Abstract
Background:
Low energy availability (LEA) is characterized by mismatch between energy intake and exercise energy expenditure. LEA is common in female athletes and can induce a catabolic physiologic state, reducing muscle protein synthesis. While emerging evidence reflects impaired neuromusculoskeletal training response among adult athletes with LEA, this has not been explored in adolescents, including females who undergo anterior cruciate ligament reconstruction (ACLR), who may represent a high-risk sub-population, with sex-based disparities in return to sport (RTS) outcomes post-ACLR.
Hypothesis:
Female athletes with LEA indicators would demonstrate impaired strength gains on their non-operative limb, compared to those without LEA indicators, during 6- and 9-month post-ACLR testing.
Methods:
In this retrospective case-control study, females (age 13-18 years) post-ACLR who completed a standardized 10-session neuromuscular training program starting 6-months post-ACLR, with bilateral isometric strength measurements at 6- and 9-months post-ACLR, were included. Subjects with prior surgery on the ipsilateral or contralateral leg, hormonal medication exposure, and/or polycystic ovarian syndrome were excluded. Indicators of LEA were defined as menstrual dysfunction (amenorrhea, oligomenorrhea) and/or diagnosed eating disorder. Separate repeated measures analyses of variance were used to compare (non-operative limb) quadriceps, hamstrings, and gluteus maximus strength (normalized to body weight) between subjects with and without LEA at 6- and 9-months post-ACLR.
Results:
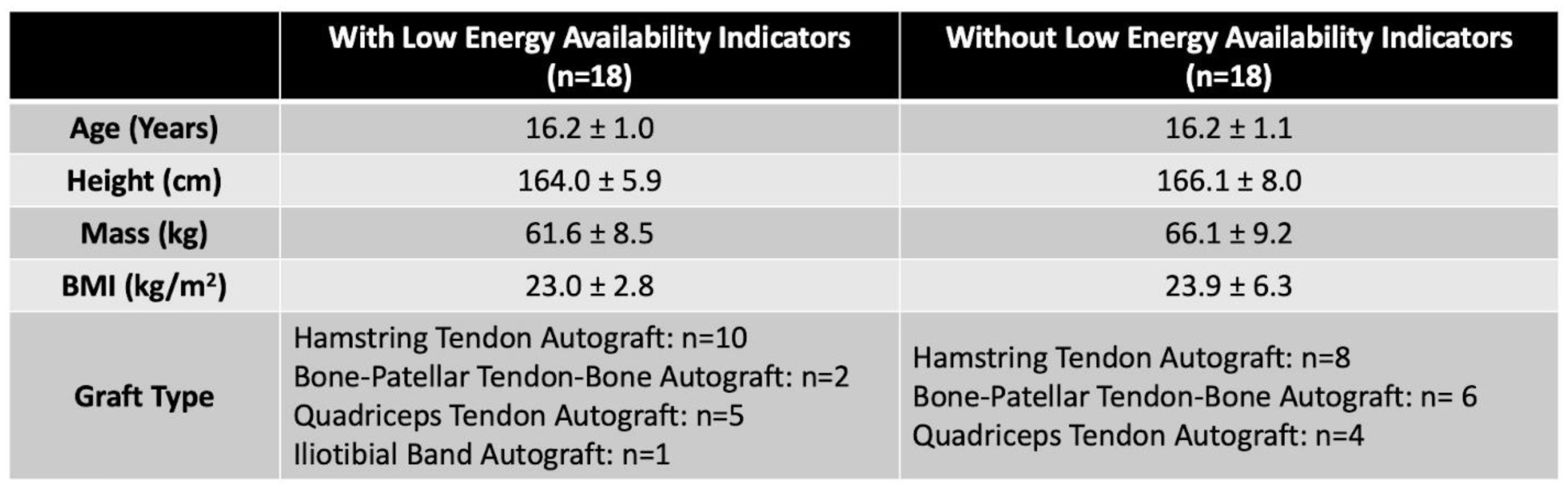
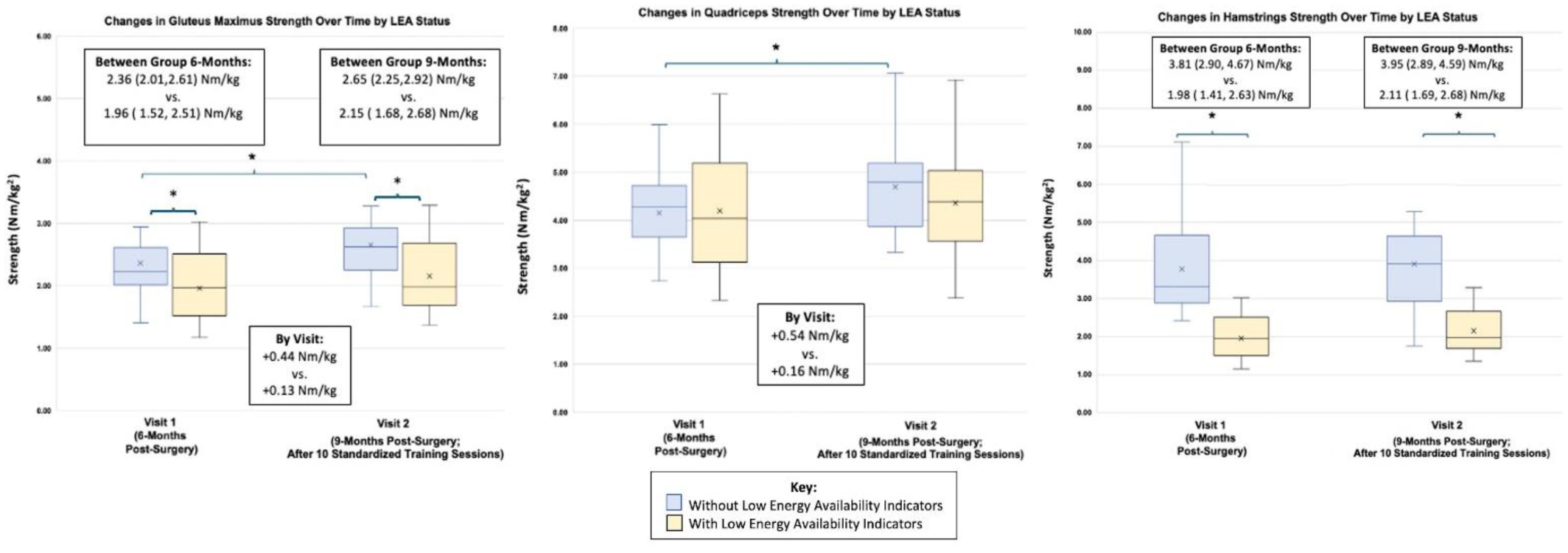
76 participants met inclusion criteria, with 18 (23.7%) classified as having LEA (age: 16.1± 1.0 years), age-matched to 18 participants without LEA (16.2± 1.1 years; Table 1). There was no significant difference in BMI (group with LEA: 23.0 ± 2.8 kg/m2, group without: 23.9 ± 6.3 kg/m2; p=0.217), nor the proportion of graft types between groups (X^2 =3.33, p=0.343). Quadriceps strength did not increase significantly in the group with LEA (+0.16 Nm/kg, p=0.594), but did in the group without (+0.54 Nm/kg, p=0.011). Hamstring strength was lower in the group with LEA than the group without at both 6- and 9-months post-ACLR (mean +1.8 Nm/kg across timepoints, p<0.001). Gluteus maximus strength did not increase significantly in those with LEA (+0.13Nm/kg, p=0.235), but did in those without (+0.44Nm/kg, p=0.015). (Figure 1)
Conclusion:
In the present study, the first investigating the impact of LEA on neuromuscular training outcomes in adolescents, female athletes with LEA demonstrated impaired strength gains on their non-operative limb during post-ACLR rehabilitation compared to those without LEA. Further research is needed to assess interventions to mitigate LEA and its impact on post-ACLR recovery, particularly among adolescent females, to optimize strength associated with RTS outcomes and ipsilateral reinjury/contralateral injury risk.