Abstract
Background:
Measuring the pupillary light response (PLR) with automated pupillometry (AP) may provide an objective biomarker that reflects underlying autonomic dysfunction (AD) following concussion. AP is quick and non-invasive, making it an ideal tool for evaluating pediatric concussion. Previous studies identified PLR abnormalities in concussed adolescents, but few have explored how pupillometry metrics vary over time or correlate with subjective measures of symptom severity.
Hypothesis:
At the initial post-injury clinic visit, PLR metrics in adolescent concussion patients will differ based on time since injury and correlate with symptom severity.
Methods:
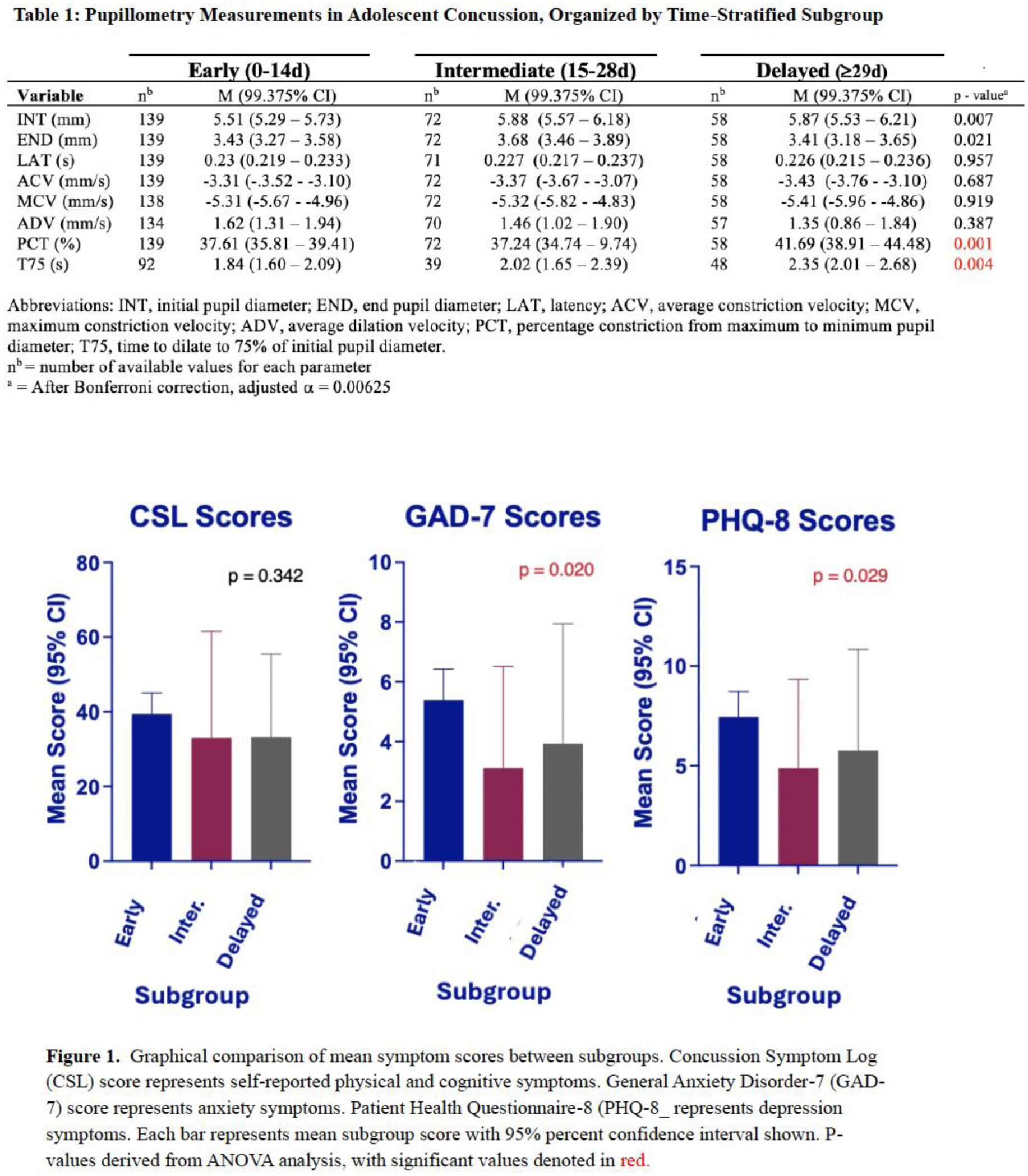
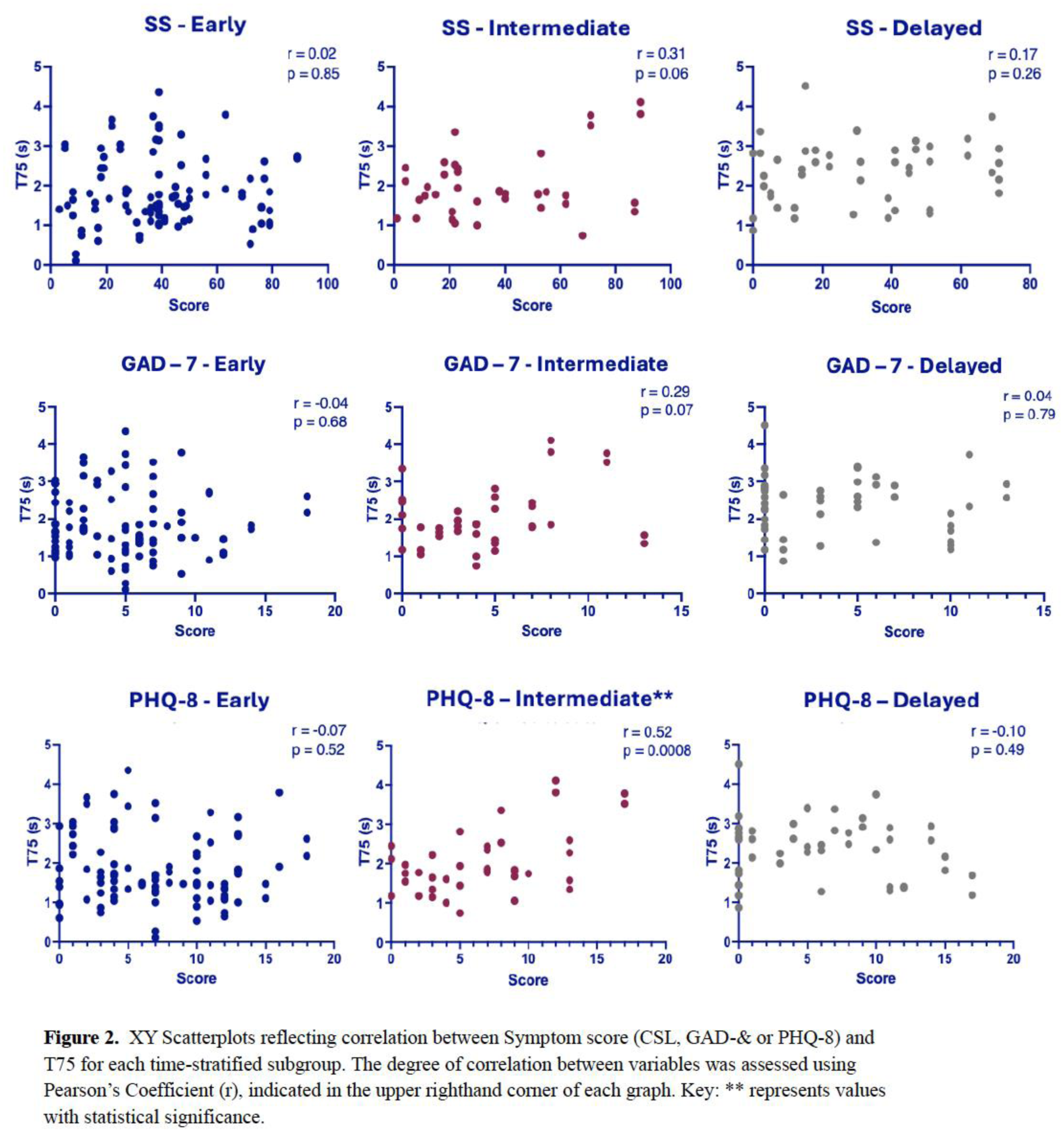
Data were prospectively collected from participants (ages 12-18) enrolled in the North Texas Concussion Registry (ConTex). At initial clinic visit, participants completed Symptom Scores (SS, via Concussion Symptom Log), PHQ-8/GAD-7, and pupillometry on one or both eyes. Each eye represented an individual data point (n=269). Data were stratified by days-post-injury (DPI) at time of presentation; early (0–14 DPI), intermediate (15–28 DPI), and delayed (29+ DPI). Eight pupillometry metrics were evaluated using two-way ANOVA with Bonferroni correction and reported as mean +/- SD. Pearson’s r was used to assess the relationship between pupillary metrics and SS across timepoints.
Results:
Pupillometry revealed significant differences in Time-to-75%-Dilation (T75, p=0.004), with greater values observed in delayed (2.4±0.3s) versus early (1.8±0.3s) and intermediate (2.0±0.4s) groups. There were no significant differences (p=0.34) in SS between early (39.4±-5.7), intermediate (33.0±9.8), and delayed (33.2±8.5) groups. GAD-7/PHQ-8 scores were significantly higher (p=0.02/p=0.03) in the early group (5.4±1.0/7.6±1.3) versus intermediate (3.1±1.2/4.9±1.5) and delayed (3.9±1.5/5.8±1.9) groups. T75 did not correlate with SS at any timepoint; early (r=0.01±0.3;p=0.90), intermediate (r=0.3±0.4;p=0.14), or delayed (r=0.1±0.4;p=0.50). T75 did not correlate with GAD-7 scores in any group; early (r=-0.1±0.3;p=0.59), intermediate (r=0.4±0.4;p=0.09), or delayed (r=-0.1±0.4;p=0.78). T75 correlated positively with PHQ-8 scores only in the intermediate (r=0.5±0.4;p=0.009) group.
Conclusion:
Concussed adolescents demonstrate prolonged pupillary response (T75) that is most apparent in those evaluated later post-injury. This may reflect a greater degree of AD in adolescents presenting later after concussion. Individuals presenting earlier reported more anxious and depressive symptoms, despite having similar symptom severity overall. T75 appears independent of SS across all timepoints, which might reflect a discrepancy between symptom burden and physiologic dysfunction. Prolonged pupil response (T75) after concussion may indicate persistent neurologic dysfunction, supporting PLR as a potential biomarker that could be used to guide recovery and return-to-play decisions. Incorporating AP into pediatric concussion assessments could improve clinicians' ability to identify persisting AD and provide opportunities for targeted interventions throughout recovery.