Abstract
Background:
Various studies have examined anatomic risk factors for Unilateral ACL tears (U-ACL). Only one study has focused on the notch width index (NWI) in patients with Contralateral ACL tears (C-ACL).
Hypothesis:
U-ACL and C-ACL will have common anatomic risk factors.
Methods:
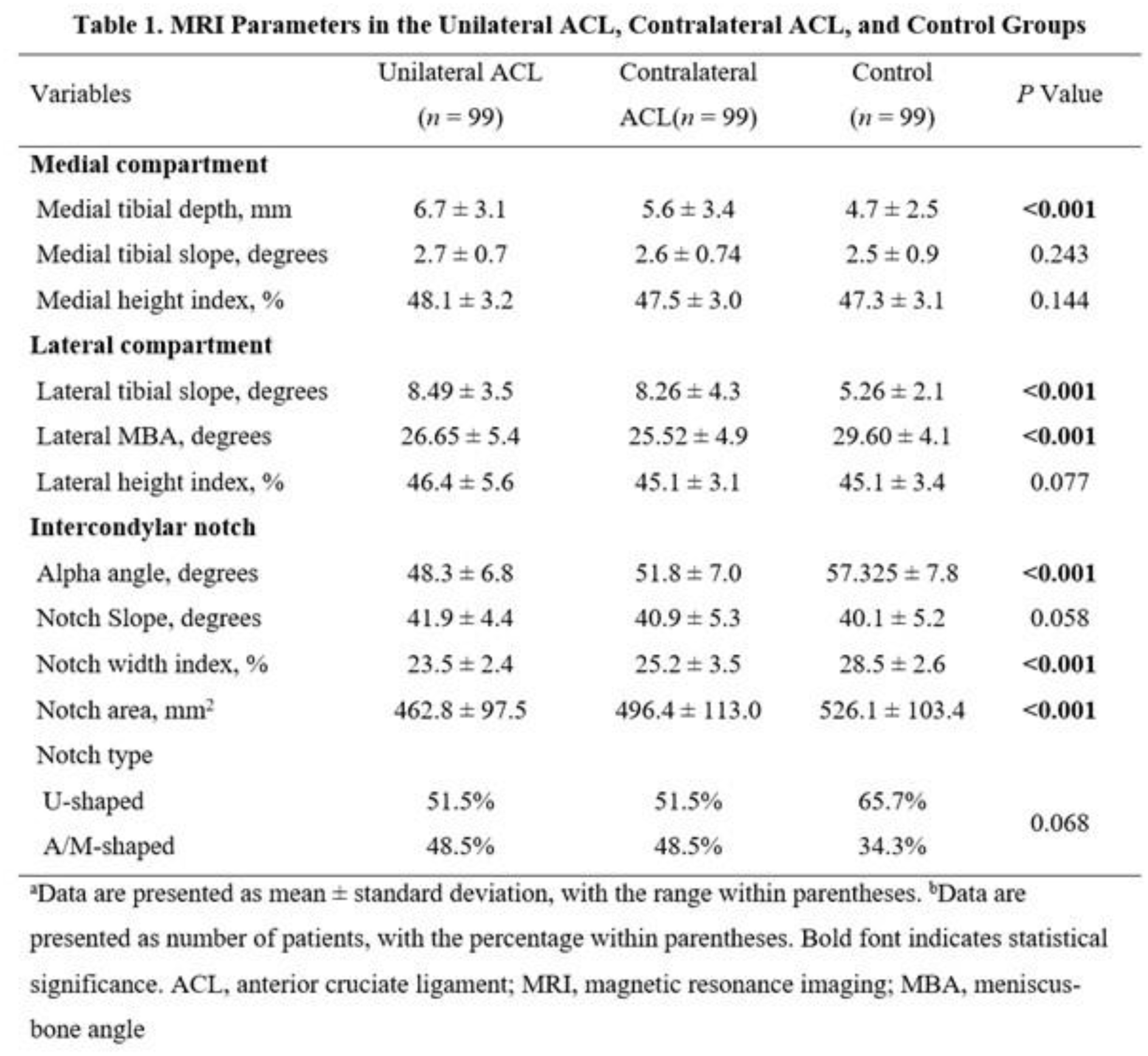
We retrospectively analyzed 297 pediatric patients matched by age, sex, and body mass index (BMI), including 99 with U-ACL, 99 with C-ACL (who had a prior ipsilateral tear), and 99 controls with anterior knee pain. These patients were treated at a single pediatric hospital between 2009 and 2024. Demographic data were collected, and MRI measurements included lateral tibial slope (LTS) and posterior lateral compartment meniscus-bone angle (LMBA) in the lateral compartment, medial tibial slope (MTS) and medial tibial depth (MTD) in the medial compartment, and alpha angle, intercondylar NWI, notch slope, notch area, and notch shape (classified as U-, M-, or A-shaped) in the intercondylar notch. Variables showing significant differences among groups in univariate analysis using Kruskal-Wallis or Chi-square tests were included as independent variables in the multivariate analysis.
Results:
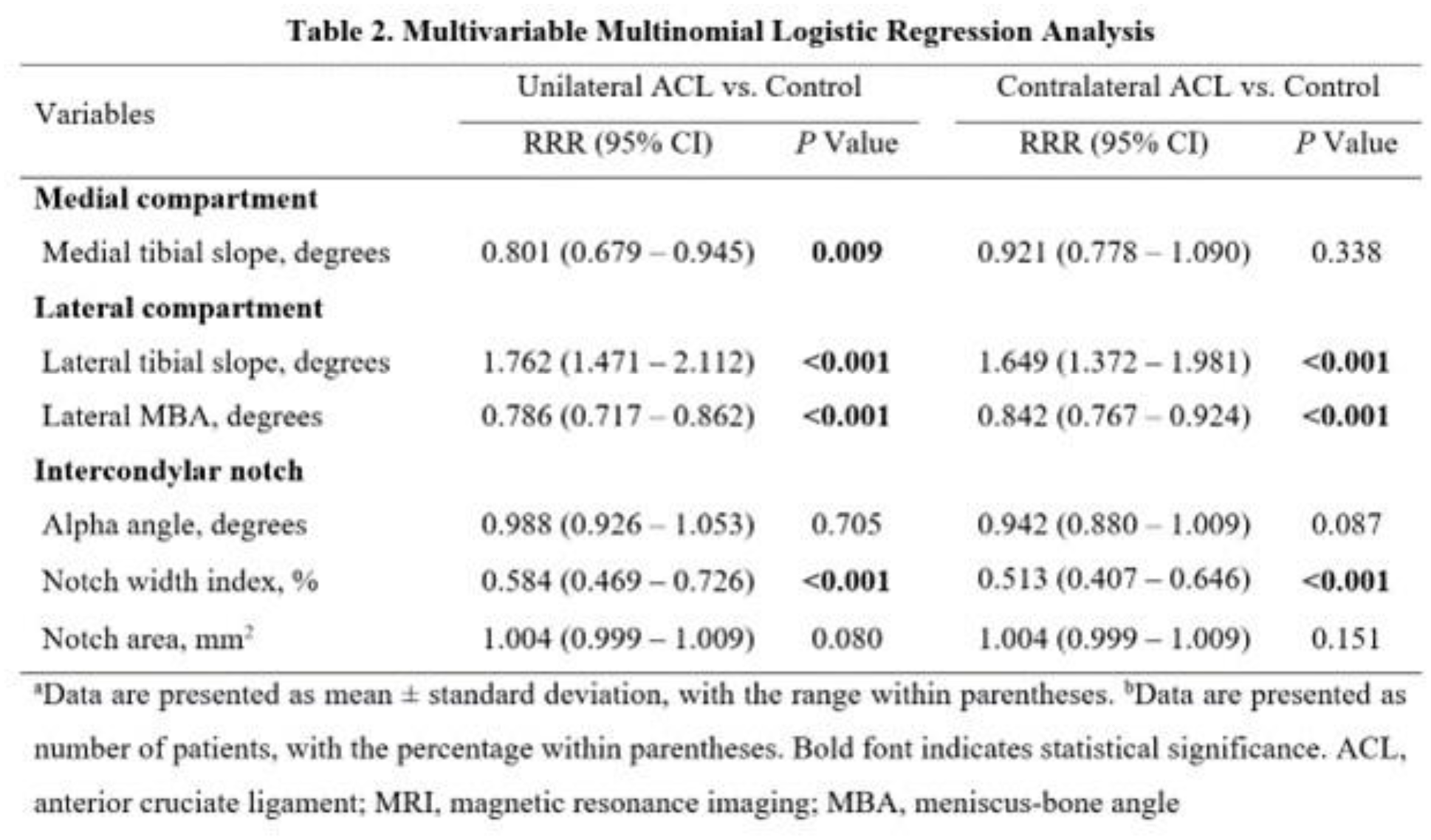
The mean age at MRI was 15.19 ± 2.1 years. Demographic characteristics were similar across groups in terms of age, sex, race, weight, and BMI (p>0.05), except for height, which was lower in the control group (p<0.05). MTD, LTS, LMBA, alpha angle, NWI, and notch area were significantly different among the groups and included in the multivariable analysis. In multivariate multinomial logistic regression, increased LTS was associated with a higher risk of both U-ACL and C-ACL (U-ACL: relative risk ratio (RRR) 1.762, 95% confidence interval (CI) 1.471–2.112; C-ACL: RRR 1.649, 95% CI 1.372–1.981). Similarly, lower LMBA (U-ACL: RRR 0.786, 95% CI 0.717–0.862; C-ACL: RRR 0.842, 95% CI 0.767–0.924) and NWI (U-ACL: RRR 0.584, 95% CI 0.469–0.726; C-ACL: RRR 0.513, 95% CI 0.407–0.646) were associated with a higher risk of both U-ACL and C-ACL. MTD was associated with U-ACL (RRR 0.801, 95% CI 0.679–0.945) but not with C-ACL (RRR 0.921, 95% CI 0.778–1.090).
Conclusion:
This is the first study to compare knee morphology on MRI between patients with U-ACL and C-ACL and controls, highlighting three key anatomical risk factors for C-ACL. High LTS, lower LMBA, and narrow intercondylar notch are common risk factors for both U-ACL and C-ACL. MTD was not a risk factor for C-ACL.