Abstract
Background:
The lateral extra-articular tenodesis (LET) is performed during ACL reconstruction to reduce graft failure and rotational laxity, particularly in pediatric patients with the highest risk of recurrent ACL tears. [1–3] Prior anatomic research in pediatric knees has shown that the Anterolateral Ligament (ALL) and Lateral Collateral Ligament (LCL) origins are close to the distal femoral physis (DFP), and accurate ALL origin position is critical for anatomic placement of the LET femoral origin. [4] Prior research has also shown significant variability in the ALL/LET origins, that varies with age. [5] This study aims to define the relationships of the DFP, the ALL and the LCL origins, to guide anatomic placement of the LET graft without causing significant femoral physeal injury.
Hypothesis:
The ALL femoral origin is closer to the Distal Femoral Physis than the LCL femoral origin.
Methods:
Seven skeletally immature cadaveric knees (aged 8 to 16) were dissected. The iliotibial band (ITB) was resected to reveal the ALL and LCL. Tibial internal rotation was utilized to enhance visualization of the ALL. Metallic pins were placed at the ALL and LCL femoral origins (Figure 1). Sagittal and coronal fluoroscopic images with a ruler were captured. The distance from each pin to the DFP was measured. The relationships of ALL and LCL origins and DFP were determined using coronal views, and sagittal views were used to verify ALL/LCL relationships.
Results:
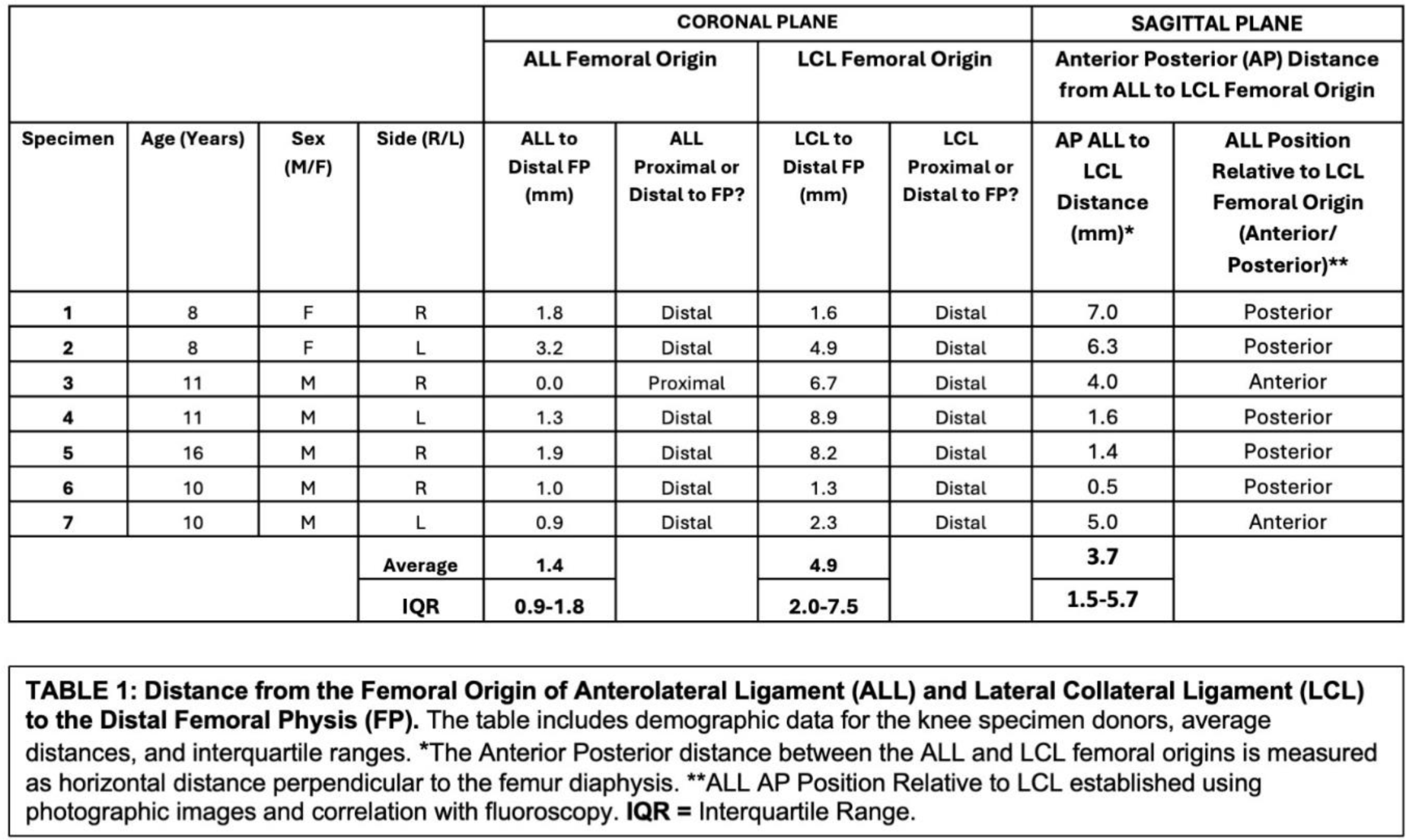
On the coronal sequences, 6/7 ALL origins, and 7/7 LCL origins were distal to the DFP. The ALL femoral origin was 1.4 mm (IQR: 0.9-1.8) distal to the DFP. The LCL femoral origin was 4.9 mm (IQR: 2.0-7.5) distal to the DFP (Table 1). In the sagittal plane, the ALL origin was 3.4 mm (IQR: 1.4-6.3) posterior to the LCL origin in 5/7 specimens and 4.5 mm (IQR: 4.3-4.8) anterior to the LCL origin in 2/7 specimens.
Conclusion:
Our findings confirm that the ALL and LCL origins are in close proximity to each other and the femoral physis, with some positional variability. Anatomic reconstruction of the LET using the ALL femoral origin as a landmark suggests that the graft origin position should be at least 1.4mm distal to the physis and 3.4 mm posterior to the LCL origin. These findings highlight the need to modify LET tunnel positioning using anatomic and radiographic landmarks to minimize the risk of physeal injury and optimize ACL/LET reconstruction outcomes in skeletally immature patients.