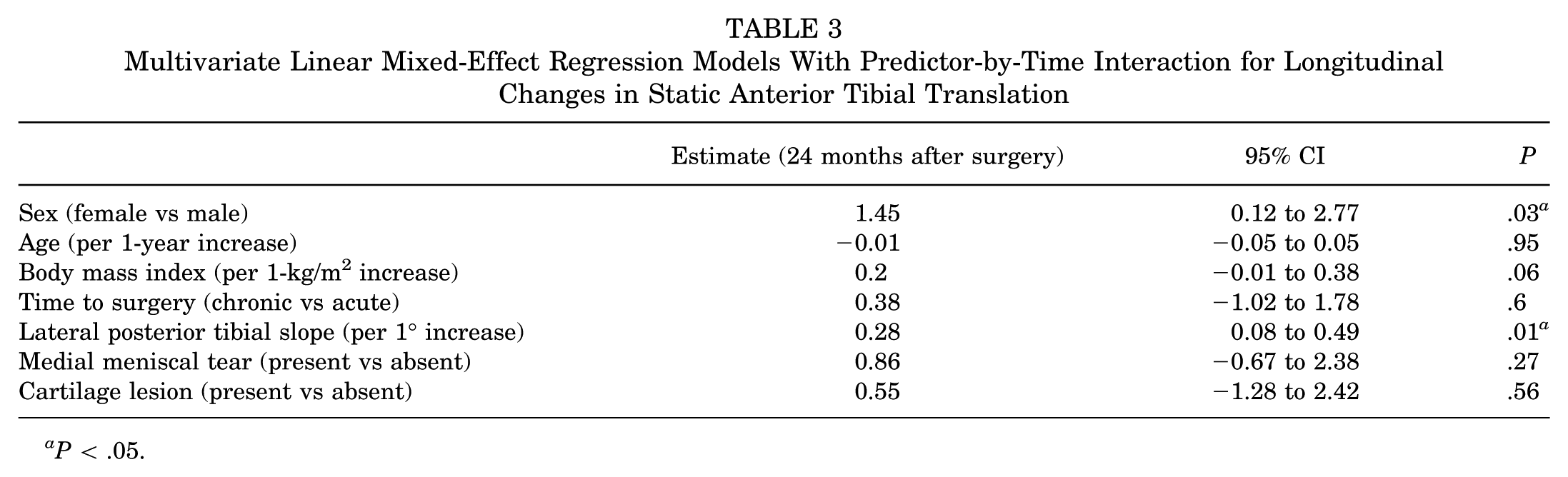
In univariate linear mixed-effects regression analyses, time to surgery, lateral PTS, medial meniscal tear, treatment of medial meniscal tear, and cartilage lesions were associated with longitudinal changes in static ATT at 24 months (P < .25) (Table 2). Because medial meniscal tear and its treatment represent closely related variables, only the presence of medial meniscal tear was included in the multivariable analysis to avoid collinearity. These variables, along with age and BMI, were included in the multivariate model as adjustment covariates regardless of their univariate P values. In the multivariate analysis, female sex emerged as an independent predictor of less postoperative improvement in static ATT (estimate, 1.45 mm; 95% CI, 0.12-2.77; P = .03). Each 1° increase in lateral PTS was associated with a 0.28-mm increase in postoperative static ATT at 24 months (95% CI, 0.08-0.49; P = .01) (Table 3).
Univariate Linear Mixed-Effect Regression Models With Predictor-by-Time Interaction for Postoperative Changes in Static Anterior Tibial Translation
Multivariate Linear Mixed-Effect Regression Models With Predictor-by-Time Interaction for Longitudinal Changes in Static Anterior Tibial Translation
P < .05.
Preoperative pivot shift grades were distributed as follows: grade 0 in 0 cases, grade 1 in 4 cases, grade 2 in 84 cases, and grade 3 in 7 cases. At 24 months postoperatively, pivot shift grades were distributed as follows: grade 0 in 86 cases, grade 1 in 7 cases, and grade 2 in 2 cases; no cases of grade 3 were observed. Accordingly, residual pivot shift (grade ≥1) was present in 9 cases. Greater static ATT at 24 months was significantly associated with residual pivot shift (odds ratio, 1.45; 95% CI, 1.10-1.92; P < .01).
Discussion
The key findings of this study were that static ATT improved after ACL reconstruction and remained stable through 24 months. Furthermore, female sex and a steeper lateral PTS were independently associated with less postoperative improvement in static ATT. Greater postoperative static ATT at 24 months was associated with residual pivot shift.
Whether ATT improves after ACL reconstruction has been debated. Although anatomic ACL reconstruction has been reported to reduce preoperative ATT to levels comparable to those of the healthy contralateral knee, 18 recent studies have suggested that preoperative ATT persists postoperatively.12,34 No previous longitudinal study has elucidated the postoperative changes in ATT beyond the early recovery phase, 35 leaving its long-term course unclear.
In this study, static ATT significantly decreased from preoperative to 6 months after ACL reconstruction and remained stable through 24 months. These results indicate early postoperative improvement in static ATT, with no further progression during follow-up. The difference between weightbearing and nonweightbearing assessments may explain the discrepancy between these findings and previous studies reporting no significant postoperative improvement in ATT.12,34 Beynnon et al 2 demonstrated that switching from nonweightbearing to weightbearing conditions substantially increased ATT in ACL-deficient knees, whereas ACL-intact knees exhibited minimal anterior tibial shift. This suggests that weightbearing magnifies the anterior tibial shear forces that the ACL counteracts. Consequently, ACL-reconstructed knees likely demonstrate smaller increases in ATT under weightbearing conditions than ACL-deficient knees. These biomechanical differences likely account for why studies measuring ATT under nonweightbearing conditions observed persistent ATT after ACL reconstruction, whereas the current study's weightbearing assessment revealed significant and sustained improvement through 24 months.
The current study also found that lateral PTS independently predicted postoperative static ATT over time. Patients with greater lateral PTS exhibited less postoperative improvement and higher residual static ATT at 24 months. PTS is a well-established factor contributing to increased preoperative ATT4,28 and is recognized as a risk factor for graft failure after ACL reconstruction. 20 A steeper PTS increases anterior tibial shear forces, causing the tibia to shift more anteriorly relative to the femur.23,24 This biomechanical effect likely explains why static ATT persists in patients with steep PTS despite anatomic ACL reconstruction. These results suggest that inherent tibial morphology influences postoperative improvement in static ATT. The morphological differences between the medial and lateral tibial plateaus may also be relevant. The lateral tibial plateau is convex, allowing greater anterolateral translation, whereas the medial plateau is concave. Consequently, greater lateral PTS has been linked to high-grade pivot shift 22 and graft failure after ACL reconstruction.3,25 These anatomic features may further explain why lateral PTS was associated with postoperative static ATT changes in the current study. In addition, female sex emerged as an independent factor associated with poorer improvement in static ATT. Zhang et al 34 reported that women exhibited greater medial ATT on magnetic resonance imaging 1 year after ACL reconstruction, although no sex differences were observed for lateral ATT. Intrinsic female risk factors such as muscle weakness or imbalance, 31 joint laxity, 29 and bony anatomy 33 may have contributed to these findings.
Time from injury to surgery was not independently associated with postoperative static ATT in the multivariate analysis; however, it may still have clinical relevance, as delayed surgery has been associated with progressive instability and secondary intra-articular damage.
Other variables, including meniscal status and cartilage lesions, were not independently associated with postoperative static ATT. Although these factors have been reported to influence preoperative ATT in previous studies,17,35 their impact on postoperative ATT may be limited.
Previous studies have demonstrated that excessive preoperative ATT is associated with ACL deficiency and a preoperative positive pivot shift.9,13 Moreover, high preoperative ATT is associated with postoperative graft failure or residual positive pivot shift even after ACL reconstruction.18,20 However, the relationship between postoperative ATT and clinical outcomes has been less studied compared with preoperative ATT. A recent study found no significant correlation between postoperative ATT and Lysholm scores at 6 months. 12 In contrast, the present study demonstrated an association between postoperative static ATT and residual pivot shift. This correlation may be explained by greater ATT representing a “resting pivoted position.” 17 Therefore, minimizing postoperative residual static ATT is important, and factors such as lateral PTS and sex that influence postoperative improvement should be carefully considered.
Although serial radiographic assessment of static ATT is not routinely performed in clinical practice, these findings suggest that postoperative static ATT may serve as a marker of knee stability and help identify patients at risk of residual pivot shift. In this context, identifying factors associated with postoperative ATT may have important clinical implications for risk stratification and surgical decision-making.
Future studies should investigate whether adjunctive procedures, such as lateral extra-articular tenodesis or slope-reducing osteotomy, may influence postoperative static ATT, particularly in patients with a steep PTS, and should further evaluate longer term outcomes and the impact of dynamic loading conditions, such as return to high-level sports, on graft function.
This study has several limitations. First, this study was conducted retrospectively. Second, only weightbearing positions were assessed; nonweightbearing positions were not evaluated. Third, detailed distinctions regarding the size, location, and type of meniscal injuries were not made. Fourth, only static ATT was measured; dynamic ATT under stress tests was not evaluated. Fifth, the present cohort consisted exclusively of patients who underwent ACL reconstruction with BPTB autograft. Thus, the generalizability of these findings to other graft types, such as hamstring tendon or quadriceps tendon grafts, remains uncertain.
Conclusion
Static ATT improved after ACL reconstruction and remained stable through 24 months. Female sex and a steeper lateral PTS were independently associated with less postoperative improvement in static ATT. Greater postoperative static ATT was associated with residual pivot shift.
Footnotes
Final revision submitted March 22, 2026; accepted April 20, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.T. has received funding grants, paid expert testimony, and speaking and lecture fees from Smith and Nephew; funding grants from Zimmer Biomet; paid expert testimony and speaking and lecture fees from Arthrex; and funding grants from Stryker.
Ethical approval for this study was obtained from the institutional review board of the University of Tokyo (IRB No. 2674). Informed consent was obtained from all individual participants included in the study.