Abstract
Background:
Pediatric ACL tears are an increasingly common injury and many ultimately require surgical reconstruction. Numerous studies have identified ACL anatomic landmarks in adult knees to guide optimal graft placement and restore function. However, limited data is available regarding pediatric ACL landmarks. This study describes the ACL femoral origin anatomy in skeletally-immature knees and with comparison to adult data. These results may improve pediatric ACL graft placement while minimizing risk of physeal damage.
Hypothesis:
We hypothesize that the relative positioning of key anatomical landmarks will be qualitatively similar to previous measurements in adult specimens, while precise measurement results will be distinct given the smaller specimen sizes and incomplete joint development.
Methods:
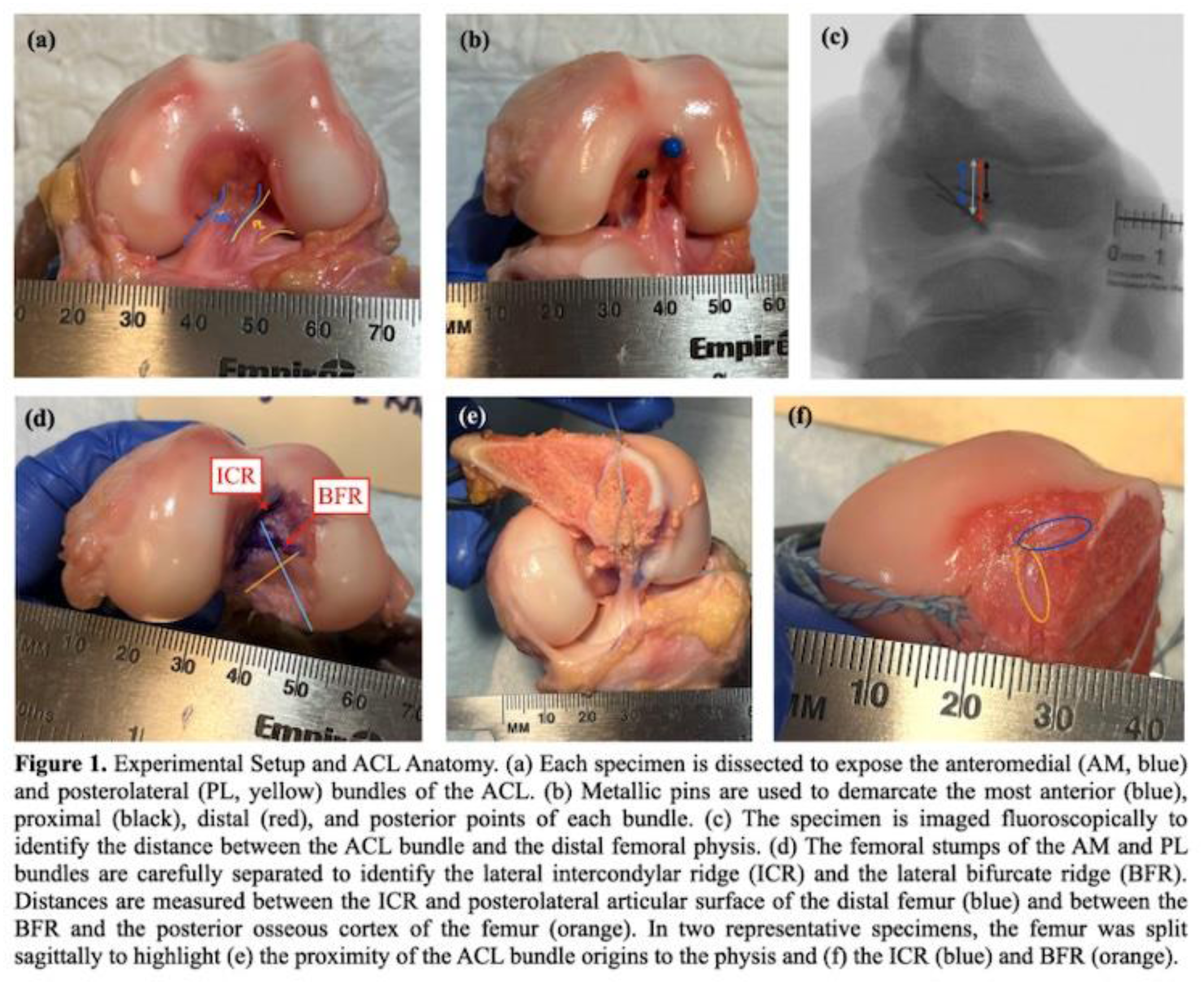
5 fresh-frozen 3-year-old pediatric cadaveric knees were dissected to expose the ACL anteromedial (AM) and posterolateral (PL) bundles. Caliper measurements of the femoral footprints of these bundles were recorded, and spatial relationships to the distal femoral physis were assessed using fluoroscopy. Finally, the ACL was carefully removed to study the osteology of the lateral intercondylar ridge (ICR) and lateral bifurcate ridge (BFR).
Results:
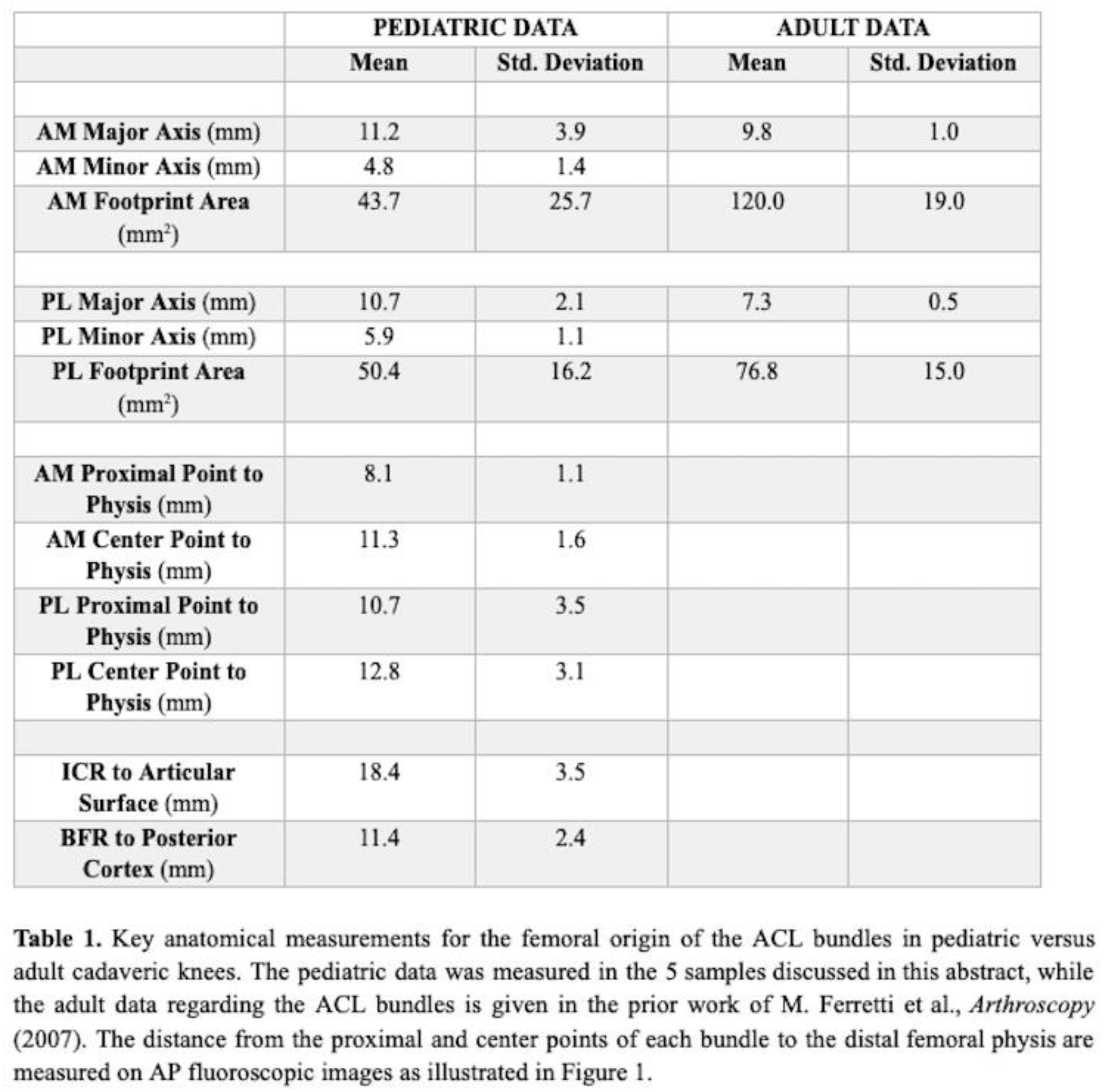
The major axis, minor axis, and area of the AM bundle footprint was (11.1±3.9)mm, (4.8±1.4)mm, and (43.7±25.7)mm^2, respectively. For the PL bundle footprint, these values were (10.7 ± 2.1)mm, (5.9±1.1)mm, and (50.4±16.2)mm^2, respectively. The center points of these footprints were (11.3±1.6)mm and (12.8±3.5)mm below the distal femoral physis, while their most proximal points were (8.1±1.1)mm and (10.7±3.5)mm, respectively. The ICR was (18.4±3.5)mm away from the femoral articular surface, and the BFR was (18.1±0.9)mm away from the posterior cortex of the intercondylar notch. Additional measurements and comparisons with prior data from adult knees are presented in Table 1.
Conclusion:
The femoral footprint areas of the ACL bundles in 3-year-old knees were approximately 50% of those in adult knees, despite being only 25% of the age of skeletal maturity. However, the eccentricity of the pediatric ACL bundle footprints was consistently higher, as the major axis length for each bundle was similar between pediatric and adult knees. The proximity of the femoral physis to the ACL origin demonstrates that precise graft placement can be performed without significant physeal injury, but the margin for error is small. These observations motivate usage of pediatric-specific techniques for restoring native ACL anatomy in skeletally-immature knees.