
Abstract
Background:
Shoulder instability and labral pathology are common in National Football League (NFL) players, yet contemporary return-to-play (RTP), return-to-performance (RTPf), and postreturn career longevity outcomes after surgical labral repair are incompletely characterized.
Purpose:
To (1) describe RTP timing and rates after surgical labral repair, (2) quantify season-to-season changes in usage and performance versus matched controls, and (3) evaluate post-RTP career longevity.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Using publicly available NFL data (2015-2024), 111 labral repair episodes were identified and indexed to surgery date. RTP was defined as the first in-game snap after surgery, with rates summarized at 2, 6, 12 and 24 months and overall (ever RTP). For RTPf, episodes required ≥100 snaps in both a preindex season (T1) and a first post-RTP season (M1); 60 cases met criteria and were matched 1:2 to 120 controls by season and position group, with additional matching on age and T1 snap rate. Changes from T1→M1 (and T1→M2 when available) were compared between groups. Outcomes included usage (games, total snaps, snaps/game) and Pro Football Focus (PFF) season grades. Career longevity post-RTP was assessed using Kaplan-Meier and stratified Cox models.
Results:
Among 111 episodes, defensive backs (25.2%) and offensive linemen (21.6%) were the most common position groups. Overall, 86.5% returned at a median 265 days (IQR, 234-316); 3.6% returned within 6 months, 73.9% within 1 year, and 84.7% within 2 years. In the matched RTPf cohort (60 cases; 120 controls), usage changes from T1→M1 did not differ (all P > .05). Offensive PFF grade trended lower versus controls (Δdiff −3.78; P = .09), while defensive PFF grade declined significantly more (Δdiff −7.13; P = .01). In the M2 subset (34 cases; 68 controls), usage and offensive PFF remained nonsignificant, whereas defensive PFF remained significantly lower (Δdiff −10.12; P = .02). Career longevity did not differ between cases and controls by log-rank or stratified Cox analyses (all P > .05).
Conclusion:
NFL players undergoing isolated labral repair demonstrated high RTP rates with preserved postreturn workload and career longevity versus matched controls. However, defensive players showed a sustained reduction in performance grades through 2 postreturn seasons, suggesting that RTP may not uniformly translate to RTPf and may vary by position.
Shoulder injuries and instability are common in the NFL, with epidemiologic studies demonstrating that >50% of NFL Combine participants exhibit radiographic or clinical shoulder pathology. 4 Rates of injury and instability vary substantially by positional demands, reflecting differences in exposure to collision forces, blocking mechanics, and tackling frequency. 2 Although labral pathology occurs across a wide range of athletic populations, the repetitive high-energy contact and joint instability inherent to American football create a distinct injury mechanism and recovery profile compared with overhead throwing athletes.9,25,26
Arthroscopic labral repair has emerged as the primary surgical intervention for symptomatic labral tears, with favorable outcomes across athletic populations.3,14,20,29 RTP rates following labral repair vary considerably by sport and procedure performed, with 68% to 100% of athletes reported to return to their prior level of competition.1,7,12,23,28 Overhead athletes, particularly baseball pitchers and tennis players, demonstrate significantly lower RTP rates (46%-79%) compared with contact and collision athletes (80%-100%).9,25 Limited data in NFL and collegiate football players suggest same-level RTP rates of approximately 93% following shoulder instability events and Bankart repair, with mean return timelines of 5 to 9 months.11,19,27 These estimates arise from heterogeneous cohorts, including mixed operative and nonoperative cases and multiple competition levels, and RTP rates alone may not reflect recovery trajectory or postreturn performance following surgery.11,19
Beyond RTP, understanding the true impact of labral repair requires examining recurrence rates, career longevity, and functional performance. Comparative studies of operative versus nonoperative management for shoulder instability across professional sports have shown that surgical intervention may reduce recurrent instability and extend career duration.11,16,28 In professional hockey, studies examining labral repair using traditional statistics (points, goals, assists, ice time) have generally shown maintained performance postoperatively,23,28 though one series noted diminished offensive production in the first year after return. 5 In the NFL, available evidence shows conflicting findings: players entering the league with preexisting labral repairs had shorter careers than those without prior shoulder surgery, 6 while studies of in-season shoulder instability suggested operative management may protect against recurrence and early retirement.11,19 To our knowledge, no study has isolated labral repair in NFL players to evaluate RTPf using objective metrics beyond participation data.
Advanced analytics have transformed performance evaluation in professional sports and expanded how postinjury outcomes can be quantified. 8 In Major League Baseball, modern advanced analytics and pitch tracking technology have revealed that players returning from labral repair often demonstrate measurable decrements in performance that traditional counting statistics miss. 13 The NFL similarly possesses comprehensive performance data, including snap-by-snap participation, advanced grading metrics by expert consensus, and position-specific efficiency measures that extend far beyond games played. 24 Despite the availability of these tools, research examining shoulder surgery outcomes in NFL players has remained confined to traditional metrics, leaving unanswered whether players truly regain their preinjury performance level or merely return to the field at diminished capacity. Therefore, the primary objective of this study is to evaluate RTP, RTPf, and career longevity following arthroscopic labral repair in NFL players using comprehensive performance analytics and position-specific metrics. Our secondary objective is to identify preoperative factors that predict successful RTPf. We hypothesize that NFL players undergoing labral repair will demonstrate high RTP rates consistent with contact athletes in other sports but will exhibit measurable decrements in performance metrics during their first 2 postoperative seasons, with recovery trajectories varying by position group.
Methods
Study Design and Data Sources
This retrospective matched-cohort study used publicly available NFL injury data from the 2015 to 2024 seasons and was determined to be not human participants research under 45 CFR 46.102; therefore, institutional review board approval was not required. All player data were sourced from the nflverse repository, 18 which included weekly injury reports, practice participation, roster details, snap counts, player demographics, and seasonal statistics. Data sets were linked via NFL Game Statistics and Information System identifiers. 18 To evaluate longer-term career outcomes, snap count and roster data from the 2012 to 2025 seasons were also incorporated. Only regular-season games were included to limit bias from differential postseason availability.
Case Identification and Episode Construction
Labral repair surgeries were identified using a multistep verification process. We first extracted all injured reserve transactions with shoulder-related injury descriptions from the Pro Sports Transactions database. 22 Each transaction was manually reviewed using targeted Google searches (eg, “[player name] shoulder surgery [year]”) to identify the reported procedure via team announcements, NFL communications, or media reports. 17 A case was included only when reporting explicitly described an isolated shoulder labral repair. Public data sources do not specify the surgical indication (eg, instability vs pain), so all confirmed isolated labral repairs were included. Reports indicating concomitant rotator cuff repair, biceps tenodesis, fracture fixation, or other concurrent shoulder procedures were excluded. To improve capture of offseason procedures and injuries not preceded by an injured reserve entry, broader searches were also performed using targeted web-based queries (eg, “NFL player labral repair [year]”), and all candidates were cross-checked against independent media sources before inclusion. 17 To maintain statistical independence, we included only 1 episode per player; for individuals with multiple identified labral repairs, the first chronological procedure was selected. Each episode was assigned an index date corresponding to the reported surgery date. RTP was recorded as the date of the player's first NFL game snap following surgery, and time to RTP was calculated in calendar days. 19 RTP rates were assessed at 2, 6, 12, and 24 months postsurgery, along with an overall “ever returned” rate.
Matched Cohort and RTPf Eligibility
A total of 111 labral repair episodes were identified. For RTPf analysis, cases were required to have ≥100 snaps both in a preinjury season (T1) and in a qualifying postoperative season (M1), defined as the first season after return in which the player logged ≥100 snaps. This 100-snap threshold was selected a priori to represent participation across multiple games and to reduce instability in performance comparisons attributable to very limited playing time. Overall, 60 cases met RTPf eligibility criteria, whereas 15 never returned to play, 30 did not have a qualifying T1 season with ≥100 snaps, and 6 returned but did not reach 100 snaps in M1. Each eligible case was matched 1:2 to controls who were active during the case's index season and matched exactly on season and primary position group; case players were excluded from the control pool. From the remaining candidates (all other NFL players active during the index season who met matching criteria and were not cases), controls were selected without replacement, prioritizing age (±2 years, widening sequentially to ±4 and ±6 years) and minimizing the absolute difference in preindex snap rate (snaps per game). When multiple eligible control pairs were available, the pair with the smallest absolute difference in T1 snap rate was selected. Covariate balance was assessed using standardized mean differences (SMDs).
Performance and Longevity Metrics
All performance and usage metrics were based on regular-season data. Position groups were categorized as quarterback (QB), running back (RB), wide receiver (WR), tight end (TE), offensive line (OL), defensive line (DL), linebacker (LB), and defensive back (DB). 18 Usage was measured by games played, total snaps, and snap rate. Our primary tool for evaluating postinjury performance was season-level Pro Football Focus (PFF) grades, an independently generated football analytics measure accessed through the online PFF platform. 21 Unlike traditional box-score statistics, which capture only outcomes (eg, yards, touchdowns), PFF grades are derived from expert film analysis in which trained evaluators assess every snap, assigning a performance score based on execution, technique, and assignment. 21 These play-level scores are aggregated and normalized into a 0 to 100 season grade for each player, with a grade of 60 representing NFL mean performance. 21 This method allows for a more complete and position-neutral measure of true performance, especially valuable for roles like OLs, whose impact is poorly reflected in traditional statistics. For this study, offensive players were evaluated using the PFF overall offense grade, and defensive players using the PFF overall defense grade. PFF performance was the primary analysis for RTPf. Secondarily, position-specific performance metrics and grades (eg, QB accuracy, RB rush grade, blocking grades for OL) were also explored and reported as supplementary analyses given relatively small sample sizes. Career longevity was measured from the RTP date to the date of the final recorded snap. Players on an active roster in week 15 of 2025 were right-censored. Longevity outcomes included (1) games played after RTP, (2) total snaps after RTP, and (3) calendar years from RTP to final game.
Statistical Analysis
Descriptive statistics were reported for all cases and the matched cohort. Continuous variables are presented as mean ± SD, categorical variables as percentages. In matched analyses, RTPf was calculated as within-player change from T1 to M1; for each case, this individual change was compared with the mean change of its 2 matched controls. Between-group differences in change were assessed using paired comparisons within matched sets (case change vs mean control change). Within-player change from T1 to the second qualifying post-RTP season (M2) was also analyzed using the same matched framework (34 cases; 68 matched controls); position-specific stratification at M2 was not performed because of limited sample size. Career longevity was compared using Kaplan-Meier curves with log-rank tests and stratified Cox proportional hazards models (stratified by matched set). Adjusted Cox models included preindex career games as a covariate. All analyses were performed in R (Version 4.3.2; R Foundation for Statistical Computing) with the data.table, survival, survminer, flextable, and officer packages. A 2-sided alpha of .05 was used without multiplicity adjustment, consistent with the study's exploratory design.
Results
A total of 111 labral repair episodes were identified. Mean age at index surgery was 25.53 ± 3.18 years, with mean height 189.47 ± 6.82 cm, weight 112.18 ± 20.91 kg, and body mass index (BMI) of 31.06 ± 4.28 (Table 1). Position distribution was highest among DB (25.2%) and OL (21.6%), followed by LB (14.4%), DL (10.8%), WR (9.0%), QB (8.1%), TE (5.4%), RB (3.6%), and special teams (SPEC) (1.8%) (Table 1). For RTPf analyses, 60 labral repair cases were successfully matched 1:2 to 120 controls (Table 2). Baseline covariates were well-balanced across groups (all SMDs <0.10), including age, BMI, T1 snap rate, total snaps, and games played. A small residual imbalance was observed for height (190.50 ± 6.68 vs 188.74 ± 6.41 cm; SMD, 0.268). Matching preserved identical distributions of primary position groups across cases and controls (Table 2).
Baseline Characteristics of All Labral Repair Episodes a
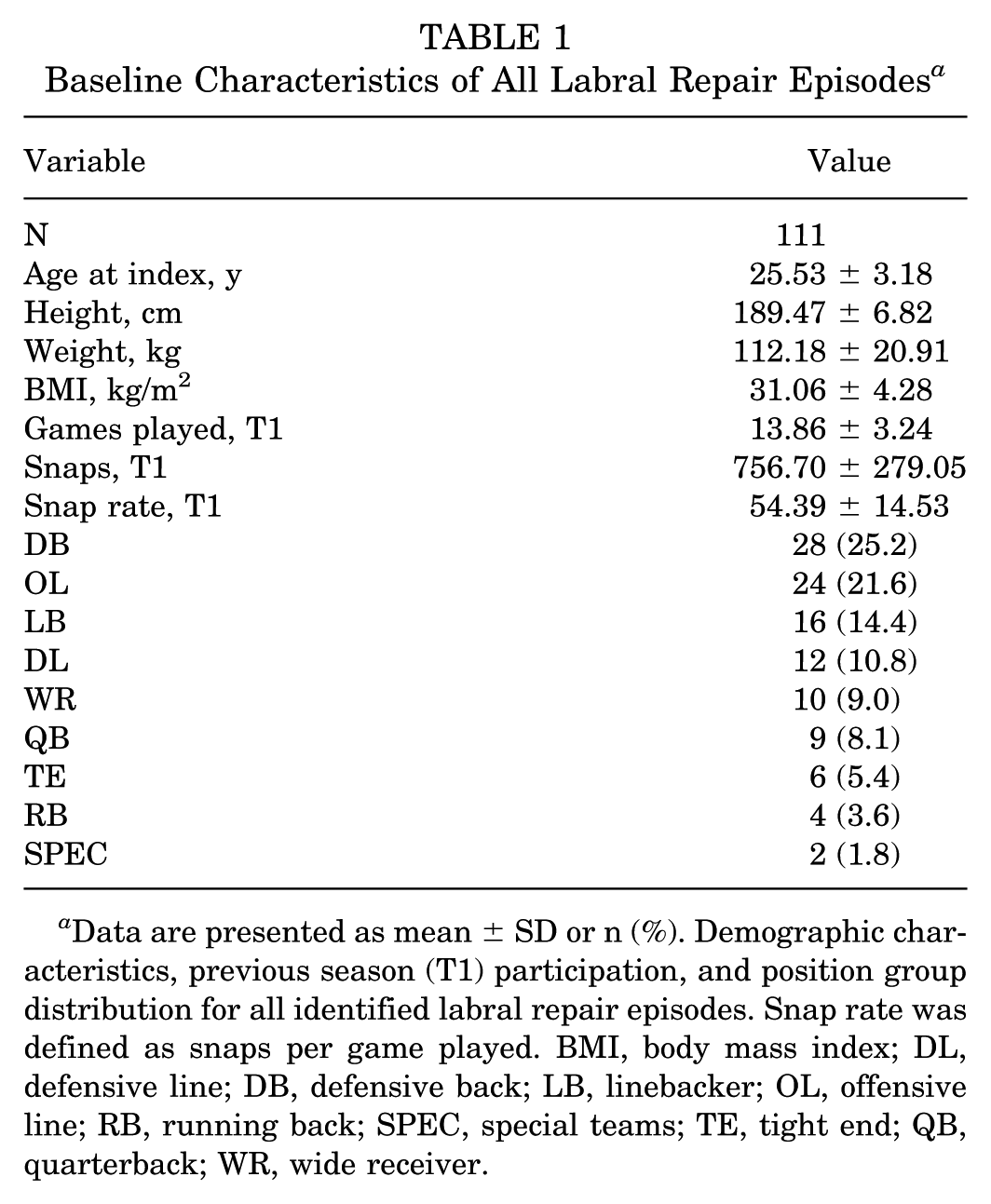
Data are presented as mean ± SD or n (%). Demographic characteristics, previous season (T1) participation, and position group distribution for all identified labral repair episodes. Snap rate was defined as snaps per game played. BMI, body mass index; DL, defensive line; DB, defensive back; LB, linebacker; OL, offensive line; RB, running back; SPEC, special teams; TE, tight end; QB, quarterback; WR, wide receiver.
Baseline Characteristics of Matched Labral Repair Cases and Controls a
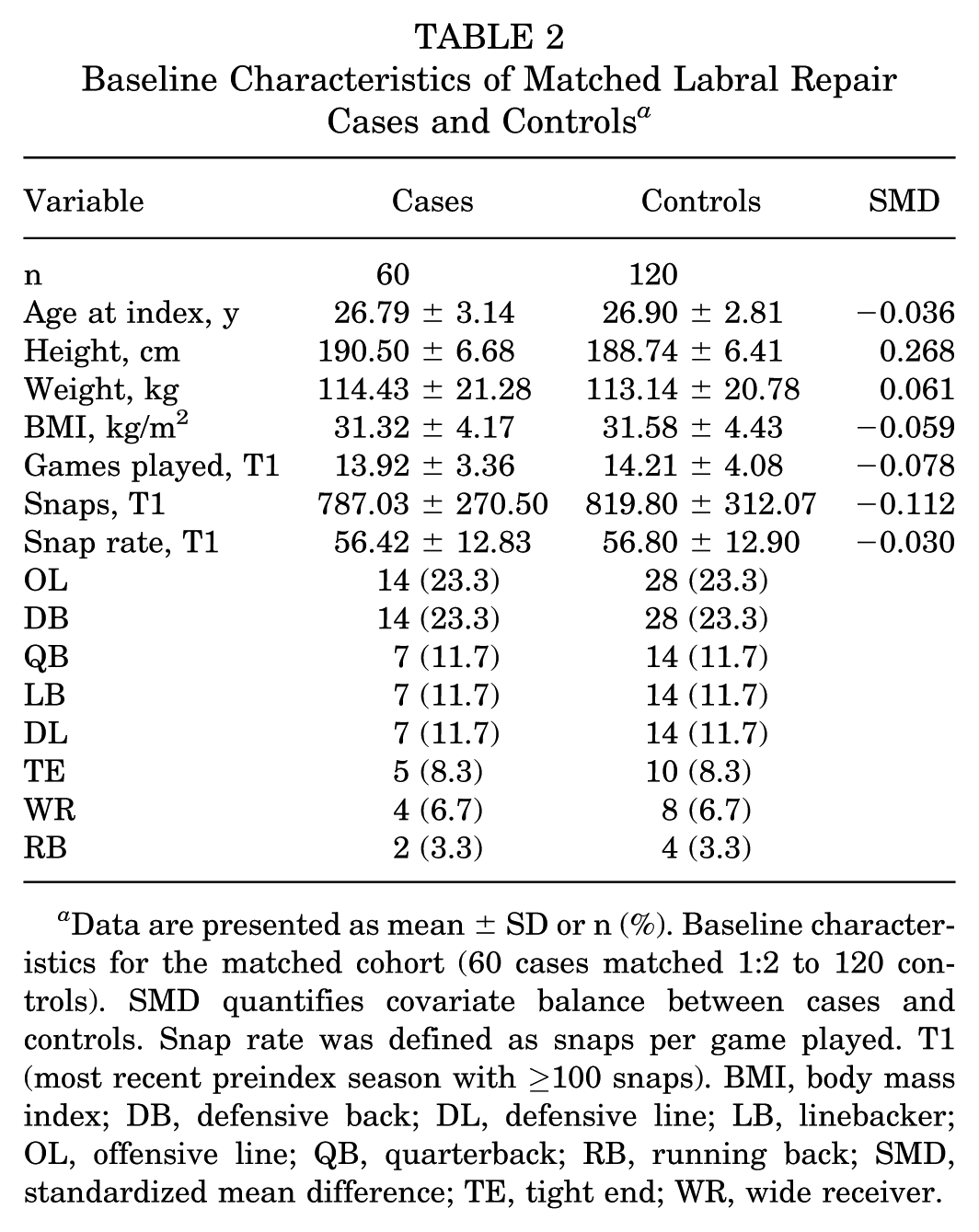
Data are presented as mean ± SD or n (%). Baseline characteristics for the matched cohort (60 cases matched 1:2 to 120 controls). SMD quantifies covariate balance between cases and controls. Snap rate was defined as snaps per game played. T1 (most recent preindex season with ≥100 snaps). BMI, body mass index; DB, defensive back; DL, defensive line; LB, linebacker; OL, offensive line; QB, quarterback; RB, running back; SMD, standardized mean difference; TE, tight end; WR, wide receiver.
RTP outcomes for all 111 episodes are summarized in Table 3. Overall, 96 players (86.5%) returned to NFL play following surgery. No players returned within 2 months (0%); 3.6% returned within 6 months, 73.9% within 1 year, and 84.7% within 2 years. Median time to RTP was 265 days (IQR, 234-316). RTP patterns were generally consistent across position groups, although small subgroup sizes limited inference for some categories. RTP was highest in QB (100%), TE (100%), and RB (100%), while rates were 89.3% in DB, 83.3% in OL, 83.3% in DL, 81.2% in LB, 80.0% in WR, and 50.0% in SPEC. Median days to RTP varied by position group, ranging from 239 days in QB (IQR, 228-293) and 242 days in LB (IQR, 212-272) to 286 days in TE (IQR, 219-356) and 312 days in SPEC (single returning player).
RTP by Position Group a
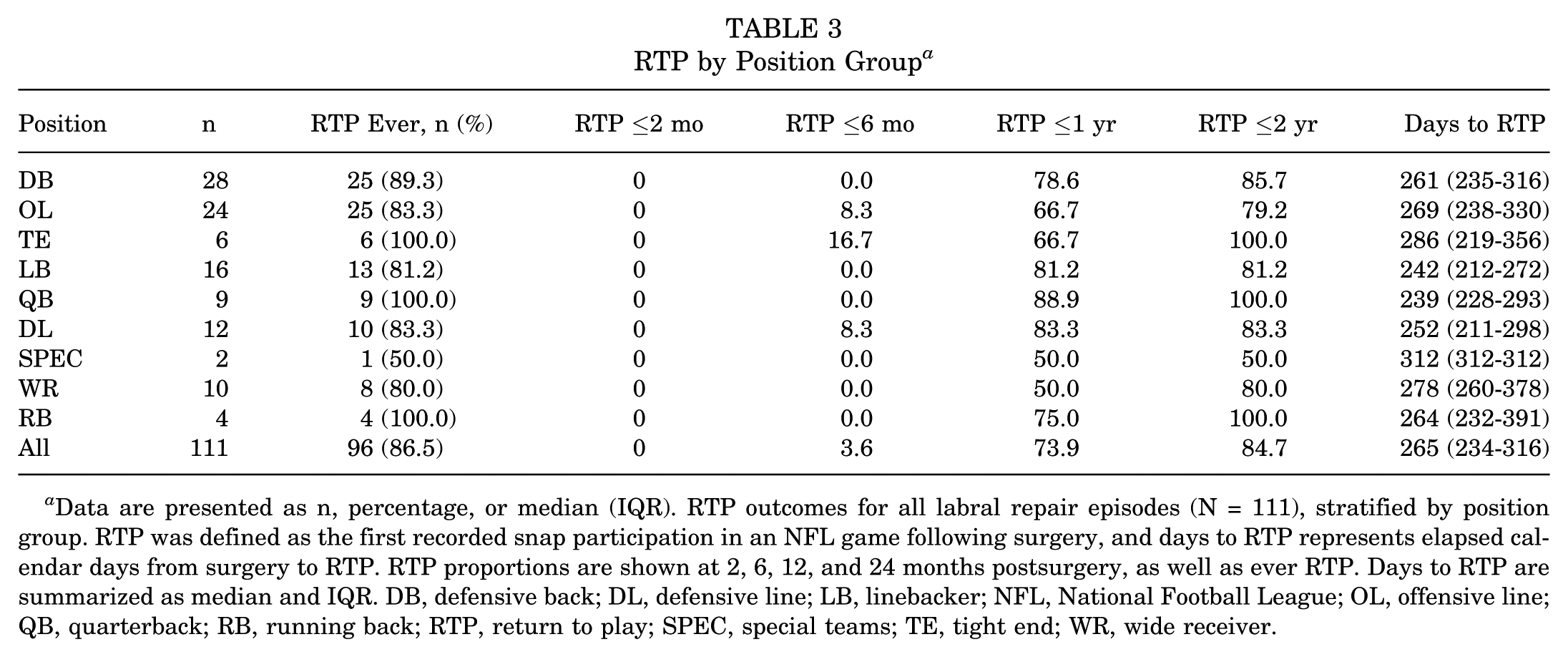
Data are presented as n, percentage, or median (IQR). RTP outcomes for all labral repair episodes (N = 111), stratified by position group. RTP was defined as the first recorded snap participation in an NFL game following surgery, and days to RTP represents elapsed calendar days from surgery to RTP. RTP proportions are shown at 2, 6, 12, and 24 months postsurgery, as well as ever RTP. Days to RTP are summarized as median and IQR. DB, defensive back; DL, defensive line; LB, linebacker; NFL, National Football League; OL, offensive line; QB, quarterback; RB, running back; RTP, return to play; SPEC, special teams; TE, tight end; WR, wide receiver.
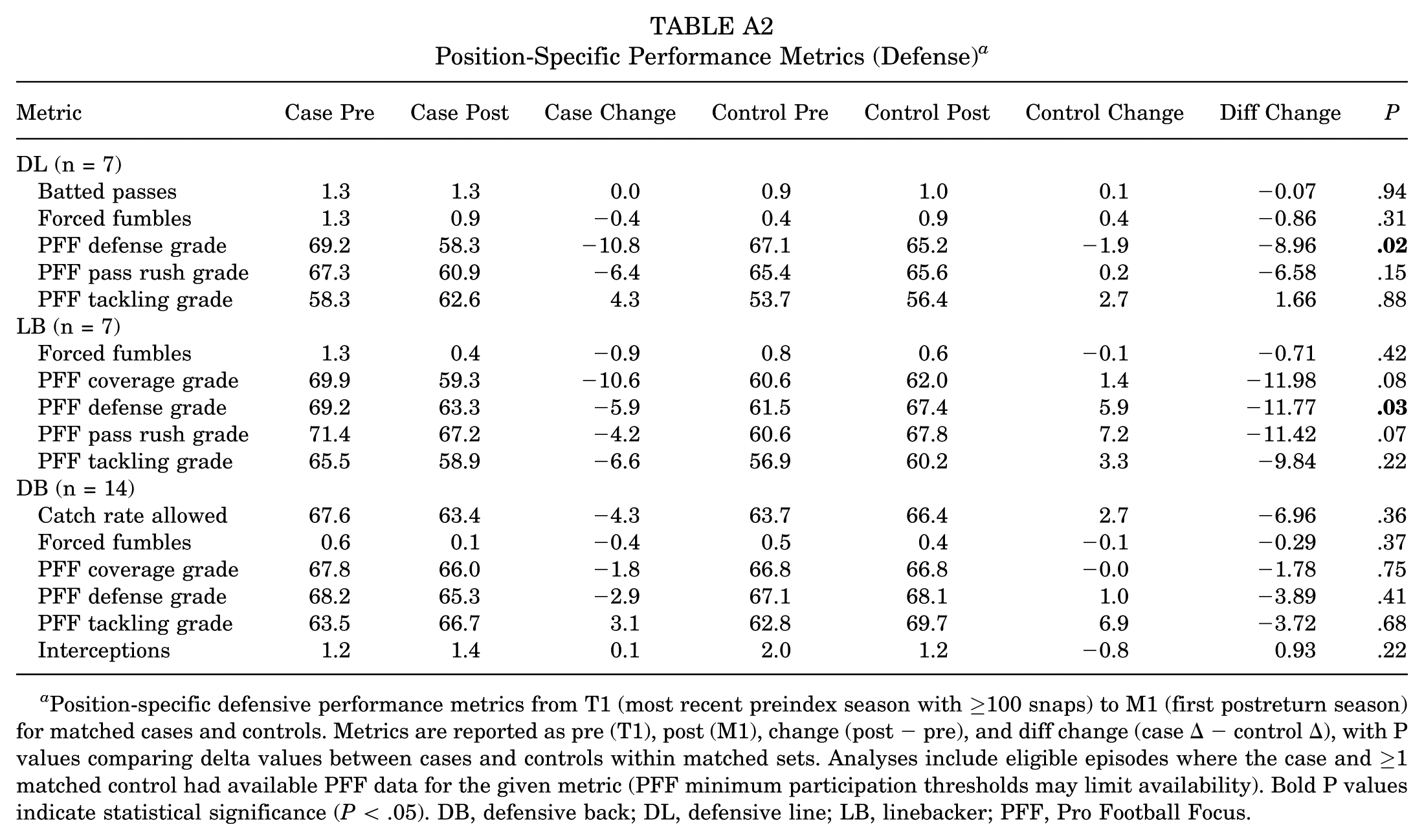
In the matched RTPf cohort, there were no between-group differences in T1 to M1 change for games played, total snaps, or snaps/game (Table 4). Among offensive players (n = 32), cases showed a larger decline in PFF offense grade than controls, but this did not reach significance (Δdiff, −3.78; P = .09). Among defensive players (n = 28), cases demonstrated a significantly greater decline in PFF defense grade versus controls (Δdiff, −7.13; P = .01). In the M2 subset (34 cases; 68 controls), between-group differences remained nonsignificant for usage metrics and for PFF offense grade (Δdiff, −1.29; P = .74), while PFF defense grade again declined significantly more in cases (Δdiff, −10.12; P = .02). Position-specific results are provided in AppendixTables A1 and A2; most comparisons were nonsignificant, with the main exceptions being significant declines in overall PFF defense grade among DLs (Δdiff, −8.96; P = .02) and LBs (Δdiff, −11.77; P = .03).
Changes in Usage, Production, and Overall PFF Grades From T1 to M1 and M2 in the Matched RTPf Cohort a
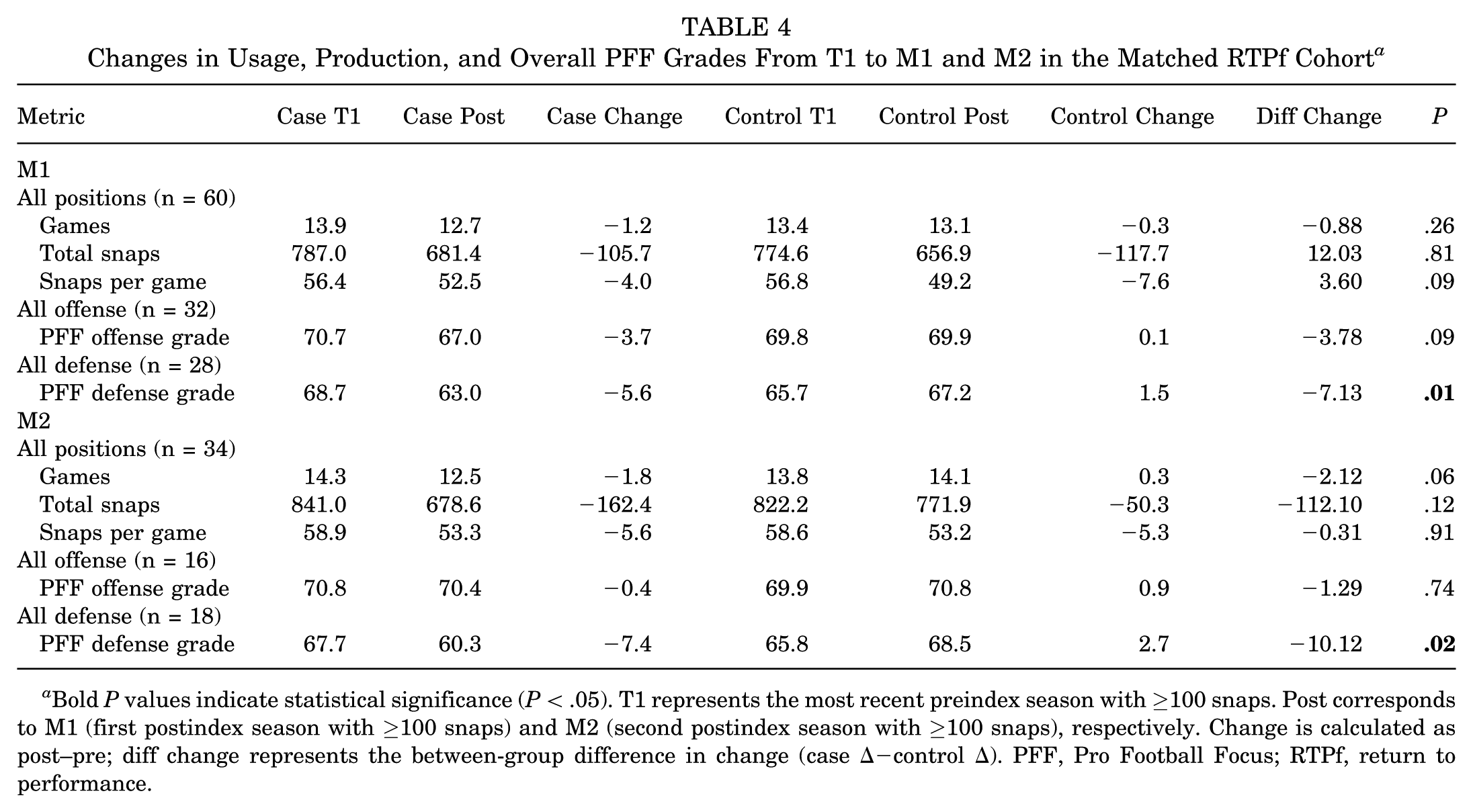
Bold P values indicate statistical significance (P < .05). T1 represents the most recent preindex season with ≥100 snaps. Post corresponds to M1 (first postindex season with ≥100 snaps) and M2 (second postindex season with ≥100 snaps), respectively. Change is calculated as post–pre; diff change represents the between-group difference in change (case Δ−control Δ). PFF, Pro Football Focus; RTPf, return to performance.
Kaplan-Meier analysis was performed to assess post-RTP career longevity (Figure 1). Log-rank tests comparing cases and controls showed no significant differences in career duration, whether measured in years (P = .32), games (P = .39), or snaps (P = .57). These results were confirmed using stratified Cox proportional hazards regression (Table 5). The unadjusted models demonstrated no significant association between labral repair and the hazard of career end for years remaining (hazard ratio [HR], 1.22; P = .42), games remaining (HR, 1.16; P = .57), or snaps remaining (HR, 1.08; P = .76). After adjusting for preindex career games, the findings remained nonsignificant (Table 5).
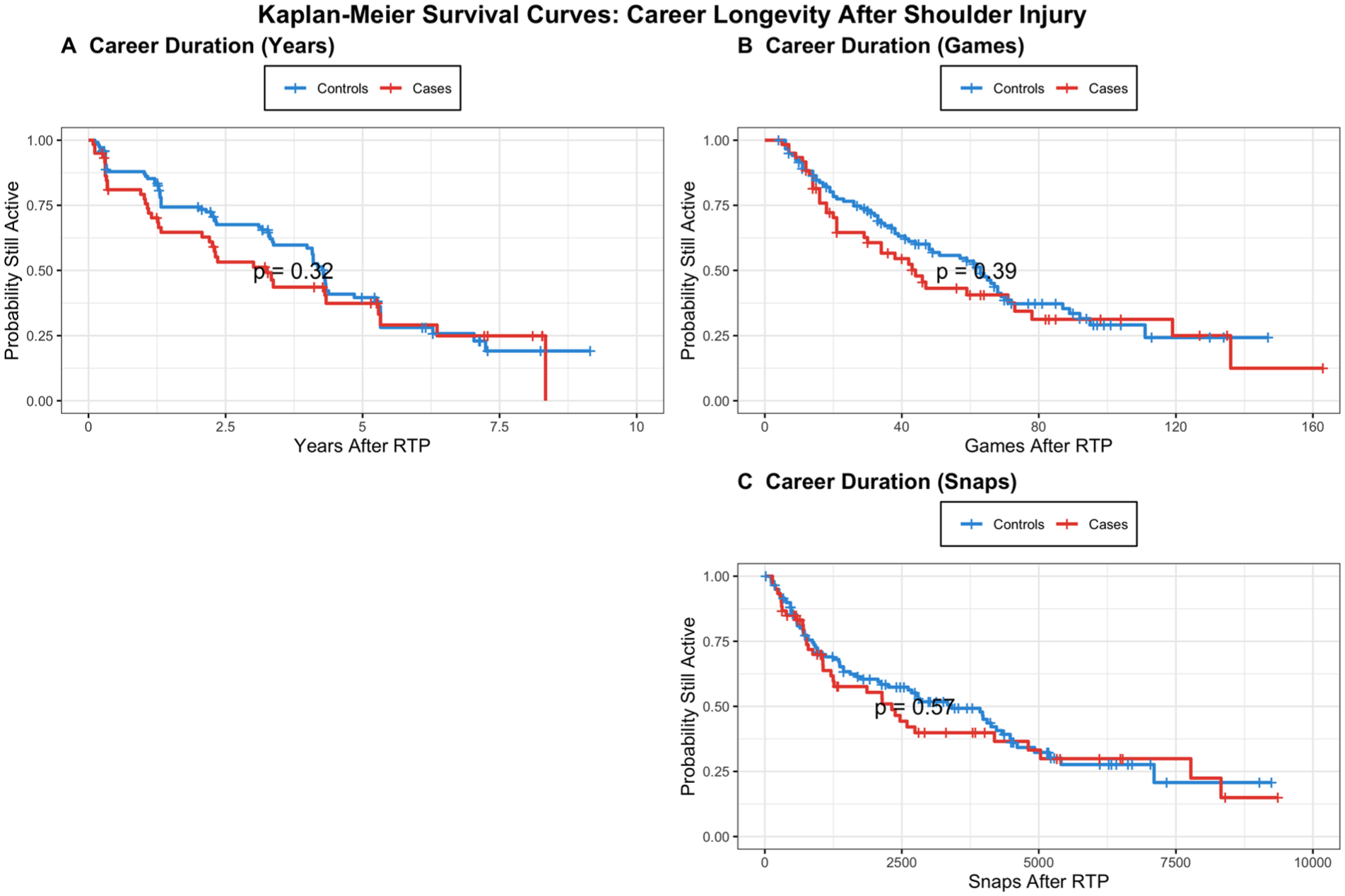
Kaplan-Meier curves compare cases versus matched controls (60 cases matched 1:2 to 120 controls) using 3 complementary post–RTP longevity metrics: (A) calendar years after RTP, (B) games after RTP, and (C) snaps after RTP. Follow-up for both cases and controls began on the case's RTP date (RTP defined as first in-game snap participation after surgery). Career termination (event) was defined as the date of final recorded snap participation. Log-rank P values are shown for each panel. RTP, return to play.
Cox Regression: Career Longevity After RTP (All Matched Pairs, Stratified by Episode) a
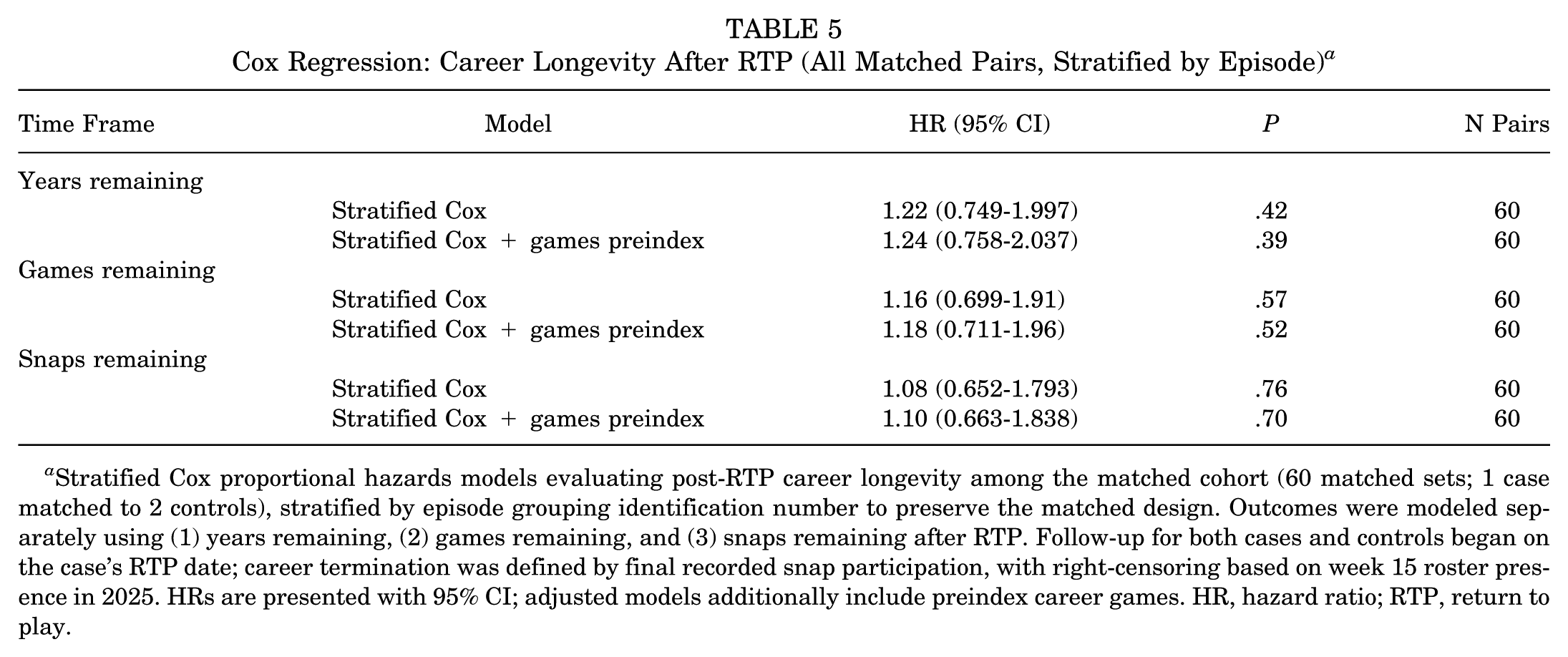
Stratified Cox proportional hazards models evaluating post-RTP career longevity among the matched cohort (60 matched sets; 1 case matched to 2 controls), stratified by episode grouping identification number to preserve the matched design. Outcomes were modeled separately using (1) years remaining, (2) games remaining, and (3) snaps remaining after RTP. Follow-up for both cases and controls began on the case's RTP date; career termination was defined by final recorded snap participation, with right-censoring based on week 15 roster presence in 2025. HRs are presented with 95% CI; adjusted models additionally include preindex career games. HR, hazard ratio; RTP, return to play.
Discussion
The primary findings of this study indicate that while NFL players undergoing labral repair achieve high rates of RTP and preserve career longevity, meaningful performance declines persist following surgery, most consistently among defensive players. Overall, 86.5% of players returned to NFL competition, with the majority doing so between 8 and 12 months postoperatively. Players who returned demonstrated usage patterns comparable with their preinjury baseline, with no significant differences in games played, total snaps, or snap rate when compared with matched controls. In the first postreturn season, both offensive and defensive players demonstrated lower PFF grades relative to matched controls, although only the defensive cohort reached statistical significance. By the second postreturn season, offensive grades were no longer different from controls, whereas defensive grades remained significantly lower, suggesting a more persistent performance impact among defensive players. Career longevity, measured in years, games, and snaps following return, did not differ between surgical cases and matched controls. Together, these findings challenge the prevailing assumption that successful RTP reflects full restoration of performance quality and underscore the critical distinction between participation and functional recovery following labral repair.
Position-dependent differences in postreturn performance may reflect both the distribution of injury mechanisms across positions and the shoulder demands required to play effectively after stabilization. Notably, OLs and DBs represented the largest share of labral repair episodes in this cohort, consistent with prior reports that these positions account for the highest proportions of shoulder instability episodes in the NFL.2,6 In contrast, the observed performance signal was more evident on the defensive side, where PFF grades declined relative to controls in the first postreturn season and remained lower into the second season. One possible explanation is that defensive roles require repetitive high-impact shoulder involvement, particularly tackling, block engagement, and collision absorption, such that even modest residual weakness, stiffness, or apprehension after repair may translate into measurable decrements despite preserved participation. Together, these findings suggest that return status alone may underestimate functional recovery, and that postreturn performance may be more sensitive to role-specific shoulder demands.
Despite measurable performance changes, we found no significant difference in career longevity between players undergoing labral repair and matched controls when assessed by post–RTP years, games, or snaps, suggesting that performance decline does not necessarily translate to shortened NFL careers. Prior NFL studies have reported variable findings: Khalil et al 11 demonstrated longer careers following operative management compared with nonoperative treatment for shoulder instability, whereas Chambers et al 6 reported shorter career duration among players entering the league with preexisting superior labral anterior-posterior repairs. Murphy et al15,16 similarly found no reduction, and in some cases greater usage, among combine participants with prior anterior or posterior labral repair at 2 years postdraft. These discrepancies likely reflect differences in injury timing and cohort composition, as players sustaining shoulder injuries after establishing themselves in the NFL may benefit from greater organizational investment and roster security than those entering the league with preexisting pathology. Our findings add to this heterogeneous body of literature by demonstrating preserved career longevity following labral repair when compared with rigorously matched controls, even in the presence of performance decrements. Similar variability has been reported in other professional sports, with Castle et al 5 identifying shorter careers after labral repair in National Hockey League players, while Swindell et al 28 suggested that operative management may preserve career length by reducing recurrence and missed time compared with nonoperative treatment.
Our observed RTP rate of 86.5% aligns with prior reports in elite contact athletes and exceeds rates reported in systematic reviews of mixed athletic populations, which have generally demonstrated return to preinjury levels ranging from 63% to 78% following labral repair.1,7,25 This disparity likely reflects fundamental differences between heterogeneous cohorts included in systematic reviews and the uniquely elite nature of NFL athletes, who represent a highly selected population with exceptional baseline physical capacity, access to specialized surgical care, and extensive rehabilitation resources. Within the American football–specific literature, our findings are consistent with those of Saper et al, 27 who reported a 93% return to the collegiate/NFL level following Bankart repair, as well as broader studies of shoulder instability in NFL players reporting return rates ~93%, although these studies did not stratify outcomes by treatment modality.11,19 While our median return timeline of 265 days falls within previously reported NFL ranges,11,19 it is longer than timelines reported in professional hockey 23 and basketball 12 (approximately 130 days), a difference that likely reflects sport-specific and positional demands rather than inferior outcomes. RTP timing may also be influenced by season-calendar considerations, as some players may elect surgery at a point that optimizes availability for the subsequent season rather than reflecting recovery time alone. Collectively, the high rates of successful same-level return observed across professional sport cohorts likely reflect access to advanced, multidisciplinary support systems that promote high-quality recovery and highlight the potential value of advanced rehabilitation approaches for optimizing recovery in athletic populations more broadly. 10
In summary, labral repair in NFL players appears to be highly effective in facilitating RTP at the highest level of professional football, with high return rates, preserved career longevity, and sustained participation despite position-dependent performance changes. These findings support operative stabilization as a reliable option for elite athletes whose careers depend on shoulder stability and durability under contact. However, the sustained performance declines among defensive players highlight the importance of accounting for position-specific biomechanical and psychological demands during recovery. Defensive athletes may experience greater functional consequences from residual weakness or apprehension, warranting more individualized rehabilitation strategies and potentially extended recovery timelines to ensure both physical readiness and confidence at the point of contact. Collectively, these results emphasize that successful outcomes following labral repair in NFL players are best achieved through a position-aware, multidisciplinary approach that prioritizes safe and confident return to elite-level performance rather than expedited clearance alone.
Limitations
This study is not without limitations. First, the analysis relied on publicly available injury and roster data, which precluded confirmation of diagnosis and surgical details including the specific indication for surgery (eg, instability vs pain) and prevented characterization of clinically important factors such as tear location, pattern, degree of glenoid bone loss, and fixation constructs (eg, number/type of anchors or screws). Second, surgery dates and clinical recovery milestones were not directly observable; although indexing was performed to the reported surgery date and RTP was defined objectively as first in-game snap, misclassification of timing and heterogeneity in injury chronicity may persist. Third, postoperative care is likely not standardized across the NFL; and team medical staffs, rehabilitation resources, and return-to-competition criteria may vary across teams, potentially influencing both RTP timing and postreturn performance. Fourth, performance outcomes (including PFF grades) are composite, context-dependent metrics that may be influenced by scheme, coaching changes, role adjustments, and concurrent injuries; accordingly, we cannot exclude that some observed performance declines reflect postinjury role modification or changes in utilization rather than isolated physiologic limitation attributable to surgery. Finally, the RTPf cohort required ≥100 snaps in both T1 and M1, which may select for healthier, more established players and limit generalizability to fringe roster players or special teams–only contributors.
Conclusion
NFL players undergoing isolated labral repair demonstrated high RTP rates with preserved postreturn participation and career longevity versus matched controls. However, defensive players showed a sustained reduction in performance grades through 2 postreturn seasons, suggesting that RTP may not uniformly translate to RTPf and may vary by position.
Footnotes
Appendix
Position-Specific Performance Metrics (Defense) a
| Metric | Case Pre | Case Post | Case Change | Control Pre | Control Post | Control Change | Diff Change | P |
|---|---|---|---|---|---|---|---|---|
| DL (n = 7) | ||||||||
| Batted passes | 1.3 | 1.3 | 0.0 | 0.9 | 1.0 | 0.1 | −0.07 | .94 |
| Forced fumbles | 1.3 | 0.9 | −0.4 | 0.4 | 0.9 | 0.4 | −0.86 | .31 |
| PFF defense grade | 69.2 | 58.3 | −10.8 | 67.1 | 65.2 | −1.9 | −8.96 |
|
| PFF pass rush grade | 67.3 | 60.9 | −6.4 | 65.4 | 65.6 | 0.2 | −6.58 | .15 |
| PFF tackling grade | 58.3 | 62.6 | 4.3 | 53.7 | 56.4 | 2.7 | 1.66 | .88 |
| LB (n = 7) | ||||||||
| Forced fumbles | 1.3 | 0.4 | −0.9 | 0.8 | 0.6 | −0.1 | −0.71 | .42 |
| PFF coverage grade | 69.9 | 59.3 | −10.6 | 60.6 | 62.0 | 1.4 | −11.98 | .08 |
| PFF defense grade | 69.2 | 63.3 | −5.9 | 61.5 | 67.4 | 5.9 | −11.77 |
|
| PFF pass rush grade | 71.4 | 67.2 | −4.2 | 60.6 | 67.8 | 7.2 | −11.42 | .07 |
| PFF tackling grade | 65.5 | 58.9 | −6.6 | 56.9 | 60.2 | 3.3 | −9.84 | .22 |
| DB (n = 14) | ||||||||
| Catch rate allowed | 67.6 | 63.4 | −4.3 | 63.7 | 66.4 | 2.7 | −6.96 | .36 |
| Forced fumbles | 0.6 | 0.1 | −0.4 | 0.5 | 0.4 | −0.1 | −0.29 | .37 |
| PFF coverage grade | 67.8 | 66.0 | −1.8 | 66.8 | 66.8 | −0.0 | −1.78 | .75 |
| PFF defense grade | 68.2 | 65.3 | −2.9 | 67.1 | 68.1 | 1.0 | −3.89 | .41 |
| PFF tackling grade | 63.5 | 66.7 | 3.1 | 62.8 | 69.7 | 6.9 | −3.72 | .68 |
| Interceptions | 1.2 | 1.4 | 0.1 | 2.0 | 1.2 | −0.8 | 0.93 | .22 |
Position-specific defensive performance metrics from T1 (most recent preindex season with ≥100 snaps) to M1 (first postreturn season) for matched cases and controls. Metrics are reported as pre (T1), post (M1), change (post − pre), and diff change (case Δ− control Δ), with P values comparing delta values between cases and controls within matched sets. Analyses include eligible episodes where the case and ≥1 matched control had available PFF data for the given metric (PFF minimum participation thresholds may limit availability). Bold P values indicate statistical significance (P < .05). DB, defensive back; DL, defensive line; LB, linebacker; PFF, Pro Football Focus.
Acknowledgements
The authors would like to thank the nflverse project and its contributors for making professional football data publicly accessible through their open-source ecosystem, which made this study possible.
Final revision submitted April 12, 2026; accepted April 28, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.N.L. receives consulting fees and royalties from Zimmer Biomet. C.M.J. is a paid consultant for Smith & Nephew. C.S.A. receives royalties and research support from Arthrex, research support from Major League Baseball and Stryker, and consulting fees from Arthrex.
Ethical approval was not sought for the present study.