
Abstract
Background:
Medial opening wedge high tibial osteotomy (MOWHTO) is widely used to treat medial compartment osteoarthritis with varus malalignment. Variations in proximal tibial intra-articular morphology may influence alignment correction during osteotomy, but their clinical significance remains unclear.
Purpose/Hypothesis:
The purpose of this study was to evaluate whether different plateau morphologies are associated with differences in radiographic changes, clinical outcomes, and cartilage regeneration. It was hypothesized that proximal tibial plateau morphology does not significantly influence clinical outcomes or cartilage regeneration after MOWHTO.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
That data of 186 patients who underwent unilateral MOWHTO between 2016 and 2022 were retrospectively reviewed. Based on the angular relationship between the medial and lateral tibial plateaus, knees were classified as depressed (n = 60), flat (n = 83), or convex (n = 43). Radiographic parameters including medial proximal tibial angle, hip-knee-ankle angle, joint line convergence angle (JLCA), and weightbearing line ratio were measured preoperatively and postoperatively. Changes in JLCA were analyzed using repeated-measures analysis of variance. Clinical outcomes were assessed using the Knee injury and Osteoarthritis Outcome Score (KOOS). Cartilage regeneration was evaluated arthroscopically according to the International Cartilage Regeneration & Joint Preservation Society grading system during second-look arthroscopy.
Results:
Baseline characteristics and postoperative radiographic parameters were comparable among groups. A significant group × time interaction was observed for JLCA (P = .016), with the convex type showing greater JLCA change than the depressed (P = .018) and flat (P = .049) types; however, the magnitude of the difference was small (<1°). Postoperative KOOS values were similar among groups, and plateau inclination analyzed as a continuous variable was not correlated with KOOS (Pearson r = 0.112; P = .13). Second-look arthroscopy was performed in 103 patients, demonstrating cartilage improvement in 53.1%, 58.3%, and 52.2% of the depressed, flat, and convex groups, respectively (P = .790).
Conclusion:
Proximal tibial plateau morphology did not significantly affect clinical outcomes or changes in cartilage status after MOWHTO.
Medial opening wedge high tibial osteotomy (MOWHTO) is a widely adopted surgical procedure for the management of medial compartment osteoarthritis associated with varus knee alignment.16,18 The procedure aims to offload the medial compartment by shifting the mechanical axis of the lower limb toward the lateral side. In addition to overall limb alignment, which has been the primary focus of most previous studies, individual variations in bone morphology may also play an important role. These variations may arise from differences in femoral deformity, tibial deformity, or even intra-articular morphology.5,13,20,21 Theoretically, such anatomic heterogeneity could influence the biomechanical environment after osteotomy and potentially affect surgical outcomes.
With respect to the intra-articular morphology of the proximal tibia, the configuration of the tibial plateau joint line can generally be classified into 3 types—depressed, flat, and convex (pagoda-like)—based on the angular relationship between the medial and lateral tibial plateaus. 12 Previous studies have suggested that in patients with the convex type, correction with MOWHTO may lead to insufficient contact of the lateral compartment due to the inclination of the lateral tibial plateau after realignment. 3 Consequently, it has been proposed that such patients are potential candidates for tibial condylar valgus osteotomy (TCVO). Several reports of TCVO have demonstrated favorable clinical outcomes in this subgroup.3,6,11
However, whether high tibial osteotomy (HTO) results in different clinical outcomes across these 3 morphological types remains unclear. To our knowledge, only 1 study has examined this issue and reported greater postoperative changes in the joint line convergence angle (JLCA) in convex-type tibial plateaus, particularly in cases requiring larger correction during HTO. 8 Nevertheless, that study did not evaluate patient-reported outcomes or cartilage regeneration. Therefore, the clinical implications of proximal tibial intra-articular morphology in patients undergoing HTO remain insufficiently understood and warrant further investigation.
Therefore, the purpose of this study was to determine whether different proximal tibial intra-articular morphologies (depressed, flat, and convex types) are associated with differences in clinical outcomes after MOWHTO, with a particular focus on patient-reported outcomes and cartilage regeneration.
Methods
This retrospective observational study was conducted at the National Taiwan University Hospital with approval from the institutional Ethics Committee (approval No.: 202407168RINA). The requirement for informed consent was waived because of the retrospective study design. Between March 2016 and March 2022, 220 consecutive patients who underwent unilateral MOWHTO were initially identified. The inclusion criteria were symptomatic medial compartment osteoarthritis confirmed on standing knee radiographs, a mechanical tibiofemoral angle ≥5°, and a flexion contracture <10°.
Fifteen patients were excluded because preoperative or postoperative standing full-length anteroposterior radiographs were unavailable in the picture archiving and communication system. One patient who underwent concomitant proximal fibulectomy was also excluded. In addition, 2 patients who died during follow-up and 2 patients who underwent further surgery on the same limb were excluded. Clinical outcome data were unavailable for 14 patients. Ultimately, 186 patients who underwent unilateral MOWHTO were included in the final analysis.
Surgical Technique and Rehabilitation Protocol
Diagnostic arthroscopy was routinely performed before MOWHTO. After completion of the arthroscopic procedure, a skin incision was created along the anteromedial aspect of the proximal tibia. The subsequent surgical technique generally followed previously reported methods. A biplanar medial opening wedge osteotomy was then carried out. The primary transverse osteotomy was made from the medial cortex toward the lateral cortex of the tibia above the proximal tibiofibular joint, followed by an ascending anterior cut in the coronal plane to create the biplanar configuration. Fixation was achieved using an A-plus locking plate (A-Plus Biotechnology Co, Ltd) specifically designed for the medial proximal tibia. The planned correction aimed to shift the mechanical axis so that the weightbearing line (WBL) passed through the Fujisawa point.14,24
Postoperatively, patients were permitted partial weightbearing immediately, with progression to full weightbearing at approximately 4 weeks. A structured rehabilitation program, including range of motion and muscle strengthening exercises, was initiated on the second postoperative day under the supervision of a physiotherapist. Thereafter, rehabilitation was tailored to each patient according to physical condition and functional goals, with most patients expected to return to their preoperative activity level within 3 to 6 months.
Plate removal was considered 1 year after surgery if radiographic union of the osteotomy site had been confirmed, and the procedure was performed only on patient request. Second-look arthroscopy was routinely performed at the time of hardware removal.
Radiological Assessment and Classification of Tibial Intra-articular Morphology
The morphology of the tibial plateau was categorized as flat, depressed, or convex according to the relative inclination of the medial and lateral articular surfaces. Measurements were performed using the method described by Itou et al. 8 For each plateau, an inclination line was defined by connecting the outer margin of the tibial plateau to the midpoint between this margin and the apex of the intercondylar ridge (Figure 1). The inclination angle of the articular surface was considered positive when the surface demonstrated a convex configuration superiorly.
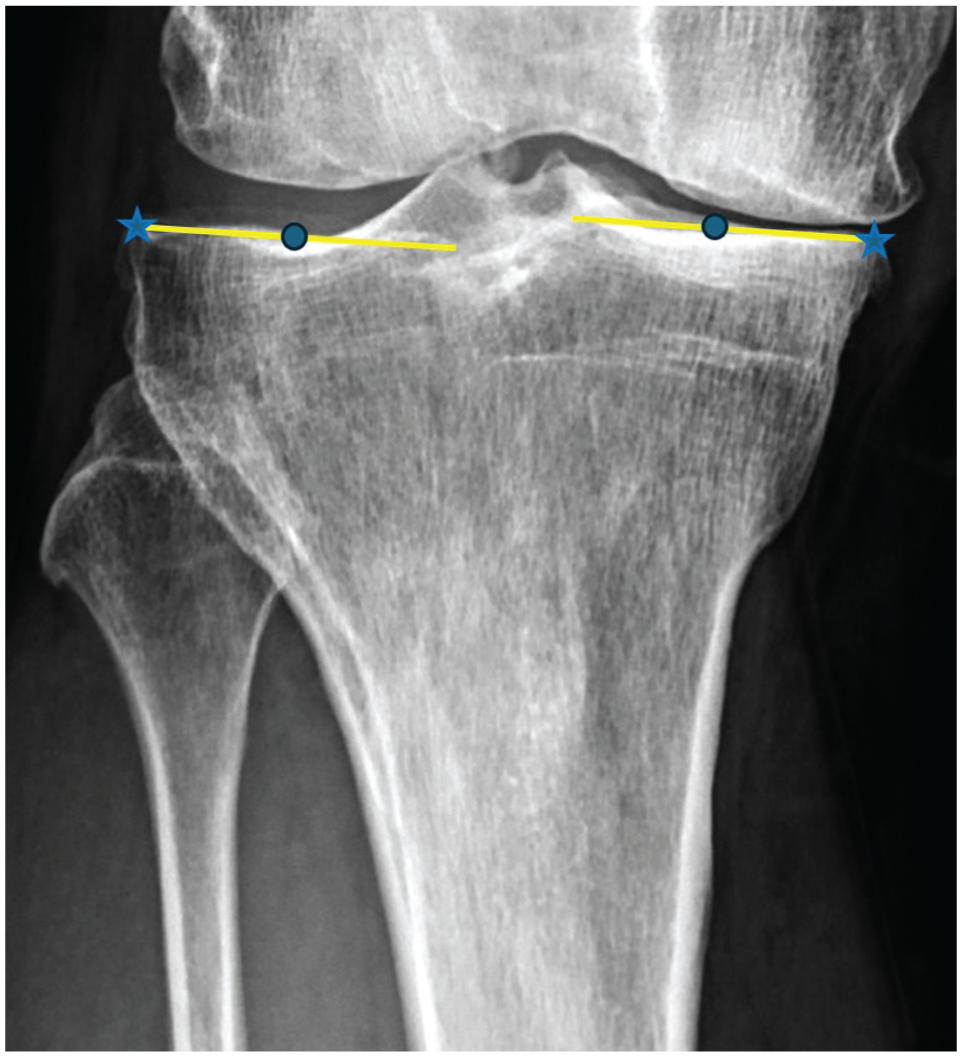
Measurement of the inclination angle. The star indicates the outer margin of the tibial plateau, and the circle indicates the midpoint between the tibial outer edge and the apex of the intercondylar ridge.
Based on this measurement, plateau morphology was classified as flat when the difference in inclination between the medial and lateral articular surfaces was within ±3°, depressed when the value was <−3°, and convex when it was >3°. 8 Representative examples of the 3 types are shown in Figure 2.
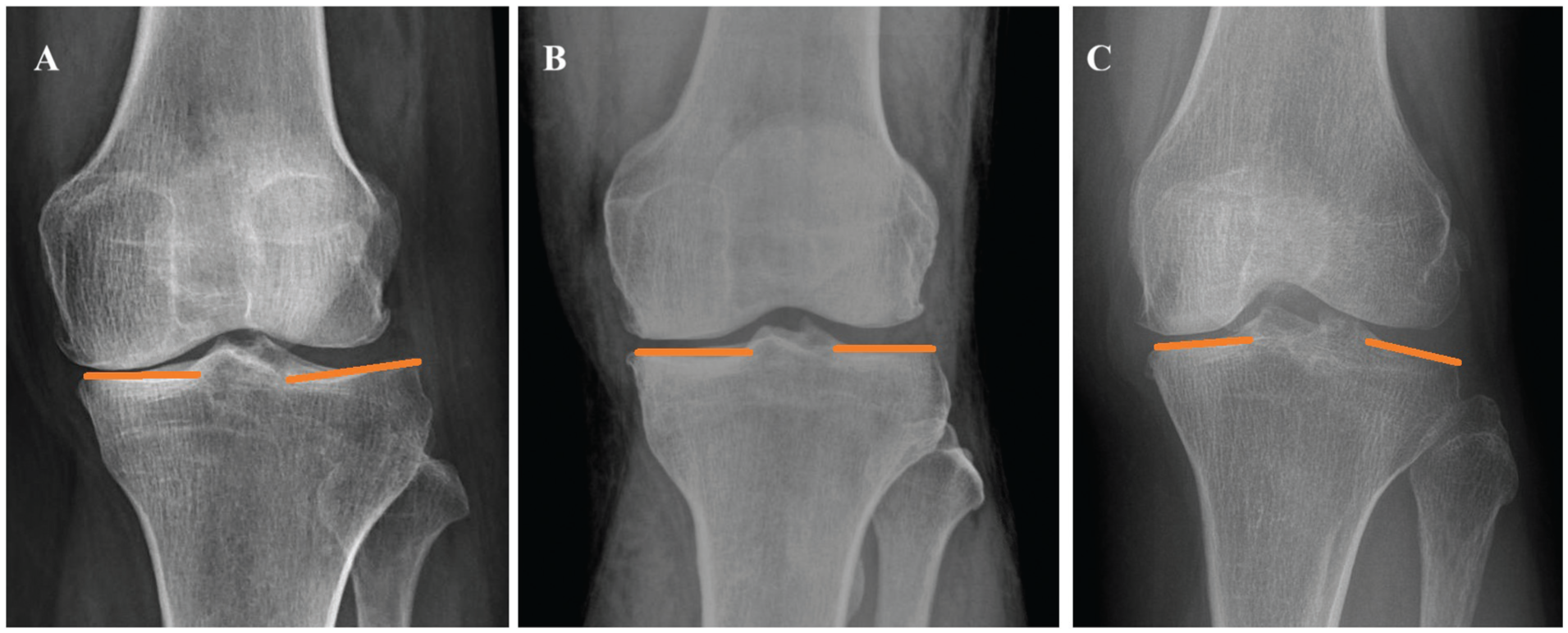
Representative examples: (A) depressed, (B) flat, and (C) convex types.
Evaluation of Baseline Characteristics, Radiological Parameters, Clinical Outcome, and Cartilage Regeneration
Descriptive variables, including age, sex, height, and body weight, were recorded to compare baseline characteristics among the 3 groups. Preoperative and postoperative medial proximal tibial angle (MPTA), JLCA, hip-knee-ankle angle (HKA), and WBL ratio were measured and compared. The WBL was determined by identifying the point where a line drawn from the center of the femoral head to the center of the talus intersects the articular surface of the proximal tibia. The WBL ratio was calculated by dividing the distance from the medial edge of the tibial plateau to this intersection by the total width of the tibial articular surface. Representative images illustrating the measurement of these radiographic parameters are shown in Figure 3. Postoperative patient-reported outcomes were assessed using the Knee injury and Osteoarthritis Outcome Score (KOOS). Complications, including nonunion, loss of reduction, and plate breakage, were also recorded and analyzed. Loss of reduction was defined as a change in MPTA ≥3° between the immediate postoperative measurement and the final follow-up. 22
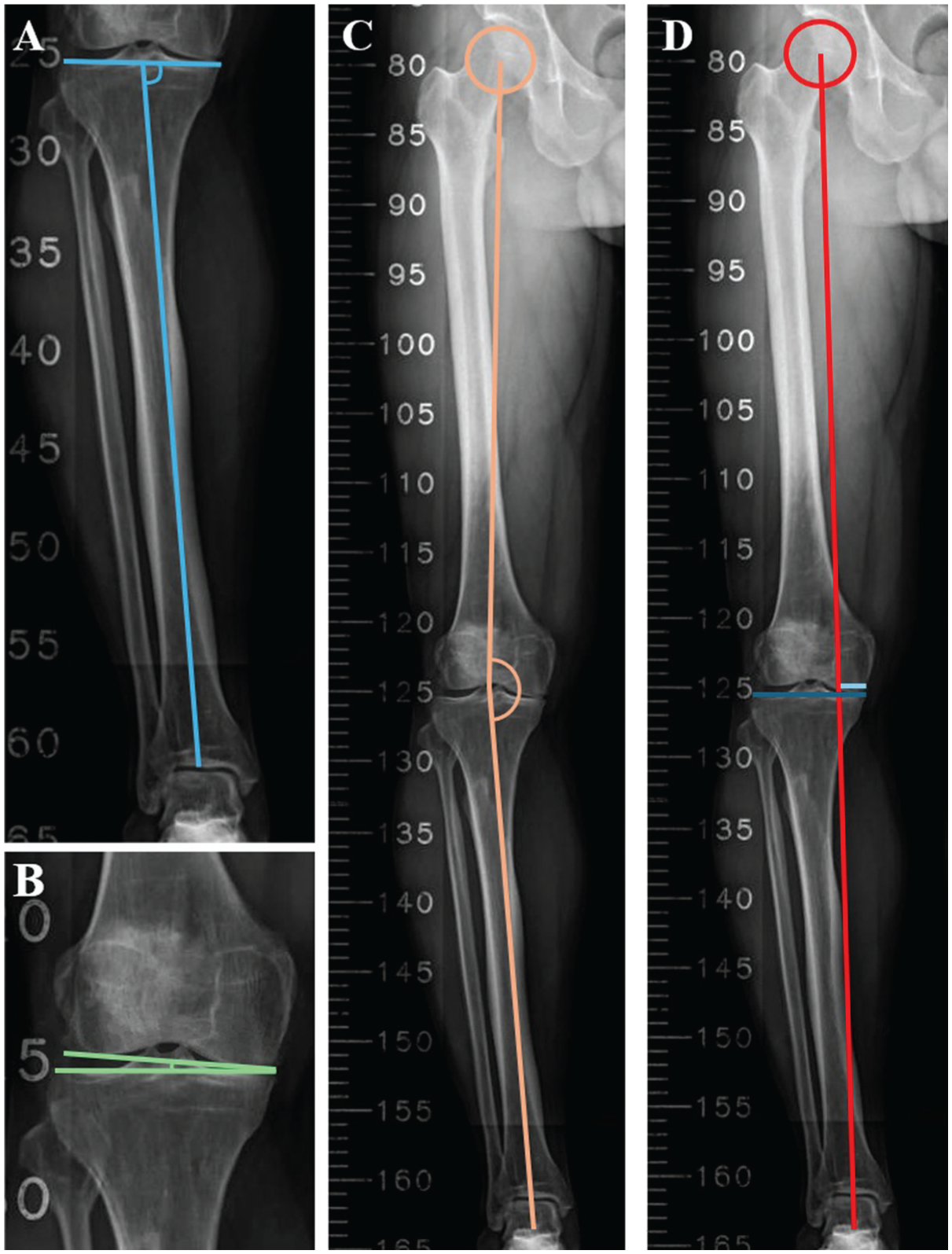
Representative examples: (A) medial proximal tibial angle, (B) joint line convergence angle, (C) hip-knee-ankle angle, and (D) weightbearing line ratio: the ratio of the length of the light blue line to that of the dark blue line.
Arthroscopic findings at initial arthroscopy and second-look arthroscopy were reviewed to evaluate cartilage regeneration. Cartilage status of the medial femoral condyle was graded according to the International Cartilage Regeneration & Joint Preservation Society (ICRS) classification. The tibial side was not evaluated because the arthroscopic images in our series were frequently insufficient for reliable and consistent grading and were therefore excluded from analysis. ICRS grading was based on operative records and was independently reassessed by the corresponding author (T.H.T.) in a blinded manner using pre- and postoperative arthroscopic views. In cases of ambiguous findings, final determination was made by the senior author (J.H.W.). Representative images are presented in Figure 4. Based on the arthroscopic ICRS grade, patients were categorized into 3 groups: improved, unchanged, and worsened.
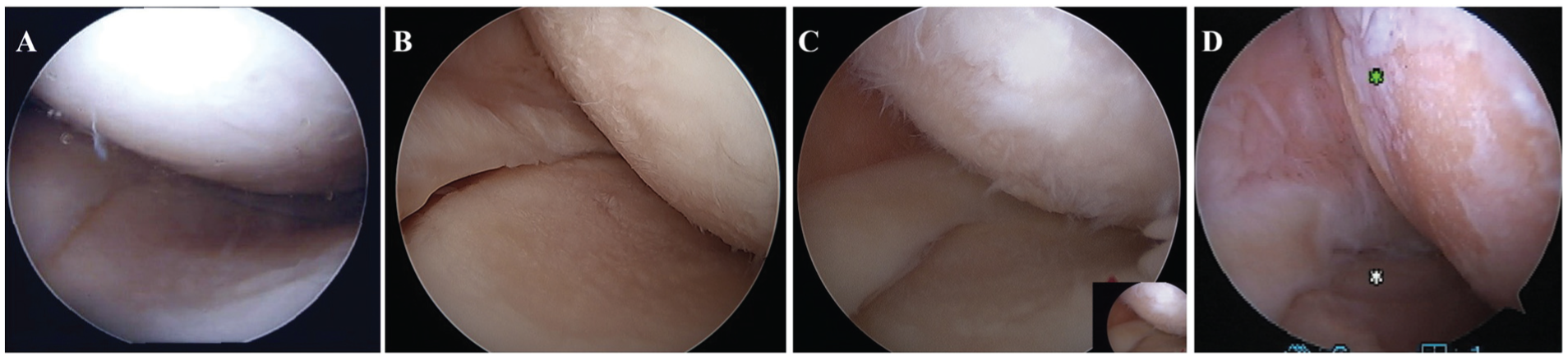
Representative examples: International Cartilage Regeneration & Joint Preservation Society grades (A) 1, (B) 2, (C) 3, and (D) 4.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation, whereas categorical variables are presented as frequency and percentage. Differences in baseline characteristics and radiographic parameters among the 3 groups were analyzed using 1-way analysis of variance (ANOVA) for continuous variables and the chi-square test for categorical variables. The correlation between 2 continuous variables was evaluated using Pearson correlation analysis. Differences in cartilage status (improved, stable, or worsened) among groups were analyzed using the chi-square test.
To evaluate differences in the change in JLCA (ΔJLCA) between the 3 morphological groups, a repeated-measures ANOVA (RM-ANOVA) was performed with time (preoperative vs postoperative) as the within-patient factor and morphology group as the between-patient factor. When a significant interaction effect was detected, post hoc pairwise comparisons with Bonferroni correction were performed to compare ΔJLCA among the 3 groups. A P value <.05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 31.0.0.0; IBM Corp).
Results
A total of 186 patients were included in this study, consisting of 81 men and 105 women, with a mean age of 60.3 ± 7.1 years and a mean body mass index (BMI) of 27.5 ± 3.8 kg/m2. The mean WBL ratio shifted from 15.0% ± 14.3% preoperatively to 63.2% ± 14.8% postoperatively across the tibial plateau.
Based on intra-articular morphology, 60 (32.3%) patients were classified as having the depressed type, 83 (44.6%) the flat type, and 43 (23.1%) the convex type. The corresponding inclination angles for these groups were −6.4°± 2.3°, 0.3°± 1.8°, and 6.2°± 1.8°, respectively. Baseline characteristics, including age, sex distribution, BMI, and osteoarthritis severity, were comparable among the 3 groups. In addition, no significant differences were observed in preoperative radiographic parameters, including MPTA, JLCA, HKA, and WBL ratio. Detailed baseline data are presented in Table 1.
Patient Characteristics and Preoperative Parameters Based on Tibial Morphology a
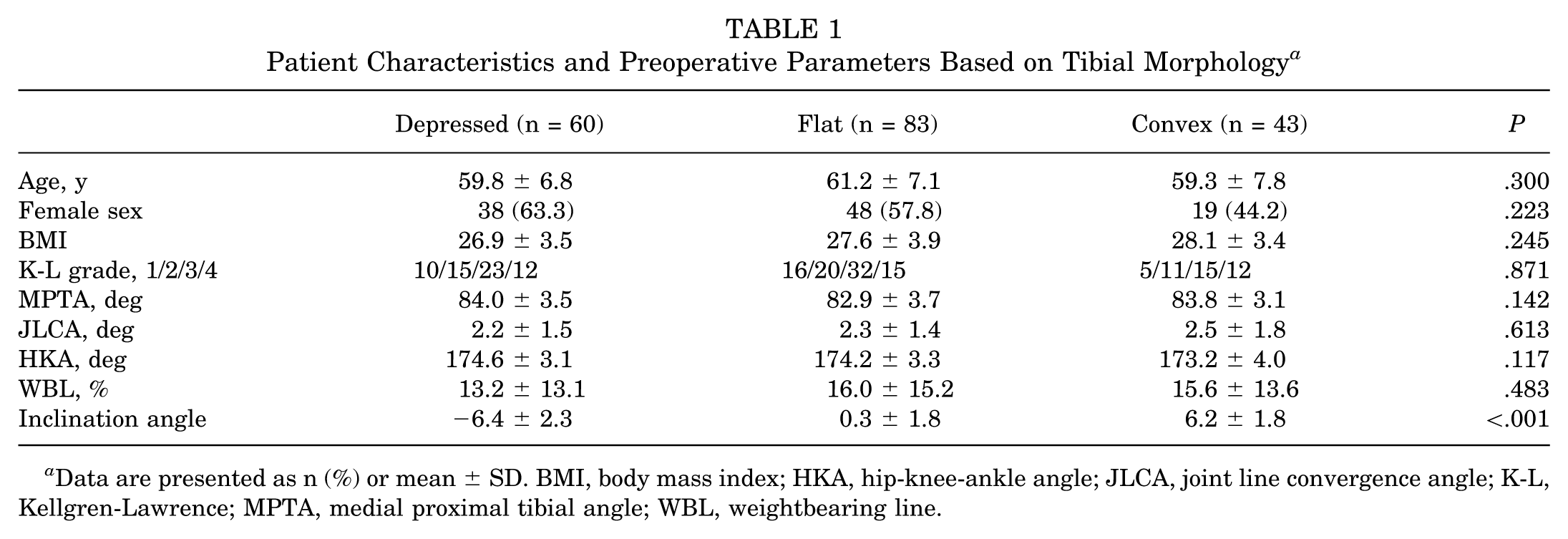
Data are presented as n (%) or mean ± SD. BMI, body mass index; HKA, hip-knee-ankle angle; JLCA, joint line convergence angle; K-L, Kellgren-Lawrence; MPTA, medial proximal tibial angle; WBL, weightbearing line.
Postoperative radiographic parameters, including MPTA, JLCA, HKA, and WBL ratio, were comparable among the 3 groups, with no statistically significant differences observed. Detailed postoperative radiographic results are presented in Table 2. With regard to ΔJLCA, RM-ANOVA demonstrated a significant group × time interaction (P = .016). Subsequent post hoc analysis revealed that the convex type exhibited a significantly greater ΔJLCA compared with both the depressed (P = .018) and flat (P = .049) types. Postoperative KOOS assessments were obtained at a mean follow-up of 41.6 ± 12.2 months. The mean total KOOS and subscale values were comparable among the 3 groups (Table 2). Furthermore, when inclination was analyzed as a continuous variable, it also showed no significant correlation with KOOS (Pearson r = 0.112; P = .13).
Postoperative Parameters and Outcome Based on Tibial Morphology a
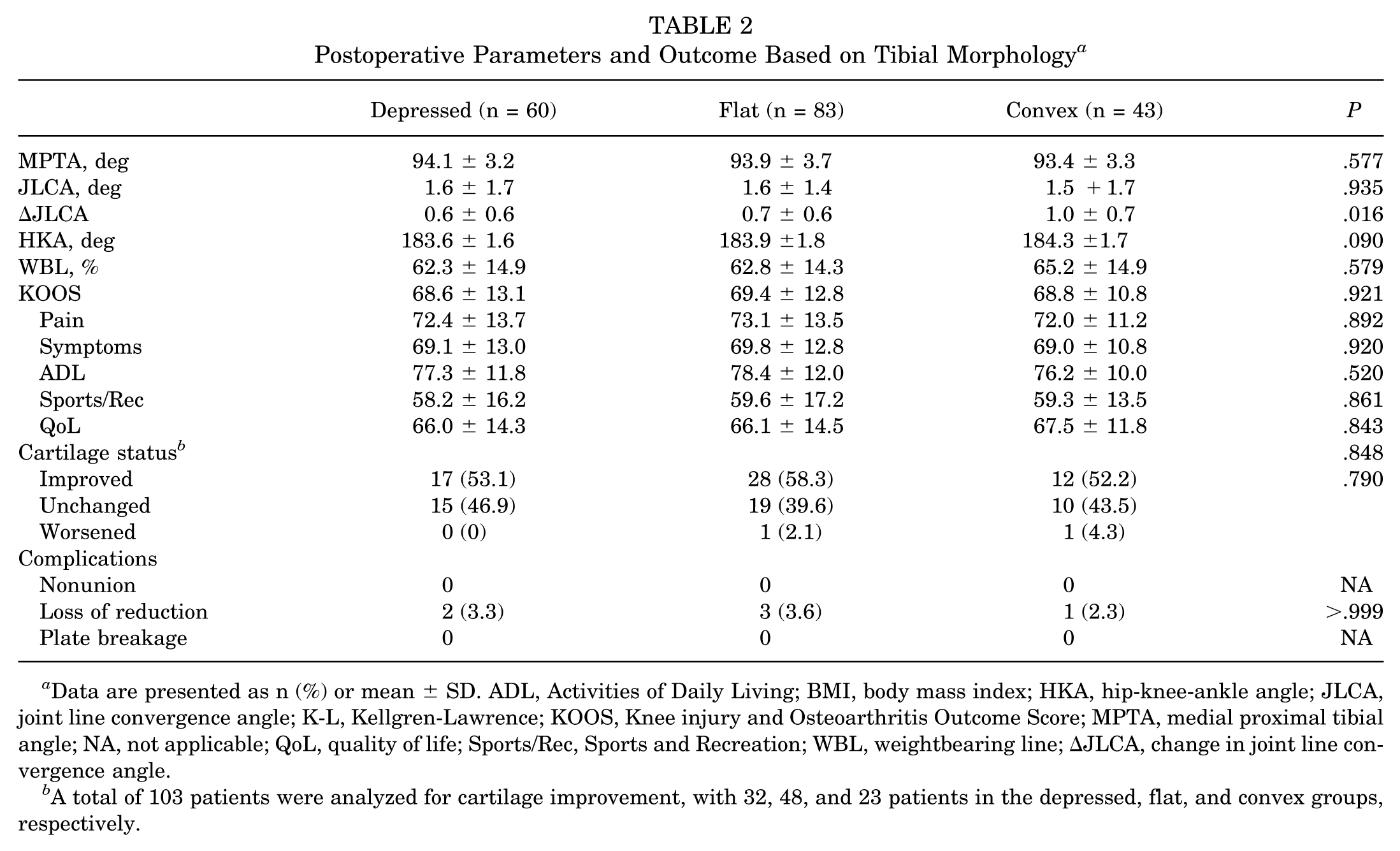
Data are presented as n (%) or mean ± SD. ADL, Activities of Daily Living; BMI, body mass index; HKA, hip-knee-ankle angle; JLCA, joint line convergence angle; K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; MPTA, medial proximal tibial angle; NA, not applicable; QoL, quality of life; Sports/Rec, Sports and Recreation; WBL, weightbearing line; ΔJLCA, change in joint line convergence angle.
A total of 103 patients were analyzed for cartilage improvement, with 32, 48, and 23 patients in the depressed, flat, and convex groups, respectively.
Second-look arthroscopy was performed in 103 patients at a mean follow-up of 18.8 ± 6.8 months after HTO, including 32 (31.1%) depressed-type, 48 (46.6%) flat-type, and 23 (22.3%) convex-type knees. Improvement in ICRS cartilage grade was observed in 53.1%, 58.3%, and 52.2% of patients in the depressed-, flat-, and convex-type groups, respectively. The proportions of unchanged cartilage status were 46.9%, 39.6%, and 43.5%, respectively, whereas worsening was observed in 0%, 2.1%, and 4.3% of patients, respectively. Changes in ICRS grades did not differ significantly among the 3 groups (P = .790). Detailed results are presented in Table 2.
Discussion
The primary finding of this study was that proximal tibial plateau morphology did not significantly influence postoperative clinical outcomes after MOWHTO. To our knowledge, this is the first study to evaluate the association between tibial plateau morphology and postoperative outcomes after HTO. These findings suggest that when tibial plateau morphology falls within the range of normal anatomic variation rather than representing a pathological deformity, MOWHTO can provide satisfactory correction and clinical improvement regardless of whether the morphology is depressed, flat, or convex. Changes in cartilage status were also comparable among the 3 groups.
A previous study suggested that ΔJLCA tends to increase with the magnitude of correction in knees with a convex tibial plateau morphology. 8 Consistent with this observation, our results also demonstrated that ΔJLCA was greater in the convex-type group. However, the magnitude of this increase was relatively small, with a mean difference of <1°. Correspondingly, although the intraoperative correction target was the same among groups, the postoperative WBL ratio in the convex-type knees was a mean of approximately 2% higher than that of the other groups. This finding is consistent with previous reports indicating that a 1°ΔJLCA may correspond to an approximately 2% to 3% shift in the WBL ratio. 1
Mechanistically, this phenomenon may be explained by the fact that the final coronal alignment after HTO is determined not only by the geometric bony correction at the osteotomy site but also by intra-articular and periarticular soft tissue behavior. Correction of varus alignment alters medial-lateral soft tissue tension, ligament balance, and compartmental load distribution, which in turn may influence joint line convergence and be reflected as changes in postoperative JLCA.2,7,23 Nevertheless, the magnitude of ΔJLCA observed in the present study was relatively small, and its impact on overall limb alignment was therefore limited. Given that MOWHTO allows for a relatively broad range of acceptable postoperative alignment without compromising clinical outcomes, such minor variations are unlikely to have meaningful clinical implications. This may explain why neither patient-reported outcomes nor cartilage regeneration differed significantly among the 3 morphological groups.
Another important finding of the present study is that short-term postoperative clinical outcomes and cartilage regeneration were not associated with different tibial plateau morphological types. In recent years, several studies have suggested that the optimal correction target for MOWHTO may not necessarily need to reach the traditional Fujisawa point of 62.5%. Instead, many studies have reported comparable clinical outcomes when the WBL is corrected to approximately 55% of the tibial plateau width.14,15,17 In contrast, insufficient correction, or undercorrection, has consistently been identified as an important factor associated with unfavorable outcomes after HTO.4,9,10,19 In our cohort, the postoperative WBL ratio in all 3 morphological groups remained within the generally accepted target range, indicating that adequate mechanical realignment was achieved regardless of tibial plateau morphology. This may explain why postoperative clinical outcomes and cartilage regeneration were comparable among the depressed, flat, and convex groups in the present study. Therefore, our findings suggest that achieving sufficient coronal alignment correction may be a more critical determinant of surgical success than the underlying morphological subtype of the proximal tibia. From a clinical perspective, these results provide additional reassurance that satisfactory outcomes can be expected across different tibial plateau morphologies, provided that appropriate alignment correction is achieved during MOWHTO.
This study has several limitations. First, the retrospective design may introduce potential selection bias despite the inclusion of consecutive cases. Second, cartilage status was assessed using the ICRS grading system during arthroscopy, which has several inherent limitations. Arthroscopic evaluation was based on available intraoperative images, which may not consistently represent identical anatomic regions across time points. To mitigate this issue, the most severe cartilage lesion identified in each compartment was used for grading at each time point. However, this approach may still be subject to sampling bias and may overestimate the extent of overall cartilage improvement. In addition, grading based on retrospective image review may be subject to interobserver variability and limited reproducibility. Furthermore, changes in ICRS grade do not necessarily reflect true hyaline cartilage regeneration, but may instead represent fibrocartilaginous repair tissue. Therefore, these findings should be interpreted with caution. Third, the classification of tibial plateau morphology was based on radiographic measurements and may be affected by imaging projection or measurement variability. Finally, patients with posttraumatic arthritis were excluded from this study, and therefore extreme tibial plateau morphologies, such as inclination angles >15° or <−15°, were not represented in this cohort. Consequently, the findings of this study may not be generalizable to patients with severe deformities or pathological plateau morphology and should instead be interpreted within the spectrum of relatively normal anatomic variation. Future prospective studies with longer follow-up are warranted to further clarify the influence of tibial plateau morphology on long-term outcomes and survivorship after HTO.
Conclusion
Proximal tibial plateau morphology did not significantly affect clinical outcomes or changes in cartilage status after MOWHTO. Although convex morphology was associated with a slightly greater ΔJLCA, the magnitude of this effect was small and had minimal influence on overall alignment. When appropriate mechanical correction was achieved, satisfactory outcomes were observed regardless of whether the morphology was depressed, flat, or convex. Therefore, tibial plateau morphology alone may not represent a contraindication to MOWHTO.
Footnotes
Final revision submitted April 27, 2026; accepted May 9, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was received from the institutional Ethics Committee of National Taiwan University Hospital (approval No.: 202407168RINA).