
Abstract
Background:
Posterior medial meniscus root tears (PMMRTs) are frequently observed injuries that alter tibiofemoral biomechanics, yet the long-term outcomes are poorly described.
Purpose:
To perform a systematic review and meta-analysis of the current literature on long-term clinical and radiographic outcomes of operatively managed PMMRTs.
Study Design:
Meta-analysis and systematic review; Level of evidence, 4.
Methods:
A systematic review was performed with the inclusion criteria of English-language studies, diagnosis of PMMRT on magnetic resonance imaging, and minimum 5-year radiographic or patient-reported outcome (PRO) metrics. Data analysis included management strategy, surgical technique, meniscal extrusion, medial joint space, PROs, and radiographic measurements. Failure was defined as conversion to arthroplasty, subsequent partial medial meniscectomy (PMM) and/or proximal tibial osteotomy, or clinical failure on PROs. Continuous outcome variables were analyzed with a random effects meta-analysis of mean differences. Chi-square meta-analysis was also used to analyze categorical variables.
Results:
Twelve studies were identified with >5-year follow-up after PMMRT (mean ± SD, 84.1 ± 11.0 months). Five studies performed PMM, 6 performed medial meniscus root repair (MMR), and 1 utilized either meniscectomy or repair. There were 797 total patients (female, n = 667; 83.7%), with mean ages ranging from 47.2 to 65. Both interventions showed significant PRO improvements after surgery: PMM (pre- vs postoperative Lysholm, 56.1 vs 68.2; P < .01) and MMR (Lysholm, 52.1 vs 83.1; International Knee Documentation Committee [IKDC], 40.0 vs 72.8; P < .01). MMR had significantly lower Kellgren-Lawrence grades (PMM vs MMR, 2.4 vs 1.8; P < .01) and superior IKDC scores (46.5 vs 72.8; P < .01) as compared with PMM. Additionally, PMM had a significantly higher failure rate (23% vs 5.3%) and conversion to knee arthroplasty (20.5% vs 3.5%) as compared with MMR, with odds ratios of 9.8 and 10.2, respectively.
Conclusion:
This systematic review and meta-analysis of studies with >5-year minimum follow-up found that PMM was associated with a 10-fold increase in clinical failure and conversion to knee arthroplasty relative to MMR in observational studies. In addition, MMR demonstrated superior Kellgren-Lawrence grades and IKDC scores as compared with PMM. The findings of the current analysis suggest that MMR is associated with superior outcomes as compared with PMM at mid- to long-term follow-up.
Posterior medial meniscus root tears (PMMRTs) are an increasingly recognized pathology in the literature.1,11,20 A PMMRT is defined as an avulsion or complete radial tear within 1 cm of the anatomic origin of the posterior medial root. 15 These injuries are frequently seen in patients in the fourth to sixth decades of life and are more common in female patients. 15 They most commonly occur as the knee goes into deep flexion, with the knee in external rotation such as a squat. 22
Biomechanical evidence has shown that PMMRTs significantly impair the meniscus's ability to convert axial tibiofemoral loads into hoop stresses.14,24 Additionally, PMMRTs are associated with extrusion of the medial meniscus outside of the joint space.26,28 Together, these altered biomechanics lead to increased cartilage degeneration and osteophyte formation. After PMMRTs, several treatment modalities have been proposed, including nonoperative protocols, 19 partial medial meniscectomy (PMM), 25 and several medial meniscus root repair (MMR) techniques. 12
While the biomechanical evidence suggests that anatomic repair is able to restore native contact pressures in cadaveric specimens,23,31 there are few studies that report on the longer-term sequela and patient-reported outcomes (PROs) of the management of PMMRTs. Previous systematic reviews have reported on short-term outcomes of PMMRT treatment modalities and have found repair to be favorable with respect to cartilage degeneration and cost-effectiveness.10,32 However, these reviews included only studies with minimum 1- or 2-year follow-up.10,32 This study aimed to perform a systematic review and meta-analysis of the current literature examining mid- to long-term clinical and radiographic outcomes of PMMRTs with or without treatment. By consolidating this information, the current analysis seeks to provide a reference to guide clinicians and knee surgeons about the optimal treatment strategies for managing PMMRTs.
Methods
A systematic review of articles was completed per the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) on the mid- to long-term outcomes of PMMRTs via PubMed, Scopus, and Google Scholar (1995-2025). The query was performed in March 2025. The specific search terms utilized were “medial meniscus” AND “outcome” OR “outcomes” (Figure 1).
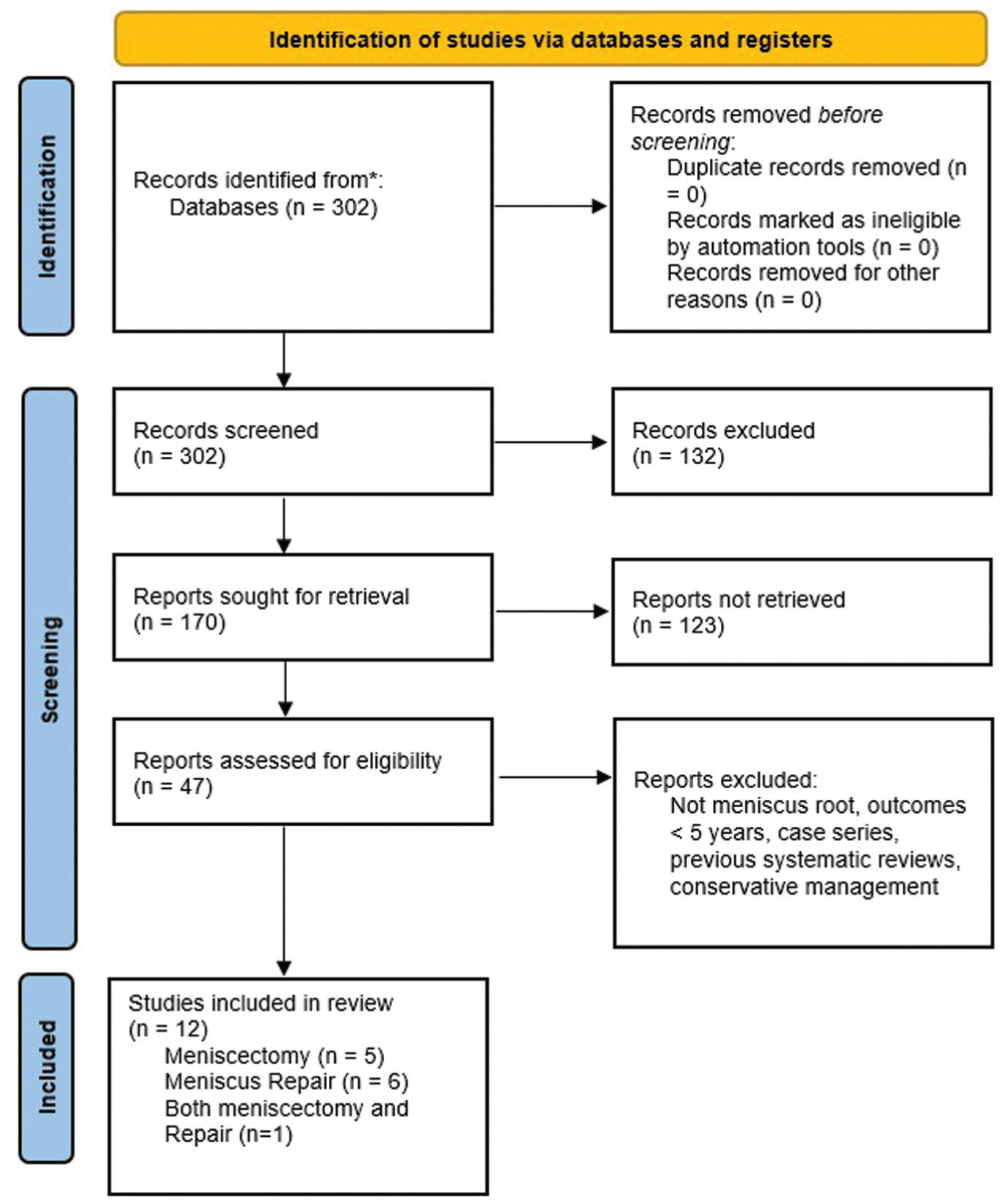
PRISMA flowchart of the current study.
The inclusion criteria for the systematic review consisted of the following: English-language studies, diagnosis of PMMRT on magnetic resonance imaging (MRI) with confirmation on arthroscopy if managed operatively, and studies with minimum 5-year radiographic and/or PRO metrics. The exclusion criteria consisted of studies with <5-year minimum outcomes, non–English language studies, non–meniscus root tears or inability to isolate and stratify cases of root tear, nonoperative management, case studies (level 5 evidence), and/or previous systematic review or meta-analysis. Two investigators (R.S.D. and R.M.) independently reviewed the abstracts from all identified articles. When necessary, full-text articles were obtained for review to allow further application of the established inclusion and exclusion criteria.
Data Extraction
The variables of interest that were extracted from each study for the systematic review and meta-analysis included descriptive article information, patient demographics, diagnosis modality, management strategy, surgical technique, concomitant pathologies, amount of meniscal extrusion on MRI (in millimeters), medial compartment joint space on plain radiographs (in millimeters), and pre- and postoperative PRO scores. Additionally, when available, radiographic arthritis findings were collected, as defined by the Kellgren-Lawrence classification system or Outerbridge classification. PRO scores were recorded pre- and postoperatively. Failure was defined as conversion to arthroplasty, subsequent PMM and/or proximal tibial osteotomy, or clinical failure on PROs (Lysholm <65). 7
Quality Assessment
Two reviewers (R.S.D. and R.M.) independently assessed the risk of bias of the included articles using the Newcastle-Ottawa Scale. This validated assessment tool is used to evaluate nonrandomized studies based on 3 main criteria: how study groups are selected, the degree of comparability between groups, and how outcomes of interest are measured. Study quality was classified as good, fair, or poor, with a maximum possible score of 9. 35 Studies scoring between 7 and 9 stars were considered high quality, those with 4 to 6 stars were deemed fair, and scores from 0 to 3 indicated poor quality.
Data Analysis
We extracted and pooled outcomes of interest and related standard error using DerSimonian and Laird random effect models. 9 Heterogeneity among studies was quantified by the I2 statistic. Random effects models were used when the I2 value was >50%. To determine the statistical significance between groups in the random effects model, we used a Z test for differences in pooled means. 2 To determine statistical significance of categorical variables in the meta-analysis, a chi-square test was utilized. Odds ratios (ORs) were used to assess the likelihood of failure and conversion to knee arthroplasty between the meniscectomy and meniscal repair cohorts. P < .05 was considered statistically significant.
Results
The literature search identified 302 studies. Of these, 170 abstracts and 47 full texts were reviewed. Ultimately, 12 studies were included in the final analysis. In total, these studies included 797 patients with PMMRTs, all of which were diagnosed with preoperative MRI. There were 130 males and 667 females. The mean ages of the patients in the final analysis ranged from 47.2 to 65.6 years,4,29 and the mean body mass index (BMI) ranged from 25.1 to 32.9. 4 All 12 studies were considered high quality by the Newcastle-Ottawa Scale, relative to risk of bias; specific grades are presented in Table 1.
Studies Included in the Final Analysis a
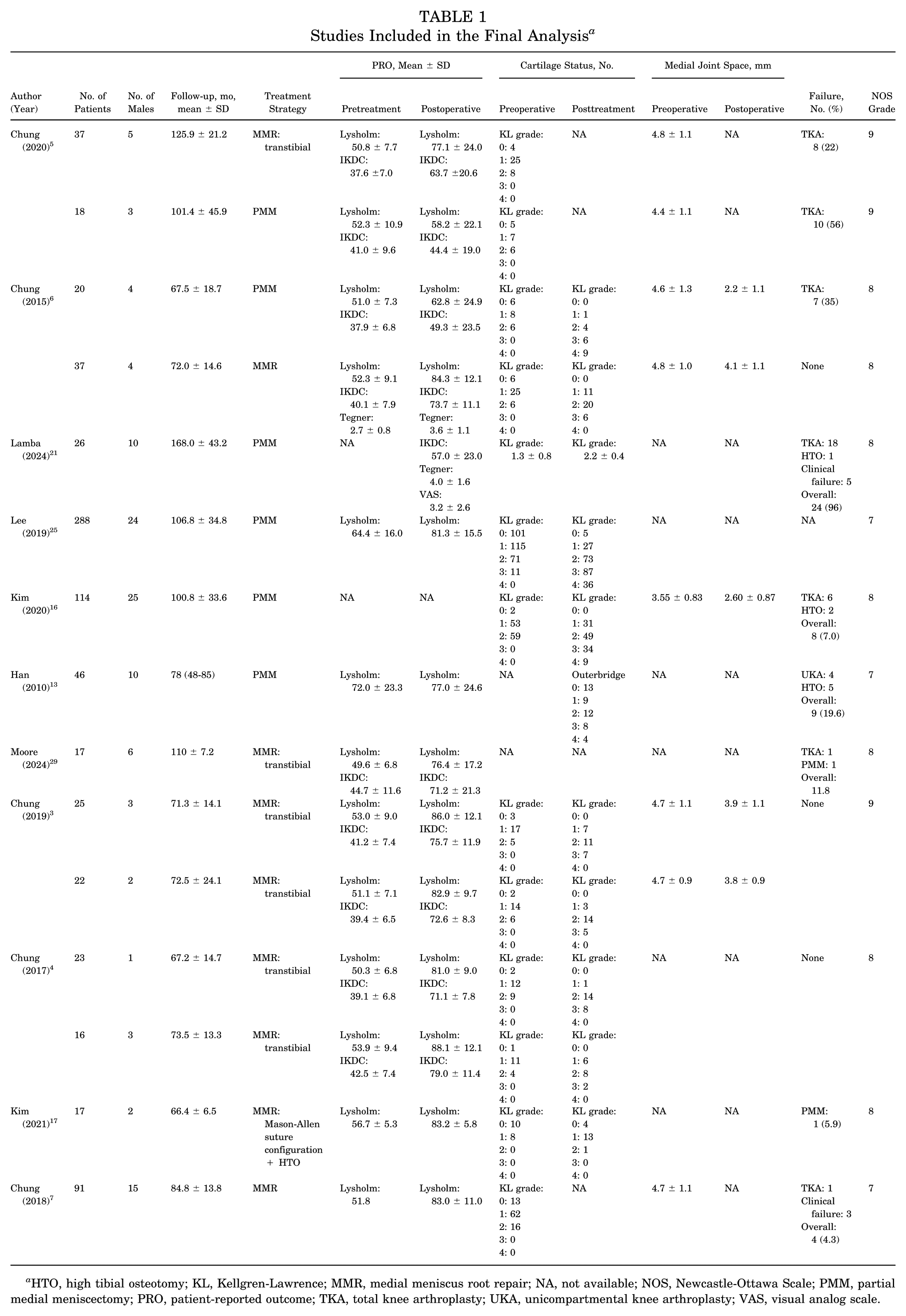
HTO, high tibial osteotomy; KL, Kellgren-Lawrence; MMR, medial meniscus root repair; NA, not available; NOS, Newcastle-Ottawa Scale; PMM, partial medial meniscectomy; PRO, patient-reported outcome; TKA, total knee arthroplasty; UKA, unicompartmental knee arthroplasty; VAS, visual analog scale.
There were 5 studies5,6,13,16,21,25 that performed partial medial meniscectomies and 6 studies3-7,17,29 that performed meniscal repairs; 1 comparative study included patients undergoing repair and PMM. 5 Among repair studies, 6 (85.7%)3-7,29 utilized a transosseous repair technique, and 1 study 17 performed a high tibial osteotomy with Mason-Allen suture anchor repair. Two studies16,17 (n = 71; 8.4%) stated that a portion of patients had varus deformities (defined as >3°); 17 of these patients from a single study were treated with a proximal tibial osteotomy and concomitant MMR 17 and 54 were treated with PMM. 16
Meta-Analysis
Comparative data between the demographic variables of the PMM and MMR cohorts are presented in Table 2. Additionally, Table 3 provides analysis of the PRO metrics, as well as radiographic and imaging analysis comparing the MMR and PMM cohorts. The forest plots for this analysis are presented in Appendix Figures A1 to A8.
Demographic Variables Comparing the Partial Medial Meniscectomy Cohort With the Meniscal Repair Cohort a
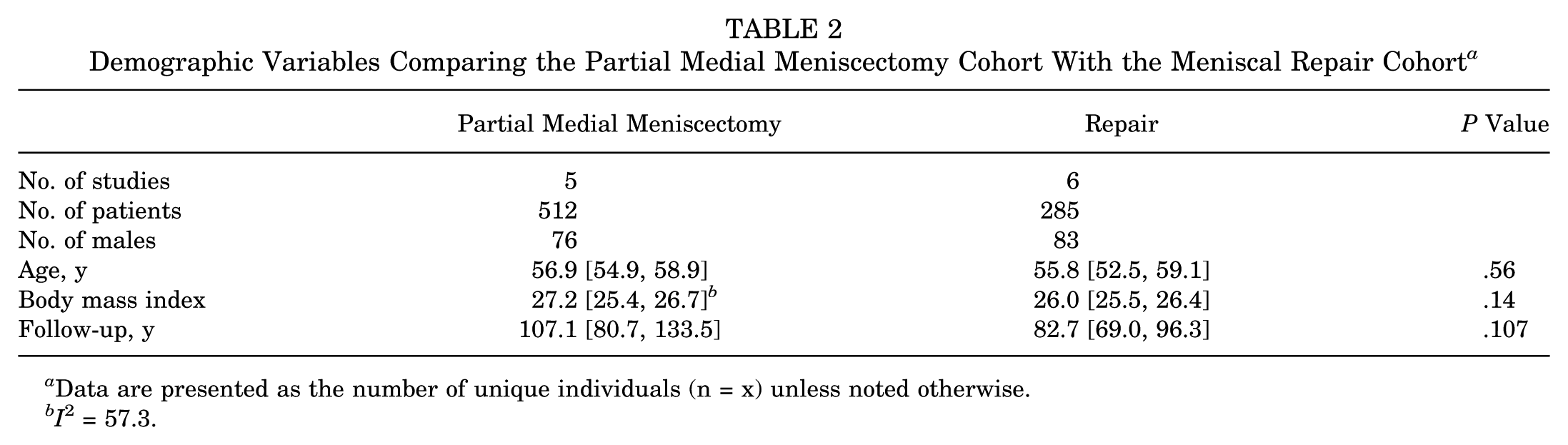
Data are presented as the number of unique individuals (n = x) unless noted otherwise.
I 2 = 57.3.
Outcome Variable Comparison Between the Meniscectomy Cohort and the Meniscal Repair Cohort a
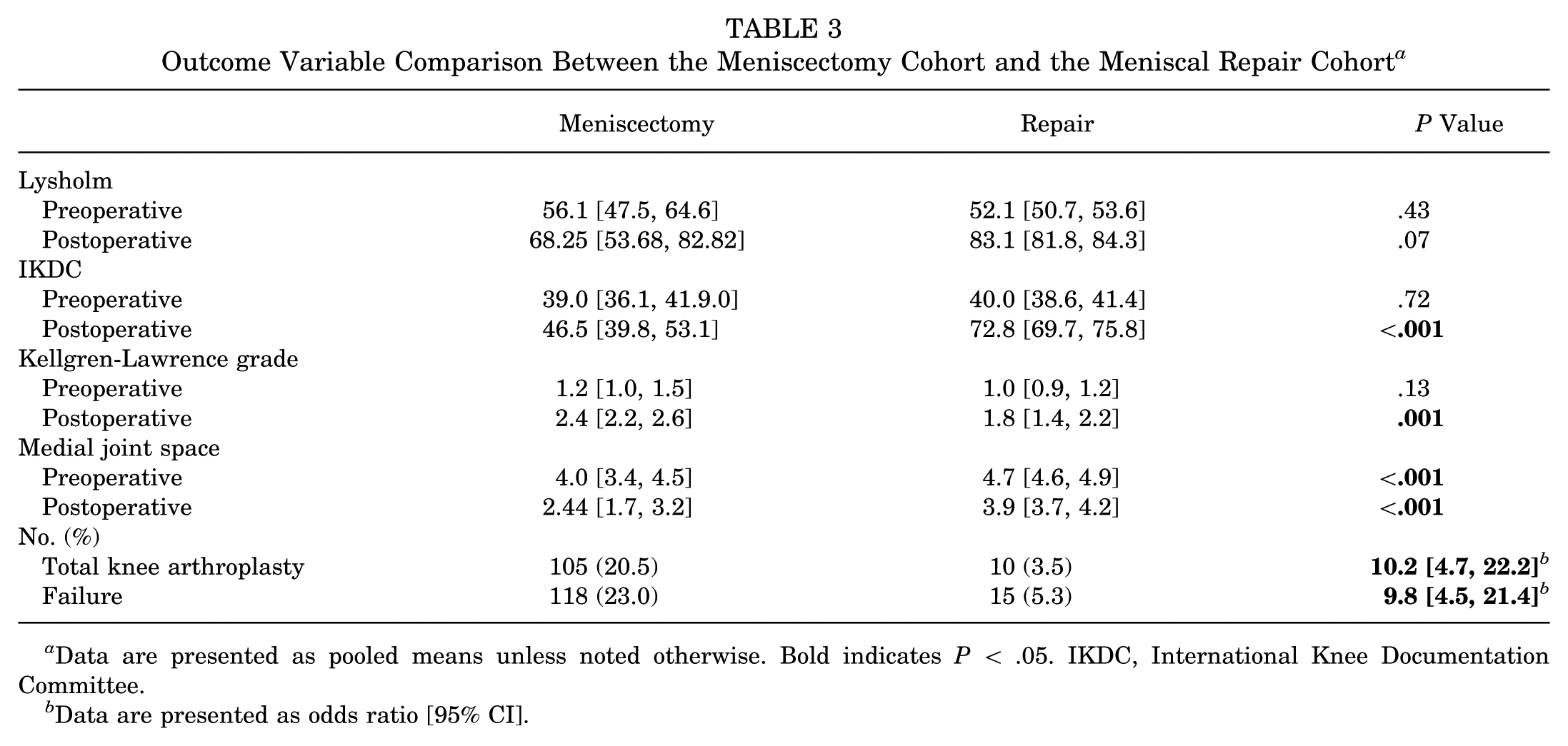
Data are presented as pooled means unless noted otherwise. Bold indicates P < .05. IKDC, International Knee Documentation Committee.
Data are presented as odds ratio [95% CI].
The preoperative Kellgren-Lawrence grades for the meniscectomy cohort were as follows: grade 0, 111; grade 1, 206; grade 2, 114; grade 3, 13; and grade 4, 0. In the meniscal repair cohort, the preoperative Kellgren-Lawrence grades were as follows: grade 0, 35; grade 1, 149; grade 2, 48; grade 3, 0; and grade 4, 0. On chi-square analysis, the distribution by grade in these cohorts was significantly different (P < .01).
The postoperative Kellgren-Lawrence grades for the meniscectomy cohort were as follows: grade 0, 5; grade 1, 59; grade 2, 136; grade 3, 127; and grade 4, 54. The postoperative KL grades for the meniscus root repair cohort were as follows: grade 0, 4; grade 1, 41; grade 2, 68; grade 3, 28; and grade 4, 0. Both these postoperative cohorts were significantly different from their preoperative cohorts. In the postoperative meniscectomy group, 181 (38.2%) patients had Kellgren-Lawrence grade 3 or 4. In the postoperative meniscal repair group, 28 (19.9%) patients had Kellgren-Lawrence grade 3 or 4 at latest available follow-up, as compared with 0 patients with these grades preoperatively.
Tables 4 and 5 present further analysis comparing preoperative PROs and radiographic parameters for both cohorts.
Comparison Between Pre- and Postoperative Outcomes of the Meniscectomy Cohort a
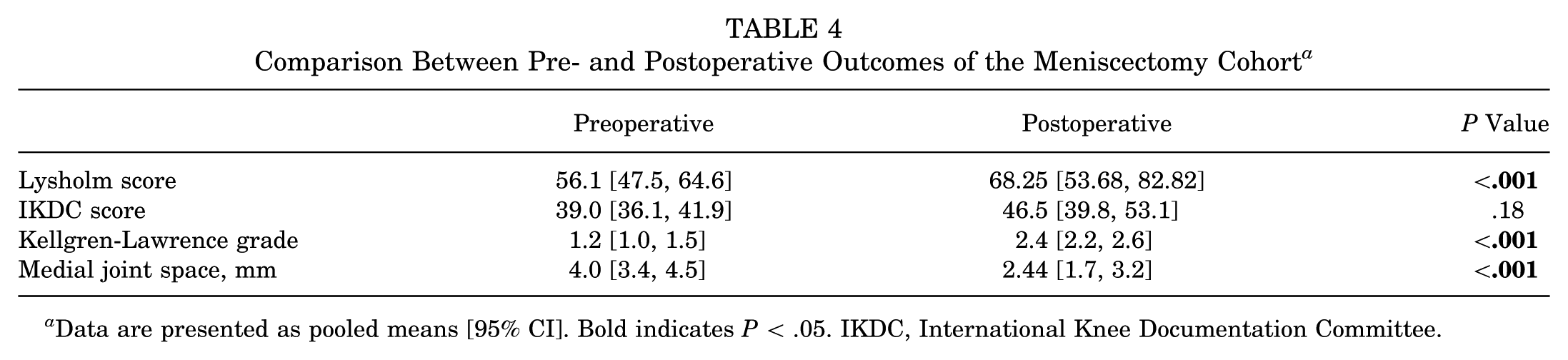
Data are presented as pooled means [95% CI]. Bold indicates P < .05. IKDC, International Knee Documentation Committee.
Comparison Between Pre- and Postoperative Outcomes of the Meniscal Repair Cohort a
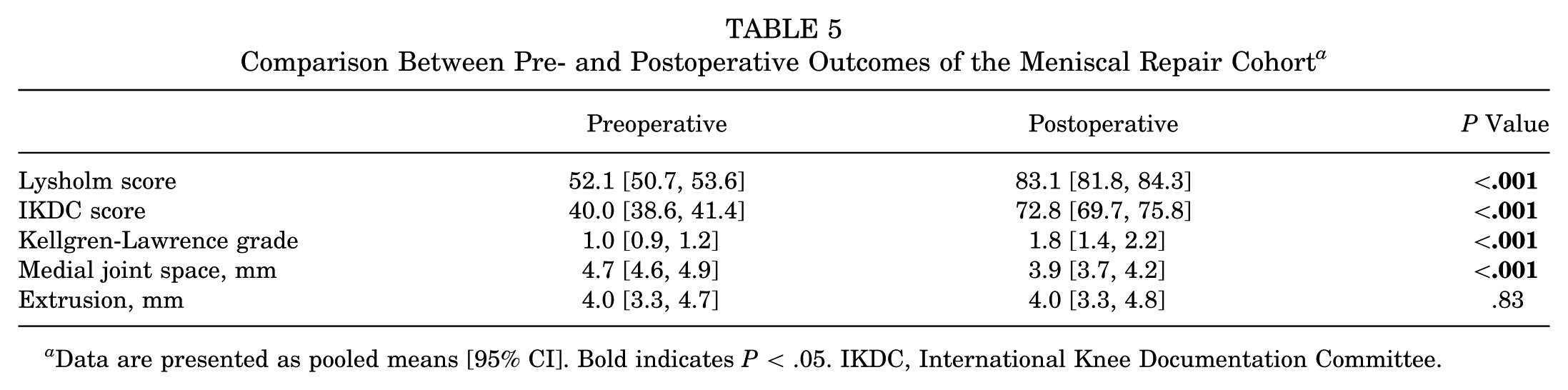
Data are presented as pooled means [95% CI]. Bold indicates P < .05. IKDC, International Knee Documentation Committee.
Discussion
The primary findings of the current analysis were that PMM was associated with an approximately 10-fold increase in clinical failure and conversion to knee arthroplasty when compared with MMR. Additionally, MMR had statistically superior International Knee Documentation Committee (IKDC) and Kellgren-Lawrence scores as compared with PMM at long-term follow-up among the studies. Ultimately, this study demonstrates that the early favorability of MMR and PMM is maintained and even expanded at longer-term follow-up (minimum 5 years). Clinicians can use this study to better counsel their patients about the long-term risks and expectations of both interventions and encourage surgeons to attempt MMR when possible.
The current analysis found an increased OR for conversion to total knee arthroplasty (OR, 10.2) and failure (OR, 9.8) with PMM was compared with MMR. Similarly, this study revealed superior IKDC scores and greater medial joint space in the MMR group. A previous meta-analysis 10 reported lower estimated 10-year costs and cartilage degeneration with MMR compared with PMM based on Markov models that utilized minimum 1-year follow-up data. Additionally, a meta-analysis that included minimum 2-year follow-up outcomes noted greater improvements in Lysholm score and lower rates of arthritis progression and reoperation with MMR. 33 The current analysis adds to the findings of these previous studies and demonstrates that the superiority of MMR over PMM persists at longer-term follow-up.
Despite the superior radiographic and clinical outcomes among the MMR cohort as compared with the PMM cohort, it is important to note that both groups had improved PRO scores at the latest available follow-up as compared with the preoperative PROs. Of the included studies, a majority of patients had Kellgren-Lawrence grade 2, which is important to note as recent reports have revealed significantly faster progression of symptomatic arthritis in patients with worse preoperative cartilage status. 34 Additionally, the findings of the current analysis can be compared with the work from Krych et al, 18 who performed a retrospective comparative study of PMM versus PMMRT cases managed nonoperatively and found no significant difference between the cohorts with respect to PROs, arthritis progression, or failure rate. The current meta-analysis demonstrates a clinically significant improvement in PROs with PMM and MMR, despite the inferior radiographic measurements with either surgical intervention; however, future studies should examine this comparison in a prospective randomized fashion. Additionally, despite the clinical and radiographic improvements identified with MMR in the current study, no significant improvement was found in amount of meniscal extrusion at latest available imaging follow-up. Previous literature has reported complete meniscus root healing on second-look arthroscopy at 2-year follow-up in approximately 75% of MMRTs. 8 A previous biomechanical analysis showed that at baseline the meniscus is 1.5 mm extruded outside the joint 30 and that meniscal extrusion >4 mm outside the medial compartment leads to significantly increased tibiofemoral contact pressures. 27 On the basis of the reported healing data, biomechanical principles, and findings of this analysis, we suggest that despite the high healing rates, the repaired meniscus likely undergoes physiological changes. As a result, it may remain or become extruded after repair, reducing its effectiveness in distributing loads as compared with the native medial meniscus. Thus, further research (clinical and preclinical) is needed to better understand the relationship among root healing, meniscal extrusion, and clinical outcomes.
We acknowledge that the current analysis is not without limitations. First, the studies had variable clinical and/or radiographic follow-up (range, 5-14 years). As there is an important difference between 2- and 5-year follow-up, we also appreciate that a significant difference may exist between 5- and 14-year follow-up. Similarly, measurements of meniscal extrusion can vary in technique and timing across studies, leading to potential heterogeneity and inaccuracies. Additionally, the included studies did not include thorough descriptions of the amount of meniscus removed during PMM. As such, this cohort is likely relatively heterogeneous. Similarly, 6 of 7 repair studies utilized a transtibial pullout repair technique, while only 1 study utilized a Mason-Allen suture anchor repair technique. Therefore, we were unable to perform an analysis between the repair techniques given the limited sample size in the suture anchor repair cohort. Finally, we acknowledge that there are other potential contributing factors (eg, age, BMI, and varus alignment) that may contribute to the success of each treatment modality. While the current analysis was able to determine that there were no significant differences between treatment groups with respect to BMI and age, the studies did not contain sufficient data with respect to alignment to analyze the effects of this potentially confounding variable. Only 1 study performed simultaneous proximal tibial osteotomies with MMR, and just 1 study performed PMM in the setting of PMMRT with varus alignment (>3°).
Conclusion
This systematic review and meta-analysis of studies with >5-year minimum follow-up found that PMM was associated with a 10-fold increase in clinical failure and conversion to knee arthroplasty relative to MMR in observational studies in observational cohorts. In addition, MMR demonstrated superior Kellgren-Lawrence grades and IKDC scores as compared with PMM. The findings of the current analysis suggest that MMR is associated with superior outcomes as compared with PMM at mid- to long-term follow-up.
Footnotes
Appendix
Final revision submitted April 19, 2026; accepted April 28, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.J.K. reports the following disclosures: American Journal of Sports Medicine, editorial or governing board; Arthrex, Inc, intellectual property royalties, paid consultant; Arthroscopy Association of North America, board or committee member; International Cartilage Repair Society, board or committee member; Springer, editorial or governing board. B.R.W. reports the following disclosures: Johnson & Johnson/Depuy Orthopedic, other professional activities; Elsevier, other professional activities; Kaliber AI, stock option; Arthrex GmbH, other professional activities; Sparta, stock and other professional activities; Vericel Corporation, other professional activities; Arthroscopy, journal board of trustees, 2025-present; American Shoulder Elbow Surgeons, podcast host, technology committee; American Orthopaedic Society for Sports Medicine, council of delegates; American Orthopaedic Association, traveling fellowship committee; American Academy of Orthopaedic Surgeons, Instructional Course Lecture committee chair, board of directors or committee member; Journal of Cartilage & Joint Preservation, Video Journal of Sports Medicine, and Arthroscopy, editorial or governing board.