
Abstract
Background:
The arthroscopic modified Bröstrom procedure (AMBP) is widely used to treat chronic lateral ankle instability (CLAI). However, in patients with poor or absent ligament remnants, the outcomes may be suboptimal, suggesting a clinical need for alternative techniques.
Purpose:
To introduce all-inside arthroscopic lateral capsular shift (ALCS) and compare outcomes with those for AMBP.
Study design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively analyzed 132 patients (139 ankles) with CLAI who underwent all-inside arthroscopic procedures between November 2017 and December 2022 and had a minimum follow-up of 24 months: 88 ankles with good ligament remnants underwent AMBP, and 51 ankles with poor or absent ligament remnants underwent ALCS. Clinical outcomes were evaluated using visual analog scale pain scores and Foot and Ankle Outcome Scores. Radiological outcomes were evaluated by anterior displacement of the talus and talar tilt angle. Between-group comparisons were performed using parametric or nonparametric tests, with significance set at a P value <.05.
Results:
The 2 groups were comparable in baseline demographics, including age, sex distribution, and follow-up duration, with no significant differences between groups. The mean follow-up was 41.5 months (range, 24-89 months). For both groups, functional scores improved significantly after surgery, with no significant differences between groups in final scores or the proportion of patients who achieved functional score improvements exceeding the minimal important change (all P > .05). Final radiological parameters and degree of correction were also comparable between groups. No significant differences between groups were observed for overall complication rates (P = .725), with 5.7% (95% CI, 2.5%-12.6%) for AMBP group and 7.8% (95% CI, 3.1%-18.5%) for ALCS group, and recurrent instability (P > .999), occurring in 2.3% (95% CI, 0.6%-7.9%) of ankles (n = 2) in AMBP group and in 2.0% (95% CI, 0.3%-10.3%) of ankles (n = 1) in ALCS group.
Conclusion:
Our study showed that ALCS achieved clinical and radiological outcomes comparable to those of AMBP, with low recurrence rates after at least 2 years of follow-up. Our results suggest that ALCS may be a viable operative treatment option for patients with CLAI but poor ligament remnants. Future prospective studies are needed to further validate and generalized the findings of this study.
Keywords
Lateral ankle sprains are common injuries that typically respond well to nonoperative treatment, including protected mobilization, muscle strengthening, and proprioceptive rehabilitation. However, as many as 30% of acute lateral ankle sprains progress to chronic lateral ankle instability (CLAI), characterized by lateral ankle pain, the sensation that the ankle is giving way, and recurrent ankle sprain events. 34
When nonoperative treatment is ineffective, operative treatment can be considered. The most frequently performed surgical procedure for treating CLAI is the modified Bröstrom procedure (MBP), during which the anterior talofibular ligament (ATFL) is anatomically repaired and the inferior extensor retinaculum (IER) is plicated, leading to favorable outcomes and long-term satisfaction rates as high as 90%. 34 Recently, the all-inside arthroscopic MBP (AMBP) has gained popularity due to its minimally invasive nature, which reduces soft tissue trauma and postoperative pain, resulting in early recovery.1,12,31 Despite the generally favorable outcomes after AMBP, whether surgical outcomes are impacted by poor ATFL remnant quality, which can result from severe ligament attenuation or the excision of a large os subfibulare, remains controversial.7,15,24,36,38 The need for additional reinforcement or an alternative procedure has been suggested in several studies in cases with poor quality or absent ATFL remnant.15,19,20,33
In response to these concerns, various techniques have been suggested to address CLAI in patients with insufficient or absent ATFL remnants.4,20,23,33 In this context, the present study introduces an all-inside arthroscopic lateral capsular shift (ALCS) technique that can be used for CLAI patients with poor ATFL remnant. The purpose of this study was to compare the short- to intermediate-term clinical and radiological outcomes of ALCS with those of the conventional AMBP. We hypothesized that ALCS would show significant clinical and radiological improvement, and outcomes would be comparable to those of AMBP.
Methods
This study was approved by our institutional review board, which waived the requirement for informed consent due to the retrospective nature of the study (approval No.: 3-2025-0273).
Between November 2017 and December 2022, 160 patients (171 ankles) underwent all-inside arthroscopic procedures to treat CLAI. All procedures were performed by the senior author (S.H.H.) at a single center. Indications for surgery were persistent CLAI with recurrent ankle sprains and a giving-way sensation after at least 6 months of nonoperative treatment, including peroneal muscle strengthening and proprioceptive rehabilitation, and a positive inversion or anterior drawer test. Exclusion criteria were large osteochondral lesions of the talus (≥1.5 cm2); inflammatory arthritis; neuromuscular disorders; diffuse arthritic changes; previous surgery or ankle fracture, other than an avulsion fracture of the tip of the distal fibula on the ipsilateral ankle; obvious cavovarus deformity; and follow-up data for <24 months (Figure 1). Patients were divided into 2 groups according to the surgical technique used.
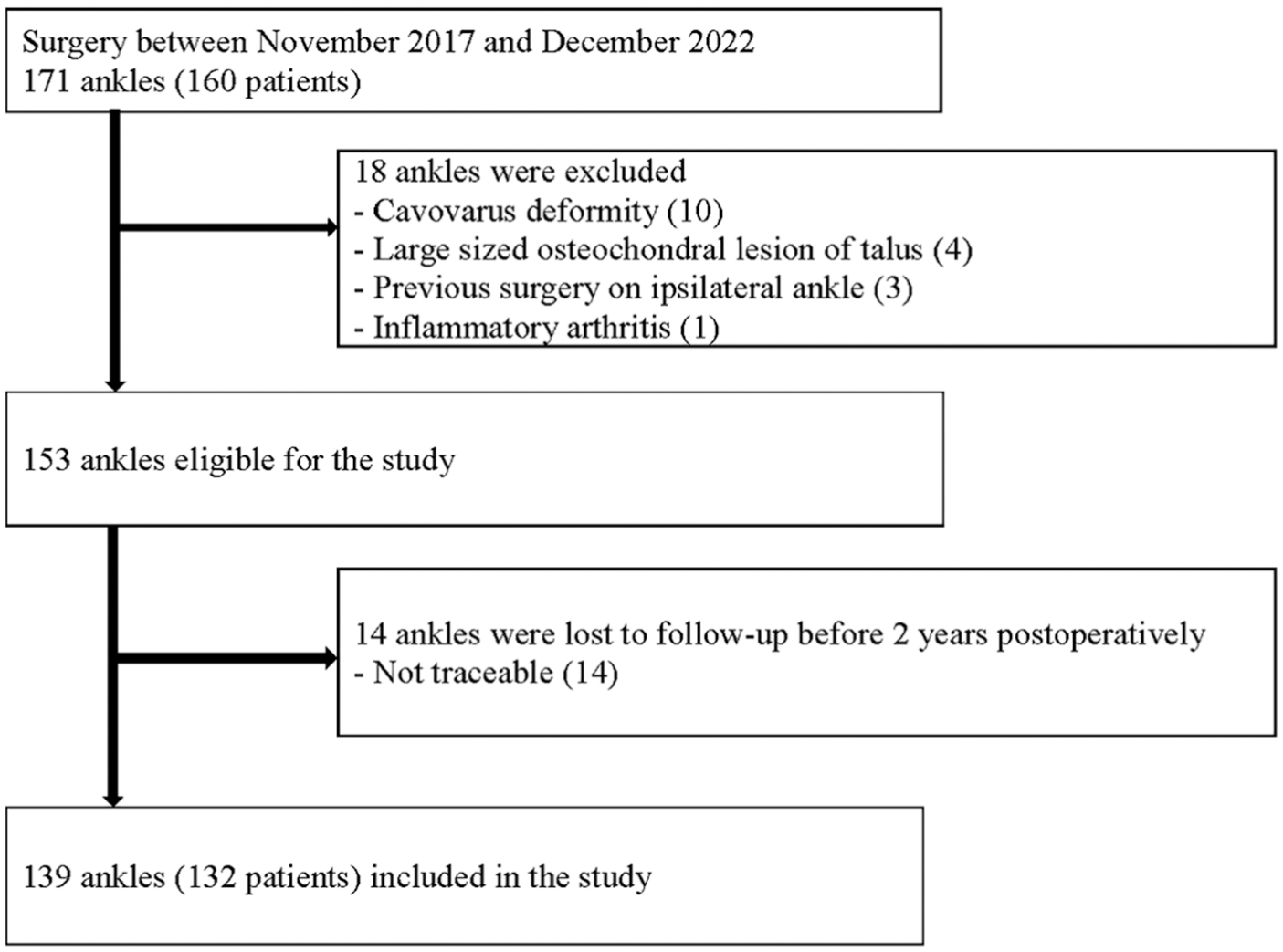
Flowchart of patients participating in this study.
Surgical Technique
Arthroscopic Examination
Under general or spinal anesthesia, noninvasive ankle joint distraction was applied, standard anteromedial and anterolateral portals were made, and a 2.7-mm, 30°-angled arthroscope was inserted to evaluate concomitant intra-articular lesions, such as osteochondral lesions, soft tissue impingement, synovitis, and prominent bony spurs. Any identified intra-articular lesions were treated before the ligament repair procedure began. When syndesmotic widening was accompanied by soft tissue impingement, arthroscopic debridement was performed without syndesmotic fixation. An accessory anterolateral (AAL) portal was made 1.0 to 1.5 cm anterior to the tip of the distal fibula. A motorized shaver was introduced through the AAL portal to debride synovial tissues. When an os subfibulare was identified, its relationship with the surrounding soft tissues was first assessed using an arthroscopic probe. The ossicle was then excised using a motorized shaver and arthroscopic grasper while taking care to avoid injury to the ligament remnant. 8 In cases with relatively large ossicles, fragmentation with a punch was performed to facilitate removal. Arthroscopic evaluation was then used to grade the ATFL remnant, as described in a previous study (Table 1). 30 If the ATFL remnant was scored as grade 1 or 2, indicating a good remnant, AMBP was indicated. If the ATFL remnant was absent or severely attenuated (grade 3 or 4 or after excision of a large os subfibulare), ALCS was indicated.
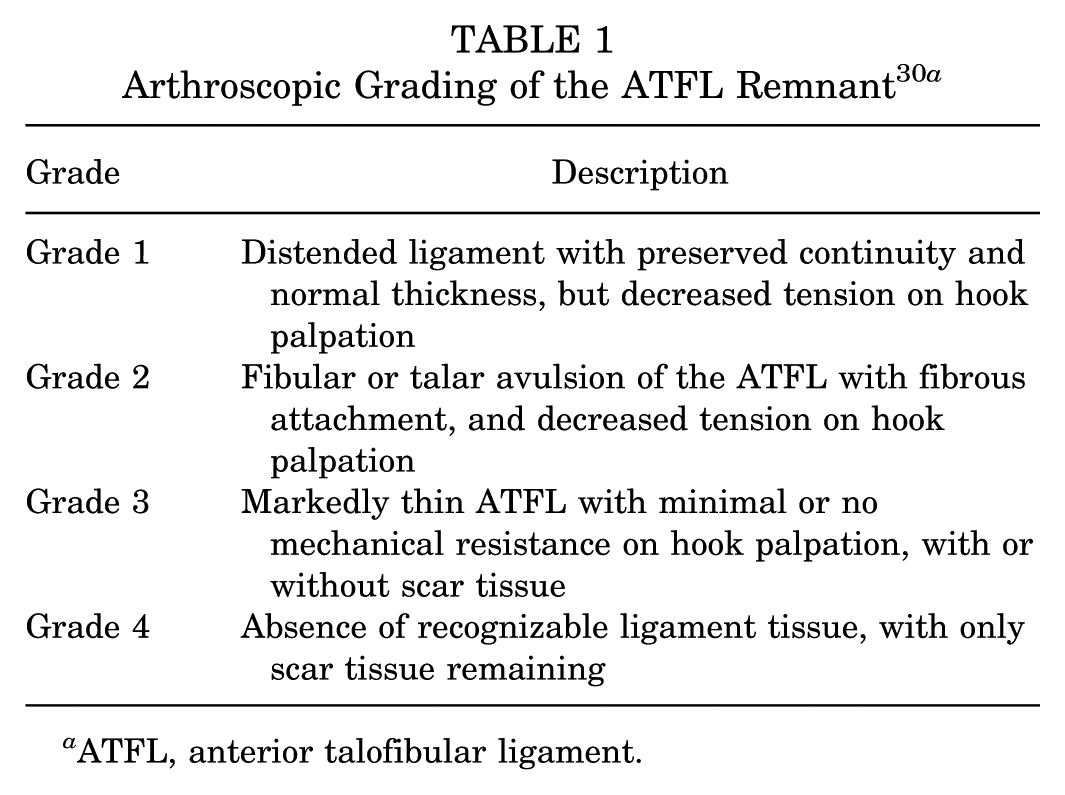
ATFL, anterior talofibular ligament.
Arthroscopic MBP
AMBP was performed using a modified lasso-loop stitch, as previously described.17,29 A double-loaded suture anchor (3.0 × 14.5 mm, SutureTak; Arthrex) was inserted on the fibular footprint of the ATFL, just proximal to the fibular obscure tubercle, taking care to avoid penetrating the articular surface of the lateral gutter. An 18-gauge needle carrying a 2-0 polydioxanone (PDS; Ethicon) suture loop was passed through the AAL portal, penetrating the inferior margin of the visible ATFL remnant and directed toward the lateral aspect of the talus. The loop was retrieved via a grasper through the AAL portal. One limb of the suture anchor was shuttled through the ATFL remnant by passing the suture into the polydioxanone loop and pulling the opposite end of the loop out through the AAL portal. The pulled anchor suture was then looped through the remaining ligament, and the remaining anchor suture thread was passed into this loop. Subsequently, the loop was rotated to form a second loop, and the same suture limb was passed into the second loop. Gentle traction applied to the suture strand was used to tighten the loops around the ligament. Arthroscopic visualization was used to tie a secure knot and confirm that the ATFL stump was firmly attached to its fibular footprint when the ankle was positioned with a slight eversion. To plicate the IER, a mosquito clamp was inserted through the AAL portal to bluntly dissect the IER subcutaneously, and a free needle was advanced through the AAL portal to penetrate the IER approximately 1.5 to 2.0 cm distal to its edge. One remaining suture limb was then shuttled through the IER, and the final limb was passed approximately 1 cm away from the previous limb. Both limbs were retrieved through the AAL portal by subcutaneous dissection and were tied securely.
Arthroscopic Lateral Capsular Shift
A 3.0-mm, double-loaded suture anchor was inserted just proximal to the fibular obscure tubercle. When this landmark could not be clearly identified after large ossicle excision, the anchor was inserted at approximately one-third of the distance between the inferior tip and the anterior tubercle on the anterior tubercle of the fibula.14,16 A lasso needle containing a loop wire was inserted through the AAL portal to penetrate the posterolateral tip of the distal fibula just anterior to the superior margin of the peroneal tendons, maintaining a trajectory away from the course of the sural nerve. 1 One limb of the suture anchor was loaded onto the loop and shuttled through the posterolateral tip of the distal fibula (Figure 2), and the remaining suture limbs were shuttled through the anterolateral capsule and IER, similar to the method used for AMBP. These sutures were dissected subcutaneously, brought through the AAL portal to engage the anterior capsule below the fibular obscure tubercle (Figure 3), and firmly tied under arthroscopic visualization to secure the capsule and IER to the fibula (Figure 4).
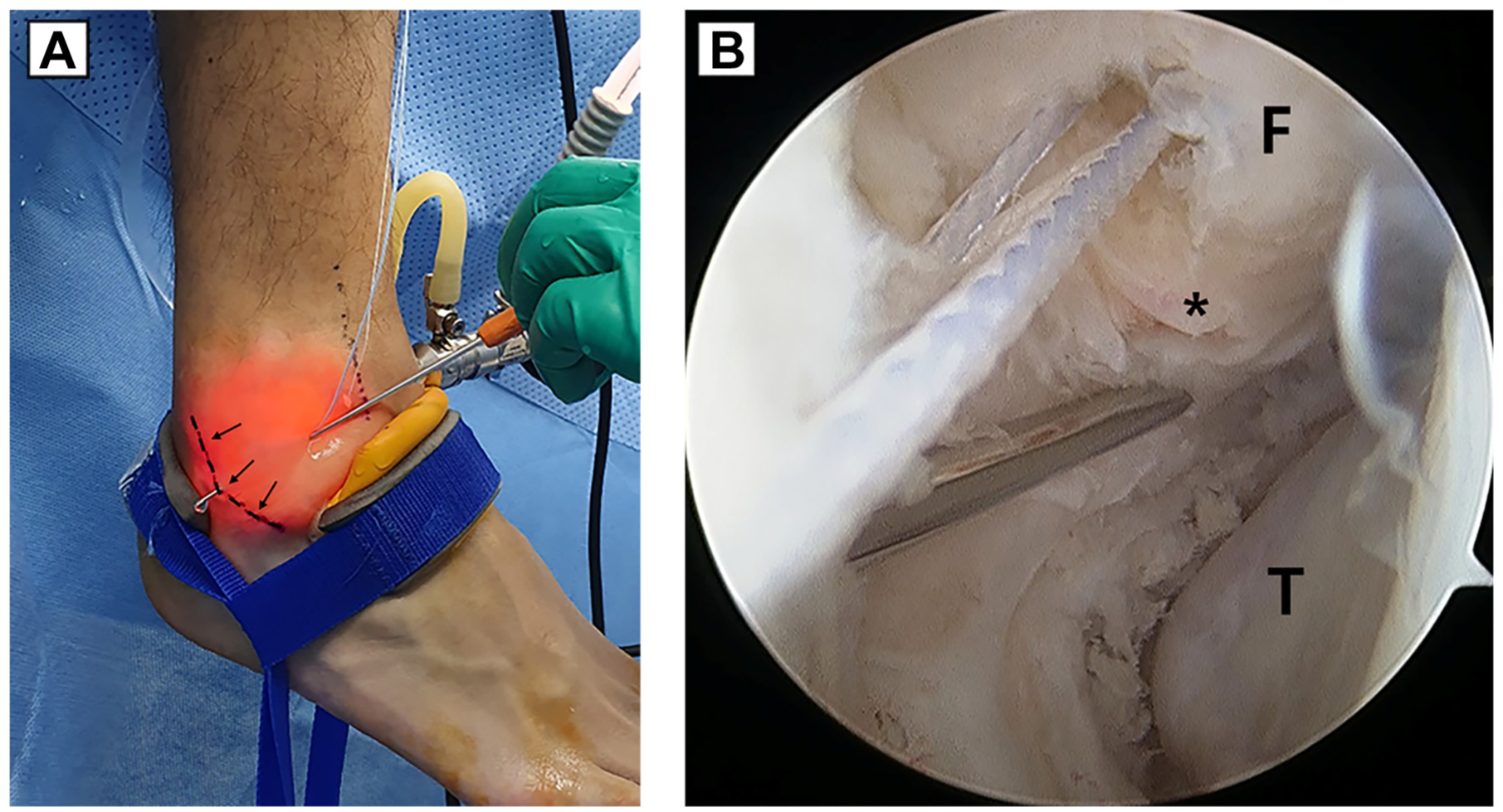
(A) Penetration through the inferolateral ankle capsule. The dotted line indicates the superior border of the peroneal tendons, and the arrow highlights this structure. (B) Corresponding arthroscopic view from the anteromedial portal. The asterisk indicates the fibular obscure tubercle. F, fibula; T, talus.
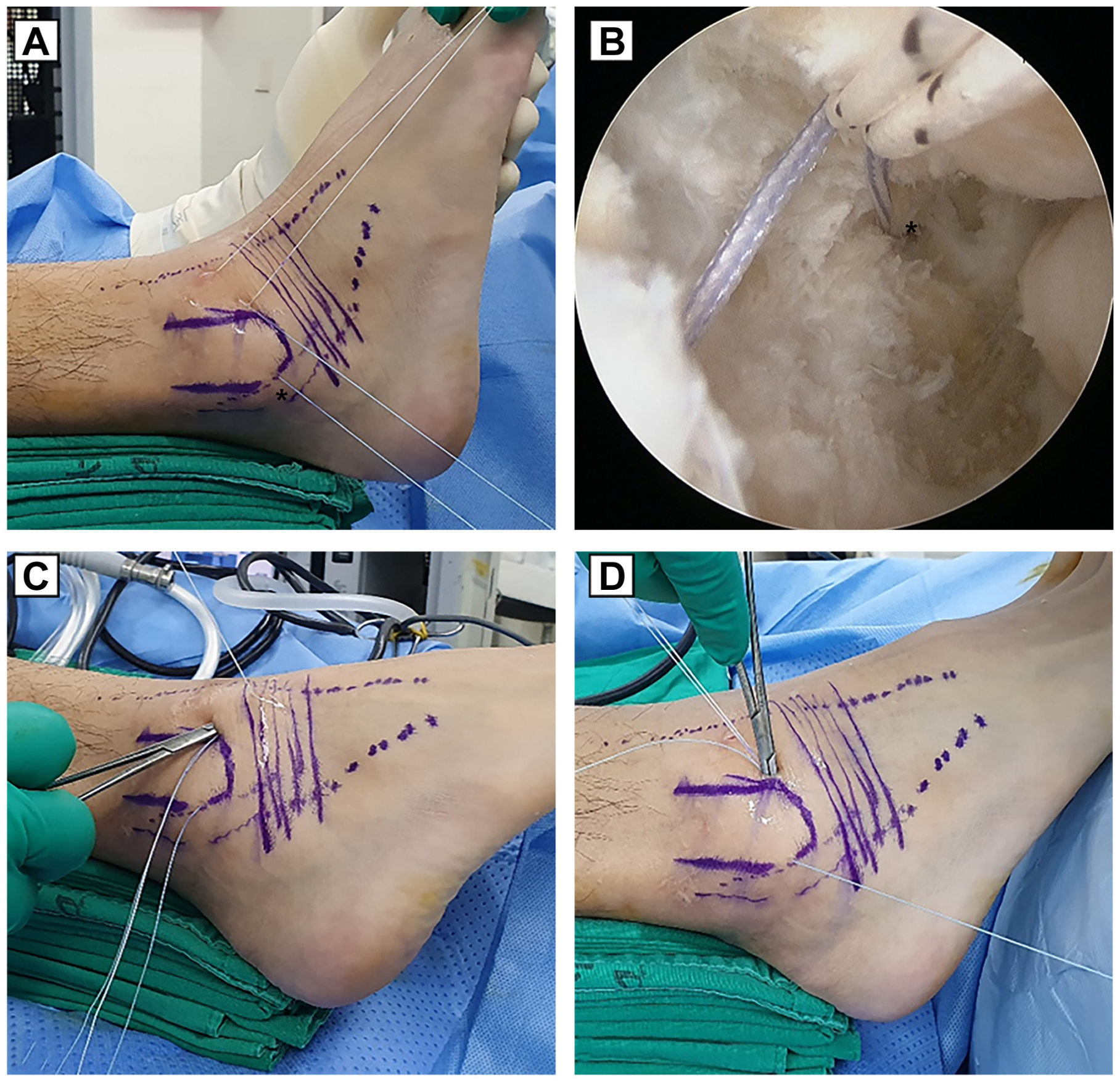
(A) Completion of suture shuttling through the inferolateral capsule, just before passage through the anterolateral capsule and inferior extensor retinaculum. The asterisk indicates the site of suture passage through the inferolateral capsule. The suture is passed just anterior to the peroneal tendons to avoid the sural nerve. (B) Corresponding arthroscopic view demonstrating suture passage through the inferolateral capsule (asterisk), corresponding to the same point indicated in panel A. (C) Subcutaneous dissection through the accessory anterolateral portal to retrieve sutures passed through the anterolateral capsule and inferior extensor retinaculum. (D) Subcutaneous dissection through the accessory anterolateral portal to retrieve sutures passed through the inferolateral capsule.
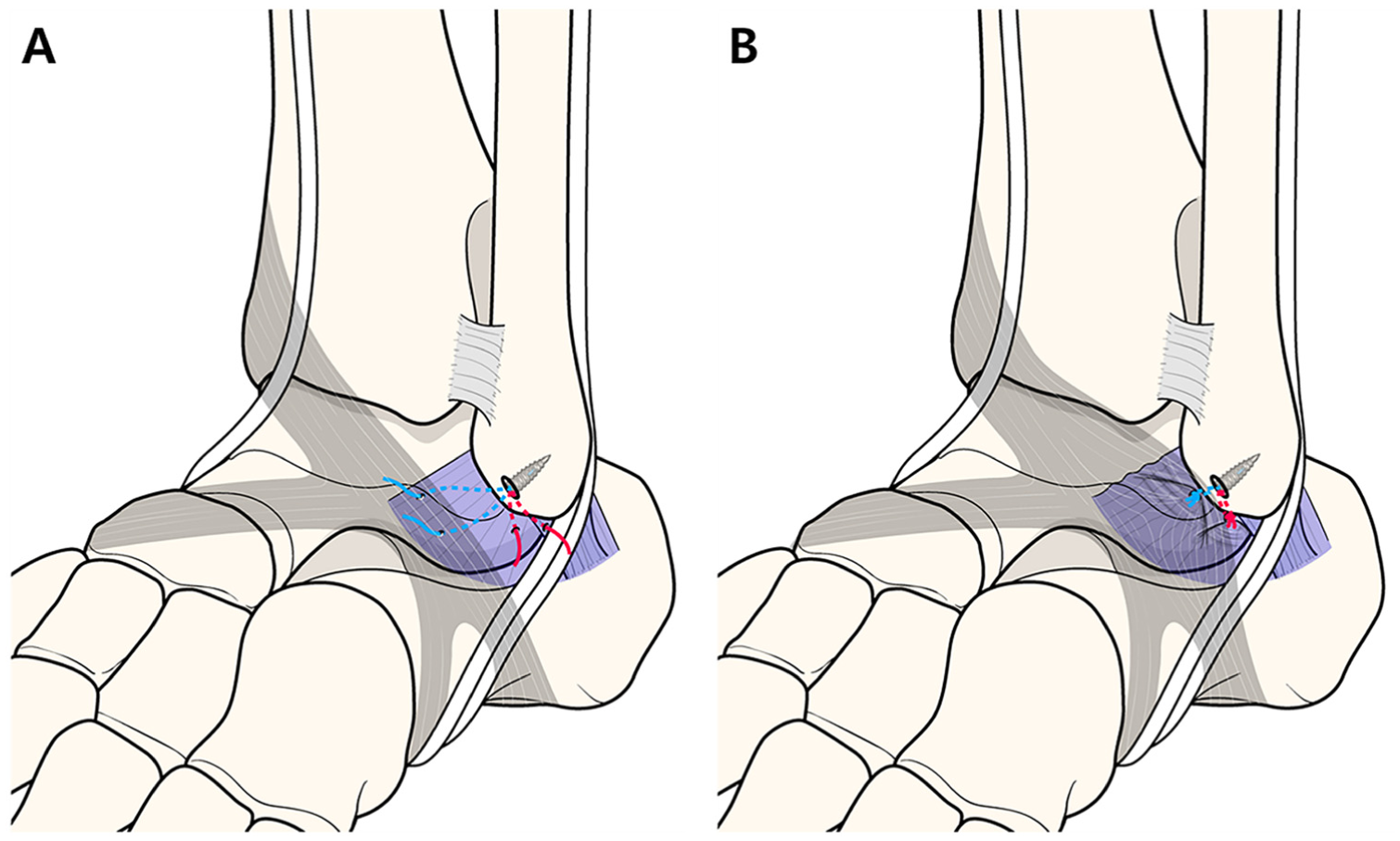
(A) Schematic illustration showing suture passage through the inferolateral capsule, anterolateral capsule, and inferior extensor retinaculum. (B) Final configuration after firm suture tying, demonstrating stabilization of the lateral capsular structures relative to the fibula.
Postoperative Care
The same postoperative management protocol was applied to both groups. A short leg cast was applied after surgery and remained in place for 4 weeks, followed by the use of an Air Stirrup brace (Seoul Prosthesis Co, Ltd.) for 2 months. Tolerable weightbearing was permitted starting 2 weeks after surgery in all patients. Range of motion, proprioceptive exercises, and peroneal muscle strengthening exercises were started 4 weeks after surgery. Return-to-sports activities, including sport-specific training, was permitted from 3 months after surgery, depending on clinical recovery.
Clinical Evaluation
Baseline patient information was collected from our institution's electronic medical records system. All outcomes were assessed by 2 independent observers who were blinded to the purpose of this study. To evaluate functional outcomes, the Foot and Ankle Outcome Score (FAOS) 27 and visual analog scale pain score were assessed and recorded at various time points: preoperatively; 3, 6, and 12 months after surgery; and annually thereafter. The FAOS is a validated and disease-specific measurement tool for CLAI. 27 In patients who underwent bilateral procedures, clinical scoring was performed separately for each ankle after the patient was thoroughly informed and asked to assess each side independently. All intraoperative findings, postoperative complications, and reoperations were recorded.
Radiological Evaluation
Preoperative weightbearing anteroposterior and lateral radiographic imaging and stress radiography using a TELOS device with a load of 150 N, as well as magnetic resonance imaging, were performed to assess ligament status and concomitant intra- or extra-articular pathologies. The talar tilt angle, defined as the angle between the articular surface of the distal tibia and the talar dome, was measured on the varus stress view. 10 Anterior talus displacement, defined as the shortest distance between the talus and the most distal point of the posterior lip of the distal tibia, was measured on the anterior drawer stress view. 10 Ankle radiographs under weightbearing conditions were taken 1, 3, 6, and 12 months after surgery and annually thereafter. Stress radiographs were taken every 12 months after surgery. All radiographic measurements were performed by 2 independent, fellowship-trained foot and ankle surgeons (Y.K.Y. and D.W.S.) who were not involved in patient care and were blinded to both patient information and each other's findings, to avoid potential bias. Interobserver reliability was assessed using interclass correlation coefficients, which were interpreted as poor (<0.5), moderate (0.5-0.75), good (0.76-0.9), or excellent (>0.9).
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics Version 26.0 (IBM). The Kolmogorov-Smirnov test was used to assess the normality of the data distribution for each variable. Paired t tests or Wilcoxon signed-rank tests were used to compare preoperative and postoperative values. Intergroup differences in continuous variables were analyzed using the Student t test or Mann-Whitney U test, whereas differences in categorical variables were assessed using the chi-square test or Fisher exact test. No missing data were present among the cases; therefore, no imputation or deletion methods were applied. Significance was set at a P value <.05.
A post hoc power analysis was conducted to determine whether the sample size was sufficient to detect a minimal important change (MIC) in FAOS subscale values. 28 Using the observed preoperative standard deviations and the actual group sizes, we calculated effect sizes from 0.833 to 1.328, corresponding to post hoc powers of 0.997 to 1.000, respectively, at a significance level of .05. These results indicate that the sample size of the present study was sufficient.
Results
Baseline patient characteristics are summarized in Table 2. The final cohort included 139 ankles in 132 patients, with a mean follow-up period of 41.5 months (range, 24-89 months). The AMBP group included 88 ankles, and the ALCS group included 51 ankles. Among the 51 ankles in the ALCS group, 27 (53.0%) were indicated for ALCS due to severe ATFL remnant attenuation, whereas 24 (47.0%) were indicated for ALCS after the excision of a large os subfibulare. The ALCS group showed significantly higher prevalences of prominent bony spurs on the anterior lip of the distal tibia (P = .01) and os subfibulare (P < .001) than the AMBP group, but all other factors and follow-up durations were comparable between groups.
Clinical Characteristics of Study Patients a
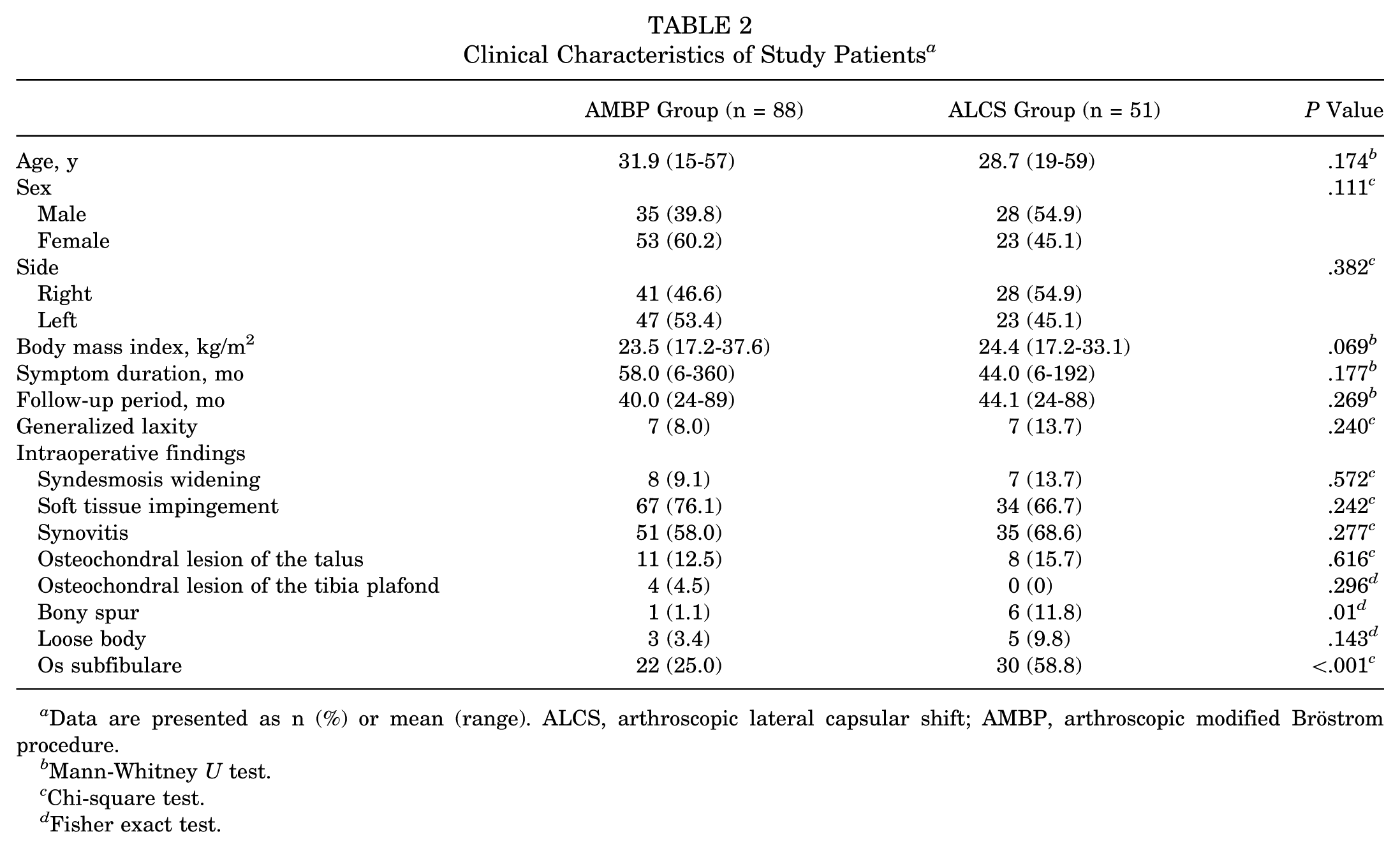
Data are presented as n (%) or mean (range). ALCS, arthroscopic lateral capsular shift; AMBP, arthroscopic modified Bröstrom procedure.
Mann-Whitney U test.
Chi-square test.
Fisher exact test.
Clinical Outcomes
Preoperative and postoperative clinical scores are shown in Table 3. All preoperative scores were comparable between groups, and all scores improved significantly from preoperatively to the last follow-up visit for both groups (all P < .001), with mean improvements in all FAOS subscale values exceeding the reported MICs for CLAI (21.8 for pain, 18.9 for activities of daily living, 19.9 for sports, and 25.5 for quality of life). 28 For all FAOS subscales with established MIC thresholds, the proportions of patients who achieved functional score improvements exceeding the MIC were comparable between groups, with no significant differences observed. At the last follow-up, all scores were comparable between groups.
Comparison of Functional Outcomes Between 2 Groups a
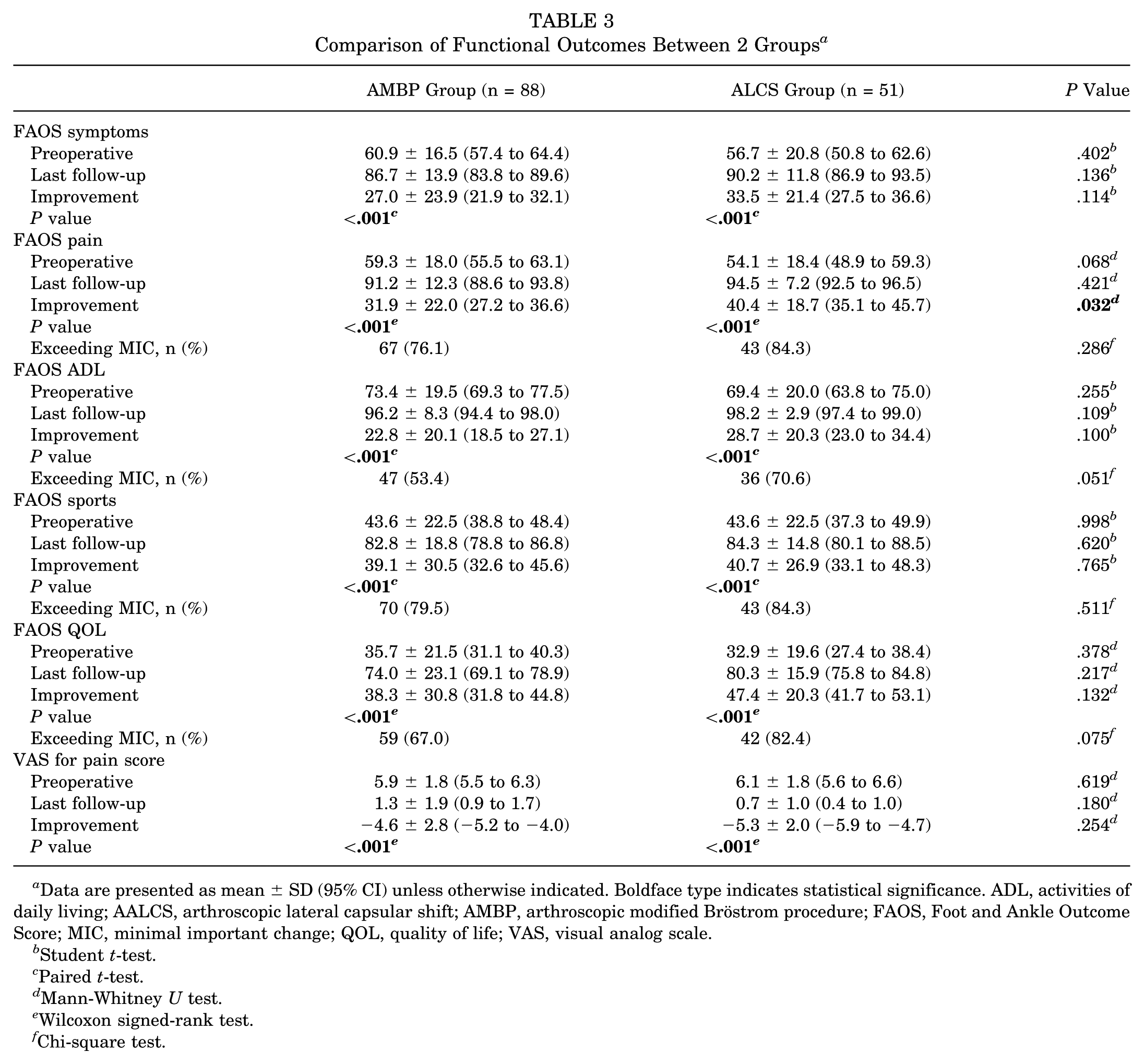
Data are presented as mean ± SD (95% CI) unless otherwise indicated. Boldface type indicates statistical significance. ADL, activities of daily living; AALCS, arthroscopic lateral capsular shift; AMBP, arthroscopic modified Bröstrom procedure; FAOS, Foot and Ankle Outcome Score; MIC, minimal important change; QOL, quality of life; VAS, visual analog scale.
Student t-test.
Paired t-test.
Mann-Whitney U test.
Wilcoxon signed-rank test.
Chi-square test.
Radiological Outcomes
The radiological outcomes are summarized in Table 4. The interobserver reliability for radiographic measurements was excellent, with interclass correlation coefficients of 0.980 (95% CI, 0.895-0.993) for anterior talar displacement and 0.985 (95% CI, 0.927-0.995) for talar tilt. The mean preoperative anterior talar displacement was 8.2 mm in the AMBP group and 7.8 mm in the ALCS group. The mean preoperative talar tilt was significantly larger in the ALCS group (11.7°) than in the AMBP group (10.0°) (P = .031). At the last follow-up visit, both groups showed significant improvements in all radiological parameters (all P < .001). The mean postoperative anterior talar displacement was 5.6 mm in the AMBP group and 5.5 mm in the ALCS group, and the mean postoperative talar tilt was 6.1° in the AMBP group and 7.1° in the ALCS group. All final radiological parameters and degree of correction were comparable between groups.
Comparison of Radiological Outcomes Between Groups a
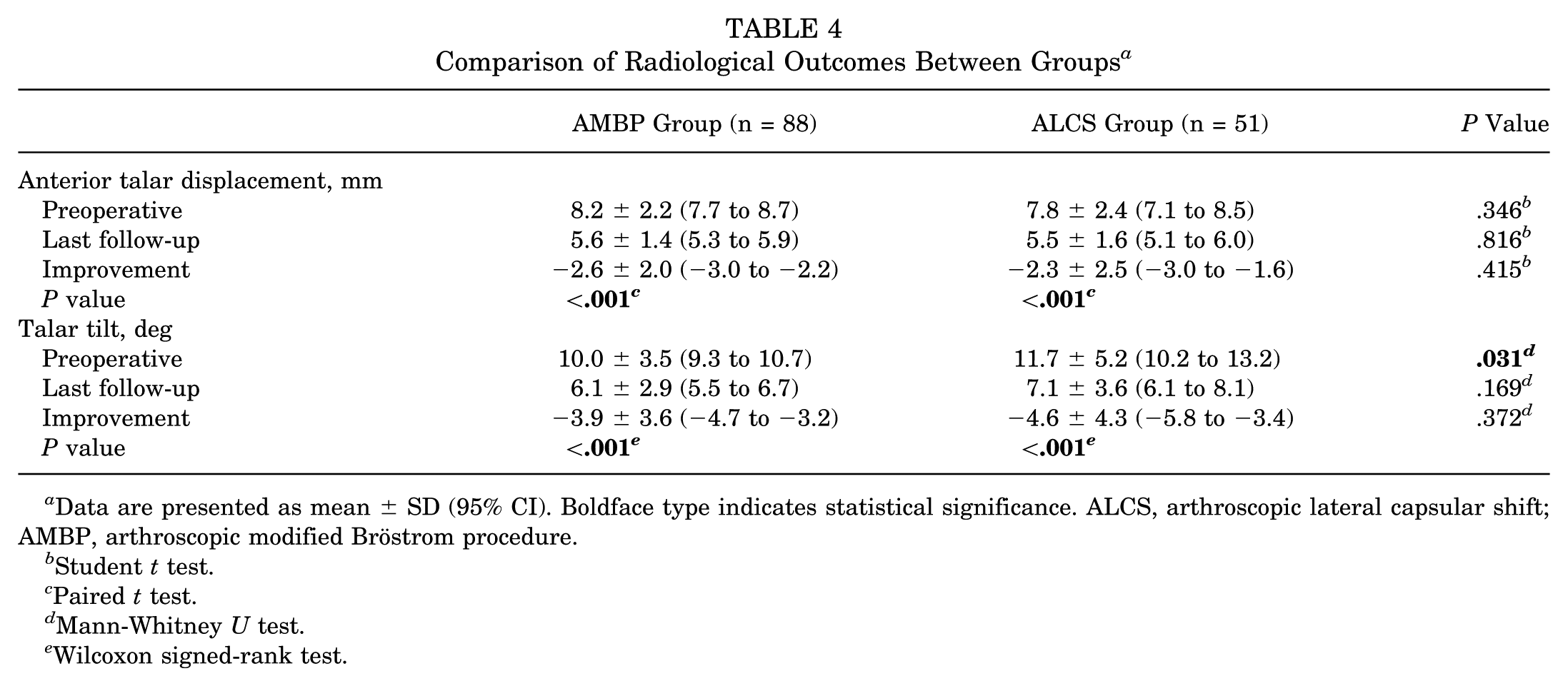
Data are presented as mean ± SD (95% CI). Boldface type indicates statistical significance. ALCS, arthroscopic lateral capsular shift; AMBP, arthroscopic modified Bröstrom procedure.
Student t test.
Paired t test.
Mann-Whitney U test.
Wilcoxon signed-rank test.
Complications, Recurrence, and Reoperations
The overall complication rate was 6.5% (95% CI, 3.4%-11.8%) with no significant difference between groups (P = .725) (Table 5). Recurrent instability, defined as patient-reported persistent giving-way sensation and/or ≥2 episodes of ankle inversion injuries after surgery, occurred in 2 ankles (2.3% [95% CI, 0.6%-7.9%]) in the AMBP group and 1 ankle (2.0% [95% CI, 0.3%-10.3%]) in the ALCS group, without statistical significance (P > .999). No patients with recurrent instability wanted revision surgery during the follow-up period. Superficial peroneal nerve irritation was observed in 3 ankles (3.4%) in the AMBP group and 2 ankles (3.9%) in the ALCS group, all of which resolved within 6 months, including 4 with spontaneous resolution and 1 with pregabalin treatment. One patient (2.0%) in ALCS group underwent prominent knot removal. No superficial or deep infections were observed.
Complications and Reoperations a
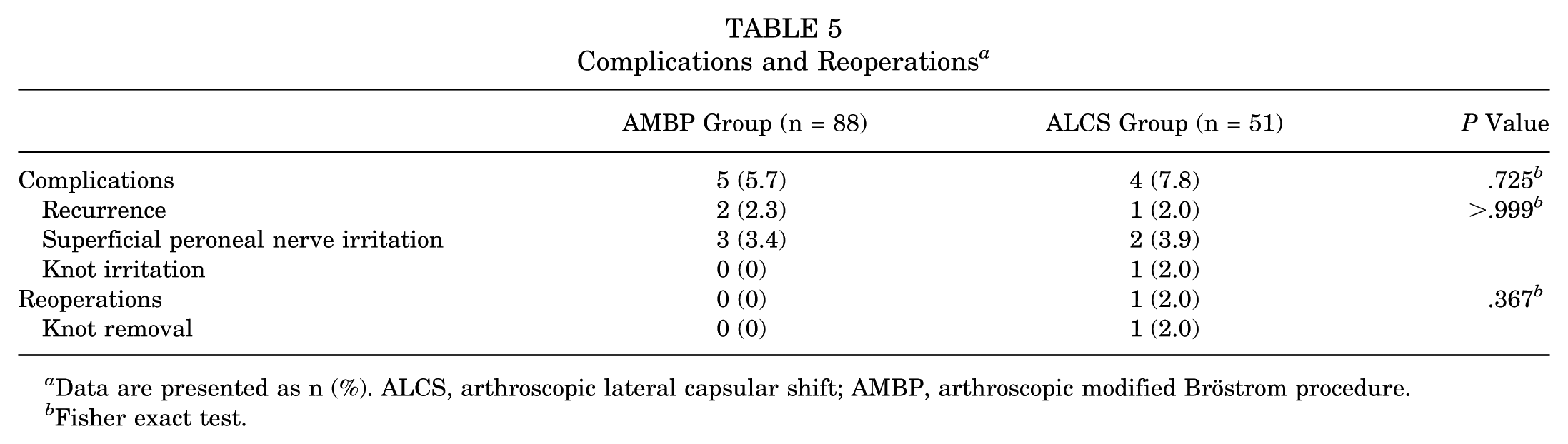
Data are presented as n (%). ALCS, arthroscopic lateral capsular shift; AMBP, arthroscopic modified Bröstrom procedure.
Fisher exact test.
Discussion
The major findings of our study showed that 2 all-inside arthroscopic procedures for CLAI—AMBP and ALCS—yielded satisfactory clinical and radiological outcomes, with similarly low recurrence (2.3% vs 2.0%) and total complication (5.7% vs 7.8%) rates. Based on these findings, all-inside ALCS may represent a reasonable surgical option for CLAI with poor or absent ATFL remnants.
Whether ATFL remnant quality affects lateral ligament repair outcomes in cases of CLAI remains controversial. In their retrospective analysis of 60 ankles that underwent MBP, Park et al 25 demonstrated similar functional outcomes in all FAOS subscales, regardless of the presence of ATFL remnant on ultrasound, magnetic resonance imaging, and arthroscopy. Several authors have reported favorable clinical and radiological outcomes after MBP with os subfibulare excision, regardless of the size of the os subfibulare, implying that the quantity of ATFL remnant does not affect surgical outcomes.2,5 By contrast, Kim et al 11 reported that anterior stability was not achieved after MBP with the excision of a large-sized os subfibulare, stating that the excision of a large os subfibulare introduces a large ATFL defect that could not be augmented and suggesting that osteosynthesis to replace the excised os subfibulare or other ligament reconstruction method should be used instead of MBP in cases with ossicle excision.11,37 With respect to the all-inside AMBP, Feng et al 7 retrospectively compared outcomes among patients with at least 2 years of follow-up after undergoing all-inside AMBP with and without direct ATFL remnant repair and found that both groups had similar functional scores, anterior stability, and rates of return to preoperative sport levels. Similarly, Park et al 24 conducted a retrospective analysis of 135 patients who underwent AMBP using the knotless anchor technique and were classified into 4 groups according to the arthroscopic grade of ATFL remnants; they found favorable clinical and radiological outcomes regardless of ATFL remnant quality, including comparable final functional Karlsson scores, FAOS subscale values, anterior talar translation and talar tilt measures, and recurrence rates. Contrary to these results, Luthfi et al 15 retrospectively analyzed 56 arthroscopic ATFL repair procedures with and without calcaneofibular ligament (CFL) repair, reporting that poor ATFL remnant quality was more frequently observed in ankles that experienced recurrence after surgery, indicating that a poor ATFL remnant may represent a risk factor for recurrent instability after arthroscopic ATFL repair. Yoshimoto et al 38 reviewed 68 ankles treated with AMBP using the lasso-loop stitch, reporting similar functional scores between a group with poor ATFL remnants and a group with intact ATFL remnants; however, the recurrence rate was significantly higher for the group with poor ATFL remnants than for the group with intact ATFL remnants. Most recently, Won et al 36 compared outcomes for patients with at least 2 years of follow-up after arthroscopic ATFL repair according to ATFL remnant grade and found that the poor remnant group (n = 64) had significantly lower FAOS sports values, inferior posturography scores, higher rates of ATFL retear on magnetic resonance imaging, and higher rates of recurrence than the good remnant group (n = 77). Because a key procedure of arthroscopic ligament repair involves suturing the superior ATFL fascicle on the articular side, a poor or absent ATFL remnant may be more detrimental for AMBP than for MBP, which allows for easier concomitant lateral capsule plication and CFL repair. Therefore, surgical options that allow for additional plication could be worth considering when ATFL remnants are poor or absent.
Several studies have demonstrated the role of the anterolateral ankle capsule in lateral ankle stability. For example, serial sectioning of the ATFL, CFL, and anterolateral capsule in a cadaveric study revealed that anterolateral capsule sectioning induced approximately 30% of lateral ankle instability, independent of the contributions of the ATFL and CFL. 3 Anterolateral joint capsule thickening is frequently observed in patients with CLAI, suggesting that the anterolateral capsule plays a compensatory stabilizing role in ankles with lateral ligament insufficiency. 32 This possibility is further supported by a recent cadaveric study, conducted by Kakegawa et al, 9 which found that 42% of specimens demonstrated an inferior fascicle of the ATFL that was integrated with the joint capsule and showed anatomic continuity with both the CFL and the posterior talofibular ligament. 9 These findings suggest that the lateral capsule functions as a structural and functional complex with all 3 lateral ligaments. Moreover, capsule loosening has been posited to contribute to recurrence after arthroscopic ATFL repair. 21 These anatomic relationships provide the theoretical rationale for plicating this region during lateral ligament complex stabilization, particularly with the potential to reinforce the inferior fascicle of the ATFL and the CFL. A previous study described augmenting fibrotic tissue, the superior anterolateral capsule, and the IER in ankles with poor ATFL remnants, whereas the ALCS technique also plicates the inferolateral joint capsule, contributing to a more comprehensive plication of the lateral ligament complex.7,22 The ALCS technique is conceptually similar to the capsular shift procedure that is widely used to treat shoulder instability, with well-established efficacy in restoring joint stability.6,26
Various techniques have been suggested to address poor ATFL remnants. Park and Park 23 retrospectively reviewed 22 ankles that underwent MBP with periosteal flap augmentation after the excision of a large os subfibulare and reported improved functional and radiological outcomes without recurrence. Cao et al 4 suggested anatomic ligament reconstruction with allograft for CLAI patients with a large os subfibulare, reporting a satisfaction rate of 87.5%. Nakasa et al 20 performed additional mini-open CFL repair after arthroscopic ATFL repair in ankles with poor ATFL remnants and reported similar functional outcomes, despite inferior talar tilt angles compared with ankles with intact ATFL remnants. Recently, suture tape augmentation techniques have gained popularity as an adjunct to lateral ligament repair in cases with inadequate remnant tissue. 13 Recent systematic reviews have reported favorable outcomes comparable to those of MBP or AMBP.18,35 Regarding all-inside arthroscopic procedures, Vega et al 33 reported satisfactory short-term outcomes without major complications or recurrence in 15 ankles with poor ATFL remnants treated with arthroscopic all-inside ATFL repair with nonabsorbable suture augmentation. Compared with previously suggested alternative techniques for poor ATFL remnants, the outcomes for ALCS observed in the present study were satisfactory, with a low rate of recurrent instability. Taken together, the ALCS technique offers several potential advantages, including an all-inside arthroscopic approach without the need for talar anchors or synthetic augmentation materials, and may therefore represent a useful alternative for managing CLAI with poor or absent ATFL remnants.
This study has limitations. First, the retrospective nature of the study introduces the risk of assessment bias; however, we used prospectively collected data from consecutive patients and blinded the senior author to data collection and analysis to mitigate this limitation. Second, all procedures examined in this study were conducted by a single surgeon (S.H.H.), which may limit generalizability. Arthroscopic lateral ligament repair procedures may require a learning curve. However, ALCS is based on standard arthroscopic portals and instrumentation, which may facilitate reproducibility among surgeons experienced in ankle arthroscopy. Third, this study did not include direct radiological assessment of the repaired ligamentous structures, such as postoperative magnetic resonance imaging scans. Fourth, intraobserver reliability for radiographic measurements was not assessed in this study. Lastly, no biomechanical studies have been conducted to validate the stabilizing effects of this technique. Future cadaveric and prospective multicenter studies are needed to validate and generalize the findings of this study.
Our study showed that ALCS achieved clinical and radiological outcomes comparable to those of AMBP, with low recurrence rates after at least 2 years of follow-up. Our results suggest that ALCS may be a viable operative treatment option for patients with CLAI but poor ligament remnants.
Footnotes
Acknowledgements
MID (Medical Illustration & Design), a member of the Medical Research Support Services of Yonsei University College of Medicine, provided excellent support with medical illustration.
Final revision submitted March 30, 2026; accepted May 10, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
This study was approved by the institutional review board of Gangnam Severance Hospital (approval No.: 3-2025-0273).