
Abstract
Background:
Drug overdose and poisoning deaths in the pediatric and adolescent population have recently surpassed cancer as the third-leading cause of death, resulting in the opioid epidemic being declared a public health emergency. Federal mandates, such as the Controlled Substance Utilization Review and Evaluation System (CURES) database that followed, were created to improve monitoring of opioid prescriptions. The impact of CURES on pain management for children and adolescents undergoing common arthroscopic procedures has not been assessed.
Hypothesis:
Post-CURES reduction in opioid prescriptions will not result in additional postsurgical triage contacts or additional prescription needs in a pediatric and adolescent cohort undergoing arthroscopic procedures.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Pediatric and adolescent patients (ages 10-19 years) undergoing common arthroscopic knee and shoulder procedures by a single surgeon at a single, tertiary care pediatric hospital from 2013 through 2023 were reviewed. Demographics, surgical details, and postoperative outcomes were compared across pre- (before 2018) and post-CURES (2018 and later) cohorts defined as before and after implementation of a change in opioid prescription habits that occurred in response to the mandatory reporting in CURES. Primary outcomes included phone calls or messages to the triage nurse related to pain. Secondary outcomes included additional opioid prescriptions required to manage pain.
Results:
The post-CURES cohort (N = 224) was prescribed significantly fewer morphine milligram equivalents (total MMEs prescribed) compared with the pre-CURES cohort (N = 244) (89.4 ± 8.3 vs 444.3 ± 66.0; P < .001). Patients in the post-CURES cohort were more likely to call regarding pain (13% vs 7%; P = .03). However, there were no differences in additional pain prescriptions required (4% pre- vs 4% post-CURES; P≥ .99) to manage pain.
Conclusion:
Despite a nearly 5-fold decrease in total MMEs prescribed, there was no increase in additional pain prescriptions required even though there was a 2-fold increase in messages related to pain to the triage nurse via education and reassurance. The hypothesis was upheld in part, suggesting that effective pain management can be achieved with fewer opioids, but that the postoperative care of adolescents undergoing arthroscopy could be further improved.
Keywords
In the past decade, the alarming rise in opioid use has spurred national interest. The opioid epidemic was designated a public health emergency in 2017, with an estimated $1.5 trillion burden in the United States. 5 The epidemic is multifactorial in etiology, with approximately 32% of overdose deaths related to prescription drug abuse. 21 Overprescription of opioids is a key factor contributing to this abuse, with nearly 1 in 4 injection drug users having initiated recreational drug use with a prescription opioid. 17
Opioid prescribing patterns among children generally receive less attention compared with adult populations. 3 However, between 2006 and 2012, there were >22,000 emergency department visits for opioid-related poisoning in children. 30 Additionally, 3.6% of adolescents between 12 and 17 years old reported having misused or abused opioids in 2016.1,33 In 2016, drug overdose or poisoning was reported as the sixth-leading cause of death among children and adolescents, responsible for 4.8% of deaths among this age group. 7 However, in 2020, an updated report was released demonstrating an 83.6% increase in drug overdose and poisoning deaths, making it the third-leading cause of death in this population, now second only to firearm-related injury and motor vehicle collisions. 12
Orthopaedic surgeons are in a unique position to help address this epidemic, as orthopaedic surgery often represents some of the most painful surgeries 9 and orthopaedic surgeons are among the most frequent prescribers of opioid medications.4,20,26 Multiple studies have also documented the excessive amount of opioids prescribed in the postoperative period for common orthopaedic procedures, often citing that patients may only use a fraction of what is being prescribed, leaving excess medication in the community, creating an opportunity for misuse and abuse. Currently, there are no standardized opioid prescribing guidelines in pediatric orthopaedics, leading to considerable variation in prescriptions across different orthopaedic procedures.11,15,16,23,26
To help address the growing opioid crisis, California's Department of Justice mandated physicians to consult the Controlled Substance Utilization Review and Evaluation System (CURES) database beginning in 2018.6,19,24 The CURES database helps monitor prescription drugs and tracks all schedule 2 to 4 substances dispensed.19,24 A primary goal of CURES was to prevent overprescription of opioids by improving the reporting and tracking of prescriptions >90 morphine milligram equivalents (MME)/day. 6 So, prescribing practices could be adapted to reduce the impact of CURES by prescribing less than the mandatory MME reporting value. The effect on pain management related to these lower prescription amounts is not known for pediatric and adolescent patients undergoing common arthroscopic procedures. Therefore, the aim of this study is to investigate if this change in postoperative pain regimen led to an unintended change in the postoperative experience for pediatric and adolescent patients undergoing common arthroscopic knee and shoulder procedures, particularly the need to seek triage care for uncontrolled pain. A secondary aim was to determine the need for any additional narcotic prescriptions in response to those pain management concerns. The hypothesis was that the post-CURES reduction in opioid prescriptions would not result in additional postoperative triage contacts or additional prescription needs in a pediatric and adolescent cohort undergoing common shoulder and knee arthroscopic procedures.
Methods
Approval was obtained from the institutional review board with a waiver for informed consent.
Participants
Pediatric and adolescent patients (aged 10-19 years) undergoing common arthroscopic knee and shoulder procedures by a single surgeon (E.W.E.) at a single, tertiary care pediatric hospital from 2013 through 2023 were reviewed. Arthroscopic procedures included shoulder stabilization and associated procedures (Current Procedural Terminology [CPT] codes 29806 and 29807) and knee anterior cruciate ligament reconstruction (ACLR) with or without meniscal work (CPT code 29888). Patients were excluded for the reasons outlined in Figure 1.
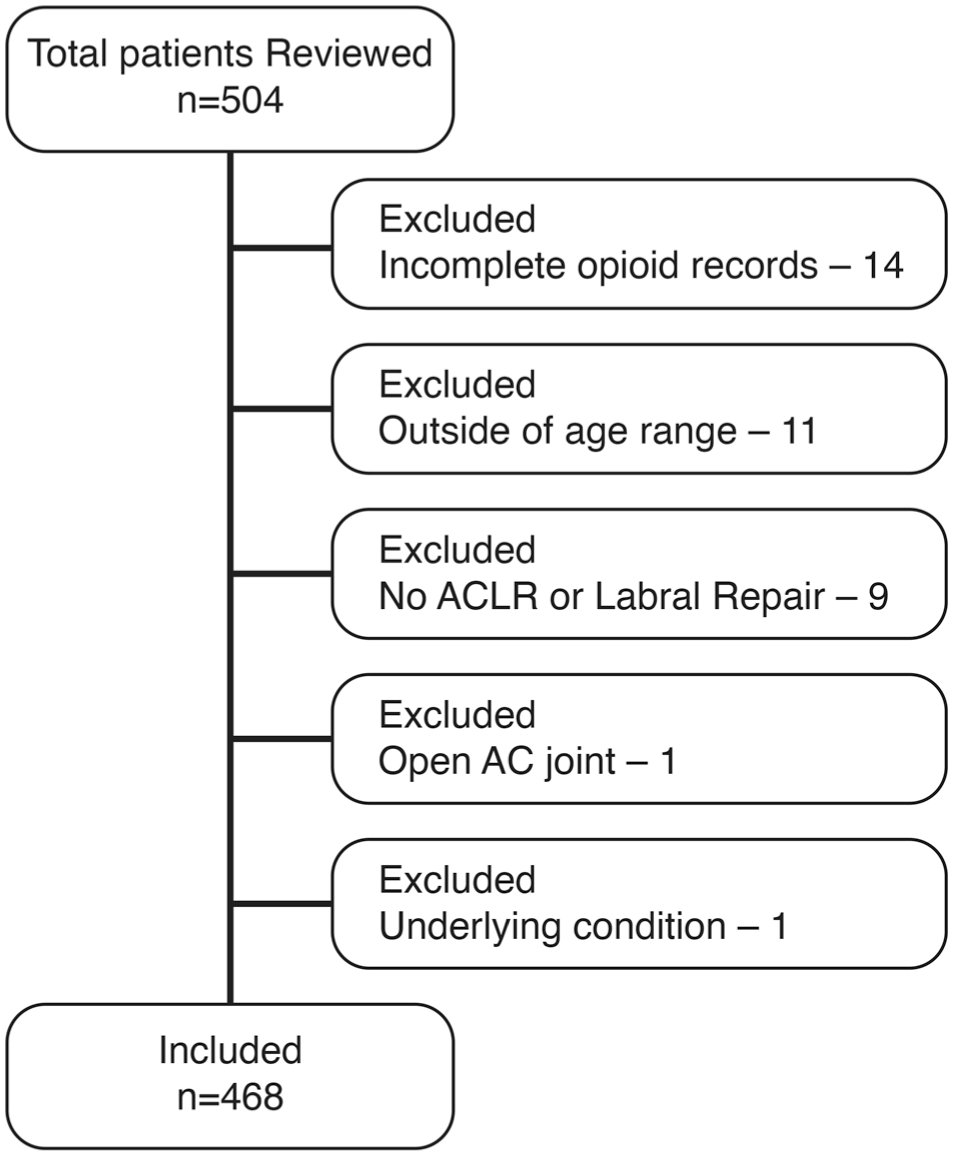
Distribution of exclusion criteria for the study cohort. AC, acromioclavicular; ACLR, anterior cruciate ligament reconstruction.
To investigate the impact of the CURES mandate and corresponding change in opioid prescribing patterns at this institution beginning in 2018, cohorts were defined as (1) pre-CURES patients undergoing arthroscopic knee and shoulder surgery before 2018 and (2) post-CURES patients undergoing surgery after 2018. The study surgeon changed the postoperative narcotic prescription protocol in response to the CURES mandate in 2018 in order to avoid mandated reporting based on prescribed MME amounts. We chose the years 2013-2014 to protect against surgeons that may have preemptively changed prescribing practice because they knew the CURES mandate was on the horizon, and 2022-2023 because by then the post-CURES prescribing practices would have been fully implemented and routine (Figure 2). No other purposeful changes were made to postoperative pain management protocols during this time. Data were collected via review of their electronic medical records.
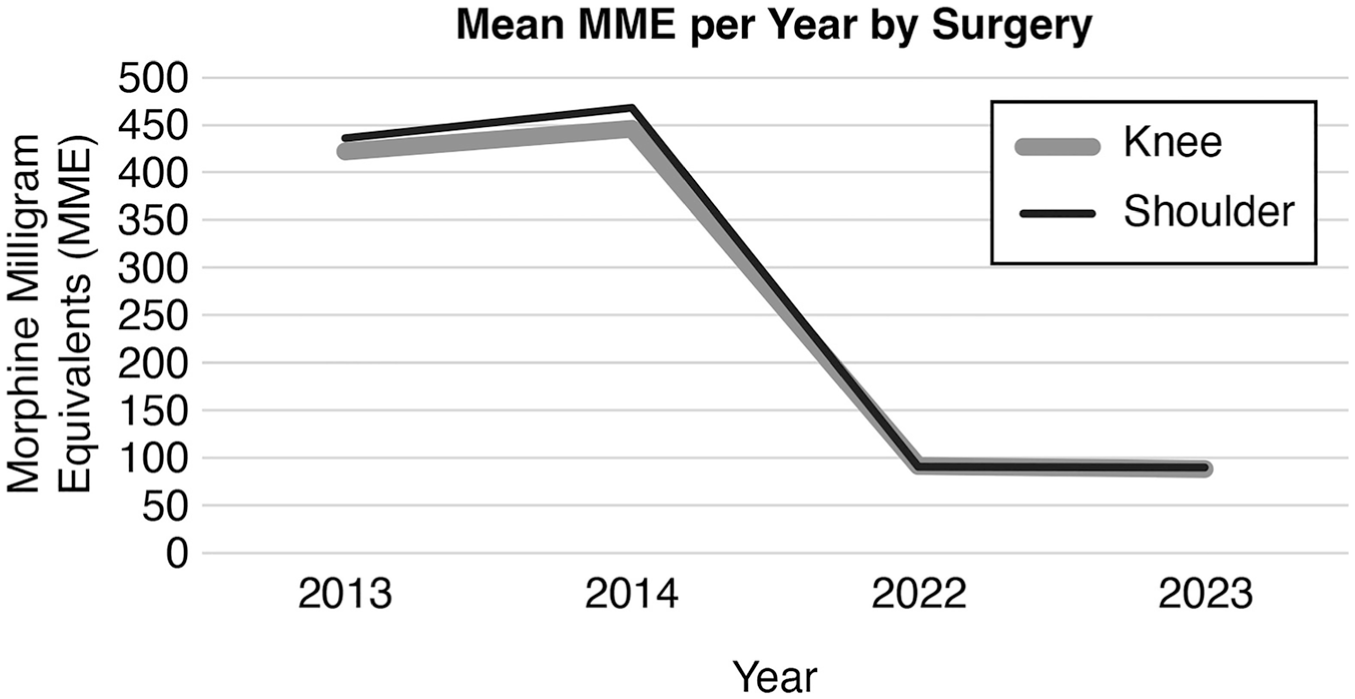
Change in postoperative pain prescriptions pre- and post-CURES instituted in 2018. CURES, Controlled Substance Utilization Review and Evaluation System; MME, morphine milligram equivalent.
Demographic data collected included sex, height, weight, body mass index (BMI), age, race, and ethnicity. Race and ethnicity were self-reported. Race included, in alphabetical order: American Indian or Alaska native, Asian Indian, Black or African American, Chinese, decline to answer, Filipino, Guamanian or Chamorro, Hispanic/Latino, Japanese, Korean, Middle Eastern/North African, native Hawaiian, Other, other Asian, other Pacific Islander, Samoan, Unknown, Vietnamese, or White/Caucasian. Although Hispanic is not normally recorded as a race, our electronic health system allows families to select it as a race, independent as a selection for ethnicity. For statistical purposes, race was considered in 4 categories: White, Black, Hispanic, and Other (which included any of the other categories). Ethnicity included 4 options: Hispanic or Latino, non-Hispanic, refusal to say, and Unknown. Data on procedure laterality, procedure performed, additional procedures performed, anesthetic plan, perioperative regional anesthesia, tourniquet time, and prescription of opioids (total MMEs prescribed) (Table 1) were also collected. To evaluate differences in outcome and pain across the pre- and post-CURES cohorts, primary outcome measures included patient phone calls to the triage nurse or electronic medical record messages to the care team regarding pain. During the study period, access to the triage line and the electronic medical record system did not change from pre-2018 to post-2018. Secondary outcomes included additional pain medications needed in the acute postoperative period (<30 days).
Morphine Milligram Equivalent (MME) Conversions

Statistical Analysis
Basic descriptive statistics are presented. Continuous data were evaluated with the Shapiro-Wilk test of normality and found to be nonparametric and therefore evaluated with the Kruskal-Wallis H or the Mann-Whitney U. Categorical data were evaluated with Pearson chi-square or Fisher exact test. No a priori power analysis was performed. Statistical analysis was performed using IBM SPSS (Version 29; IBM). Statistical significance was defined as P < .05.
Results
A total of 468 patients were included after applying criteria: 244 pre-CURES and 224 post-CURES. Demographic data of the 2 cohorts were equivalent (P > .05) with regard to sex (40% female pre- vs 36% female post-CURES; P = .42), age (16.4 ± 1.5 years pre- vs 16.2 ± 1.6 years post-CURES; P = .22), and BMI (25.2 ± 5.1 pre- vs 25.1 ± 5.6 post-CURES; P = .41) (Table 2). There were different distributions of self-reported race between the cohorts (2.5% vs 6.3% Black, 0.8% vs 29.1% Hispanic, and 41.3% vs 12.6% Other pre- vs post-CURES). Ethnicity, however, was similar between groups (42% Hispanic pre- vs 43% Hispanic post-CURES; P = .84). There was no difference in pain-related phone calls among self-reported race (P = .06), self-reported ethnicity (P = .50), or sex assigned at birth (P = .08).
Cohort Demographics a
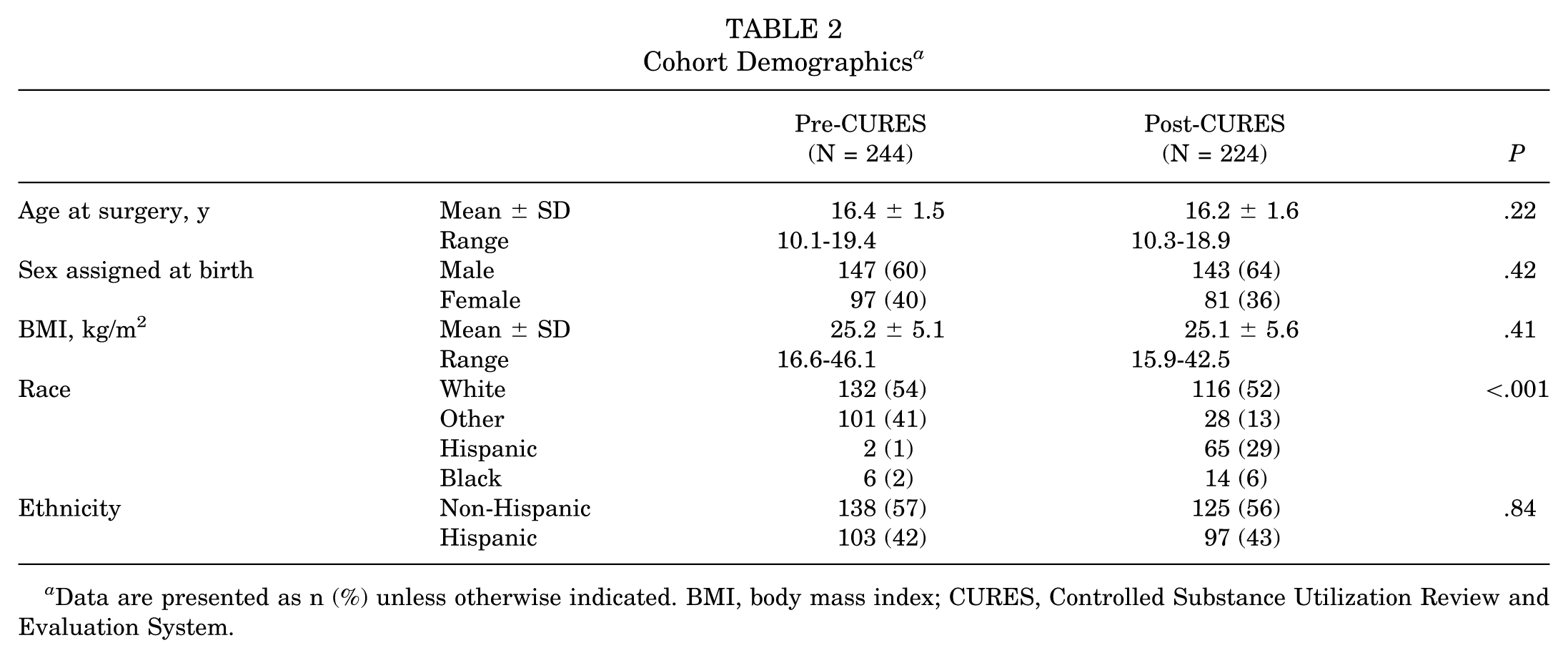
Data are presented as n (%) unless otherwise indicated. BMI, body mass index; CURES, Controlled Substance Utilization Review and Evaluation System.
There were differences in the number of ACLRs (52% pre- vs 77% post-CURES) and shoulder (48% pre- vs 23% post-CURES) arthroscopic stabilization procedures across cohorts (P < .001). The regional anesthetic plan differed among cohorts and those undergoing an ACLR, as there was a change in practice that coincided with the change in opioid prescribing patterns: in the pre-CURES cohort, nearly all (99%) knee arthroscopic procedures received femoral nerve blocks whereas in the post-CURES cohort, no femoral blocks were administered because of changes in anesthesia policy to reduce the risk to motor nerves. Instead, lower extremity peripheral nerve blocks (PNBs) primarily consisted of adductor canal with (43.4%) or without (54.3%) infiltration between the popliteal artery and capsule of the knee (IPACK) for the post-CURES cohort (Table 3). Participants receiving adductor PNBs alone required similar MMEs overall compared with those receiving combined adductor and IPACK PNBs (90.6 ± 11.7 vs 88.3 ± 7.2 MMEs; P = .44). For shoulder arthroscopic procedures, there was no difference in regional anesthetic used in the pre-CURES versus post-CURES cohorts (P = .30) (Table 3).
Distribution of Regional Nerve Block Pre- and Post-CURES a
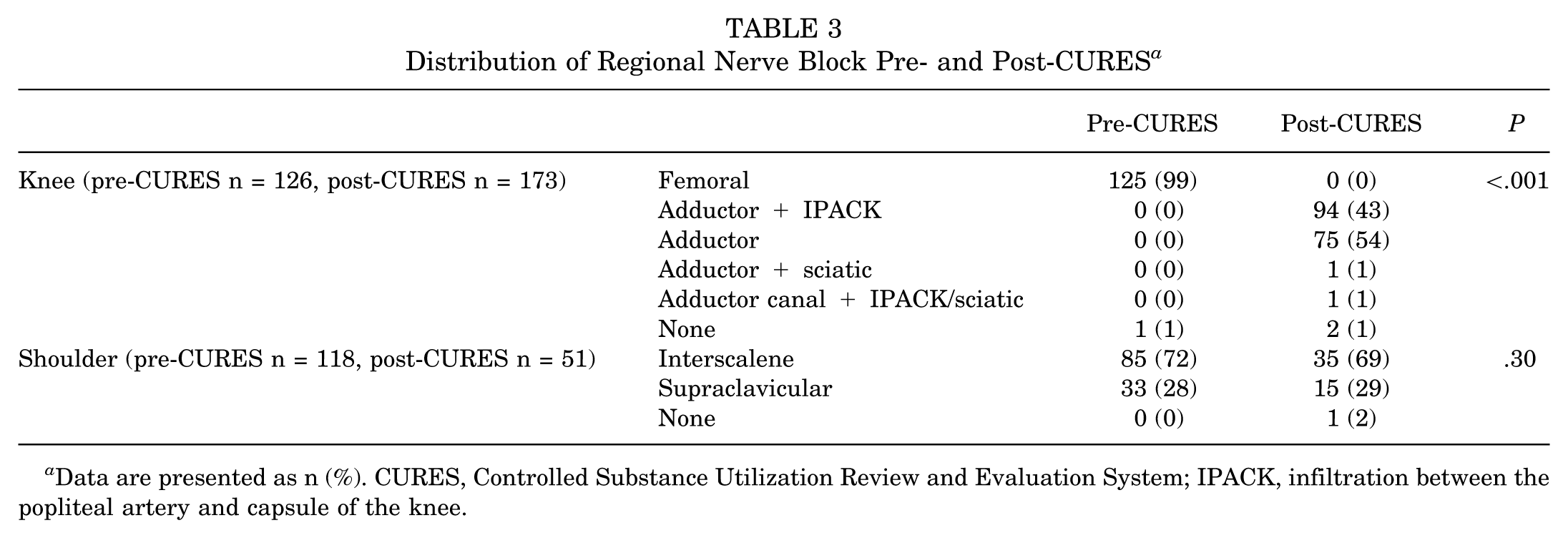
Data are presented as n (%). CURES, Controlled Substance Utilization Review and Evaluation System; IPACK, infiltration between the popliteal artery and capsule of the knee.
As a result of prescription pattern changes, the post-CURES cohort was given a mean of 89.4 ± 8.3 MME compared with the pre-CURES cohort at a mean 444.3 ± 66.0 (P < .001). Phone calls or messages related to pain (including from visits to the emergency department) differed between cohorts, with the post-CURES cohort contacting the office more often regarding pain compared with the pre-CURES cohort (13% vs 7%; P = .03). There were no readmissions in either cohort. With the pre-CURES and post-CURES cohorts combined, the patients who called regarding pain had been prescribed fewer MMEs than those who did not call (207.2 ± 166.4 vs 281.7 ± 184.3; P = .003). There were no differences in subsequent opioid prescriptions required between cohorts (4% pre- vs 4% post-CURES; P≥ .99). The most common intervention provided in response to a phone call related to pain was education regarding current medication management and reassurance. A distribution of our outcomes related to pain management can be found in Table 4.
Distribution of Outcomes of Interest Pre- and Post-CURES a
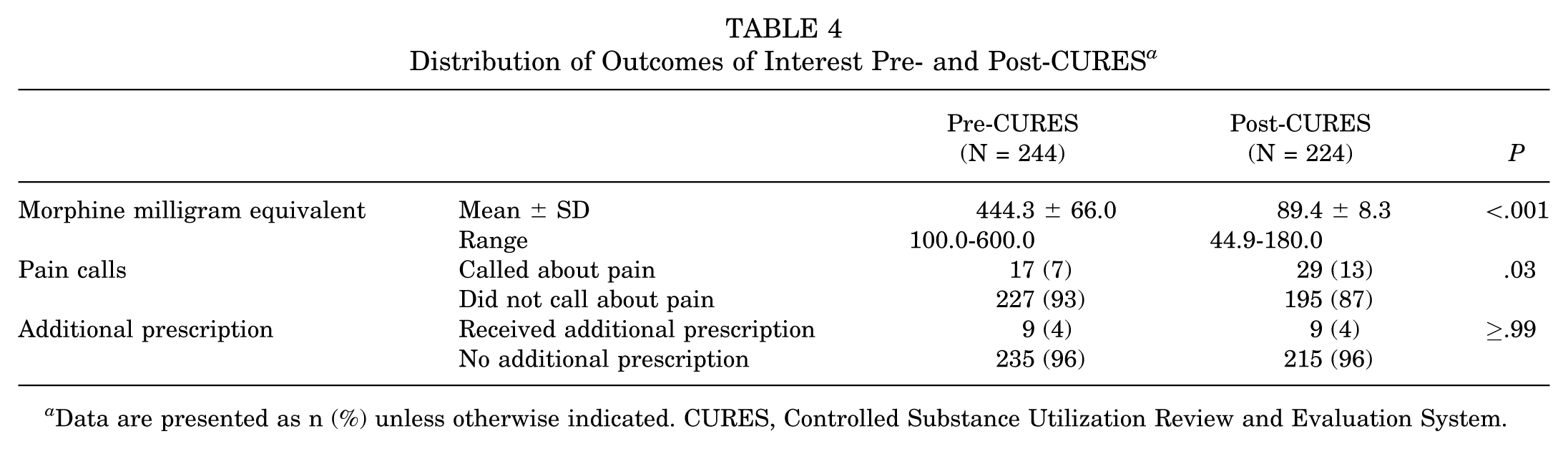
Data are presented as n (%) unless otherwise indicated. CURES, Controlled Substance Utilization Review and Evaluation System.
Discussion
This study describes the impact of reducing the initial postsurgical opioid prescriptions in response to the guidelines set forth by the CURES database, and it suggests that our hypothesis is partially refuted. There was a significant increase in the number of phone calls and messages related to postoperative pain for patients in the post-CURES cohort; yet, there was no change in the need to prescribe additional opioids after the family contacted the triage line or care team. The outcomes of decreasing opioid prescriptions for pediatric and adolescent patients undergoing ACLR or shoulder stabilizing surgery indicate that surgeons cannot merely reduce the number of pills prescribed. In fact, pain is known to be multifactorial in etiology and perception, and therefore, management needs to be multimodal as well. 13
Prior studies that included adolescent patients have utilized medication diaries to document that 5 to 7 hydrocodone/acetaminophen (5 mg/325 mg) pills (approximately 50-75 MME) may be sufficient for pain management after knee arthroscopy.28,32 Steinmetz et al 28 included participants between ages 10 and 18 years undergoing revision knee arthroscopy, ligamentous reconstruction, or bony osteotomy. Wojahn et al 32 included patients ranging from age 14 to 72 years undergoing knee arthroscopy for meniscal repair, partial meniscectomy, debridement, chondroplasty, or loose body removal. Both diary studies documented underutilization of total pills prescribed, resulting in a surplus of opioids. However, with significant variety in perioperative analgesia plans and age of participants, this number may not apply to all patients for all providers. Additionally, because of the variety of arthroscopic procedures performed, these findings may not be generalizable to all knee arthroscopy procedures. There is also evidence in adult patients undergoing shoulder and knee arthroscopy that a multimodal opioid-sparing postoperative protocol does equally well to opioid protocols in managing pain. 22 Wohjahn et al's randomized controlled trial demonstrated that these older patients undergoing a similar surgery could be managed well without opioids. In the present study, opioid prescription amounts decreased by nearly 80% (from 443 to 89 MME) after the implementation of the opioid-limiting postoperative pain regimen. This reduction in opioid prescriptions did not lead to an increased need for subsequent narcotic prescriptions in the first 30 days following surgery. This lack of increase in additional prescriptions supports the approach of the new perioperative pain protocol to the ideal perioperative pain regimen. Together, the present findings and these previous studies suggest that opioids risk being overprescribed. In fact, although participants initially prescribed fewer opioids in the post-CURES cohort were twice as likely to call regarding pain after surgery, this did not translate to additional narcotics required. Thus, their postoperative pain regimen did not change. Rather, additional education on pain management including the use of nonnarcotics was the only intervention required from our department. Furthermore, the increase in the number of phone calls related to pain in the post-CURES cohort, while statistically significant and important to the patients and their families, may not have been a substantial change in the burden for the clinical staff, as the total number of phone calls received was not numerically significant.
Exploring the utility of nonopioid pain management, such as regional nerve blocks, is an essential strategy to tackle opioid overprescription. There is considerable variability in pain management techniques for pediatric orthopaedic procedures.23,31 The most common perioperative analgesia plan for pediatric and adolescent ACLR included adductor nerve block perioperatively (81%) and ibuprofen postoperatively (60.9%). 31 A study investigating differences in efficacy between femoral PNB alone and combined femoral and sciatic PNB found combined PNB improved analgesia postoperatively according to the highest Numeric Pain Rating Scale score in the postanesthesia care unit. 14 Similarly, the current findings indicate that the joint use of adductor and IPACK was associated with slightly fewer MMEs required compared with adductor PNB alone (88.3 vs 90.6), though this difference was not statistically significant. Perhaps guidelines are needed for common orthopaedic sports procedures for ideal postoperative, multimodal pain regimens to decrease variability and improve patient experiences.
Other methods to reduce opioid overprescription include comprehensive, system-wide initiatives and perioperative education.8,18,25 Andereck and colleagues 2 found that openly comparing the opioid prescribing patterns of providers to their peers reduced opioid prescribing more than the release of standardized Centers for Disease Control and Prevention opioid prescribing guidelines. Perioperative education of patients has also been shown to help reduce postoperative pain and opioid use. 8 This is congruent with the present finding that postoperative concerns were addressed with education or reassurance alone, without the need for additional narcotics. Although not statistically significant, participants in this study identifying as Hispanic were more likely to call regarding pain postoperatively compared with other self-reported racial groups. Previous literature has suggested that language and culture discordance are major barriers in health care among Latino patients. 10 Consideration of targeted preoperative education could help reduce the observed disparities.
Policy interventions, such as the CURES mandate, further research and development of nonopioid analgesics, and multimodal perioperative pain regimens, constitute important methods of reducing opioid prescription in the health care setting. One study found patients aged <24 years represented the age group prescribed the most amount of opioids in 2015, followed by a net decrease by 2018. 24 This decline coincided with the 2016 requirement that all licensed prescribers register for access to CURES, though mandatory CURES consultations did not start until 2018. Indeed, this institution saw a sharp decline in opioid prescribing practices following the 2018 enforcement of the CURES mandate. Although there are many confounding variables, these results taken alongside our present findings suggest the CURES mandate may have contributed to a decrease in opioid prescriptions, either directly or indirectly. The present study underscores the potential impact of policy interventions such as CURES to shape prescribing patterns and could help guide the development of future programs aimed at addressing the opioid epidemic.
Limitations
The current study has several limitations related to the retrospective study design. It was a single-surgeon series at a single, pediatric tertiary care center, without pain levels provided at various time points, which may limit generalizability of the findings; however, it is strengthened by consistency of preoperative counseling, surgical factors, and postoperative instructions that are often standardized for any given provider, thus limiting potential confounders related to technique or postoperative care. Although orthopaedic surgery is frequently cited as one of the most painful surgical disciplines for postoperative pain, the studied procedures are not frequently on the upper threshold of pain within the specialty. This study did not evaluate the possibility that patients may have been able to obtain narcotics from other sources, although any amount from a legitimate source would have resulted in a mandatory reporting to the CURES system. One notable confounder that cannot be overlooked is the simultaneous change in regional anesthetic techniques for ACLRs. At the exact time a change in opioid-prescribing habits was implemented, the femoral nerve blocks were replaced with either adductor canal block or adductor canal block with IPACK supplementation. Additionally, the post-CURES cohort had higher numbers of ACLR, which may further amplify the potential confounding effect that changing the regional anesthetic may have. However, there was no change in the regional anesthesia for shoulder instability, and when evaluating phone calls by surgical location (knee or shoulder), there was no significant difference in phone calls recieved about pain between shoulder and knee patients. Thus, it can be deduced that the regional anesthetic alone was not the sole culprit leading to this increase in patient contact in the first 30 days postoperatively. Moreover, previous studies in this age cohort and surgery type comparing these femoral nerve and adductor canal regional blocks with and without IPACK have not demonstrated any differences in postoperative analgesic needs.27,29 Further investigation is warranted to determine which factors contribute to the increased contact to allow for interventions to improve the postoperative experience for patients and families. However, decreasing the amount of opioid prescribed postoperatively for pediatric and adolescent ACLR and shoulder instability appears feasible and should be considered.
Conclusion
The CURES database, implemented in 2018, aimed to better understand prescribing patterns by carefully monitoring and tracking the dispensing of controlled substances. This study demonstrates the experience with changing opioid prescribing patterns in response to the CURES mandate, wherein there was a nearly 5-fold decrease in MMEs prescribed without any significant change in the need for rescue opioid medications prescribed in the first 30 days postoperatively. However, this reduction in index opioid prescription did result in increased triage phone calls and electronic messages related to pain management, most of which were addressed through reassurance and education on utilizing multimodal opioid-sparing techniques and medications. Although the hypothesis is upheld, the results indicate that future direction may include augmenting perioperative patient education to improve patient expectations and pain control in this younger cohort.
Footnotes
Final revision submitted April 16, 2026; accepted April 19, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.W.E. has received support for education from Elevate Surgical; compensation for services other than consulting from Arthrex; and research support from RTI Surgical; he is a board or committee member for the Pediatric Orthopaedic Society of North America.
Ethical approval was obtained from the University of California San Diego institutional review board (No. 192008) with a waiver for informed consent.