Abstract
Background:
The management of full-thickness cartilage lesions within the patellofemoral joint presents unique challenges for the treating surgeon. The use of a cryopreserved viable chondrocyte osteochondral allograft (OCA) has become popular in the management of these lesions due to its size, shape, and malleability. These allografts provide a flexible material that conforms to the variable contour of the patellar articular surface. Although this product has been studied for patellofemoral lesions in adults, it has yet to be studied in adolescents.
Hypothesis:
To report on the utilization and outcomes of cryopreserved viable chondrocyte OCA for the treatment of patellar osteochondral lesions in adolescents.
Methods:
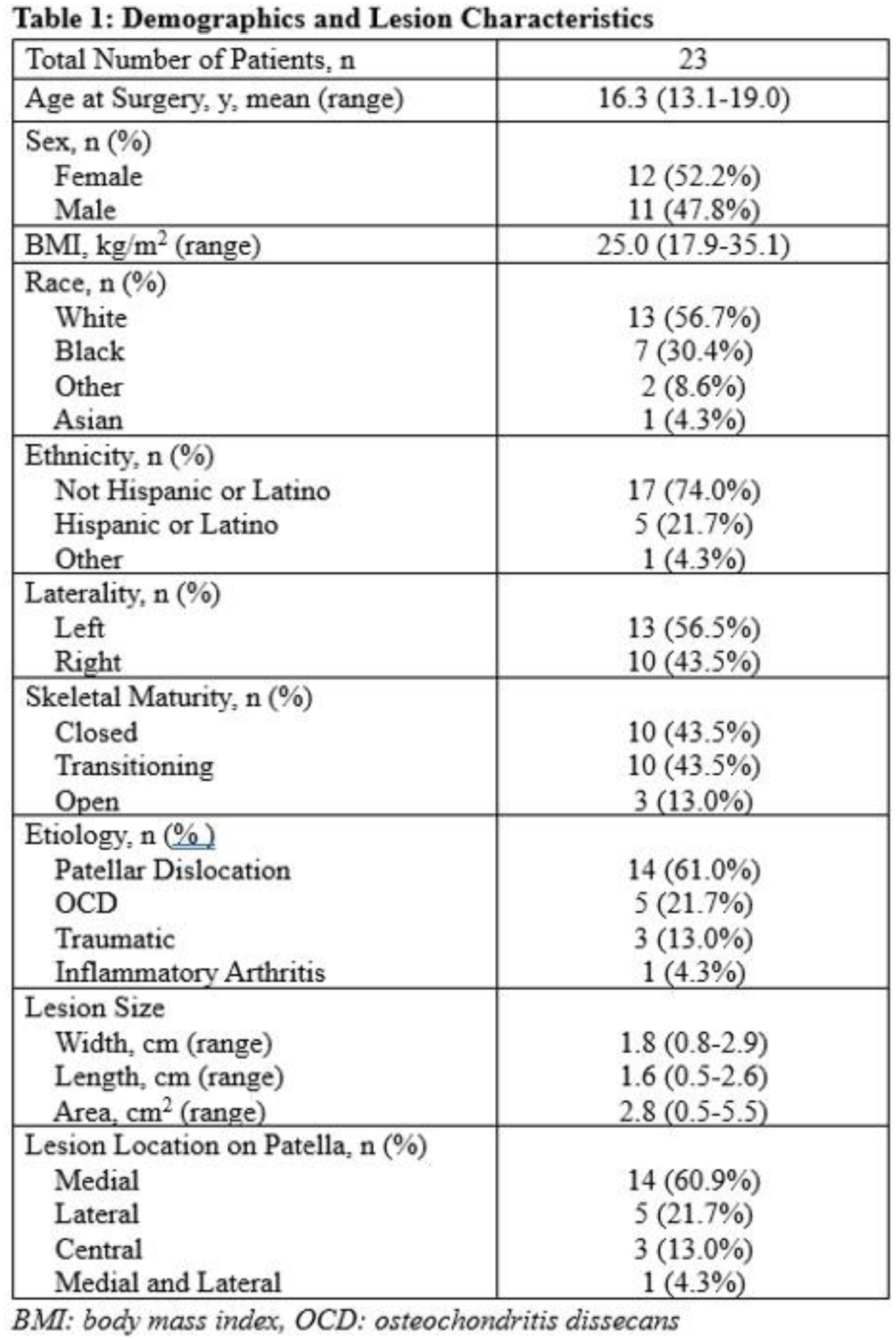
A retrospective analysis of a consecutive series of patients treated at a single institution with cryopreserved viable chondrocyte OCA for patellar osteochondral lesions was performed. Skeletal maturity was determined by distal femoral and proximal tibial physeal status on MRI (open: both physes open, transitioning: either physis in transition, closed: both physes closed). All lesion characteristics were recorded from surgeon operative reports. Postoperative outcomes were collected via chart review. All patients were included regardless of follow-up length to ensure the inclusion of all complications. Descriptive statistics were performed of cohort demographics, lesion characteristics, concomitant procedures, and postoperative outcomes.
Results:
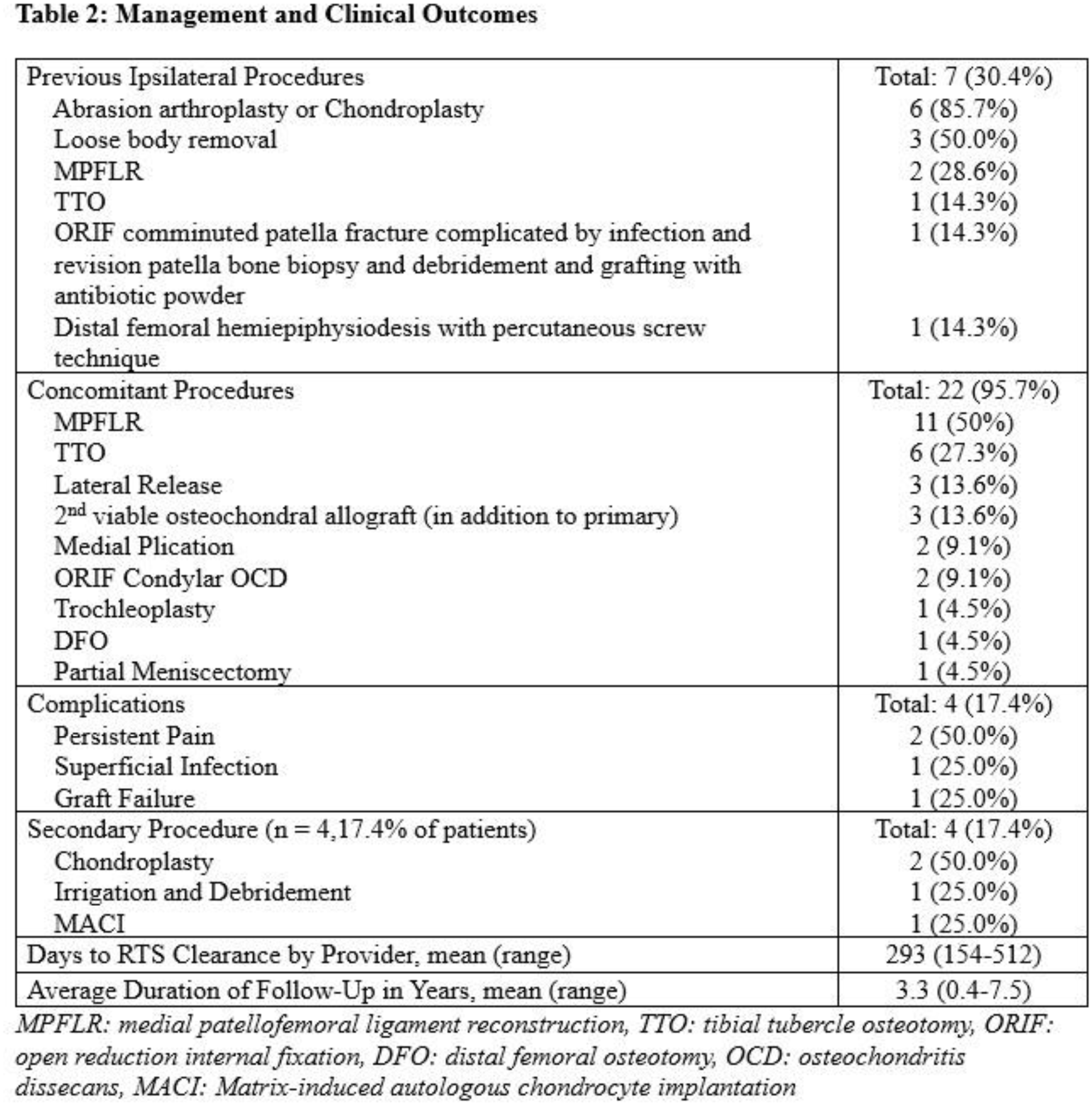
A total of 23 patients underwent cryopreserved viable chondrocyte OCA transplantation for patellar cartilage defects. Mean follow-up was 3.3 years (range, 0.4-7.5 years). The average age was 16.3 (13.1-19.0) years, of which 13/23 (57%) demonstrated open or transitional physeal status. The most common etiology of patellar osteochondral disease was patellar instability (61%). The most common lesion location was the medial patellar facet (61%). 30% of patients underwent a prior procedure and 96% underwent a concomitant procedure, most commonly an MPFL reconstruction (48%). Four (17%) patients experienced a complication: 2 (9%) had persistent pain and underwent a knee arthroscopy with chondroplasty, 1 (4%) developed a superficial infection requiring incision and drainage, and 1 (4%) experienced graft failure requiring a second cartilage procedure. On average, patients were cleared to return to sports at 9.1 months.
Conclusion:
Cryopreserved viable chondrocyte OCA appears to be a safe and versatile option for the treatment of patellar osteochondral defects in both skeletally immature and mature adolescent patients. These allografts allow for single-stage treatment of a variety of moderate to large patellar chondral lesions with complication rates comparable to other graft options.