
Abstract
Background:
High tibial osteotomy (HTO) realigns the mechanical axis and reduces medial compartment overload in knee osteoarthritis. Microfracture (MFx) is often added to stimulate cartilage repair, yet whether MFx provides additional clinical benefit in the degenerative osteoarthritic environment remains uncertain. Emerging evidence suggests that structural cartilage changes do not consistently correlate with symptoms, raising the possibility of structure-symptom discordance.
Purpose/Hypothesis:
The purpose of this study was to evaluate whether MFx performed during HTO improves cartilage regeneration and postoperative patient-reported outcomes and to determine whether structural improvement corresponds with symptomatic benefit. It was hypothesized that MFx would enhance cartilage regeneration and lead to superior clinical outcomes compared with HTO alone.
Study Design:
Cohort study; Level of evidence 3.
Methods:
A total of 62 patients who underwent navigation-assisted medial opening-wedge HTO with second-look arthroscopy at 2 years were included. Patients were categorized into 2 groups: HTO alone (group 1; n = 30) and HTO with MFx for well-shouldered focal defects (group 2; n = 32). Cartilage status was graded using the International Cartilage Regeneration & Joint Preservation Society (ICRS) system, and improvement was defined as a decrease in grade. Clinical outcomes were assessed at 2 years using the International Knee Documentation Committee (IKDC) subjective score. Group comparisons, correlation analyses, and multivariable linear regression were performed to determine independent predictors of postoperative IKDC score.
Results:
Cartilage improvement occurred in 33.3% of group 1 and 62.5% of group 2 (P = .04). In the MFx group, patients achieving low-grade postoperative lesions (ICRS 1-2) had significantly smaller initial defects (2.0 vs 6.0 cm2; P < .01). Despite better structural improvement, no significant between-group difference in 2-year IKDC score was found (55.2 vs 50.6; P = .26). MFx was identified as an independent negative predictor of postoperative IKDC score (β = −14.4; P = .01). Changes in cartilage status (ΔICRS) were not correlated with symptomatic improvement (ΔIKDC; ρ = −0.18; P = .14), demonstrating a structure-symptom discordance.
Conclusion:
MFx performed during HTO improved cartilage morphology but did not yield superior clinical outcomes. MFx was associated with significantly lower adjusted IKDC scores, and structural improvement did not correlate with symptomatic benefit.
In medial compartment osteoarthritis (OA), high tibial osteotomy (HTO) realigns the mechanical axis transferring weightbearing load from the medial to the lateral compartment. 19 This biomechanical correction decreases excessive compressive forces and improves the metabolic imbalance between anabolic and catabolic activities within the knee joint. 1 Through this rebalancing mechanism, HTO alleviates symptoms and slows disease progression, making it an effective joint-preserving option for early- to midstage OA. Unlike arthroplasty, which replaces the degenerated joint, HTO modulates the rate of OA progression and delays the need for joint replacement. 35 The reported 10-year survival rate of HTO ranges from 74.7% to 97.6%, and the procedure has been widely recognized as an effective surgical option for improving symptoms in medial compartment OA. 19
Chondral lesions of the medial femoral condyle (MFC) are frequently encountered during HTO,2,43 the optimal management of these cartilage defects remains unclear. Some studies reported cartilage regeneration after HTO alone, with improvement observed in 44.6% to 62.1% of patients,21,29,30 whereas others found no clinical difference between HTO alone and HTO combined with microfracture (MFx).28,40 Quantitative magnetic resonance imaging (MRI) assessments such as T2 mapping and magnetic resonance observation of cartilage repair tissue scoring have shown that regenerated tissue after MFx did not achieve the same structural or compositional quality as native hyaline cartilage. 16 These findings have raised concerns regarding whether MFx, which induces fibrous rather than hyaline cartilage healing, provides any meaningful benefit when combined with HTO.
Conversely, other investigations reported that performing MFx concurrently with HTO not only improved clinical outcomes but also resulted in superior cartilage regeneration, which was observed in 50% to 85% of patients.3,39 Furthermore, some suggested that cartilage regeneration after HTO correlated with symptom improvement.3,50 These inconsistent findings highlight ongoing uncertainty regarding whether MFx provides additive benefit during HTO.
Therefore, this study aimed to determine whether performing MFx concurrently with HTO improves cartilage regeneration and postoperative clinical outcomes. Demographic, radiologic, and arthroscopic factors potentially influencing postoperative outcomes were analyzed, and multiple regression analysis was conducted to adjust for confounding variables and to evaluate the independent effect of MFx on clinical results. The hypothesis of this study was that performing MFx at the time of HTO would enhance better cartilage regeneration and superior postoperative clinical outcomes compared with HTO alone.
Methods
Study Design
This study evaluated whether performing MFx concurrently with HTO provides additional benefit in cartilage regeneration and postoperative clinical outcomes. Patients who underwent HTO followed by second-look arthroscopy between September 2010 and April 2020 were retrospectively reviewed. Only patients with a concomitant International Cartilage Regeneration & Joint Preservation Society (ICRS) grade 4 lesion of the MFC at the time of HTO were eligible for inclusion. Of 119 initially screened patients, exclusions were lack of 2-year radiographs (n = 2), missing clinical scores (n = 20), concomitant procedures other than MFx (OAT, ACI, enhanced MFx, stem cell therapy, or meniscal repair; n = 11), and initial MFC lesions classified as ICRS grades 1 to 3 at the time of HTO (n = 24). A total of 62 patients were included (Figure 1). HTO was performed in patients with symptomatic medial compartment osteoarthritis and varus malalignment in the absence of progressive degenerative changes in the lateral compartment. Chondral lesions in the patellofemoral joint were not used as an exclusion criterion.
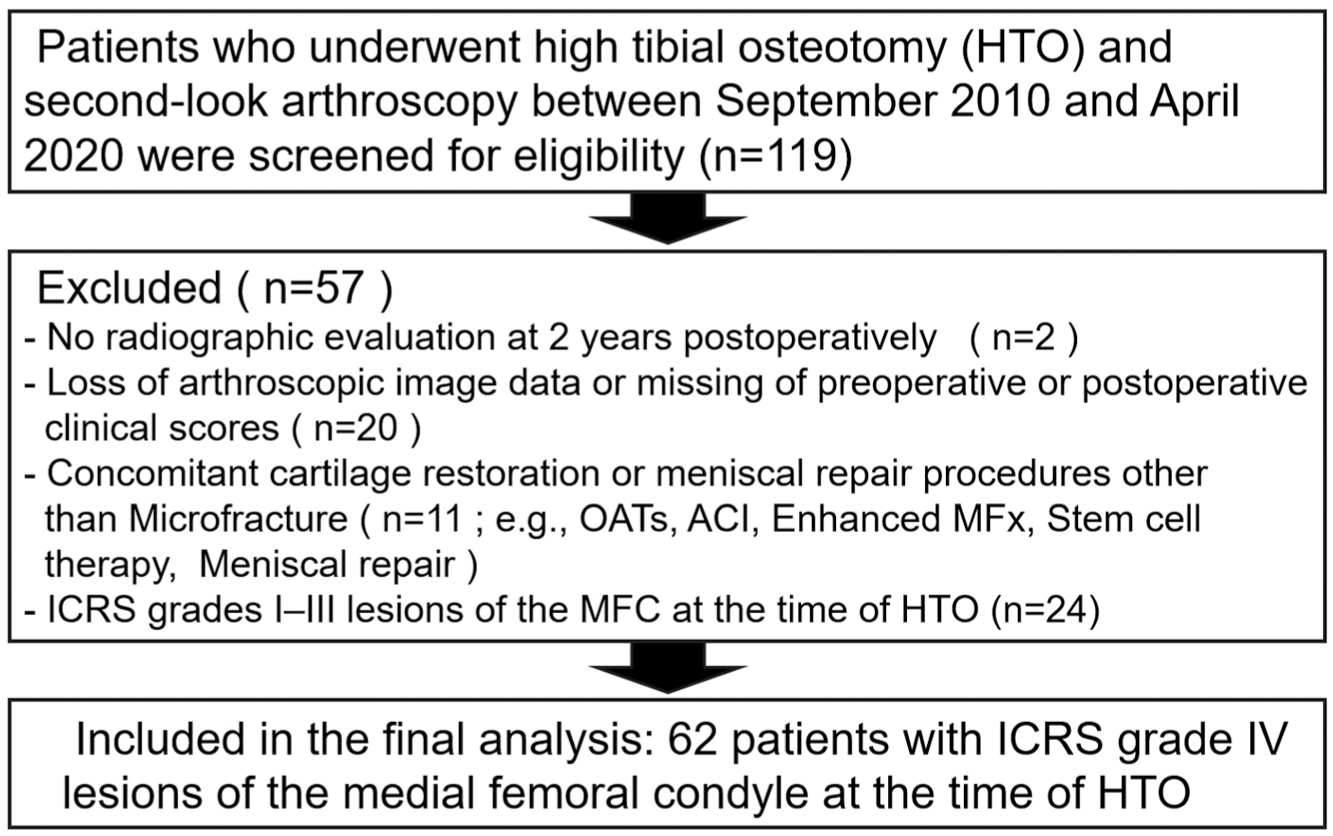
Flowchart showing patient enrollment and exclusion. ACI, autologous chondrocyte implantation; HTO, high tibial osteotomy; ICRS, International Cartilage Regeneration & Joint Preservation Society; MFC, medial femoral condyle; MFx, microfracture; OATS, osteochondral autograft transfer system.
Patient Evaluation
To identify factors that could potentially influence cartilage status and clinical outcomes, patients were categorized into 3 major groups for analysis.
(1) Patient factors: age and body mass index (BMI) were evaluated.
(2) Arthroscopic findings at the time of HTO: based on intraoperative arthroscopic evaluation, the size of the MFC chondral lesion, the presence of a kissing lesion, the degree of medial meniscal hoop tension loss, and whether MFx was performed were assessed. Hoop tension loss was determined by identifying medial meniscal degenerative complex tears, radial tears, or root tears that could compromise meniscal hoop tension. The location of meniscal damage was recorded according to the Cooper classification, and the extent of hoop tension loss was graded as follows: ● Grade 0: intact meniscus with preserved hoop tension continuity ● Grade 1: damage confined to zone 3 (meniscal functional loss <33%) ● Grade 2: damage extending to zone 2 (33% < functional loss < 66%) ● Grade 3: damage extending to zone 1 (functional loss >66%)
For patients who underwent partial meniscectomy during HTO, the degree of hoop tension loss was evaluated based on the final meniscectomized state.
(3) Radiologic parameters at the time of second-look arthroscopy: standing long-leg scanograms were obtained to evaluate lower-limb alignment. The mechanical axis (MA) and weightbearing line (WBL) ratio were measured, and the joint line convergence angle (JLCA) and Kellgren-Lawrence (K-L) grade were assessed to determine the degree of osteoarthritis progression.
The cartilage status of the MFC was evaluated at the time of HTO and at the second-look diagnostic arthroscopy using the ICRS grading system. A single fellowship-trained knee surgeon (D.K.L.) with approximately 10 years of experience at a tertiary referral hospital performed 2 separate evaluations to determine the ICRS grade of the MFC cartilage. To minimize observer bias, cartilage improvement was defined by comparing the ICRS grades obtained independently from the arthroscopic images taken at the time of HTO and at the second-look arthroscopy. Improvement of cartilage was defined as a decrease in ICRS grade on the second-look arthroscopy compared with the grade at the time of HTO, while cases showing no change in grade were classified as no change. Furthermore, postoperative cartilage lesions of the MFC were classified into 2 categories: low-grade chondral lesions (ICRS grade 1 or 2) and high-grade chondral lesions (ICRS grade 3 or 4).
To minimize potential subjectivity arising from variations in arthroscopic magnification, the size of the MFC chondral lesion and the degree of meniscal hoop tension loss were standardized. The measurements were determined by matching arthroscopic images, in which a probe was used for direct measurement of meniscal or chondral defect size, with the corresponding operative records. Preoperative MRI was initially considered to confirm the meniscal and cartilage conditions; however, MRI evaluation was ultimately excluded since most scans performed at outside institutions had been routinely deleted from the hospital server owing to storage limitations, making consistent MRI assessment impractical.
The clinical outcomes were evaluated using the International Knee Documentation Committee (IKDC) subjective score. Assessments were performed on the day before HTO and 2 years postoperatively, on the day before the second-look diagnostic arthroscopy.
Surgical Procedure and Patient Grouping
HTO procedures were performed using a navigation-assisted technique (HTO Version 1.3, Orthopilot; Aesculap) with the correction target set at a postoperative mechanical valgus alignment of 3° to unload the medial compartment and avoid excessive overcorrection. The osteotomy site was opened according to the preoperatively determined correction angle, using a laminar spreader, and fixed with a Tomofix plate and locking screw (Synthes). The gap in the osteotomy site was filled with a cancellous bone chip allograft. At approximately 2 years, hardware removal and second-look diagnostic arthroscopy were performed to evaluate cartilage status. Partial meniscectomy was selectively conducted for flap tears or unstable degenerative horizontal tears likely to cause mechanical symptoms.
During HTO, MFx was performed only when the surrounding cartilage was healthy and the margin of the chondral defect was clearly demarcated, representing a well-shouldered lesion. MFx was not performed for diffuse lesions with indistinct margins or poor surrounding cartilage quality. Patients with diffuse lesions not suitable for MFx were classified as group 1 (n = 30), whereas those with well-shouldered lesions appropriate for MFx formed group 2 (n = 32). The demographic characteristics of both groups are summarized in Table 1. Although patient factors and postoperative alignment did not differ significantly between groups, substantial differences were observed in MFC lesion size, presence of a kissing lesion, degree of medial meniscal hoop-tension loss, JLCA, and K-L grade. These findings indicate that group 1 had more advanced osteoarthritic changes at baseline.
Baseline Demographics and Radiographic Parameters of the Study Population a
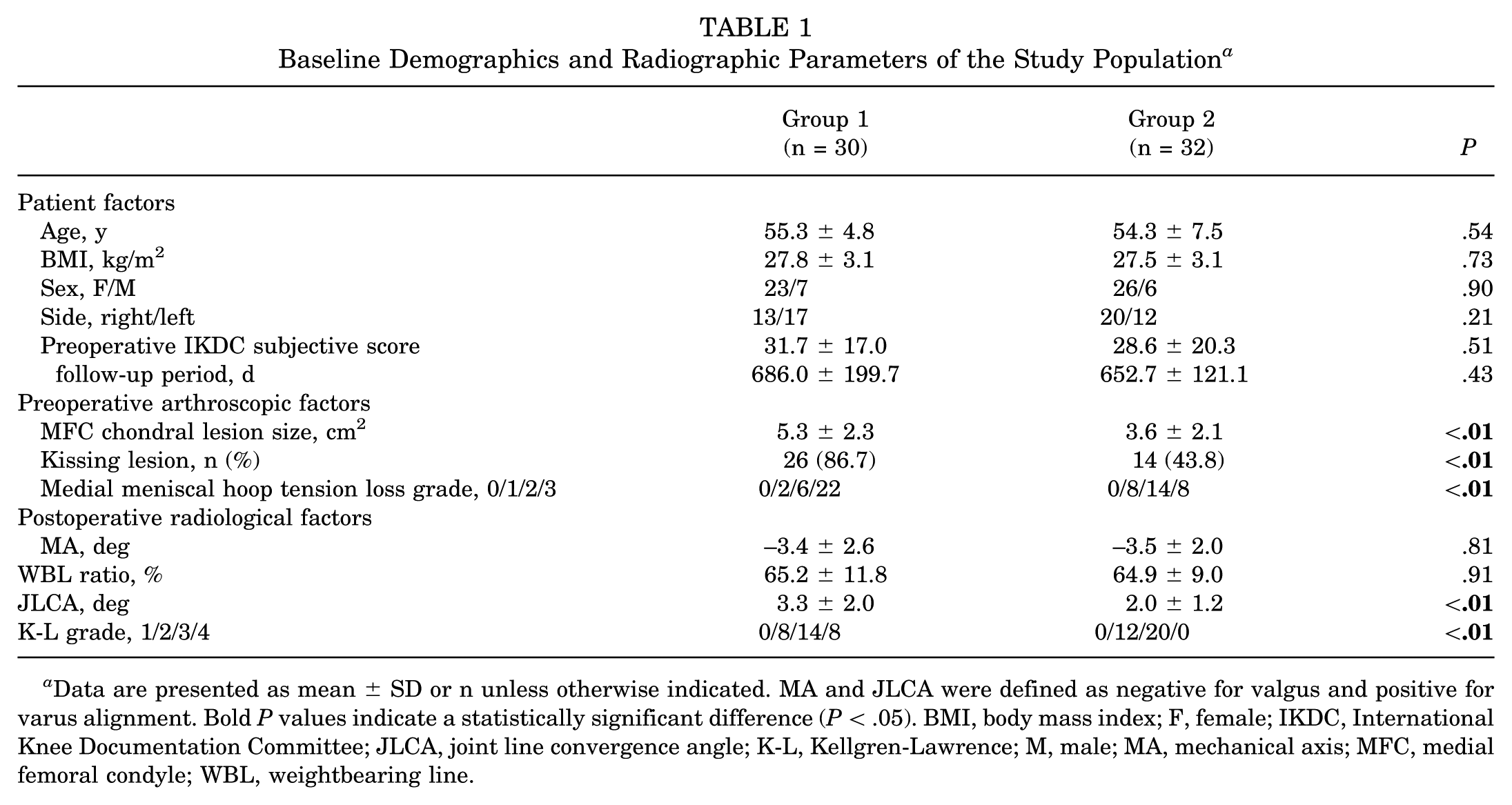
Data are presented as mean ± SD or n unless otherwise indicated. MA and JLCA were defined as negative for valgus and positive for varus alignment. Bold P values indicate a statistically significant difference (P < .05). BMI, body mass index; F, female; IKDC, International Knee Documentation Committee; JLCA, joint line convergence angle; K-L, Kellgren-Lawrence; M, male; MA, mechanical axis; MFC, medial femoral condyle; WBL, weightbearing line.
Outcome Measurement
Cartilage regeneration was analyzed by comparing the proportion of patients with improved or unchanged ICRS grades between groups. Within group 2, the relationship between initial lesion size and postoperative ICRS grade was assessed. Postoperative IKDC scores were compared between groups and further analyzed according to postoperative ICRS grade. Multivariable linear regression included age, BMI, arthroscopic findings (MFC lesion size, kissing lesion, hoop-tension loss, MFx), radiologic parameters (MA, WBL, JLCA, K-L), and postoperative ICRS grade to identify independent predictors of IKDC outcomes.
Statistical Analysis
The normality of continuous variables was assessed using the Shapiro-Wilk test. Multicollinearity among covariates was evaluated prior to multivariable regression. Continuous variables were expressed as mean ± SD when normally distributed and as median (range) when nonnormally distributed, whereas categorical variables were described as frequencies and percentages. Group comparisons were performed using the independent t test for parametric data, the Mann-Whitney U test for nonparametric data, and the chi-square test or Fisher exact test for categorical variables.
For continuous outcomes, multivariable linear regression was performed to determine whether MFx independently influenced postoperative clinical results after adjusting for demographic, arthroscopic, and radiologic factors. Both unstandardized (β) and standardized (β†) coefficients were reported to indicate effect magnitude, and between-group differences were additionally summarized using Cohen d. Partial regression plots were generated to illustrate the adjusted association between MFx and postoperative IKDC scores.
The relationship between changes in cartilage status and clinical outcomes was assessed using Spearman rank correlation between ΔICRS and ΔIKDC, with ρ and P values reported. Scatterplots with regression trend lines visualized the association.
All analyses were performed using Python 3.11 with standard scientific libraries. P < .05 was considered statistically significant, and values between .05 and .10 were regarded as borderline significant.
Results
Changes in ICRS Grade of the MFC Cartilage
In group 1, postoperative ICRS grade improved in 33.3% (10/30), whereas improvement was observed in 62.5% (20/32) in group 2. The improvement rate was significantly higher in group 2 (P = .04) (Table 2).
Comparison of Postoperative ICRS Grades of MFC Cartilage Between Groups a
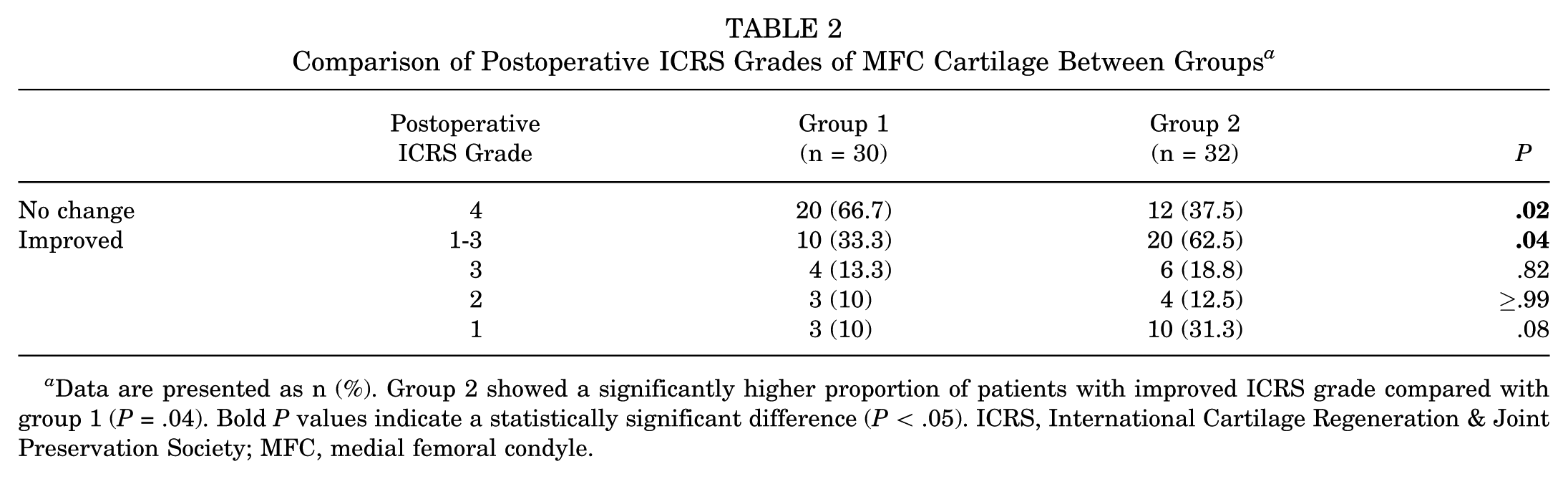
Data are presented as n (%). Group 2 showed a significantly higher proportion of patients with improved ICRS grade compared with group 1 (P = .04). Bold P values indicate a statistically significant difference (P < .05). ICRS, International Cartilage Regeneration & Joint Preservation Society; MFC, medial femoral condyle.
Initial MFC Chondral Lesion Size According to Postoperative ICRS Grade After MFx
In group 2, patients who improved to low-grade lesions (ICRS grade 1-2) had significantly smaller initial MFC lesions than those who remained high grade (3-4) (2.0 [1.0-4.5] vs 6.0 [1.5-7.5]; P < .01) (Figure 2).
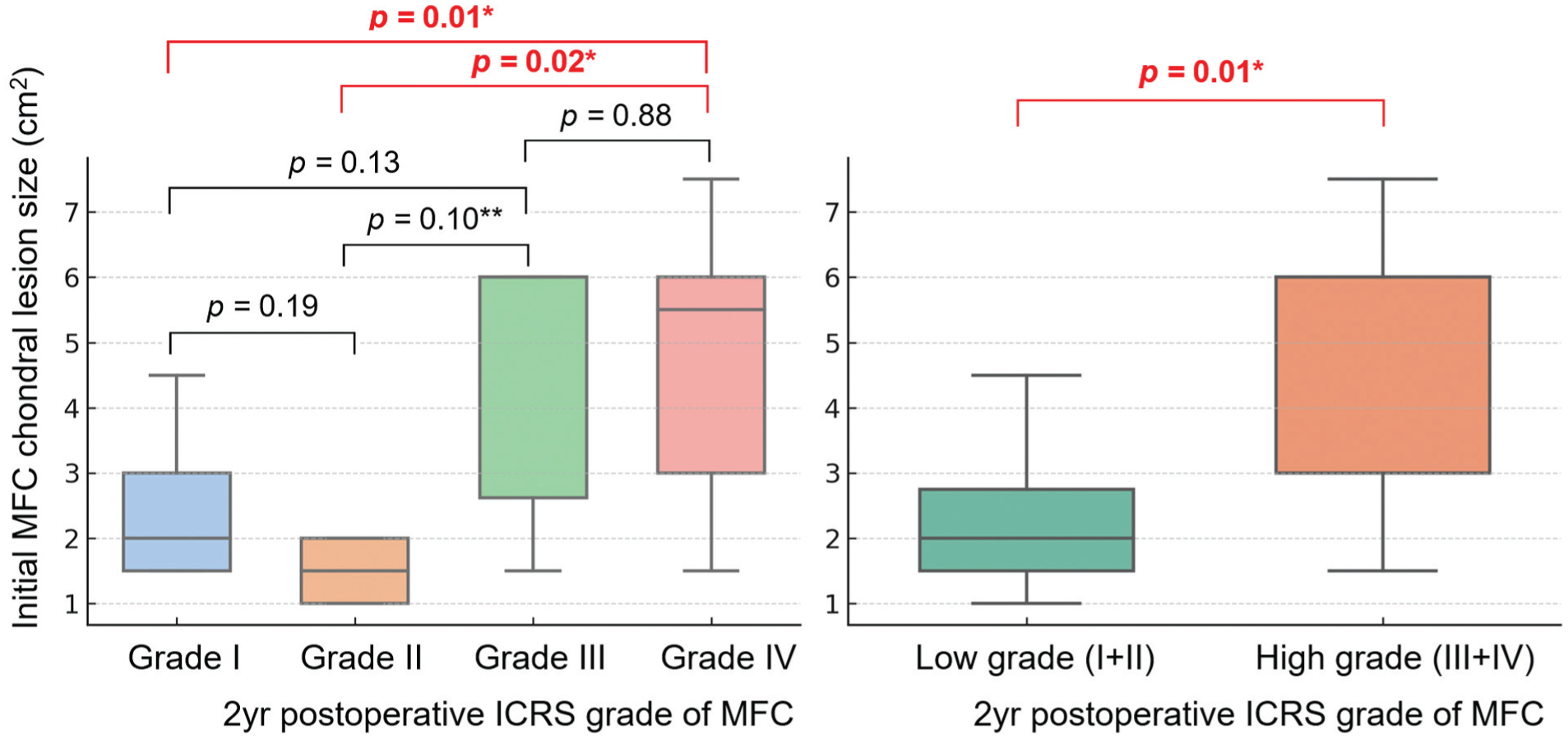
Initial MFC chondral lesion size according to postoperative ICRS grades (left) and grade classification (right) among all patients. High-grade lesions demonstrated significantly larger MFC chondral defects compared with low-grade lesions (P = .01). Data are shown as boxplots with individual data points overlaid. *P < .05; **.05 < P < .10 (borderline statistically significant difference). ICRS, International Cartilage Regeneration & Joint Preservation Society; MFC, medial femoral condyle.
IKDC Scores According to Postoperative ICRS Grade
Postoperative IKDC scores tended to decrease with higher postoperative ICRS grades. Grade 1 demonstrated significantly higher scores than grade 4 (63.2 [41.0-81.6] vs 51.7 [10.3-92.0]; P = .02). The correlation between postoperative ICRS grade and IKDC score was weak and nonsignificant (ρ = −0.205; P = .11) (Figure 3).
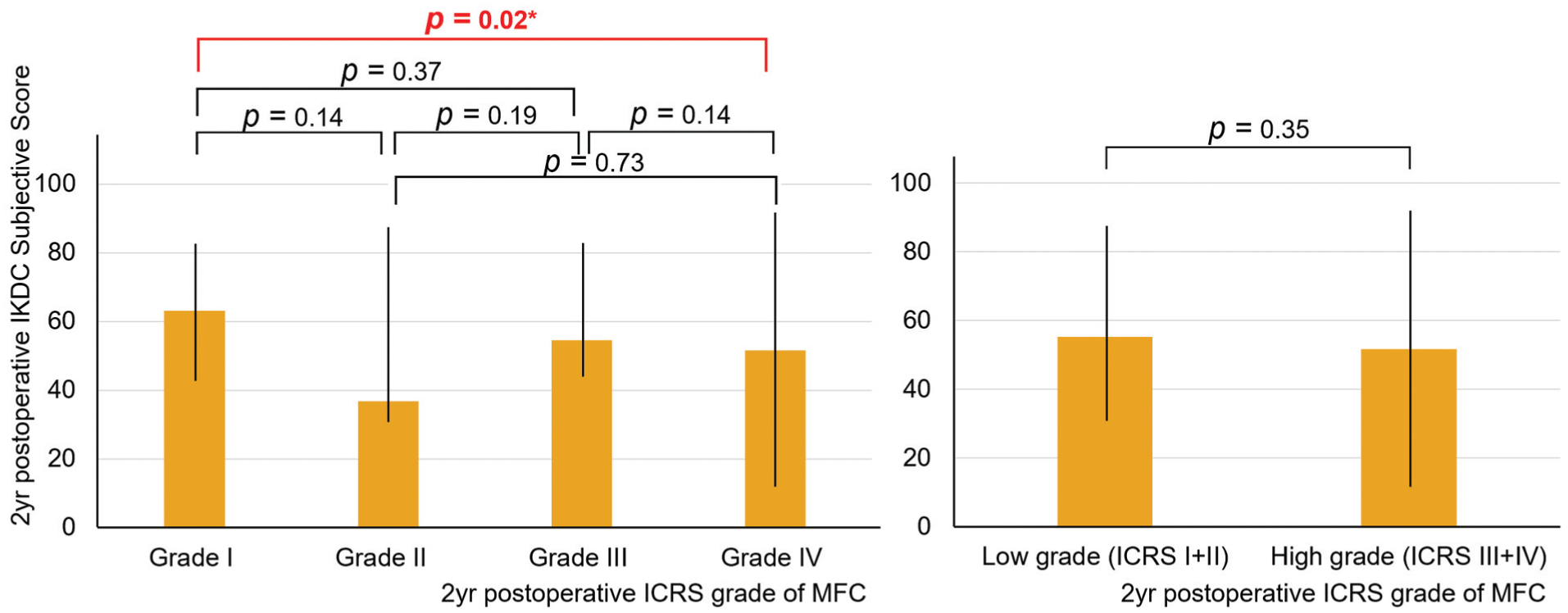
Comparison of 2-year postoperative IKDC subjective scores according to ICRS grade.
IKDC Score Comparison Between Groups
No significant difference in 2-year IKDC scores was observed between group 1 and group 2 (55.2 [14.9-92.0] vs 50.6 [10.3-81.6]; P = .26). Although group 2 tended to show lower IKDC scores across postoperative ICRS grades 2 to 4, differences were not significant. Among patients improving to ICRS grade 2, group 2 showed borderline lower scores (77.0 [46.0-85.1] vs 33.9 [32.2-36.8]; P = .06) (Figure 4).
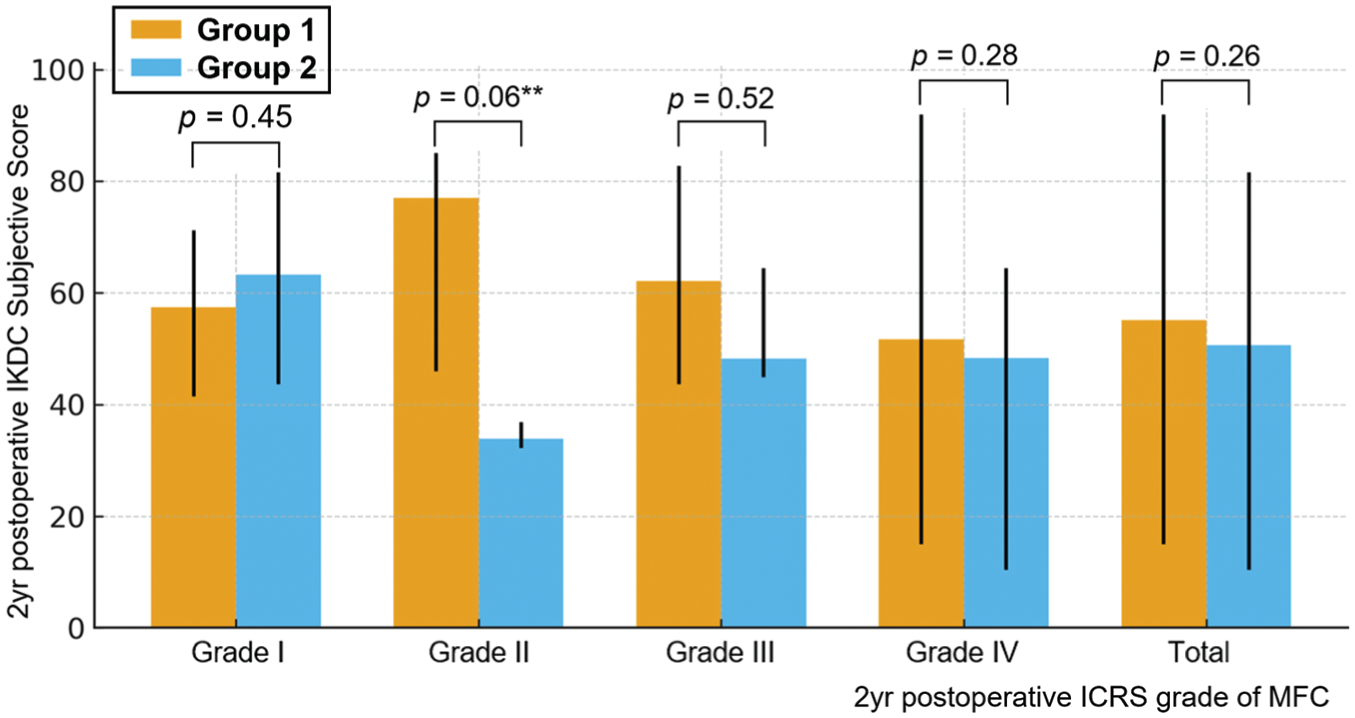
Comparison of postoperative IKDC subjective scores according to postoperative ICRS grades between the 2 groups. Group 2 (patients who underwent microfracture) showed lower postoperative IKDC subjective scores than group 1, although the differences were not statistically significant. Patients with postoperative ICRS grade 2 improvement demonstrated borderline statistical significance, showing lower postoperative IKDC subjective scores in group 2 compared with group 1 (77.0 [46.0-85.1] vs 33.9 [32.2-36.8]; P = .06). Bars represent the median values, and error bars indicate the range (minimum-maximum). **05 < P < .10 (borderline statistically significant difference). ICRS, International Cartilage Regeneration & Joint Preservation Society; IKDC, International Knee Documentation Committee; MFC, medial femoral condyle.
Multivariable Linear Regression for Postoperative IKDC Score
After adjusting for demographic and radiologic differences, MFx was an independent negative predictor of postoperative IKDC score (β = −14.4; P = .01). The standardized β† of −0.8 indicated a large effect size, and partial regression plots showed its inverse association with postoperative function (Table 3, Figure 5). ΔICRS and ΔIKDC demonstrated no significant correlation, indicating structure-symptom discordance (ρ = −0.18; P = .14) (Figure 6).
Multivariable Regression Analysis for Postoperative IKDC Subjective Score a
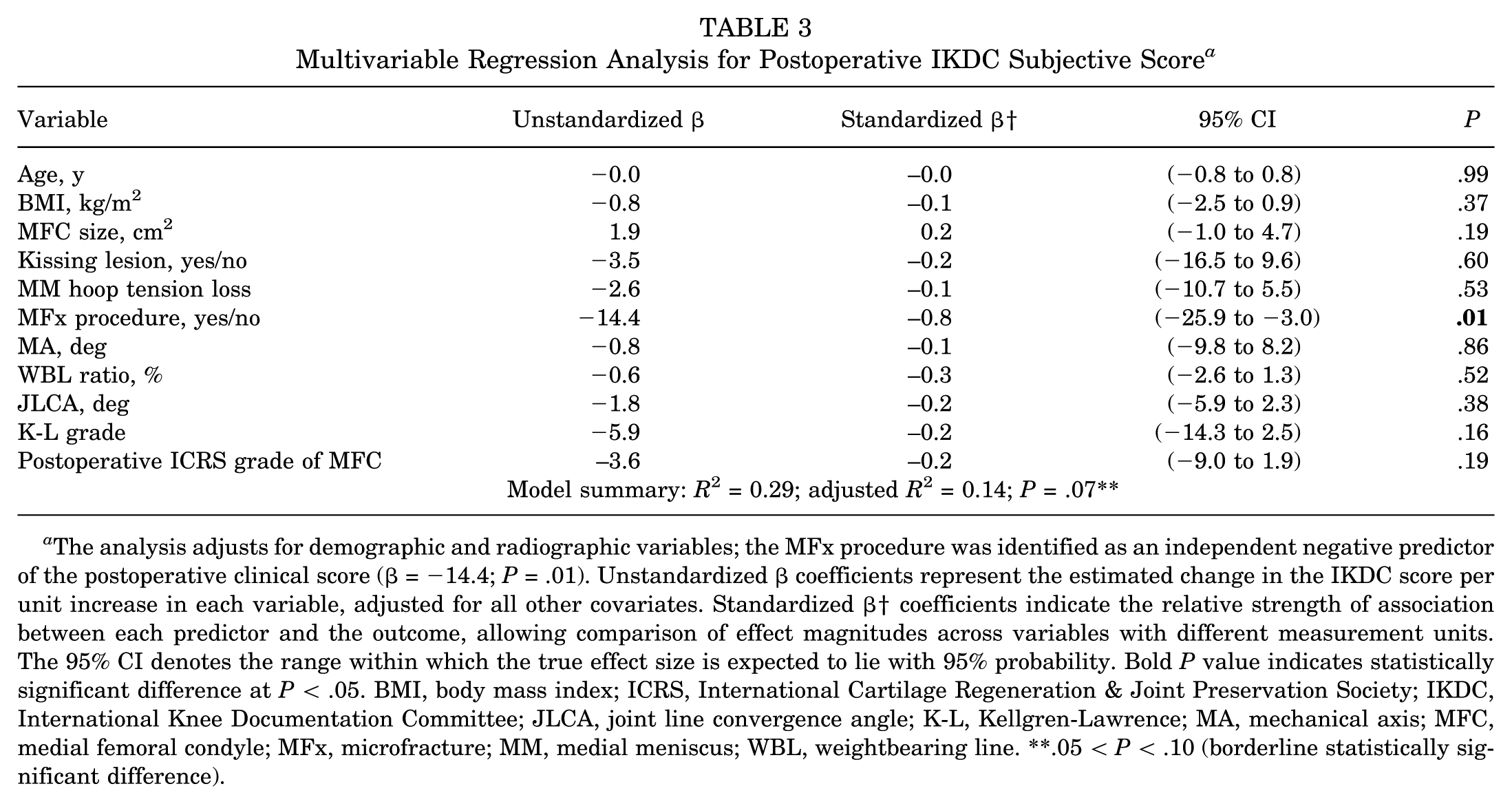
The analysis adjusts for demographic and radiographic variables; the MFx procedure was identified as an independent negative predictor of the postoperative clinical score (β = −14.4; P = .01). Unstandardized β coefficients represent the estimated change in the IKDC score per unit increase in each variable, adjusted for all other covariates. Standardized β† coefficients indicate the relative strength of association between each predictor and the outcome, allowing comparison of effect magnitudes across variables with different measurement units. The 95% CI denotes the range within which the true effect size is expected to lie with 95% probability. Bold P value indicates statistically significant difference at P < .05. BMI, body mass index; ICRS, International Cartilage Regeneration & Joint Preservation Society; IKDC, International Knee Documentation Committee; JLCA, joint line convergence angle; K-L, Kellgren-Lawrence; MA, mechanical axis; MFC, medial femoral condyle; MFx, microfracture; MM, medial meniscus; WBL, weightbearing line. **.05 < P < .10 (borderline statistically significant difference).
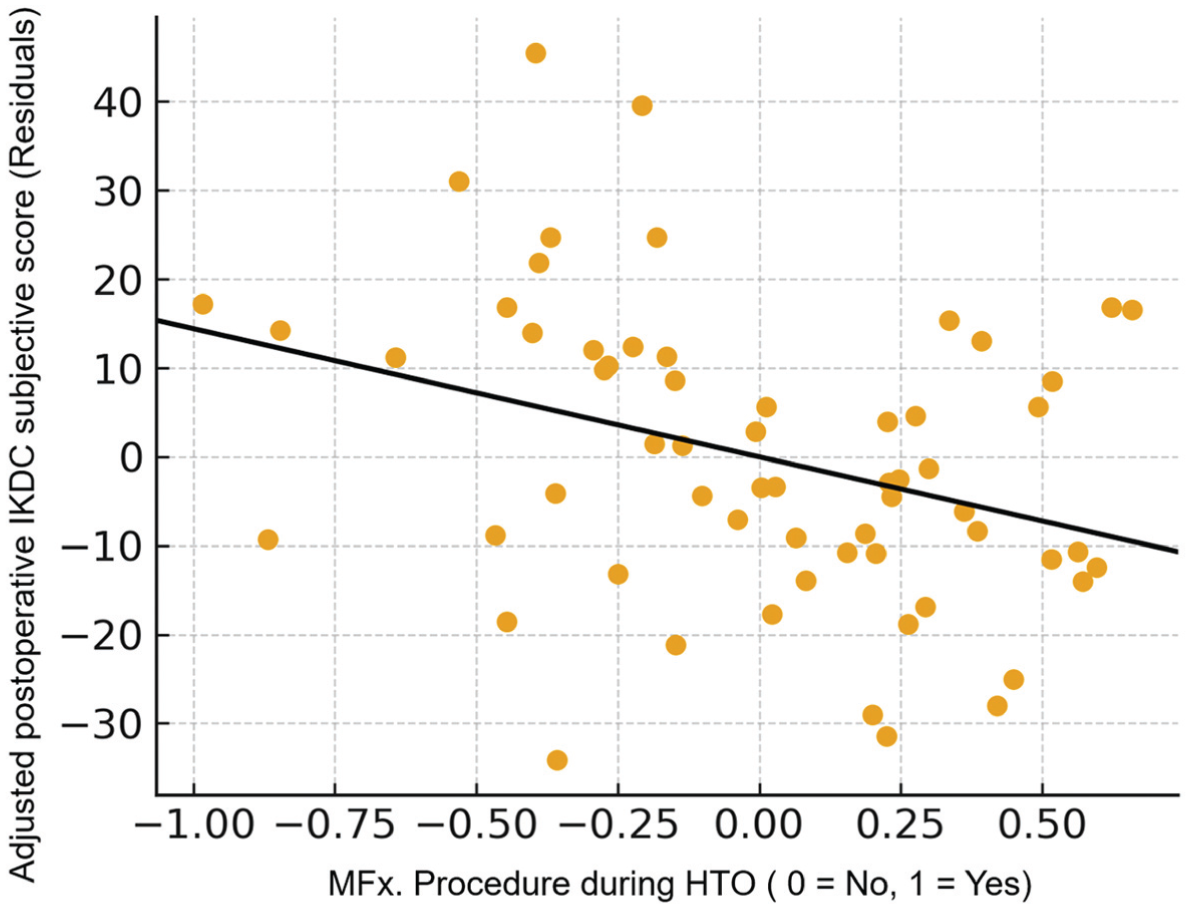
Partial regression plot showing the adjusted relationship between the MFx procedure and postoperative IKDC subjective score after controlling for baseline covariates (age, body mass index, medial femoral condylar size, mechanical axis, weightbearing lie, joint line convergence angle, Kellgren-Lawrence grade, Kissing lesion, Cooper classification, and postoperative International Cartilage Regeneration & Joint Preservation Society grade). Patients who underwent MFx. demonstrated significantly lower adjusted postoperative clinical scores (β = −14.4; P = .01). HTO, high tibial osteotomy; IKDC, International Knee Documentation Committee; MFx, microfracture.
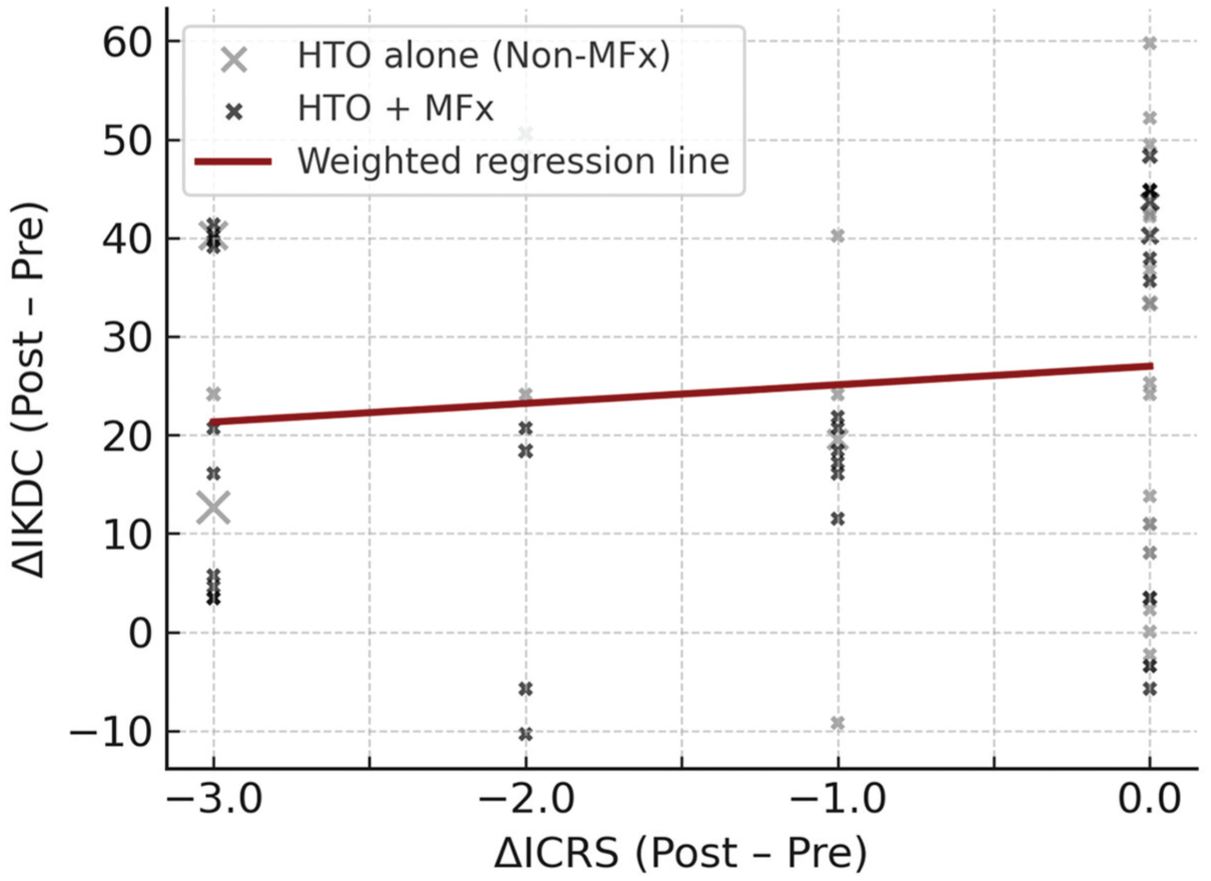
Scatterplot illustrates the relationship between structural and symptomatic recovery after HTO. Each dot represents 1 knee: gray = HTO-alone group and black = HTO + MFx group. The red regression line shows the overall trend (ρ = −0.18; P = .14). Changes in cartilage grade (ΔICRS) were not significantly correlated with improvements in clinical score (ΔIKDC), suggesting a structure-symptom discordance between morphological regeneration and patient-reported outcomes. HTO, high tibial osteotomy; ICRS, International Cartilage Regeneration & Joint Preservation Society; IKDC, International Knee Documentation Committee; MFx, microfracture.
Discussion
In the present study, patients who underwent MFx during HTO demonstrated greater improvement in cartilage regeneration than those who did not. However, MFx was selectively performed in well-shouldered defects with clear margins and healthier surrounding cartilage, whereas non-MFx cases showed diffuse chondral degeneration. These baseline differences indicate that osteoarthritic severity was not identical between groups, so it is difficult to attribute superior regeneration solely to MFx. Systematic reviews have suggested that cartilage regeneration after the combined use of cartilage regeneration procedures and HTO is influenced by postoperative limb alignment, lesion characteristics, and patient-specific factors. 13 Previous investigations have reported cartilage regeneration after HTO alone in 44.6% to 62.1% of patients within 1 to 2 years,21,29,30 whereas studies combining HTO with MFx have shown rates of 50% to 85%.3,39 In the present study, MFx was selectively performed in well-shouldered chondral lesions, with cartilage improvement in 62.5% of patients. This finding suggests that MFx may provide a limited synergistic effect on cartilage regeneration when used in carefully selected lesions with favorable biological environments. 1 When the outcomes of prior HTO-alone studies are considered, the additional benefit of MFx appears modest rather than remarkable.21,29,30 It is also noteworthy that cartilage regeneration was not achieved in all patients who underwent MFx. Among the MFx group, those whose cartilage improved to low-grade lesions (ICRS grade 1 or 2) tended to have smaller initial chondral defect sizes (mean, 2 cm2), whereas patients with larger lesions showed less improvement after surgery. These findings indicate that the efficacy of MFx may depend on lesion size, with better cartilage regeneration in smaller defects. 7 This observation aligns with the established principle that MFx yields the most favorable results in focal chondral defects <2 cm2, as demonstrated in previous reports. 36
In medial OA, most chondral lesions are regarded as secondary degenerative changes rather than primary pathologies, except in acute trauma or osteochondritis dissecans. 2 Such lesions typically arise from mechanical overload related to varus malalignment, ligamentous laxity, or meniscal deficiency. In many patients undergoing HTO, degeneration of the meniscus results in diminished shock absorption and lubrication functions. Degenerative meniscal tear—including horizontal, complex, or root tears—increased contact pressure and a reduced contact area, thereby accelerating cartilage degeneration.2,22,38 Although some clinicians consider the cartilage defect itself as the primary target of treatment, cartilage damage in OA is more appropriately interpreted as a secondary pathological manifestation resulting from altered joint kinematics due to meniscal dysfunction or limb malalignment. From this standpoint, the principal therapeutic mechanism of HTO is correction of limb alignment toward the lateral compartment, which reduces medial compartment compressive stress. Medial collateral ligament release during HTO further modifies load distribution and joint biokinematics, decreasing excessive medial compartment stress. 1 These biomechanical adjustments can help restore the metabolic balance between anabolic and catabolic processes within the cartilage environment, allowing partial cartilage recovery even without additional cartilage regeneration procedures.21,29,30 MFx may provide an additional biological stimulus by introducing marrow-derived cells and growth factors, although its regenerative capacity appears limited in advanced degenerative conditions.15,49 Patients with subtotal meniscectomy, obesity, or systemic comorbidities such as diabetes, cardiovascular disease, or chronic renal dysfunction often exhibit impaired subchondral circulation and reduced biological activity, which restrict the potential for regeneration even after HTO.6,8,21-23,26,41 Therefore, variability in patient selection, surgical indications, and meniscal management across studies likely contributes to inconsistencies in previously reported cartilage regeneration outcomes after HTO.3,13,21,29,30,39
Whether postoperative cartilage status influences clinical outcomes after HTO remains controversial. Some studies have reported no significant correlation between cartilage regeneration and clinical improvement,21,29 and others have suggested that greater cartilage regeneration is associated with better clinical outcomes.3,48,50 This discrepancy has led to ongoing debate regarding whether concurrent cartilage regeneration procedures, such as MFx, should be performed during HTO to enhance patient outcomes. In the present study, no statistically significant difference was observed in 2-year IKDC subjective scores between patients who underwent HTO with MFx and those who underwent HTO alone. Considering that group 2 (MFx group) consisted of patients with less advanced OA and a higher rate of cartilage regeneration, superior clinical outcomes would be expected in line with our initial hypothesis. However, the MFx group showed slightly lower mean IKDC scores than the HTO-alone group, although this difference was not statistically significant. When postoperative IKDC scores were analyzed according to MFC ICRS grade, a trend toward lower scores with increasing ICRS grade was observed, but the negative correlation was not significant. After adjusting for potential confounders, including patient demographics, postoperative radiologic parameters, and osteoarthritis severity, the MFx procedure emerged as the only independent factor significantly associated with postoperative clinical outcomes, with an estimated 14.4-point lower IKDC score in the MFx group. MFx induces fibrocartilage rather than hyaline cartilage, and clinical improvement typically peaks within the first postoperative year, with gradual decline as the fibrocartilage deteriorates over time. 31 From this clinical perspective, the finding that the MFx group showed lower IKDC scores at 2 years postoperatively compared with the non-MFx group appears counterintuitive, given that MFx is generally intended to enhance cartilage repair and postoperative recovery. Previous studies have reported that alignment correction influences postoperative outcomes. 4 However, in the present study, no statistically significant difference in postoperative limb alignment was observed between group 1 and group 2, suggesting that limb alignment is unlikely to have influenced the difference in clinical outcomes between the 2 groups.
Although it is difficult to clearly explain the divergent response in which microfracture was associated with a 14.4-point decrease in postoperative clinical scores, several plausible mechanisms can be considered. First, it is well-established that cartilage lesions are often asymptomatic and do not necessarily correlate with clinical pain or symptomatic or functional impairment.2,32,34 If cartilage damage were directly responsible for symptoms, patients with end-stage OA and complete cartilage wear would be expected to experience constant pain, although some report only mild discomfort. Conversely, individuals with early- to moderate-stage OA (K-L grade 1-3) and minimal cartilage degeneration can experience severe pain, particularly when a medial meniscus root tear causes abrupt disruption of joint mechanics. Several previous studies have reported that the radiographic OA severity does not correlate with pain intensity, supporting the concept that OA pain is more closely linked to acute biomechanical or inflammatory changes than to structural cartilage loss.20,34
According to the definition proposed by the Osteoarthritis Research Society International, OA is a condition in which the homeostasis between anabolic and catabolic activities within the joint is disrupted, leading to both anatomical and physiological degeneration. 25 From this perspective, the therapeutic goal in OA management should focus less on repairing visible structural lesions–such as cartilage defects or meniscal lesions identified on imaging or arthroscopy–and more on restoring biological and metabolic balance within the joint microenvironment. This concept underlies a stepwise treatment strategy. Initially, conservative management such as pharmacologic therapy, intra-articular injection, and muscle-strengthening exercises aims to restore metabolic balance and reduce catabolic activity.14,45 When these measures fail to control symptoms because of persistent metabolic imbalance, joint-preserving surgical interventions such as HTO or meniscal repair can be considered. 43 These procedures alter intra-articular kinematics, reduce the rate of catabolic processes, and can improve symptoms by inducing rebalance of metabolic homeostasis within the joint.10,12,19,42,47 When severe comorbid conditions that accelerate catabolic processes are present, or when irreversible biomechanical osteoarthritic changes make it difficult to restore metabolic balance through joint-preserving interventions, arthroplasty becomes a definitive option by eliminating the pathological joint environment and suppressing further catabolic progression.6,11,17,24,43 From a surgical perspective, the key challenge lies in identifying which patients can achieve symptomatic relief through modulation of the catabolic process by biomechanical correction. Currently, there are no established guidelines to assist surgeons in making this determination.5,19,24,44 Recent studies have demonstrated that patients with advanced cartilage lesions exhibit poorer clinical outcomes after HTO than those with low-grade lesions.3,17,50 This observation supports the concept that once irreversible biomechanical derangement develops, mechanical realignment alone may not be sufficient to restore joint homeostasis or symptomatic improvement. 43 Surgical decision making should therefore be individualized based on physiological age, activity level, and systemic comorbidities rather than solely on radiologic or arthroscopic findings. 6
Second, performing MFx during HTO may trigger an additional inflammatory healing response at both osteotomy and cartilage regeneration sites. This amplified inflammatory activity could contribute to postoperative discomfort and altered muscle physiology. Previous studies have reported that inflammation-related pain can lead to asymmetric muscle atrophy, a phenomenon known as pain-related secondary sarcopenia. 27 In this process, inflammatory mediators influence both nociceptive and motor pathways, resulting in localized muscle weakness around the affected joint. Recent investigations have identified inflammatory cytokines and knee pain as key contributors to muscle atrophy and deterioration of muscle quality.18,27,37,46 Muscle weakness has been shown to be closely associated with pain and symptoms in patients with knee OA.9,31,33 Lee et al 27 further demonstrated that pain-related secondary sarcopenia involves not only a reduction in muscle volume but also fatty degeneration—an irreversible structural change that contributes to a lasting decline in muscle quality and delayed recovery. Considering these mechanisms, it is plausible that while MFx may offer visual satisfaction to the surgeon by achieving fibrocartilaginous filling of the chondral defect, the accompanying inflammatory response during cartilage healing could induce localized and partly irreversible muscle degeneration. This process may explain the inferior postoperative clinical scores observed in the MFx group in the present study. Pathophysiologically, the link between structural restoration and symptomatic recovery likely depends on the integrity of the neuromuscular system governing dynamic joint stability. Even when cartilage regeneration is achieved morphologically, inadequate periarticular muscle strength and impaired proprioceptive control may prevent effective load redistribution, thereby sustaining abnormal joint stresses and pain perception. This biomechanical-biological uncoupling provides a mechanistic explanation for why structural repair does not necessarily lead to symptomatic improvement.2,7,13,32,34,48 Thus, achieving joint homeostasis may require concurrent restoration of both structural and neuromuscular integrity rather than cartilage regeneration alone. Future studies incorporating quantitative muscle assessment could further clarify the biological pathways linking structural and symptomatic recovery after HTO.
Limitations
This study has several limitations. First, the 2 groups showed significant demographic and baseline differences, including arthroscopic findings at HTO (MFC lesion size, presence of a kissing lesion, and degree of meniscal hoop-tension loss) and radiographic indicators of OA severity (JLCA and K-L grade). Direct comparison between such heterogeneous groups may not be fully valid. Nevertheless, despite group 2’s having less advanced OA, demonstrating greater cartilage regeneration, and undergoing MFx, no significant difference was observed in 2-year clinical outcomes, and the MFx group even showed lower scores. After adjusting for demographic and radiologic differences, MFx remained an independent negative predictor. Second, this study did not include a detailed evaluation of systemic comorbidities, which may influence cartilage metabolism, inflammatory responses, or postoperative recovery. Third, degenerative changes in the patellofemoral and lateral compartments were not separately graded. Although patients with progressive lateral compartment degeneration were not considered candidates for HTO, residual confounding related to the severity of multicompartmental degenerative change, particularly in the patellofemoral joint, cannot be excluded. Additionally, the relatively small sample size may have rendered the study underpowered to detect modest between-group differences, particularly in postoperative clinical outcomes. Therefore, the negative findings should be interpreted with caution. Despite these limitations, the present findings suggest that although MFx may promote cartilage regeneration during HTO, it is associated with a divergent clinical response characterized by limited symptomatic improvement. The discordance between morphological and symptomatic recovery after HTO may reflect an interplay among cartilage regeneration, inflammation, and neuromuscular impairment.
Conclusion
Concurrent MFx during HTO produced morphological improvement without corresponding symptomatic benefit, indicating a structure-symptom discordance. Structural benefit was more evident in small, well-defined focal cartilage lesions, whereas no meaningful clinical advantage was observed.
Footnotes
Final revision submitted March 30, 2026; accepted April 19, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2024-00340610) and the Nano & Material Technology Development Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Science and ICT (RS-2024-00407234).
Ethical approval for this study was obtained from Samsung Changwon Hospital Institutional Review Board (file No. 2025-11-038).