
Abstract
Background:
Revision meniscal repair may yield better postoperative outcomes than meniscectomy. Few studies concerning the postoperative results of revision meniscal repair are available.
Purpose:
To evaluate the clinical outcomes following revision meniscal repair for meniscal retears after isolated meniscal repair.
Study Design:
Case series; Level of evidence, 4.
Methods:
The cases of 11 knees with ≥1 year of postoperative follow-up were retrospectively analyzed after they had undergone revision as a result of retear at the initial suture site between 2018 and 2024. We compared the patients' presurgical and final follow-up values on the Tegner sports activity score (Tegner score), Lysholm score, and International Knee Documentation Committee (IKDC) Subjective Knee Form by Wilcoxon signed-rank test. At 1 year postoperatively, the revision site was structurally evaluated by magnetic resonance imaging (MRI). To account for multiple comparisons across outcome measures, a Bonferroni correction was applied, with statistical significance set at a P value of < .02.
Results:
Of the 11 knees, 7 were male and 4 were female (median age at revision: 23 years; IQR, 17-32 years). The median Lysholm and IKDC scores both improved significantly from 57.0 (IQR, 40.0-81.0) and 50.8 (IQR, 37.9-72.4) before revision surgery to 91.0 (IQR, 90.0-100.0) and 88.5 (74.7-94.3) at the final follow-up (P = .002, r = 0.89; P = .002, r = 0.89), respectively. Postoperative MRI findings revealed low-signal intensity changes at the revision site in 8 of 11 patients, whereas 3 patients demonstrated persistent high-signal intensity.
Conclusion:
Our study showed that revision meniscal repair may improve short-term clinical results in carefully selected patients with retears. Further research is required to define optimal indications and techniques.
The meniscus plays a crucial role in the body's load transmission, shock absorption, proprioception, cartilage lubrication, and joint stability.25,34 Meniscal injuries are one of the most common injuries in the knee joint, with an occurrence rate reported at 23.8 per 100,000 individuals per year. 3 Traditionally, a meniscectomy was considered the gold standard treatment for meniscal injuries, 2 but meniscal repair is now recommended whenever possible to achieve better clinical outcomes.9,23 Arthroscopic meniscal repair has demonstrated favorable outcomes to date16,19,27,30,32 and is strongly recommended, particularly for younger patients. 22 However, according to systematic reviews, the reported failure rate after meniscal repair surgery is approximately 11% to 23%.6,8,21 In addition, even in cases in which the repaired meniscus is clearly healed at second-look arthroscopy, the possibility of retear at the same site has been pointed out. 15
Until recently, partial meniscectomy has tended to be preferred for failed meniscal repair procedures.17,24,26 However, revision meniscal repair may offer better postoperative outcomes than a meniscectomy, but few studies have investigated this.7,12,14,33 There is little documentation of the postoperative outcomes in particular, including imaging assessments of revision meniscal repairs for retears after an initial meniscal repair of isolated meniscal tears without concomitant procedures such as ligament reconstruction. 12 The purpose of our study was to evaluate the clinical outcomes following revision meniscal repair for meniscal retears after isolated meniscal repair. Our hypothesis was that revision meniscal repair results in favorable postoperative clinical scores and demonstrates structural continuity at the revision site as assessed by magnetic resonance imaging (MRI).
Methods
Ethical Considerations
Informed consent for the use of the data collected in this study was obtained from all patients preoperatively. The study complied with the Declaration of Helsinki.
Patients
During the period 2018 to 2024, a total of 1250 individuals who underwent isolated arthroscopic meniscal repairs at the participating research institution were included after our initial search. Cases involving around-knee osteotomy (AKO) or ligament reconstruction were excluded from the study. The indications for meniscal repair surgery were as follows: ≥1 meniscal tear accompanied by locking or catching symptoms, meniscal tear(s) in the red-red (R-R) zone or red-white (R-W) zone, meniscal tear(s) resistant to conservative therapy for ≥3 months, and no obvious degeneration at the site of the meniscal tear.
A complex tear is defined as the presence of ≥2 tears, either horizontal, radial, or longitudinal, within 5 mm of the peripheral area. Regarding the tear location, we defined the area within 3 mm of the meniscal periphery as the peripheral R-R zone, and we defined the peripheral area between 3 and 5 mm as the central R-W zone.
Meniscal suturing was performed arthroscopically after rasping, using vertical sutures or stacked sutures for meniscal repair. Depending on the case, the all-inside technique (Fast-Fix, Smith & Nephew Endoscopy; or Air, Stryker), the inside-out technique (zone specific or Henning), 10 the outside-in technique, or combinations thereof were used. The number of sutures was determined based on the tear size, with additional sutures placed during probing until the torn meniscus stabilized. In addition, a fibrin clot was used for tears with poor healing prospects, such as radial tears or horizontal tears, and for cases with large tear sizes.
We examined the condition of the articular cartilage using arthroscopy, and in all cases, it was either normal (International Cartilage Regeneration & Joint Preservation Society [ICRS] grade 0) or nearly normal (ICRS grade 1). We also assessed the percentage mechanical axis (%MA) and posterior tibial slope (PTS) using standing knee and full-length lower limb radiographs prior to revision.
All surgeries were performed arthroscopically under general anesthesia, and no nerve blocks were used. All previous repair sutures were removed during the revision surgery. Postoperative rehabilitation protocols were standardized across all cases. For the first 4 weeks postoperatively, patients were instructed to avoid weightbearing and range of motion exercises. Full weightbearing and unrestricted range of motion exercises were initiated at 4 weeks postoperatively.
Follow-up Evaluation
The clinical evaluation was carried out based on the Tegner sports activity score (Tegner), 29 the Lysholm score, 18 and the International Knee Documentation Committee (IKDC) Subjective Knee Form. 13 The prerevision results were compared with the final survey results. Postoperative follow-up assessments were conducted by 1 of 3 surgeons (T.S., S.Y., and K.H.). MRI was performed and evaluated for all cases to conduct structural evaluations at 1 year postrevision. Signal changes at the revision site were assessed on T2-weighted images according to the criteria established by Stoller et al. 28 Grade 0 represents a normal meniscus. Grade 1 (central globular intrameniscal alternation) and grade 2 (linear horizontal, triangular, or bandlike signal alternation confined within the meniscus) were defined as meniscal signal changes not reaching the articular surface. Grade 3 was defined as linear changes continuous with the meniscal surface, and grade 4 was defined as multiple complex changes. 12 Low to intermediate signal intensity at the revision site was defined as an MRI finding indicating structural continuity. High signal alternation comparable with that of the intra-articular fluid was classified as MRI findings suggestive of incomplete tissue remodeling. 11 In this study, 2 blinded sports arthroscopic knee surgeons (S.Y., and K.H.) (certified by the Japanese Knee Society) at the research institution evaluated the MRI scans. Intraobserver reliability and interobserver reliability was assessed using Cohen kappa coefficient. To ensure intraobserver reliability and account for potential recall bias, MRI evaluations were repeated after a minimum interval of 2 weeks. The kappa coefficient was interpreted as follows: <0.20, poor; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, good; and 0.81 to 1.00, excellent.
Statistical Analysis
The Tegner score, Lysholm score, and IKDC score at prerevision and at the final survey were compared using the Wilcoxon signed-rank test. To account for multiple comparisons across outcome measures (Tegner, IKDC, and Lysholm scores), a Bonferroni correction was applied, with statistical significance set at P < .02. The data were analyzed with JMP PRO 16 (SAS Institute).
Results
Among 1250 cases, 601 involved medial meniscal tears and 649 involved lateral meniscal tears. By 2025, 21 of the patients had undergone a revision for ≥1 retear of the initial suture site. Of these cases, we analyzed those of the 11 patients with ≥1 year of postoperative follow-up (Figure 1).

Flowchart of the patient cases.
Of the 1250 patients who underwent an isolated meniscal repair at our institution in 2018 to 2024, 21 patients required a revision meniscal repair for retear at the same site as the initial repair. We excluded the cases of the 3 patients who could not be followed up for ≥1 year and the 7 patients with missing data. Of the 7 patients, 4 did not undergo MRI examination at the 1-year follow-up, and 3 had unavailable preoperative clinical scores. Therefore, 11 knees were included in the final analysis.
Participant Characteristics
The 11 patients comprised 7 male and 4 female patients (median age at revision: 23 years; IQR, 17-32 years). The median body mass index was 25.8 kg/m2 (IQR, 20.6-28.4 kg/m2). The median duration between the primary operation and revision was 13 months (IQR, 6-25 months). The median follow-up period after revision meniscal repair was 20 months (range, 12-28 months). In 2 patients, the retear occurred with trauma; in the 9 others, it occurred without trauma. Ten cases involved lateral meniscal tears, and a single case involved a medial meniscal tear. The median %MA and PTS were 48.0% (IQR, 40.0%-57.8%) and 11.5° (IQR, 8.5°-13.5°), respectively. The details of each patient's case are listed in Table 1.
Characteristics of Patients With ≥1 Year of Postoperative Follow-up After Revision Meniscal Repair for Retears at the Initial Suture Site a
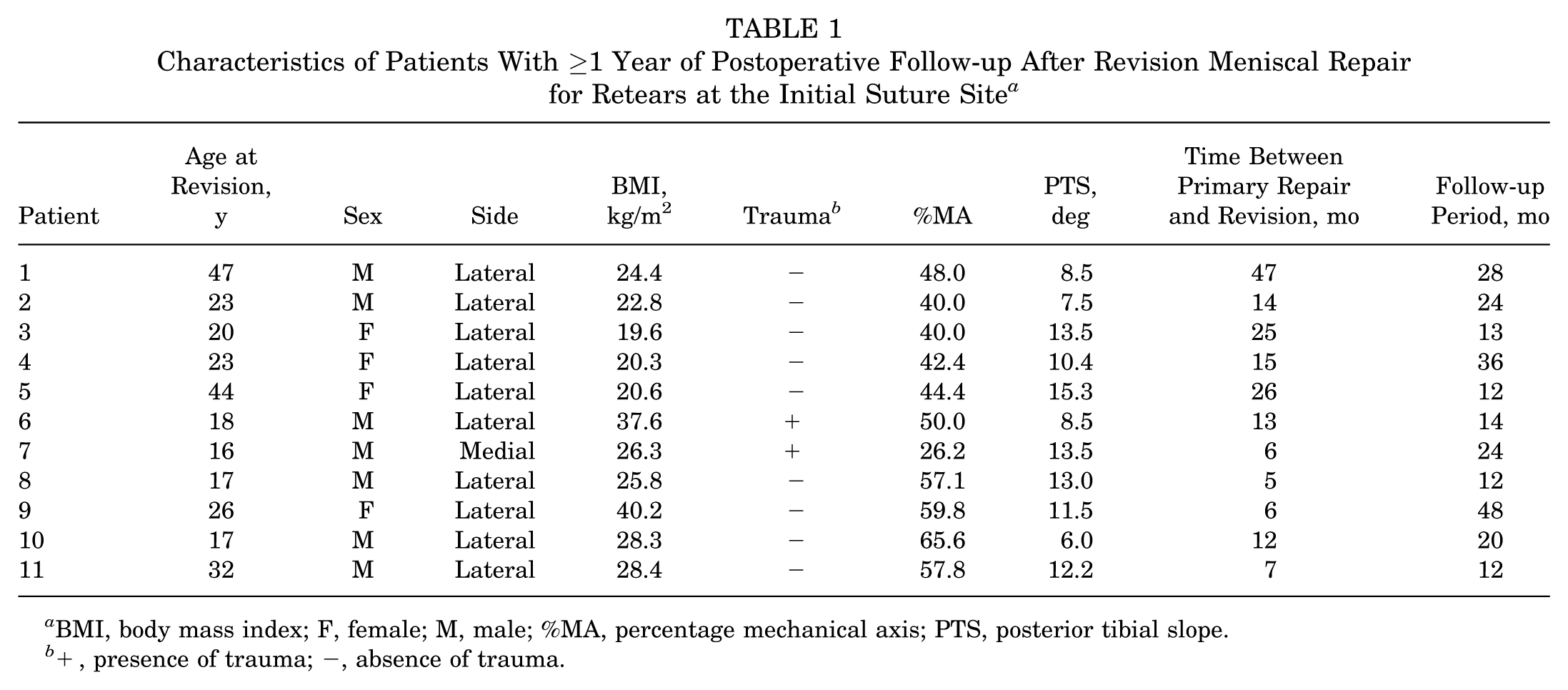
BMI, body mass index; F, female; M, male; %MA, percentage mechanical axis; PTS, posterior tibial slope.
+, presence of trauma; −, absence of trauma.
Location, Tear Type, and Number of Sutures
As summarized in Table 2, the retear occurred at the primary suturing site in all 11 cases. The retear case was located in the R-R zone, and in the other 10 cases the retear was located in the R-W zone. At the time of the primary repair, the numbers of tear types were as follows: simple longitudinal (n = 7), bucket-handle (n = 2), radial (n = 1), and horizontal (n = 1); at revision, the numbers were longitudinal (n = 5), bucket-handle (n = 2), and complex (n = 4). The tear type changed to complex tears between the primary repair and revision in 4 patients (patients 6, 7, 9, and 10). The comparison of the number of sutures required for the original tear and the revision revealed that the number increased in 6 patients, stayed the same in 4 patients, and decreased in 1 patient. Meniscal degeneration was assessed intraoperatively based on arthroscopic findings, including tissue fragility, surface fibrosis, and loss of normal meniscal structure. There were mild or moderate degenerative changes of the meniscus at revision in 4 cases (patients 2, 5, 7, and 10). The final decision for revision meniscal repair was made at the surgeon's discretion based on the quality of the meniscus and its reparability as determined by arthroscopic findings. At the time of initial surgery, 6 cases were repaired using the all-inside technique, 2 using the inside-out technique, and 1 case each using the outside-in technique, a combination of the inside-out and outside-in techniques, and a combination of the all-inside and inside-out techniques.
Location of Tear, Tear Type, Number of Sutures, and Presence/Absence of Degenerative Changes of Meniscus a
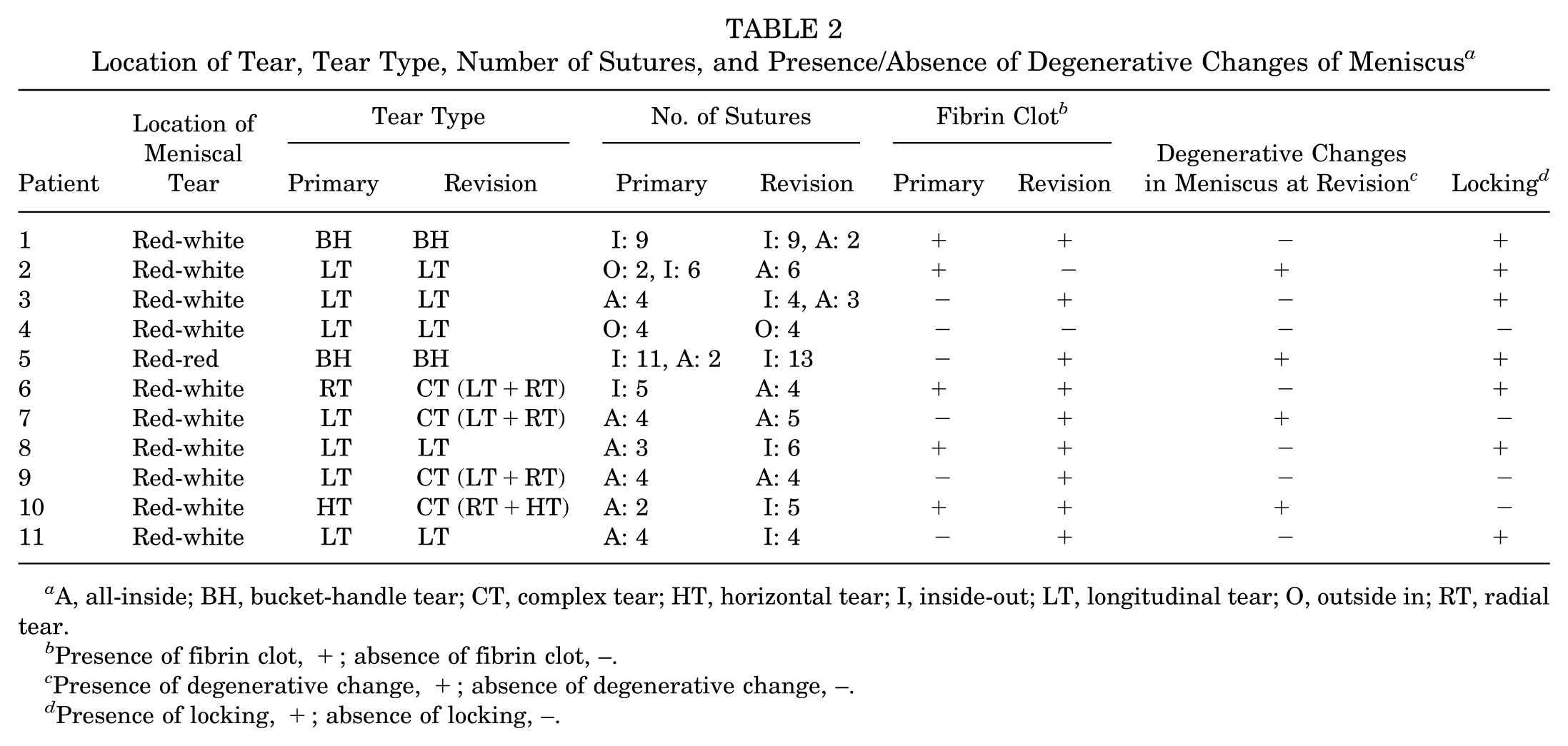
A, all-inside; BH, bucket-handle tear; CT, complex tear; HT, horizontal tear; I, inside-out; LT, longitudinal tear; O, outside in; RT, radial tear.
Presence of fibrin clot, +; absence of fibrin clot, –.
Presence of degenerative change, +; absence of degenerative change, –.
Presence of locking, +; absence of locking, –.
Complications
No short-term or long-term postoperative complications were observed during the follow-up period. Specifically, no cases of infection, joint stiffness requiring intervention, neurovascular injury, or reoperation were recorded.
Clinical Results
As illustrated in Figure 2, there was no significant difference in the patients' Tegner scores between the prerevision stage at 6.0 (IQR, 2.0-7.0) points and the final survey at 7.0 (IQR, 2.0-9.0) points (P = .57). However, in all 11 patients, the Tegner scores after revision were equivalent to or higher than the prerevision scores. The median Lysholm score improved significantly from 57.0 (IQR, 40.0-81.0) points at prerevision to 91.0 (IQR, 90.0-100.0) points at the final survey (with a median increase of 30.0 points; 95% CI, 14.1–45.6; P = .002; r = 0.89). Similarly, the median IKDC score improved significantly from 50.8 (IQR, 37.9-72.4) points at prerevision to 88.5 (IQR, 74.7-94.3) points at the final survey (with a median increase of 25.3 points; 95% CI, 19.2-40.3; P < .001; r = 0.89) (Figures 3 and 4).

Comparison of the patients' Tegner sports activity scores at prerevision and postfinal surgery. There was no significant (n.s.) difference in these scores, which changed from 6 (IQR, 2-7) to 7 (IQR, 2-9) (Wilcoxon signed-rank test; P = .57).

Comparison of the patients' Lysholm scores obtained at prerevision and postfinal surgery. The Lysholm score significantly improved from 57.0 (IQR, 40.0-81.0) preoperatively to 91.0 (IQR, 90.0-100.0) at final follow-up (Wilcoxon signed-rank test; *P = .002).

Comparison of the patients' International Knee Documentation Committee (IKDC) scores at prerevision and postfinal surgery. The IKDC score significantly improved from 50.8 (IQR, 37.9-72.4) preoperatively to 88.5 (IQR, 74.7-94.3) at final follow-up (Wilcoxon signed-rank test; *P = .002).
MRI Evaluation
The intraobserver reliability was a discrepancy between grade 3 and grade 4 in 1 of 11 cases, and the K coefficient was 0.81. Minor disagreement was observed between the 2 evaluators in 3 cases: 2 cases involved classification between grades 3 and 4, and 1 case involved a difference in the determination of low-to-intermediate signal change and high signal change. The final classification was determined through consultation between 2 observers, and the kappa coefficient for this study was 0.79. Intraobserver reliability and interobserver reliability were rated as excellent and good, respectively. The patients' postoperative MRI findings showed grade 3 lesions in 5 cases and grade 4 lesions in 6 cases (Table 3). Two cases that were grade 4 at the postoperative evaluation had been changed to grade 3 at the 1-year postoperative MRI examination (patients 2 and 8). Regardless of the presence of grade 3 or 4 lesions, 8 patients showed low signal changes at the revision site (Figure 5). However, high signal intensity changes were observed at the revision sites in 3 grade 4 cases (Figure 6).
Postrevision Results: Tegner, Lysholm, and IKDC Scores a
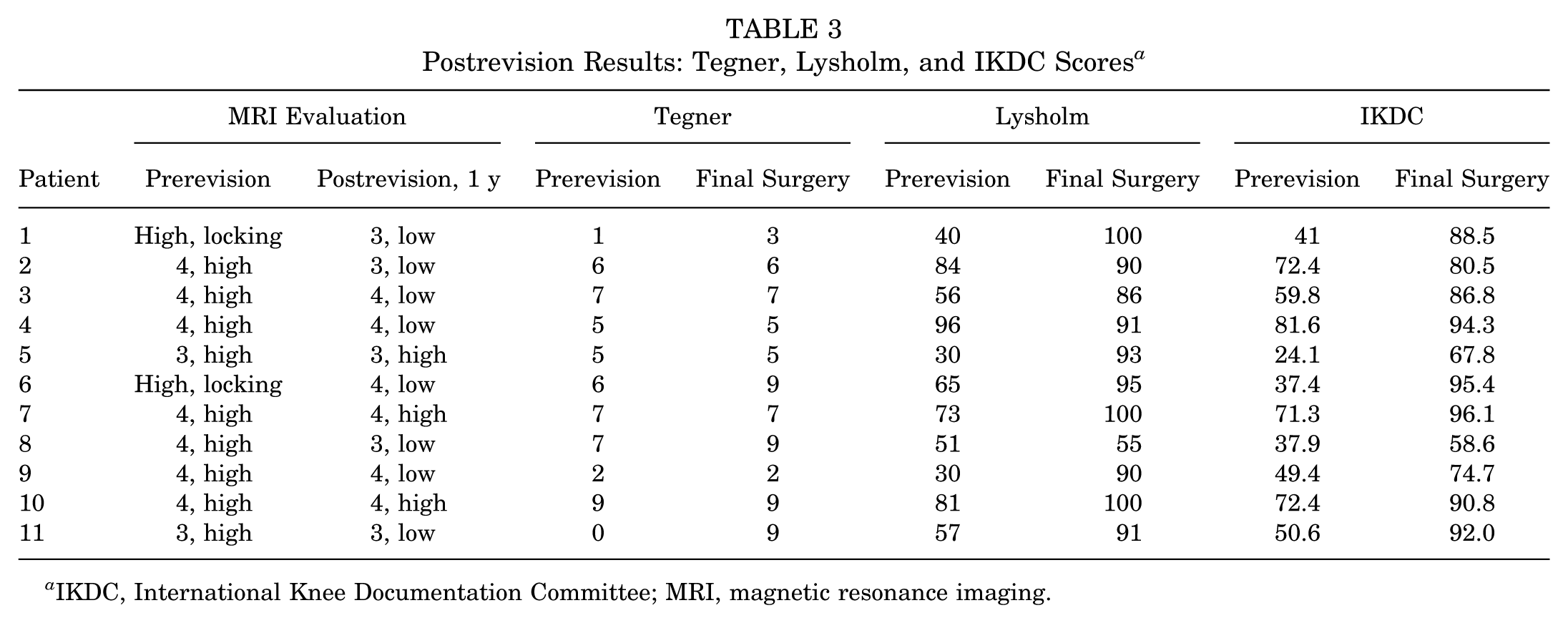
IKDC, International Knee Documentation Committee; MRI, magnetic resonance imaging.

Magnetic resonance imaging (MRI) findings of the torn area at prerevision and 1 year postrevision (coronal and sagittal sections on T2-weighted scans). In patient 1 at the prerevision stage, the meniscal fragment was displaced into the intercondylar fossa (white arrows). At 1 year postrevision, the suture site exhibited a low signal intensity change compared with the joint fluid.

Magnetic resonance imaging (MRI) findings of the torn area at the prerevision stage and at 1 year postrevision (coronal and sagittal sections on T2-weighted scans). In patient 7, at 1 year postrevision, the suture site exhibited a high signal intensity change equivalent to the joint fluid (white arrowheads).
Discussion
The major findings of our study demonstrated that clinical outcomes significantly improved after revision meniscal repair, with the Lysholm score increasing from 57.0 (IQR, 40.0-81.0) to 91.0 (IQR, 90.0-100.0) (P = .002) and the IKDC score increasing from 50.8 (IQR, 37.9-72.4) to 88.5 (IQR, 74.7-94.3) (P = .002). Our analyses revealed that satisfactory knee function and activity levels were maintained by revision meniscal repair compared with the prerevision status were achieved. Revision meniscal repair can thus be considered a valuable treatment option for cases of meniscal retear following isolated meniscal repair. Our results corroborate and extend several prior studies' findings.4,7,12,14,33
Anterior cruciate ligament (ACL) reconstruction performed concurrently with meniscal repair has been demonstrated to improve the healing rate of the repaired meniscus. 17 We thus excluded from the present study the cases of patients who underwent a ligament reconstruction surgery that included ACL reconstruction. Voloshin et al 33 analyzed 18 cases of revision meniscal repair, and they described a clinical success rate of 72% after a mean follow-up of 7 years. Imade et al 12 analyzed the outcomes of 15 cases of revision meniscal repair, reporting a 71.4% success rate for isolated meniscal retears without concomitant ACL injury at a mean follow-up of 35 ± 17 months. Fuchs et al 7 described a 75% success rate for 12 cases of isolated revision meniscal repair at a mean follow-up of 43 ± 23 months. In the present study, the patients' MRI evaluations at 1 year after final surgery indicated structural continuity of the revision site in 8 of the 11 cases (72.7%). Previous studies by Voloshin et al 33 and Krych et al 14 demonstrated that, despite favorable early outcomes, clinical results after meniscal repair deteriorate over time. Our study presents only short-term results based on a minimum of 1 year of follow-up and should not project the findings to long-term joint preservation or osteoarthritis prevention. Furthermore, in this study, the interval between primary meniscal repair and revision varied considerably between cases (5 to 47 months). Our study suggests potential heterogeneity in the failure mechanisms. Early retears may reflect biological or technical factors, whereas delayed retears may be associated with progressive degenerative changes. Although subgroup analysis based on the interval between primary meniscal repair and revision was not feasible due to the small sample size, this interval should be considered as a potential confounding factor. Future studies should increase the number of cases and analyze stratified by the duration until revision.
When degeneration of the meniscal tissue is observed, the prognosis following a revision is poor; it has been suggested that revision meniscal repair should be considered for meniscal tears without degenerative changes. 12 In our present series of cases, meniscal degeneration was observed in all of the failed cases; we thus suggest that the presence of degenerative changes on arthroscopic findings may adversely affect the outcome after revision. During arthroscopy, surgeons should carefully evaluate the quality of meniscal tissue and consider that degenerative changes may lead to poorer postoperative outcomes. In addition, the outcomes of repairs for degenerative medial meniscal tears accompanied by varus deformity (%MA < 30%) are poor. 20 In the present patient series, the revision medial meniscal repair case (patient 7) also exhibited varus alignment with a %MA at 26.1%, and healing had not been achieved on MRI at 1 year postoperatively. However, only 1 case involved the medial meniscus, with the majority being lateral meniscus. Consequently, the relationship between lower limb alignment and imaging outcomes could not be statistically analyzed. Therefore, the potential impact of alignment on revision meniscal repair outcomes remains exploratory, necessitating further studies with larger cohorts.
Functional outcomes following revision meniscal repair are favorable in several studies.7,12,14,33 Both Imade et al 12 and Fuchs et al 7 reported high Lysholm scores (97.4 and 95.2, respectively) at the midterm follow-up. Our analyses revealed that the Lysholm score at 1 year after the final surgery was 91.0, demonstrating favorable outcomes that are comparable with those in previous studies. Regarding the IKDC score, Krych et al 14 reported a good result (84.8 points) at a 6-year follow-up, and our present analyses showed a similar result at 88.5 points. However, in another investigation, Voloshin et al 33 examined functional scores at a longer follow-up (7 years) and observed lower scores, with a mean Lysholm score at 82.1 points and mean IKDC score at 78.5. Although the postoperative failure rate was similar, worsening outcomes at long-term follow-up suggest that, despite meniscal preservation by revision, the remaining meniscal tissue may gradually degenerate, leading to poorer long-term outcomes. Further investigations of the long-term outcomes of revision meniscal repair are needed to assess whether revision meniscal retears and the preservation of meniscal tissue provide long-term functional benefits.
Activity level is another important outcome after meniscal repair. The Tegner score is consistently high after meniscal repair, with mean scores ranging from 5.6 to 6.8 points.7,12,14,33 These scores are very similar to the postoperative Tegner scores ranging from 4.0 to 7.3 points observed after primary meniscal repair. 31 In the present study, a nonsignificant difference in the Tegner score was observed compared with the preoperative scores, but the postoperative Tegner score (6.5 points) was consistent with the findings of previous studies. This finding may indicate that patients were generally able to sustain their preoperative activity level following revision meniscal repair.
A notable finding of our present investigation is that among the 11 patients who underwent a revision meniscal repair, 2 presented with bucket-handle tears and 2 with longitudinal tears. According to the report by Imade et al, 12 among 7 cases requiring an isolated revision meniscal repair excluding ACL combined injuries, 3 were bucket-handle tears and 4 were longitudinal tears; 5 of the 7 cases were R-W zone lesions. Fuchs et al 7 reported that in cases requiring an isolated revision meniscal repair, 83.3% of the initial tear patterns were bucket-handle tears or longitudinal tears (5 of 12 cases were bucket-handle tears, 5 were longitudinal tears; 9 of the 12 cases were R-W zone lesions). Similar to these studies, the majority of the present study's cases involving a revision meniscal repair were extensive longitudinal tears or bucket-handle tears in the R-W zone, causing knee locking. In a study of patients with bucket-handle meniscal tears of the R-R zone and R-W zone, 82.7% achieved complete healing. 5 On the other hand, it has also been documented that 21% of revision meniscal repairs for bucket-handle meniscal tears failed. 13 These findings emphasize that although longitudinal tears and bucket-handle tears 9 within the R-W zone 1 are generally considered to heal readily, many cases experience retear leading to resuturing. For extensive longitudinal tears and bucket-handle tears that may cause locking, strong suturing is desirable for the initial repair.
Limitations
Our study has several limitations. (1) The study cohort was relatively small and only a univariate analysis was performed. However, revision meniscal repair cases are rare and we excluded the cases of patients who underwent a concomitant ligament reconstruction or osteotomy, and thus the study cohort represented a relatively homogeneous group. (2) The failure of meniscal repairs was assessed only by MRI and, because of ethical concerns, was not evaluated by second-look arthroscopy, leaving the actual failure rate potentially underestimated. (3) The minimal follow-up period was short (1 year) compared with previous studies. (4) We were unable to establish a control group that underwent conservative treatment or meniscectomy for meniscal retears, and we were thus unable to clarify whether revision meniscal repair is superior to conservative treatment or partial meniscectomy. (5) In revision, the repair technique, variations in suture count, and selective use of fibrin clots were determined based on the characteristics of the laceration and the surgeon's judgment. This technical heterogeneity represents a significant limitation of this study, making it impossible to determine whether the observed improvement was attributable to revision itself or from specific technical factors. (6) Nearly half of the eligible patients were excluded as a result of incomplete data or loss to follow-up. Although these exclusions were related to missing MRI or baseline clinical score rather than clinical failure, this level of attrition may introduce selection bias and limit the internal validity of the study. In the future, a collection of cases of revision meniscal repair, long-term follow-up, and comparative studies using control groups will be required.
Conclusion
Our study showed that revision meniscal repair may improve short-term clinical results in carefully selected patients with retears. Further research is required to define optimal indications and techniques.
Footnotes
Final revision submitted March 26, 2026; accepted April 22, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the research ethics committee of the authors' institutions (approval No. 25110501).