Abstract
Background:
Secondary anterior cruciate ligament (ACL) injury, additional ACL tear in either ipsilateral or contralateral knee following primary ACL injury, unfortunately occurs and has limited evidence in mechanism of injury (MOI) and timing of injury (TOI), especially focusing on ipsilateral and contralateral limb separately. (References 1, 2, 3, 4) Therefore, the purpose of this study was to examine characteristics of the secondary ACL injuries, particularly MOI and TOI and compare them between ipsilateral and contralateral limbs in young athletes.
Hypothesis:
MOI and TOI are different between ipsilateral and contralateral secondary ACL injuries.
Methods:
In this prospective cohort study, data from young athletes (12-22 years) who sustained a primary ACL injury, had ACL reconstruction (ACLR) surgery, and performed a return-to-sport (RTS) testing were collected. ACLR surgery was performed by a single orthopaedic surgeon, and hamstring autograft was used for all patients. The follow-up duration was three years after a primary ACLR. During the follow-up, if secondary ACL injuries were found, MOI and TOI were recorded. A binary classification, contact or noncontact, was used for MOI while the period from a primary ACLR to the time sustained secondary ACL injury was calculated for TOI. Descriptive statistics were used to analyze demographics of the participants. Chi-square analysis and t-test were employed to compare MOI and TOI between ipsilateral and contralateral secondary ACL injuries.
Results:
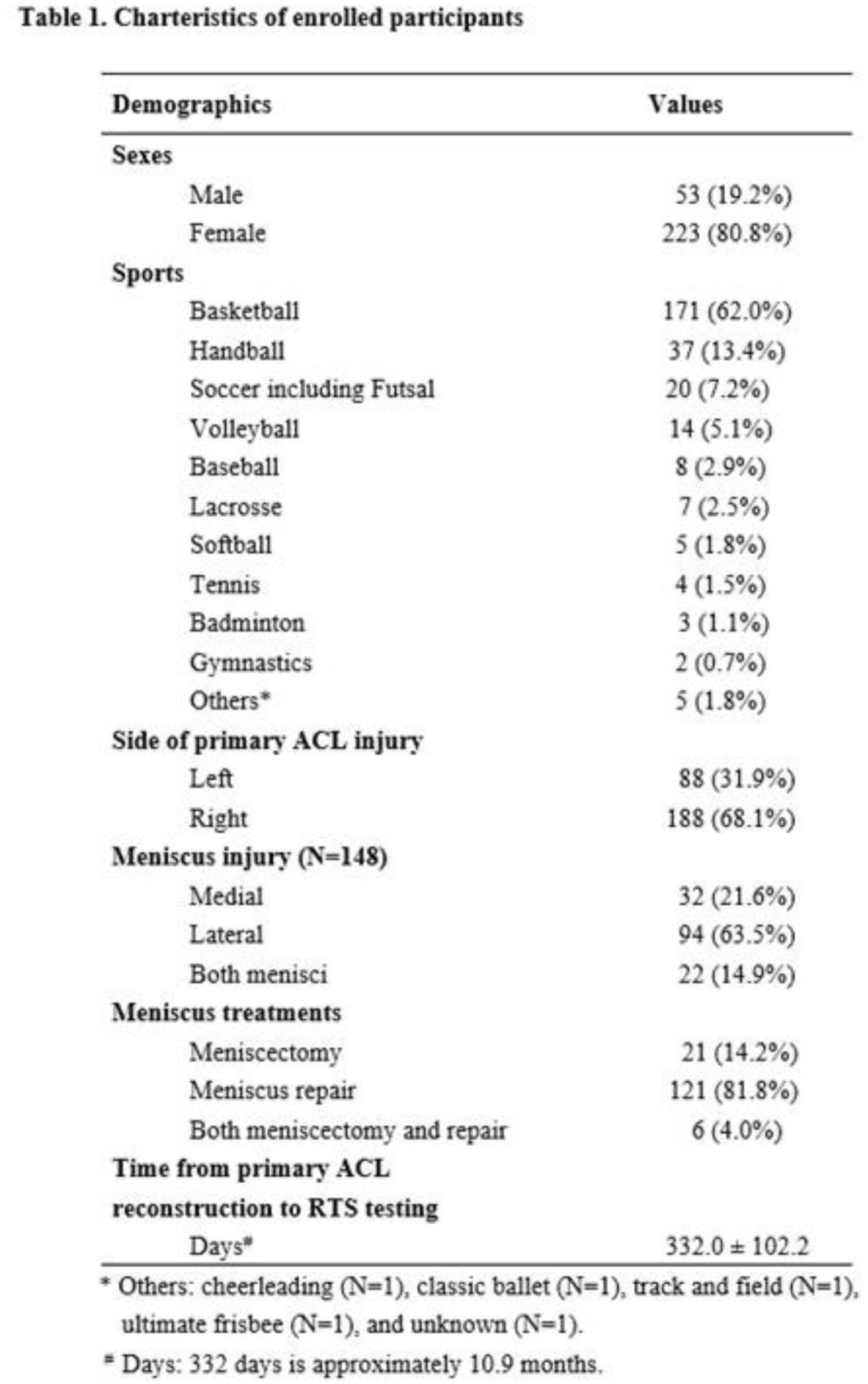
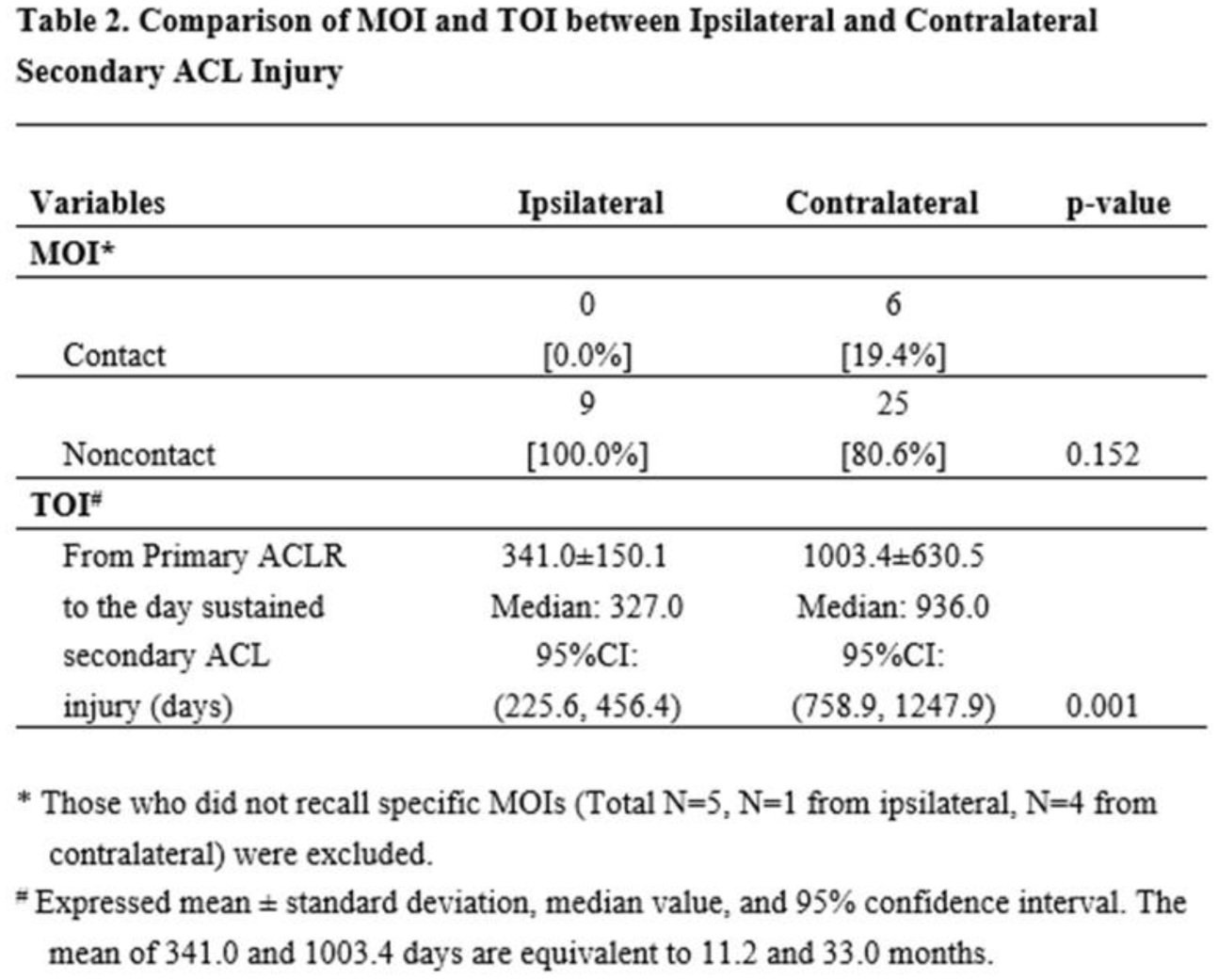
There were 276 young athletes with primary ACL injury (age:16.9±2.3 yrs, sex:female 80.8%) and 53.6% of this cohort sustained meniscus tears at the time of primary ACL injury (Table 1). During the follow-up, 45 participants sustained secondary ACL injuries (16.3%), which consisted of 10 ipsilateral (22.2%) and 35 contralateral (77.8%) sides. Among 45 secondary ACL injuries, 13.3% were contact while 75.6% were noncontact MOI. Approximately 11.1% could not recall a specific MOI. Chi-square analysis showed there was no MOI difference between ipsilateral and contralateral limbs (p=0.152, Table 2). The overall mean TOI was about 27.7 months. T-test (Mann-Whitney U) found that TOI was shorter in ipsilateral limb (mean:11.2 months) than contralateral limb (mean:33.0 months, p=0.001, Table 2).
Conclusion:
TOI of the ipsilateral limb was only 11.2 months from the primary ACLR, which was significantly sooner than contralateral side. To reduce ipsilateral secondary ACL injury, the timing of RTS testing and initiation of sport activities need to be cautiously determined. The most secondary ACL injury MOI was noncontact; thus, prevention may be possible if appropriate intervention is disseminated and implemented.