Abstract
Background:
Quadriceps strength is one of the most widely utilized criteria to evaluate recovery and determine a patient’s readiness for activity progression following anterior cruciate ligament reconstruction (ACL-R). Research has shown a wide variation in clinical practice with clinicians utilizing isometric or isokinetic testing methods, particularly during early recovery. Isometric testing statically evaluates muscle force production at a single knee angle, while isokinetic testing assesses force production throughout a range of knee motion. Since these tests employ different types of muscle contraction, they likely evaluate different aspects of muscle physiology. The influence of muscle contraction type on measured quadriceps strength is currently unknown. Understanding the effect of testing methodology on quadriceps strength after ACL-R is necessary to inform clinical decision-making. This study examines if quadriceps strength differs based on testing method in adolescents 3 months post-ACL-R.
Hypothesis:
There will be no differences in quadriceps strength measurements between isometric or isokinetic testing methods.
Methods:
A retrospective cohort study of adolescents post-ACL-R that completed isometric (60° knee flexion, 5-second holds, 5 repetitions) and isokinetic (180°/second, 5 repetitions) strength testing using a Biodex electromechanical dynamometer. A trained physical therapist performed both tests within a single session at a standardized 3-month post-operative assessment. Bodyweight normalized peak-torque (Nm/kg) was extracted, and the quadriceps limb symmetry index (Q-LSI) was calculated using the following formula (involved peak-torque/uninvolved-peak-torque)*100. A paired samples t-test evaluated the difference between isometric and isokinetic normalized strength and Q-LSI.
Results:
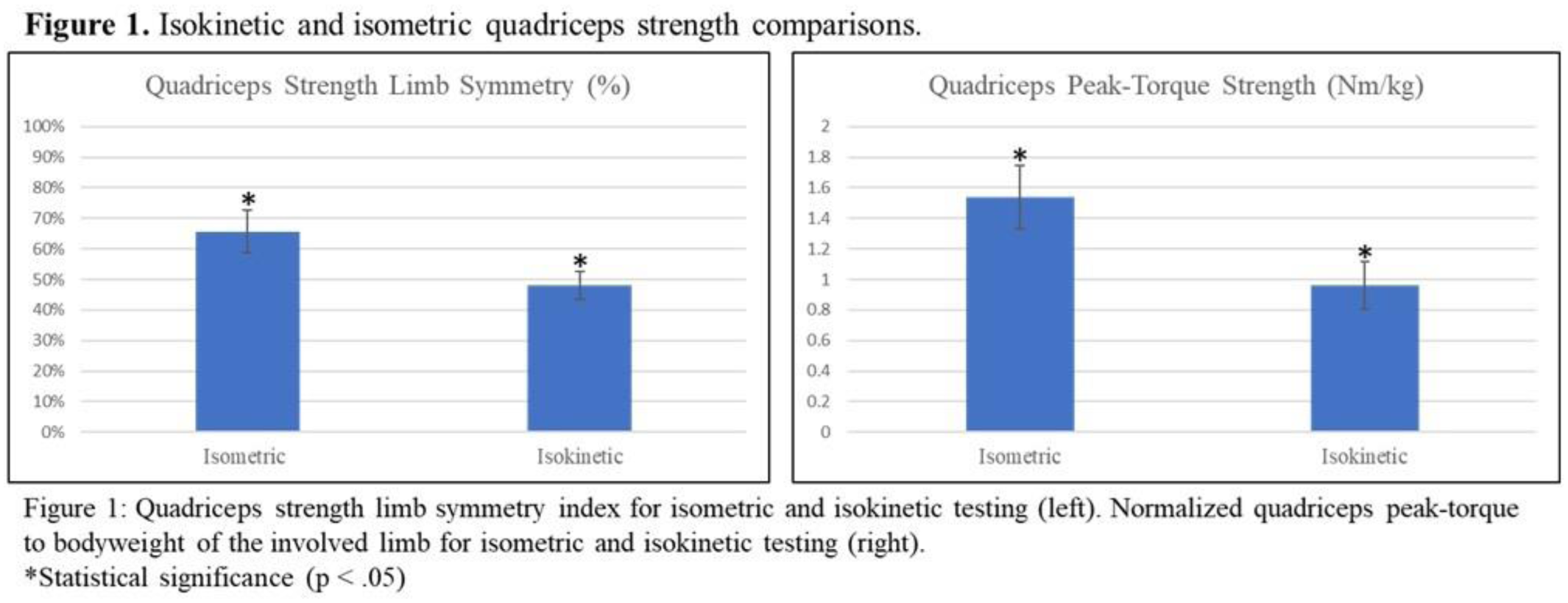
Sixteen subjects (mean 16.6 years-old, 43% female) at a mean of 97 days post-ACL-R were included (Table 1). Isometric and isokinetic assessments had statistically significant differences for both mean normalized peak-torque (1.54 Nm/kg versus 0.96, respectively; p < .001) and Q-LSI (65.6% versus 48.0%, respectively; p < .001) (Figure 1).
Conclusion:
Normalized peak-torque and Q-LSI values were different when derived from isometric or isokinetic testing methods in adolescents 3-months following ACL-R, with isometric yielding greater normalized peak-torque and higher Q-LSI than isokinetic testing. As most rehabilitation protocols utilize peak-torque and Q-LSI thresholds to determine readiness for functional progression, clinicians may make differing decisions when interpreting results from isometric or isokinetic tests. Clinicians should be aware that test methodology will affect the measured values for peak-torque and Q-LSI when making clinical judgements, developing protocols, or benchmarking patient progress against published values. Future research is necessary to understand how strength testing methods may affect clinical decision-making, patient function, or biomechanical performance during rehabilitation.